Systematic Literature Review of Health Impact Assessments in Low and Middle-Income Countries

 ,
,  ,
, 
Abstract
1. Introduction
2. Materials and Methods
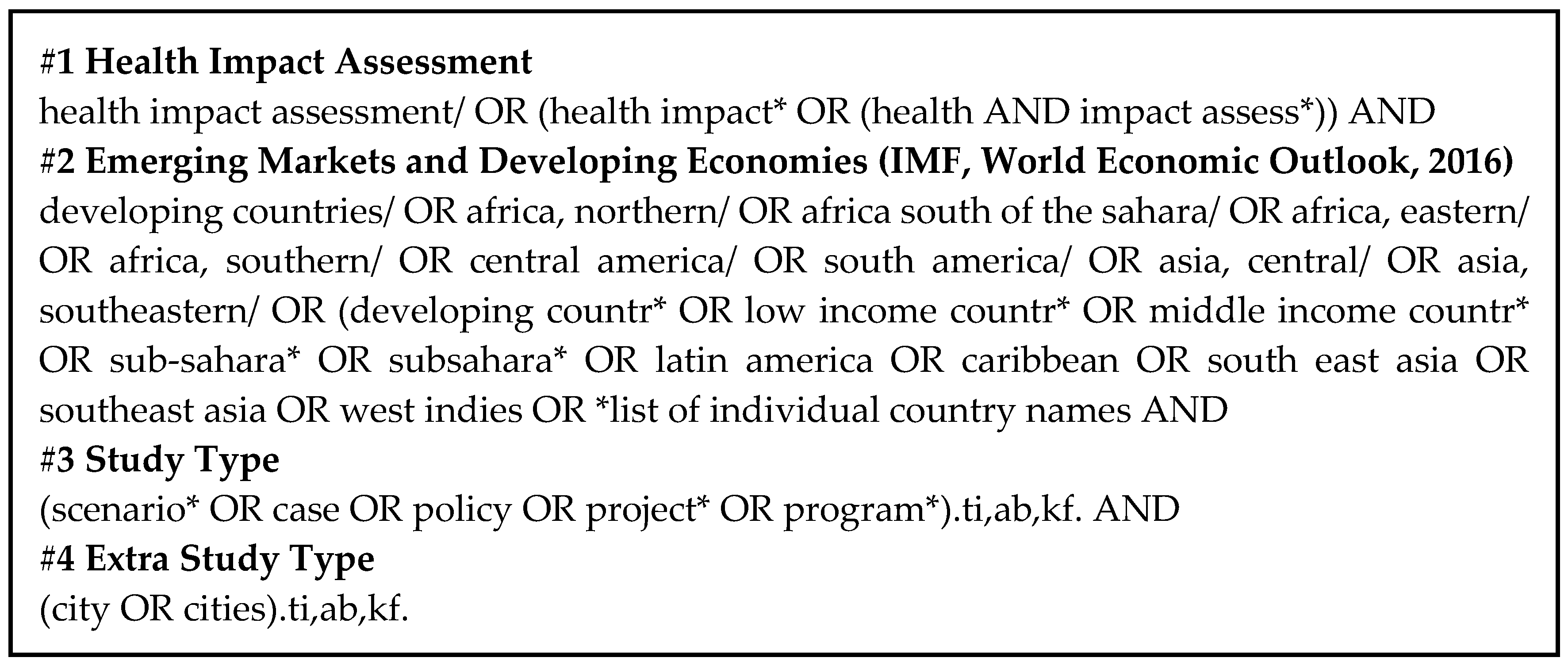
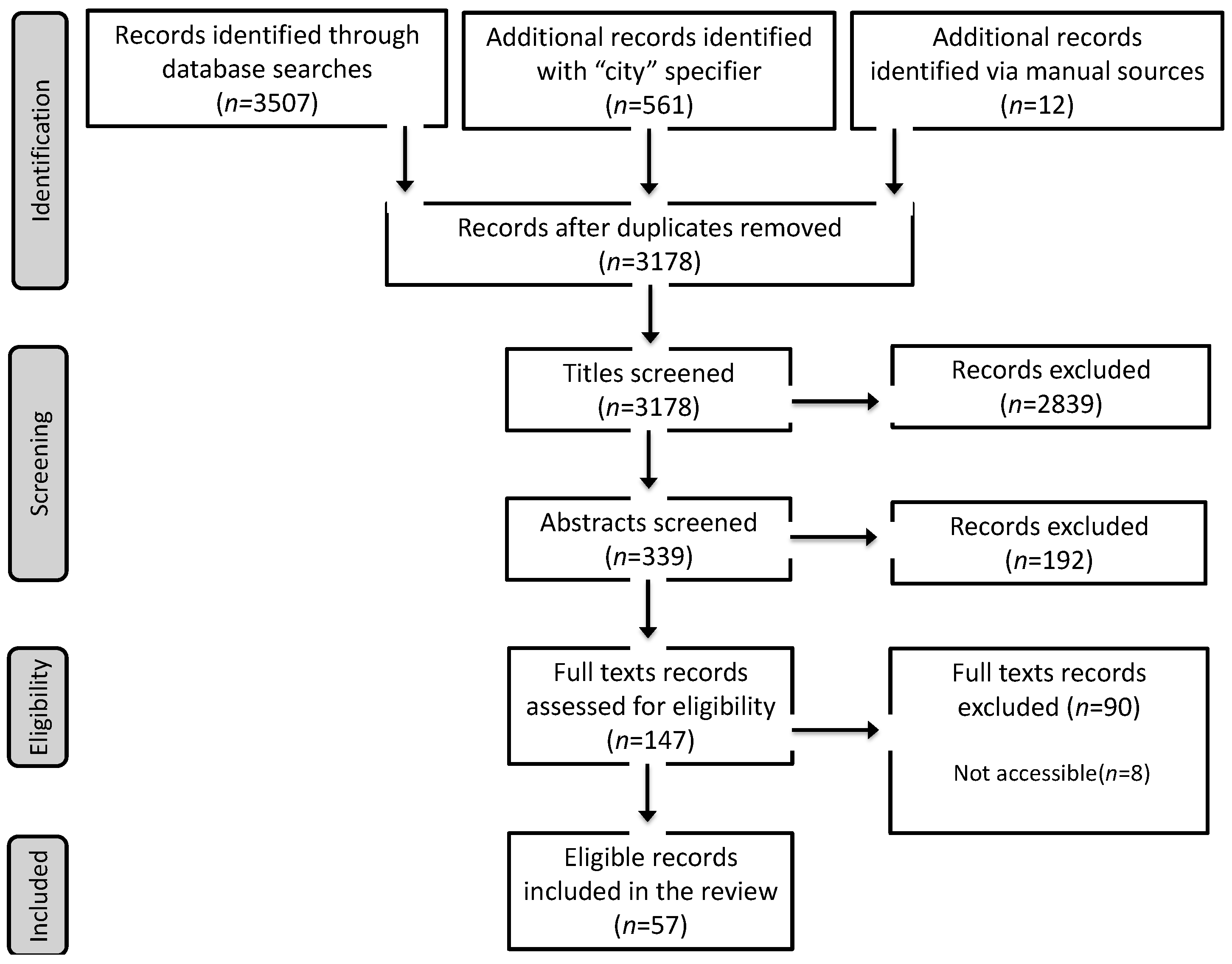
2.1. Systematic Review
2.1.1. Eligibility Criteria
- The appraisal provided a comparison between different situations and brought an assessment that would change the status quo.
- There was a clear statement and description of an intervention to be assessed. The intervention could be a program, project, or policy.
- The intervention triggered a ‘before and after’ situation: It reported a change in the distribution of exposure for at least one health pathway.
- The intervention addressed one or more problems in a specified population: It reported a change in at least one health outcome.
2.1.2. Data Extraction
2.1.3. Process Evaluation Assessment
- What data were used and what types of outcomes were calculated?
- What resources (financial, human, time) were needed to complete the HIA?
- Who and how were different stakeholders involved and engaged in the process?
- How and when were the recommendations delivered to the relevant decision makers?
- What collaborations existed that led to the publication of the HIA?
3. Results
3.1. HIA General Characteristics
3.2. Geographic Distribution and Affiliation
3.3. Results from the Process Evaluation
3.3.1. Access to Baseline Local Data
3.3.2. Reporting Resources Used
3.3.3. Based on Participatory Approaches
3.3.4. Considered Multiple Outcomes
3.3.5. Provided Recommendations
3.3.6. Fostered Cross-National Collaborations
4. Discussion
4.1. Geographic Scaling
4.2. Methods
4.3. Reporting
4.4. Recommendations
- For quantitative HIAs, assess the data availability and quality at screening and scoping stages so as to plan in advance for solutions to tackle inadequate baseline datasets (either no, insufficient, or bad data). In LMICs, both availability and quality of data should dictate whether a HIA is conducted or not; after which HIA frameworks need to be adapted to what can be done with the resources (human, financial, and time) at hand. A thorough understanding of HIA typologies (see Harris-Roxas (2011)) [137] can be helpful to identify the type of HIA most fitting for conducting a quality HIA with available data. For instance, the choice of running a rapid, intermediate or comprehensive HIA can significantly influence the scope, impact, and ultimately the action taken upon HIA estimates.
- The use and accurate reporting of participatory approaches is encouraged for all types of HIA, including quantitative HIAs.
- HIA practitioners should ensure that clear recommendations are formulated from the HIA outcomes. Such recommendations should be well-framed and delivered with adequate timing and to the right people.
- Adopt a transparent process by reporting the staff, cost, time, and training needed to conduct the HIA. This will facilitate knowledge transfer of good practices and comparative studies across countries.
- Engage into collaboration at local, regional, and international levels. Local collaboration between sectors and institutions is as important as cross-national collaborations for building awareness and increasing technical capacity in the country.
- Plan for the evaluation of successfully conducted HIAs in order to ensure quality and assess the cost-effectiveness of the process.
4.5. Study Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- European Centre for Health Policy WHO. Gothenburg Consensus Paper; European Centre for Health Policy WHO: Brussels, Belgium, 1999. [Google Scholar]
- Osofsky, S.A.; Pongsiri, M.J. Operationalising planetary health as a game-changing paradigm: Health impact assessments are key. Lancet Planet. Health 2018, 2, e54–e55. [Google Scholar] [CrossRef]
- European Centre for Health Policy WHO. Health Impact Assessment: Main Concepts and Suggested Approach; Gothenb Consens Pap Geneva WHO: Brussels, Belgium, 1999. [Google Scholar]
- Mueller, N.; Rojas-Rueda, D.; Basagaña, X.; Cirach, M.; Cole-Hunter, T.; Dadvand, P.; Donaire-Gonzalez, D.; Foraster, M.; Gascon, M.; Martinez, D.; et al. Urban and transport planning related exposures and mortality: A health impact assessment for cities. Environ. Health Perspect. 2017, 125, 89. [Google Scholar] [CrossRef] [PubMed]
- Giles-Corti, B.; Vernez-Moudon, A.; Reis, R.; Turrell, G.; Dannenberg, A.L.; Badland, H.; Foster, S.; Lowe, M.; Sallis, J.F.; Stevenson, M.; et al. City planning and population health: A global challenge. Lancet 2016, 388, 2912–2924. [Google Scholar] [CrossRef]
- Rojas-Rueda, D.; de Nazelle, A.; Andersen, Z.J.; Braun-Fahrlander, C.; Bruha, J.; Bruhova-Foltynova, H.; Desqueyroux, H.; Praznoczy, C.; Ragettli, M.S.; Tainio, M.; et al. Health Impacts of Active Transportation in Europe. PLoS ONE 2016, 11. [Google Scholar] [CrossRef] [PubMed]
- Woodcock, J.; Tainio, M.; de Sa, T.H.; de Nazelle, A.; Goel, R.; Gouveia, N.; Tiwari, G.; Verma, A.; Miranda, J.; Brage, S. Towards an Integrated Global Transport and Health Assessment Tool (TIGTHAT). J. Transp. Health 2017, 5, S99–S100. [Google Scholar] [CrossRef]
- Erlanger, T.E.; Krieger, G.R.; Singer, B.H.; Utzinger, J. The 6/94 gap in health impact assessment. Environ. Impact Assess. Rev. 2008, 28, 349–358. [Google Scholar] [CrossRef]
- Hebert, K.A.; Wendel, A.M.; Kennedy, S.K.; Dannenberg, A.L. Health impact assessment: A comparison of 45 local, national, and international guidelines. Environ. Impact Assess. Rev. 2012, 34, 74–82. [Google Scholar] [CrossRef]
- Winkler, M.; Krieger, G.R.; Divall, M.J.; Cissé, G.; Wielga, M.; Singer, B.H.; Tanner, M.; Utzinger, J. Untapped potential of health impact assessment. Bull. World Health Organ. 2013, 91, 298–305. [Google Scholar] [CrossRef]
- Health Impact Assessment (HIA) Development in ASEAN Community. Available online: https://asean.usmission.gov/innovasean_20130514/ (accessed on 14 May 2013).
- Pereira, C.A.R.; Perisse, A.R.S.; Knoblauch, A.M.; Utzinger, J.; de Souza Hacon, S.; Winkler, M.S. Health impact assessment in Latin American countries: Current practice and prospects. Environ. Impact Assess. Rev. 2017, 65, 175–185. [Google Scholar] [CrossRef]
- Tetteh, D.; Lengel, L. The urgent need for health impact assessment: Proposing a transdisciplinary approach to the e-waste crisis in sub-Saharan Africa. Glob. Health Promot. 2017, 24, 35–42. [Google Scholar] [CrossRef]
- Caussy, D.; Kumar, P.; Than Sein, U. Health impact assessment needs in south-east Asian countries. Bull. World Health Organ. 2003, 81, 439–443. [Google Scholar] [PubMed]
- Corvalán, C.F.; Kjellstrom, T.; Smith, K.R. Health, environment and sustainable development: Identifying links and indicators to promote action. Epidemiology 1999, 10, 656–660. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Global Report on Urban Health: Equitable, Healthier Cities for Sustainable Development; World Health Organization: Geneva, Switzerland, 2016; p. 242. [Google Scholar]
- Alwan, A. Global Status Report on Noncommunicable Diseases 2010; World Health Organization: Geneva, Switzerland, 2011. [Google Scholar]
- United Nations Environment Programme (UNEP). Towards a Green Economy: Pathways to Sustainable Development and Poverty Eradication; United Nations Environment Programme: Inner Robbie, Kenya, 2011. [Google Scholar]
- Landrigan, P.J.; Fuller, R.; Acosta, N.J.R.; Adeyi, O.; Arnold, R.; Basu, N.; Baldé, A.B.; Bertollini, R.; Bose-O’Reilly, S.; Boufford, J.I.; et al. The Lancet Commission on pollution and health. Lancet 2017, 391, 462–512. [Google Scholar] [CrossRef]
- O’Mullane, M. Integrating Health Impact Assessment with the Policy Process: Lessons and Experiences from Around the World; Oxford University Press: Oxford, UK, 2013. [Google Scholar]
- Silveira, M.; Fenner, A.L.D. Health impact assessment (HIA): Analyses and challenges to Brazilian health surveillance. Cienc. Saude Coletiva 2017, 22, 3205–3214. [Google Scholar] [CrossRef] [PubMed]
- Drewry, J.; Kwiatkowski, R. The role of health impact assessment in advancing sustainable development in Latin America and the Caribbean. J. Environ. Health 2015, 77, 16–20. [Google Scholar] [PubMed]
- Jobin, W. Health and equity impacts of a large oil project in Africa. Bull. World Health Organ. 2003, 81, 420–426. [Google Scholar] [PubMed]
- Winkler, M.S.; Krieger, G.R.; Divall, M.J.; Singer, B.H.; Utzinger, J. Health impact assessment of industrial development projects: A spatio-temporal visualization. Geospat. Health 2012, 6, 299–301. [Google Scholar] [CrossRef]
- Dannenberg, A.L.; Bhatia, R.; Cole, B.L.; Heaton, S.K.; Feldman, J.D.; Rutt, C.D. Use of health impact assessment in the US: 27 case studies, 1999–2007. Am. J. Prev. Med. 2008, 34, 241–256. [Google Scholar] [CrossRef]
- Künzli, N.; Kaiser, R.; Medina, S.; Studnicka, M.; Chanel, O.; Filliger, P.; Herry, M.; Horak, F.; Puybonnieux-Texier, V.; Quénel, P.; et al. Public-health impact of outdoor and traffic-related air pollution: A European assessment. Lancet 2000, 356, 795–801. [Google Scholar] [CrossRef]
- Boldo, E.; Medina, S.; Le Tertre, A.; Hurley, F.; Mücke, H.-G.; Ballester, F.; Aguilera, I.; Daniel Eilstein on behalf of the Apheis group. Apheis: Health impact assessment of long-term exposure to PM2.5 in 23 European cities. Eur. J. Epidemiol. 2006, 21, 449–458. [Google Scholar] [CrossRef]
- Harris, P.; Spickett, J. Health impact assessment in Australia: A review and directions for progress. Environ. Impact Assess. Rev. 2011, 31, 425–432. [Google Scholar] [CrossRef]
- Haigh, F.; Harris, E.; Chok, H.N.G.; Baum, F.; Harris-Roxas, B.; Kemp, L.; Spickett, J.; Keleher, H.; Morgan, R.; Harris, M.; et al. Characteristics of health impact assessments reported in Australia and New Zealand 2005–2009. Aust. N. Z. J. Public Health 2013, 37, 534–546. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Cunningham, R.; Signal, L.; Bowers, S. Evaluating Health Impact Assessments in New Zealand; Ministry of Health: Kampala, Uganda, 2011.
- Mueller, N.; Rojas-Rueda, D.; Cole-Hunter, T.; de Nazelle, A.; Dons, E.; Gerike, R.; Götschi, T.; Panis, L.I.; Kahlmeier, S.; Nieuwenhuijsen, M. Health impact assessment of active transportation: A systematic review. Prev. Med. 2015, 76, 103–114. [Google Scholar] [CrossRef] [PubMed]
- Den Broeder, L.; Uiters, E.; ten Have, W.; Wagemakers, A.; Schuit, A.J. Community participation in Health Impact Assessment. A scoping review of the literature. Environ. Impact Assess. Rev. 2017, 66, 33–42. [Google Scholar] [CrossRef]
- Veerman, J.L.; Barendregt, J.J.; Mackenbach, J.P. Quantitative health impact assessment: Current practice and future directions. J. Epidemiol. Community Health 2005, 59, 361–370. [Google Scholar] [CrossRef] [PubMed]
- Mindell, J.S.; Boltong, A.; Forde, I. A review of health impact assessment frameworks. Public Health 2008, 122, 1177–1187. [Google Scholar] [CrossRef] [PubMed]
- Taylor, L.; Quigley, R. Health Impact Assessment: A Review of Reviews; Health Development Agency: London, UK, 2002. [Google Scholar]
- Mcintyre, L.; Petticrew, M. Methods of Health Impact Assessment: A Literature Review; MRC Social & Public Health Science Unit: Glasgow, Scotland, 1999. [Google Scholar]
- Quigley, R.J.; Taylor, L.C. Evaluating health impact assessment. Public Health 2004, 118, 544–552. [Google Scholar] [CrossRef]
- Mathias, K.R.; Harris-Roxas, B. Process and impact evaluation of the greater Christchurch urban development strategy health impact assessment. BMC Public Health 2009, 9, 97. [Google Scholar] [CrossRef]
- Hoehner, C.M.; Rios, J.; Garmendia, C.; Baldwin, S.; Kelly, C.M.; Knights, D.-M.; Lesorogol, C.; McClendon, G.G.; Tranel, M. Page Avenue health impact assessment: Building on diverse partnerships and evidence to promote a healthy community. Health Place 2012, 18, 85–95. [Google Scholar] [CrossRef][Green Version]
- Davenport, C.; Mathers, J.; Parry, J. Use of health impact assessment in incorporating health considerations in decision making. J. Epidemiol. Community Health 2006, 60, 196–201. [Google Scholar] [CrossRef]
- Wismar, M.; Blau, J.; Ernst, K.; Figueras, J. The Effectiveness of Health Impact Assessment: Scope and Limitations of Supporting Decision-Making in Europe; World Health Organization: Geneva, Switzerland, 2007. [Google Scholar]
- Taylor, L.; Gowman, N.Q.R. Evaluating health impact assessment. Health Dev. Agency 2003, 118, 544–552. [Google Scholar]
- Moher, D.; Shamseer, L.; Clarke, M.; Ghersi, D.; Liberati, A.; Petticrew, M.; Shekelle, P.; Stewart, L.A.; PRISMA-P Group. Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015 statement. Syst. Rev. 2015, 4, 1. [Google Scholar] [CrossRef] [PubMed]
- IMF. World Economic Outlook, October 2015; International Monetary Fund: Washington, DC, USA, 2016. [Google Scholar]
- Birley, M. A review of trends in health-impact assessment and the nature of the evidence used. Environ. Manag. Health 2002, 13, 21–39. [Google Scholar] [CrossRef]
- Health Impact Assessment (HIA): Guides & Tools. Available online: https://www.ncchpp.ca/docs/HIAGuidesTools2008en.pdf (accessed on 6 June 2019).
- McCormick, J. A Simple Guide to Choosing a Health Impact Assessment Tool; Victoria Monash University: Victoria, BC, Canada, 2009. [Google Scholar]
- Parry, J.M.; Kemm, J.R. Criteria for use in the evaluation of health impact assessments. Public Health 2005, 119, 1122–1129. [Google Scholar] [CrossRef] [PubMed]
- Nowacki, J.; Mekel, O.; Fehr, R. Generic Health Impact Assessment (HIA) guidelines—Comparative study. Das Gesundheit. 2010, 72, 39. [Google Scholar] [CrossRef]
- Scott-Samuel, A.; Birley, M.; Ardern, K. The Merseyside Guidelines for Health Impact Assessment; International Health IMPACT Assessment Consortium: Liverpool, UK, 2001. [Google Scholar]
- Bourcier, E.; Charbonneau, D.; Cahill, C.; Dannenberg, A.L. Peer reviewed: An evaluation of health impact assessments in the United States, 2011–2014. Prev. Chronic Dis. 2015, 12, E23. [Google Scholar] [CrossRef] [PubMed]
- Fakhri, A.; Maleki, M.; Gohari, M.; Harris, P. Investigating underlying principles to guide health impact assessment. Int. J. Health Policy Manag. 2014, 3, 17–22. [Google Scholar] [CrossRef] [PubMed]
- Krieger, N.; Northridge, M.; Gruskin, S.; Quinn, M.; Kriebel, D.; Smith, G.D.; Bassett, M.; Rehkopf, D.H.; Miller, C. The HIA “Promise and Pitfalls” Conference Group. Assessing health impact assessment: Multidisciplinary and international perspectives. J. Epidemiol. Community Health 2003, 57, 659–662. [Google Scholar] [CrossRef] [PubMed]
- Winkler, M.S.; Utzinger, J. The search for underlying principles of health impact assessment: Progress and prospects: Comment on “Investigating underlying principles to guide health impact assessment”. Int. J. Heal. Policy Manag. 2014, 3, 107–109. [Google Scholar] [CrossRef] [PubMed]
- Kosa, K.; Molnar, A.; McKee, M.; Adany, R. Rapid health impact appraisal of eviction versus a housing project in a colony-dwelling Roma community. J. Epidemiol. Community Health 2007, 61, 960–965. [Google Scholar] [CrossRef] [PubMed]
- Chen, C.; Chen, B.; Wang, B.; Huang, C.; Zhao, J.; Dai, Y.; Kan, H. Low-carbon energy policy and ambient air pollution in Shanghai, China: A health-based economic assessment. Sci. Total Environ. 2007, 373, 13–21. [Google Scholar] [CrossRef] [PubMed]
- Chen, C.-H.; Kan, H.-D.; Huang, C.; Li, L.; Zhang, Y.-H.; Chen, R.-J.; Chen, B.-H. Impact of ambient air pollution on public health under various traffic policies in Shanghai, China. Biomed. Environ. Sci. 2009, 22, 210–215. [Google Scholar] [CrossRef]
- Vu, V.-H.; Le, X.-Q.; Pham, N.-H.; Hens, L. Application of GIS and modelling in health risk assessment for urban road mobility. Environ. Sci. Pollut. Res. 2013, 20, 5138–5149. [Google Scholar] [CrossRef]
- Wang, X.; Mauzerall, D.L. Evaluating impacts of air pollution in China on public health: Implications for future air pollution and energy policies. Atmos. Environ. 2006, 40, 1706–1721. [Google Scholar] [CrossRef]
- Wang, X.; Smith, K.R. Secondary benefits of greenhouse gas control: Health impacts in China. Environ. Sci. Technol. 1999, 33, 3056–3061. [Google Scholar] [CrossRef][Green Version]
- Zhang, D.; Aunan, K.; Seip, H.M.; Larssen, S.; Liu, J.; Zhang, D. The assessment of health damage caused by air pollution and its implication for policy making in Taiyuan, Shanxi, China. Energy Policy 2010, 38, 491–502. [Google Scholar] [CrossRef]
- Zhang, S.; Worrell, E.; Crijns-Graus, W.; Krol, M.; de Bruine, M.; Geng, G.; Wagner, F.; Cofala, J. Modeling energy efficiency to improve air quality and health effects of China’s cement industry. Appl. Energy 2016, 184, 574–593. [Google Scholar] [CrossRef]
- He, L.-Y.; Qiu, L.-Y. Transport demand, harmful emissions, environment and health co-benefits in China. Energy Policy 2016, 97, 267–275. [Google Scholar] [CrossRef]
- Hirschberg, S.; Heck, T.; Gantner, U.; Lu, Y.; Spadaro, J.V.; Trukenmüller, A.; Zhao, Y. Health and environmental impacts of China’s current and future electricity supply, with associated external costs. Int. J. Glob. Energy Issues 2004, 22, 155–179. [Google Scholar] [CrossRef]
- Jahn, H.J.; Schneider, A.; Breitner, S.; Eissner, R.; Wendisch, M.; Kramer, A. Particulate matter pollution in the megacities of the Pearl River Delta, China—A systematic literature review and health risk assessment. Int. J. Hyg. Environ. Health 2011, 214, 281–295. [Google Scholar] [CrossRef]
- Liu, N.; Yen, C.; Fang, Z.; Tate, J.E.; Jiang, B.; Parashar, U.D.; Zeng, G.; Duan, Z.-J. Projected health impact and cost-effectiveness of rotavirus vaccination among children <5 years of age in China. Vaccine 2012, 30, 6940–6945. [Google Scholar] [PubMed]
- Mestl, H.E.S.; Aunan, K.; Seip, H.M. Health benefits from reducing indoor air pollution from household solid fuel use in China—Three abatement scenarios. Environ. Int. 2007, 33, 831–840. [Google Scholar] [CrossRef] [PubMed]
- Ren, W.; Xue, B.; Geng, Y.; Lu, C.; Zhang, Y.; Zhang, L.; Fujita, T.; Hao, H. Inter-city passenger transport in larger urban agglomeration area: Emissions and health impacts. J. Clean. Prod. 2016, 114, 412–419. [Google Scholar] [CrossRef]
- Sabel, C.E.; Hiscock, R.; Asikainen, A.; Bi, J.; Depledge, M.; van den Elshout, S.; Friedrich, R.; Huang, G.; Hurley, F.; Jantunen, M.; et al. Public health impacts of city policies to reduce climate change: Findings from the URGENCHE EU-China project. Environ. Health 2016, 15, 25. [Google Scholar] [CrossRef] [PubMed]
- Sun, D.; Fang, J.; Sun, J. Health-related benefits of air quality improvement from coal control in China: Evidence from the Jing-Jin-Ji region. Resour. Conserv. Recycl. 2018, 129, 416–423. [Google Scholar] [CrossRef]
- Charerntanyarak, L.; Prabpai, S.; Boonyakarnkul, T.; Pitiseree, K. Health impact assessment of excreta management at Udonthani Municipality, Thailand. Epidemiology 2005, 16, 160–161. [Google Scholar] [CrossRef]
- Hengpraprom, S.; Sithisarankul, P. Developing tools for health impact assessment in environmental impact assessment in Thailand. Acta Med. Okayama 2011, 65, 123–128. [Google Scholar] [PubMed]
- Li, Y.; Crawford-Brown, D.J. Assessing the co-benefits of greenhouse gas reduction: Health benefits of particulate matter related inspection and maintenance programs in Bangkok, Thailand. Sci. Total Environ. 2011, 409, 1774–1785. [Google Scholar] [CrossRef]
- Thanh, B.D.; Lefevre, T. Assessing health benefits of controlling air pollution from power generation: The case of a lignite-fired power plant in Thailand. Environ. Manage. 2001, 27, 303–317. [Google Scholar] [CrossRef]
- Abe, K.C.; Miraglia, S.G.E.K. Health Impact Assessment of Air Pollution in Sao Paulo, Brazil. Int. J. Environ. Res. Public Health 2016, 13, 694. [Google Scholar] [CrossRef]
- Sá, T.H.D.; Tainio, M.; Goodman, A.; Edwards, P.; Haines, A.; Gouveia, N.; Monteiro, C.; Woodcock, J. Health impact modelling of different travel patterns on physical activity, air pollution and road injuries for São Paulo, Brazil. Environ. Int. 2017, 108, 22–31. [Google Scholar] [CrossRef] [PubMed]
- Scovronick, N.; Franca, D.; Alonso, M.; Almeida, C.; Longo, K.; Freitas, S.; Rudorff, B.; Wilkinson, P. Air Quality and Health Impacts of Future Ethanol Production and Use in Sao Paulo State, Brazil. Int. J. Environ. Res. Public Health 2016, 13, 695. [Google Scholar] [CrossRef] [PubMed]
- Szklo, A.S.; Yuan, Z.; Levy, D. Update and extension of the Brazil simsmoke model to estimate the health impact of cigarette smoking by pregnant women in Brazil. Cad. Saude Publica 2017, 33. [Google Scholar] [CrossRef] [PubMed]
- Mahendra, A.; Rajagopalan, L. Evaluating Health Impacts from a Bus Rapid Transit System Implementation in India Case Study of Indore, Madhya Pradesh. Transp. Res. Rec. 2019. [Google Scholar] [CrossRef]
- Sharma, S.; Patil, K.V. Emission scenarios and health impacts of air pollutants in Goa. Aerosol Air Qual. Res. 2016, 16, 2474–2487. [Google Scholar] [CrossRef]
- Srivastava, H.C.; Bhatt, R.M.; Yadav, R.S. Health Impact Assessment of Development Project: Impact of Sardar Sarovar Narmada Project on Mosquito-Borne Diseases in Gujarat, India. Available online: http://www.mrcindia.org/MRC_profile/epidemiology/HIA.pdf (accessed on 5 June 2019).
- Gharehchahi, E.; Mahvi, A.H.; Amini, H.; Nabizadeh, R.; Akhlaghi, A.A.; Shamsipour, M.; Yunesian, M. Health impact assessment of air pollution in Shiraz, Iran: A two-part study. J. Environ. Health Sci. Eng. 2013, 11, 11. [Google Scholar] [CrossRef] [PubMed]
- Marzouni, M.B.; Moradi, M.; Zarasvandi, A.; Akbaripoor, S.; Hassanvand, M.S.; Neisi, A.; Goudarzi, G.; Mohammadi, M.J.; Sheikhi, R.; Kermani, M.; et al. Health benefits of PM10 reduction in Iran. Int. J. Biometeorol. 2017, 61, 1389–1401. [Google Scholar] [CrossRef] [PubMed]
- Tashayo, B.; Alimohammadi, A.; Sharif, M. A hybrid fuzzy inference system based on dispersion model for quantitative environmental health impact assessment of urban transportation planning. Sustainability 2017, 9, 134. [Google Scholar] [CrossRef]
- Büke, T.; Köne, A.Ç. Estimation of the health benefits of controlling air pollution from the Yataĝan coal-fired power plant. Environ. Sci. Policy 2011, 14, 1113–1120. [Google Scholar] [CrossRef]
- Erkoyun, E.; Sozmen, K.; Bennett, K.; Unal, B.; Boshuizen, H.C. Predicting the health impact of lowering salt consumption in Turkey using the DYNAMO health impact assessment tool. Public Health 2016, 140, 228–234. [Google Scholar] [CrossRef] [PubMed]
- Ongel, A.; Sezgin, F. Assessing the effects of noise abatement measures on health risks: A case study in Istanbul. Environ. Impact Assess. Rev. 2016, 56, 180–187. [Google Scholar] [CrossRef]
- Benaissa, F.; Alkama, R.; Annesi-Maesano, I. Assessment of air pollution impacts on population health in Bejaia city, Northern Algeria. Iran. J. Public Health 2014, 43, 1221–1228. [Google Scholar] [PubMed]
- Laid, Y.; Atek, M.; Oudjehane, R.; Filleul, L.; Baough, L.; Zidouni, N.; Boughedaoui, M.; Tessier, J.-F. Health effects of PM10 air pollution in a low-income country: The case of Algiers. Int. J. Tuberc. Lung Dis. 2006, 10, 1406–1411. [Google Scholar] [PubMed]
- Kahn, J.G.; Muraguri, N.; Harris, B.; Lugada, E.; Clasen, T.; Grabowsky, M.; Mermin, J.; Shariff, S. Integrated HIV testing, malaria, and diarrhea prevention campaign in Kenya: Modeled health impact and cost-effectiveness. PLoS ONE 2012, 7. [Google Scholar] [CrossRef]
- Renshaw, M.; Birley, M.H.; Sang, D.K.; Silver, J.B. A rapid health impact assessment of the turkwel gorge hydroelectric dam and proposed irrigation project. Impact Assess. Proj. Apprais. 1998, 16, 215–226. [Google Scholar] [CrossRef]
- Guttikunda, S.K.; Khaliquzzaman, M. Health benefits of adapting cleaner brick manufacturing technologies in Dhaka, Bangladesh. Air Qual. Atmos. Health 2014, 7, 103–112. [Google Scholar] [CrossRef]
- Gulis, G.; Mochungong, P.I.K. Health impact assessment and evaluation of a clinical waste management policy for Cameroon. J. Public Health Africa 2013, 4, 32–37. [Google Scholar] [CrossRef]
- The Cuban Experience in the Health Impact Assessment of Investment Projects. Available online: https://www.scopus.com/inward/record.uri?eid=2-s2.0-55449099919&partnerID=40&md5=44b091d33327b26d01257f023039de7f (accessed on 5 June 2019).
- Winkler, M.S.; Divall, M.J.; Krieger, G.R.; Balge, M.Z.; Singer, B.H.; Utzinger, J. Assessing health impacts in complex eco-epidemiological settings in the humid tropics: Advancing tools and methods. Environ. Impact Assess. Rev. 2010, 30, 52–61. [Google Scholar] [CrossRef]
- Molnar, A.; Adam, B.; Antova, T.; Bosak, L.; Dimitrov, P.; Mileva, H.; Pekarcikova, J.; Zurlyte, I.; Gulis, G.; Ádány, R.; et al. Health impact assessment of Roma housing policies in Central and Eastern Europe: A comparative analysis. Environ. Impact Assess. Rev. 2012, 33, 7–14. [Google Scholar] [CrossRef]
- Hayajneh, W.A.; Daniels, V.J.; James, C.K.; Kanibir, M.N.; Pilsbury, M.; Marks, M.; Goveia, M.G.; Elbasha, E.H.; Dasbach, E.; Acosta, C.J. Public health impact and cost effectiveness of routine childhood vaccination for hepatitis a in Jordan: A dynamic model approach. BMC Infect. Dis. 2018, 18, 119. [Google Scholar] [CrossRef]
- Wallet, F.; Sicard, D.; Brey, P.; Lambrozo, J. Health impact of Dams: Lessons from a case study. Environ. Risques Sante 2016, 15, 419–425. [Google Scholar]
- Riojas-Rodríguez, H.; Álamo-Hernández, U.; Texcalac-Sangrador, J.L.; Romieu, I. Health impact assessment of decreases in PM10 and ozone concentrations in the Mexico City Metropolitan Area: A basis for a new air quality management program TT-Evaluación de impacto en salud ante reducciones de PM10 y ozono en la Zona Metropolitana de. Salud Publica Mex. 2014, 56, 579–591. [Google Scholar] [CrossRef] [PubMed]
- Hill, L.D.; Edwards, R.; Turner, J.R.; Argo, Y.D.; Olkhanud, P.B.; Odsuren, M.; Guttikunda, S.; Ochir, C.; Smith, K.R. Health assessment of future PM2.5 exposures from indoor, outdoor, and secondhand tobacco smoke concentrations under alternative policy pathways in Ulaanbaatar, Mongolia. PLoS ONE 2017, 12. [Google Scholar] [CrossRef] [PubMed]
- Bardach, A.E.; Caporale, J.E.; Alcaraz, A.; Augustovski, F.; Huayanay-Falconí, L.; Loza-Munarriz, C.; Hernández-Vásquez, A.; Pichon-Riviere, A. Burden of smoking-related disease and potential impact of cigarette price increase in Peru. Rev. Peru. Med. Exp. Salud. Publica 2016, 33, 651–661. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Zimmermann, R.; Qaim, M. Potential health benefits of Golden Rice: A Philippine case study. Food Policy 2004, 29, 147–168. [Google Scholar] [CrossRef]
- Sheffield, P.; Rowe, M.; Agu, D.; Rodriguez, L.; Aviles, K. Health impact assessments for environmental restoration: The case of Cano Martin Pena. Ann. Glob. Health 2014, 80, 296–302. [Google Scholar] [CrossRef] [PubMed]
- Semugoma, P.; Beyrer, C.; Baral, S. Assessing the effects of anti-homosexuality legislation in Uganda on HIV prevention, treatment, and care services. SAHARA J. 2012, 9, 173–176. [Google Scholar] [CrossRef] [PubMed]
- Konradsen, F.; Chimbari, M.; Furu, P.; Birley, M.H.; Christensen, N.Ø. The use of health impact assessments in water resources development: A case study from Zimbabwe. Impact Assess. 1997, 15, 55–72. [Google Scholar] [CrossRef][Green Version]
- Utzinger, J.; Wyss, K.; Moto, D.D.; Yemadji, N.; Tanner, M.; Singer, B.H. Assessing health impacts of the Chad-Cameroon petroleum development and pipeline project: Challenges and a way forward. Environ. Impact Assess. Rev. 2005, 25, 63–93. [Google Scholar] [CrossRef]
- Bell, M.L.; Davis, D.L.; Gouveia, N.; Borja-Aburto, V.H.; Cifuentes, L.A. The avoidable health effects of air pollution in three Latin American cities: Santiago, Sao Paulo, and Mexico City. Environ. Res. 2006, 100, 431–440. [Google Scholar] [CrossRef]
- Marseille, E.; Lohse, N.; Jiwani, A.; Hod, M.; Seshiah, V.; Yajnik, C.S.; Arora, G.P.; Henriksen, O.; Lieberman, N.; Chen, N.; et al. The cost-effectiveness of gestational diabetes screening including prevention of type 2 diabetes: Application of a new model in India and Israel. J. Matern. Fetal Neonatal Med. 2013, 26, 802–810. [Google Scholar] [CrossRef] [PubMed]
- Yorifuji, T.; Bae, S.; Kashima, S.; Tsuda, T.; Doi, H.; Honda, Y.; Kim, H.; Hong, Y.-C. Health Impact Assessment of PM10 and PM2.5 in 27 Southeast and East Asian Cities. J. Occup. Environ. Med. 2015, 57, 751–756. [Google Scholar] [CrossRef] [PubMed]
- Lacey, F.G.; Henze, D.K.; Lee, C.J.; van Donkelaar, A.; Martin, R.V. Transient climate and ambient health impacts due to national solid fuel cookstove emissions. Proc. Natl. Acad. Sci. USA 2017, 114, 1269–1274. [Google Scholar] [CrossRef] [PubMed]
- Bell, M.L.; Davis, D.; Cifuentes, L.; Cohen, A.; Gouveia, N.; Grant, L.; Green, C.; Johnson, T.; Rogat, J.; Spengler, J.; et al. International expert workshop on the analysis of the economic and public health impacts of air pollution: Workshop summary. Environ. Health Perspect. 2002, 110, 1163–1168. [Google Scholar] [CrossRef] [PubMed]
- Mochungong, P.I.K.; Gulis, G.; Sodemann, M. Clinical waste incinerators in Cameroon—A case study. Int. J. Health Care Qual. Assur. 2012, 25, 6–18. [Google Scholar] [CrossRef]
- Winkler, M.S.; Divall, M.J.; Krieger, G.R.; Balge, M.Z.; Singer, B.H.; Utzinger, J. Assessing health impacts in complex eco-epidemiological settings in the humid tropics: The centrality of scoping. Environ. Impact Assess. Rev. 2011, 31, 310–319. [Google Scholar] [CrossRef]
- Hengpraprom, S.; Bualert, S.; Sithisarankul, P. Testing a health impact assessment tool by assessing community opinion about a public park. Southeast Asian J. Trop. Med. Public Health 2012, 43, 236–242. [Google Scholar] [PubMed]
- Policies and Strategies to Promote Social Equity in Health. Available online: https://core.ac.uk/download/pdf/6472456.pdf (accessed on 5 June 2019).
- Fakhri, A.; Harris, P.; Maleki, M. Lessons learnt from developing a Health Impact Assessment guide in Iran. J. Public Health Policy 2016, 37, 440–452. [Google Scholar] [CrossRef] [PubMed]
- Guttikunda, S.K.; Begum, B.A.; Wadud, Z. Particulate pollution from brick kiln clusters in the Greater Dhaka region, Bangladesh. Air Qual. Atmos. Health 2013, 6, 357–365. [Google Scholar] [CrossRef]
- Abah, S.O. HIA practices in Nigeria. Impact Assess. Proj. Apprais. 2012, 30, 207–213. [Google Scholar] [CrossRef]
- Winkler, M.S.; Divall, M.J.; Krieger, G.R.; Schmidlin, S.; Magassouba, M.L.; Knoblauch, A.M.; Singer, B.H.; Utzinger, J. Assessing health impacts in complex eco-epidemiological settings in the humid tropics: Modular baseline health surveys. Environ. Impact Assess. Rev. 2012, 33, 15–22. [Google Scholar] [CrossRef]
- Chanchitpricha, C. Effectiveness of Health Impact Assessment (HIA) in Thailand: A case study of a Potash mine HIA in Udon Thani, Thailand. Ph.D. Thesis, University of East Anglia, Norwich, UK, June 2012. [Google Scholar]
- Joffe, M.; Mindell, J. A framework for the evidence base to support Health Impact Assessment. J. Epidemiol. Community Health 2002, 56, 132–138. [Google Scholar] [CrossRef] [PubMed]
- Benaissa, F.; Maesano, C.N.; Alkama, R.; Annesi-Maesano, I. Short-Term Health Impact Assessment of Urban PM10 in Bejaia City (Algeria). Can. Respir. J. 2016. [Google Scholar] [CrossRef] [PubMed]
- Jones, S.; Tefe, M.; Zephaniah, S.; Tedla, E.; Appiah-Opoku, S.; Walsh, J. Public transport and health outcomes in rural sub-Saharan Africa—A synthesis of professional opinion. J. Transp. Health 2016, 3, 211–219. [Google Scholar] [CrossRef]
- Schuchter, J.; Bhatia, R.; Corburn, J.; Seto, E. Health impact assessment in the United States: Has practice followed standards? Environ. Impact Assess. Rev. 2014, 47, 47–53. [Google Scholar] [CrossRef]
- Harris-Roxas, B.; Harris, E. The impact and effectiveness of health impact assessment: A conceptual framework. Environ. Impact Assess. Rev. 2013, 42, 51–59. [Google Scholar] [CrossRef]
- Nieuwenhuijsen, M.J.; Khreis, H.; Verlinghieri, E.; Mueller, N.; Rojas-Rueda, D. Participatory quantitative health impact assessment of urban and transport planning in cities: A review and research needs. Environ. Int. 2017, 103, 61–72. [Google Scholar] [CrossRef]
- Molnar, A.; Adany, R.; Adam, B.; Gulis, G.; Kosa, K. Health impact assessment and evaluation of a Roma housing project in Hungary. Health Place 2010, 16, 1240–1247. [Google Scholar] [CrossRef]
- de Blasio, A.; Giran, J.; Nagy, Z. Potentials of health impact assessment as a local health policy supporting tool. Perspect. Public Health 2012, 132, 216–220. [Google Scholar] [CrossRef]
- Harris, P.; Sainsbury, P.; Kemp, L. The fit between health impact assessment and public policy: Practice meets theory. Soc. Sci. Med. 2014, 108, 46–53. [Google Scholar] [CrossRef]
- Harris, P.J.; Kemp, L.A.; Sainsbury, P. The essntial elements of health impact assessment and healthy public policy: A qualitative study of practitioner perspectives. BMJ Open 2012, 2. [Google Scholar] [CrossRef] [PubMed]
- Cole, B.L.; Shimkhada, R.; Fielding, J.E.; Kominski, G.; Morgenstern, H. Methodologies for realizing the potential of health impact assessment. Am. J. Prev. Med. 2005, 28, 382–389. [Google Scholar] [CrossRef] [PubMed]
- Metzger, W.G.; Giron, A.M.; Vivas-Martinez, S.; Gonzalez, J.; Charrasco, A.J.; Mordmuller, B.G.; Magris, M. A rapid malaria appraisal in the Venezuelan Amazon. Malar. J. 2009, 8, 291. [Google Scholar] [CrossRef] [PubMed]
- Dua, B.; Acharya, A.S. Health impact assessment: Need and future scope in India. Indian J. Community Med. 2014, 39, 76–81. [Google Scholar] [PubMed]
- Kemm, J. The future challenges for HIA. Environ. Impact Assess. Rev. 2005, 25, 799–807. [Google Scholar] [CrossRef]
- Forsyth, A.; Slotterback, C.S.; Krizek, K.J. Health impact assessment in planning: Development of the design for health HIA tools. Environ. Impact Assess. Rev. 2010, 30, 42–51. [Google Scholar] [CrossRef]
- Atkinson, P.; Cooke, A. Developing a framework to assess costs and benefits of health impact assessment. Environ. Impact Assess. Rev. 2005, 25, 791–798. [Google Scholar] [CrossRef]
- Harris-Roxas, B.; Harris, E. Differing forms, differing purposes: A typology of health impact assessment. Environ. Impact Assess. Rev. 2011, 31, 396–403. [Google Scholar] [CrossRef]
- Utzinger, J.; Wyss, K.; Moto, D.D.; Tanner, M.; Singer, B.H. Community health outreach program of the Chad-Cameroon petroleum development and pipeline project. Clin. Occup. Environ. Med. 2004, 4, 9–26. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Question No. | Criteria | Associated Factors | Description |
|---|---|---|---|
| 1 | Accessed baseline local data | 1.1. Use of existing database 1.2. Primary data collection | Yes or no Yes or no |
| 2 | Reported resources used | 2.1. Human 2.2. Time 2.3. Money | Yes or no Yes or no Yes or no |
| 3 | Based on participatory approaches | 3.1. Stage of participation activity 3.2. Participant profile described | Screening, scoping, etc. Yes or no |
| 1 | Considered multiple outcomes | 4.1. Multiple outcomes 4.2. Coverage per outcome | Yes or no By mortality, morbidity, cost, social outcomes |
| 4 | Provided recommendation | 5.1. Format 5.2. Timing of delivery | Brief, separate section Early, mid and later stages |
| 5 | Fostered cross-national collaboration | 6.1. Shared authorship (local & foreign) 6.2. Local affiliation of first author | Yes or no Yes or no |
| Single-Country Location | Number of HIAs | Reference |
| China | 15 | [56,57,58,59,60,61,62,63,64,65,66,67,68,69,70] |
| Thailand | 4 | [71,72,73,74] |
| Brazil | 4 | [75,76,77,78] |
| India | 3 | [79,80,81] |
| Iran | 3 | [82,83,84] |
| Turkey | 3 | [85,86,87] |
| Algeria | 2 | [88,89] |
| Kenya | 2 | [90,91] |
| Bangladesh | 1 | [92] |
| Cameroon | 1 | [93] |
| Cuba | 1 | [94] |
| Congo | 1 | [95] |
| Hungary | 1 | [96] |
| Jordan | 1 | [97] |
| Laos | 1 | [98] |
| Mexico | 1 | [99] |
| Mongolia | 1 | [100] |
| Peru | 1 | [101] |
| Philippines | 1 | [102] |
| Puerto Rico | 1 | [103] |
| Uganda | 1 | [104] |
| Zimbabwe | 1 | [105] |
| Multi-Country Location | Number of HIAs | Reference |
| Cameroon-Chad | 2 | [23,106] |
| Chile-Brazil-Mexico | 1 | [107] |
| Israel-India | 1 | [108] |
| Lithuania-Slovakia-Hungary-Bulgaria | 1 | [96] |
| Korea-Singapore-Viet Nam | 1 | [109] |
| 101 countries across the globe | 1 | [110] |
| HIA TOPIC | Asia | Africa | Europe/Middle East | Americas |
|---|---|---|---|---|
| Air Pollution (AP) | 15 | 2 | 4 | 4 |
| Construction | 1 | - | - | - |
| Development Project | 1 | 5 | - | 1 |
| Diabetes | 1 | - | 1 | - |
| Excreta management | 1 | - | - | - |
| Golden rice | 1 | - | - | - |
| Public & Green space | 1 | - | - | - |
| Urban Transport Planning | 3 | - | 1 | 1 |
| Vaccination | 1 | - | 1 | - |
| Homosexuality Bill | - | 1 | - | - |
| Infectious Diseases | - | 1 | - | - |
| Clinical Waste | - | 1 | - | - |
| Housing | - | - | 2 | - |
| Salt consumption | - | - | 1 | - |
| Cigarette smoking | - | - | - | 2 |
| Investment program | - | - | - | 1 |
| Total number of studies | 25 | 10 | 10 | 9 |
| Country | Air Pollution | Development Projects | Urban Transport Planning |
|---|---|---|---|
| Algeria | 2 | ||
| Bangladesh | 1 | ||
| China | 11 | 1 | |
| India | 1 | 1 | 1 |
| Mongolia | 1 | ||
| Thailand | 2 | ||
| Iran | 2 | 1 | |
| Turkey | 2 | 1 | |
| Brazil | 2 | 1 | |
| Chile-Brazil-Mexico | 1 | ||
| Mexico | 1 | ||
| Chad-Cameroon | 2 | ||
| Zimbabwe | 1 | ||
| Kenya | 1 | ||
| Puerto Rico | 1 | ||
| Laos | 1 | ||
| Democratic Republic of Congo | 1 |
| Process Evaluation Criteria | No. of Studies | Associated Factors | No. of Studies |
|---|---|---|---|
| Accessed baseline local data | 57 | Use of existing databases Primary data collection | 43 14 |
| Reported resources used | 0 | Open access to publication Reporting on HIA stages | 40 17 |
| Based on participatory approaches | 7 | Participatory stage Stakeholder profile | 6 7 |
| Considered multiple outcomes | 53 | Mortality outcomes Morbidity outcomes Social determinant outcomes Cost outcomes | 33 43 11 17 |
| Provided recommendation | 35 | Brief (as part of conclusion) Separate sections Data timing of delivery | 29 6 7 |
| Fostered cross-national collaboration | 35 | Local affiliation of first author | 27 |
| No. Studies/No. of Countries | Mortality | Morbidity | SDH 1 | Costs | Mortality Morbidity | Mortality Morbidity SDH | Mortality Morbidity SDH Costs |
|---|---|---|---|---|---|---|---|
| No. Studies | 33 | 44 | 11 | 17 | 24 | 3 | 1 |
| No. of Countries | 15 | 25 | 13 | 11 | 12 | 3 | 1 |
| Stage | Prediction | Participation | Decision-Making | Resources |
|---|---|---|---|---|
| Screening | Clarify the issue at stake jointly with all parties Define the expected outcomes of HIA jointly with all parties | Conduct thorough stakeholder mapping Plan outreach strategy to stakeholders | Define the role of decision-makers in pushing HIA forward | Report on the costs of screening activities |
| Scoping | Define topic/sector of interest Scope for regions with similar features Identify local data sources and routinely collected data system Design HIA framework based on data type available and accessible data management technology | Approach institutions and individuals having access to adequate datasets | Define the decision makers agenda Fit the recommendations into adequate political timelines | Report on the costs of scoping activities |
| Appraisal | Adapt study area, indicators, and outcomes to increase validity and sensitivity of results | Report on technical working groups and workshops | Check whether involvement of decision-makers led to bias | Report on the costs needed to access the information needed |
| Dissemination | Craft clear and actionable recommendations | Deliver timely and compelling messages to appropriate audiences | Use multiple dissemination methods to access decision-makers | Report on the costs of activating dissemination process |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Thondoo, M.; Rojas-Rueda, D.; Gupta, J.; de Vries, D.H.; Nieuwenhuijsen, M.J. Systematic Literature Review of Health Impact Assessments in Low and Middle-Income Countries. Int. J. Environ. Res. Public Health 2019, 16, 2018. https://doi.org/10.3390/ijerph16112018
Thondoo M, Rojas-Rueda D, Gupta J, de Vries DH, Nieuwenhuijsen MJ. Systematic Literature Review of Health Impact Assessments in Low and Middle-Income Countries. International Journal of Environmental Research and Public Health. 2019; 16(11):2018. https://doi.org/10.3390/ijerph16112018
Chicago/Turabian StyleThondoo, Meelan, David Rojas-Rueda, Joyeeta Gupta, Daniel H. de Vries, and Mark J. Nieuwenhuijsen. 2019. "Systematic Literature Review of Health Impact Assessments in Low and Middle-Income Countries" International Journal of Environmental Research and Public Health 16, no. 11: 2018. https://doi.org/10.3390/ijerph16112018
APA StyleThondoo, M., Rojas-Rueda, D., Gupta, J., de Vries, D. H., & Nieuwenhuijsen, M. J. (2019). Systematic Literature Review of Health Impact Assessments in Low and Middle-Income Countries. International Journal of Environmental Research and Public Health, 16(11), 2018. https://doi.org/10.3390/ijerph16112018