Peripheral Neuropathy in Patients Recovering from Severe COVID-19: A Case Series

 ,
,  , ,
, , 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Main Study Procedures
2.2. Electrophysiological Examination
2.3. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Jin, Y.; Yang, H.; Ji, W.; Wu, W.; Chen, S.; Zhang, W.; Duan, G. Virology, Epidemiology, Pathogenesis, and Control of COVID-19. Viruses 2020, 12, 372. [Google Scholar] [CrossRef] [Green Version]
- Ambrosino, P.; Molino, A.; Calcaterra, I.; Formisano, R.; Stufano, S.; Spedicato, G.A.; Motta, A.; Papa, A.; Di Minno, M.N.D.; Maniscalco, M. Clinical Assessment of Endothelial Function in Convalescent COVID-19 Patients Undergoing Multidisciplinary Pulmonary Rehabilitation. Biomedicines 2021, 9, 614. [Google Scholar] [CrossRef]
- Carfi, A.; Bernabei, R.; Landi, F. Persistent Symptoms in Patients After Acute COVID-19. JAMA 2020, 324, 603–605. [Google Scholar] [CrossRef]
- Ambrosino, P.; Papa, A.; Maniscalco, M.; Di Minno, M.N.D. COVID-19 and functional disability: Current insights and rehabilitation strategies. Postgrad. Med. J. 2021, 97, 469–470. [Google Scholar] [CrossRef]
- Moriguchi, T.; Harii, N.; Goto, J.; Harada, D.; Sugawara, H.; Takamino, J.; Ueno, M.; Sakata, H.; Kondo, K.; Myose, N.; et al. A first case of meningitis/encephalitis associated with SARS-Coronavirus-2. Int. J. Infect. Dis. 2020, 94, 55–58. [Google Scholar] [CrossRef]
- Mao, L.; Jin, H.; Wang, M.; Hu, Y.; Chen, S.; He, Q.; Chang, J.; Hong, C.; Zhou, Y.; Wang, D.; et al. Neurologic Manifestations of Hospitalized Patients With Coronavirus Disease 2019 in Wuhan, China. JAMA Neurol. 2020, 77, 683–690. [Google Scholar] [CrossRef] [Green Version]
- Varatharaj, A.; Thomas, N.; Ellul, M.A.; Davies, N.W.S.; Pollak, T.A.; Tenorio, E.L.; Sultan, M.; Easton, A.; Breen, G.; Zandi, M.; et al. Neurological and neuropsychiatric complications of COVID-19 in 153 patients: A UK-wide surveillance study. Lancet Psychiatry 2020, 7, 875–882. [Google Scholar] [CrossRef]
- Helms, J.; Kremer, S.; Merdji, H.; Clere-Jehl, R.; Schenck, M.; Kummerlen, C.; Collange, O.; Boulay, C.; Fafi-Kremer, S.; Ohana, M.; et al. Neurologic Features in Severe SARS-CoV-2 Infection. N. Engl. J. Med. 2020, 382, 2268–2270. [Google Scholar] [CrossRef]
- Ftiha, F.; Shalom, M.; Jradeh, H. Neurological symptoms due to Coronavirus disease 2019. Neurol. Int. 2020, 12, 8639. [Google Scholar] [CrossRef]
- Chan, K.H.; Farouji, I.; Abu Hanoud, A.; Slim, J. Weakness and elevated creatinine kinase as the initial presentation of coronavirus disease 2019 (COVID-19). Am. J. Emerg. Med. 2020, 38, 1548.e1–1548.e3. [Google Scholar] [CrossRef]
- Orsucci, D.; Trezzi, M.; Anichini, R.; Blanc, P.; Barontini, L.; Biagini, C.; Capitanini, A.; Comeglio, M.; Corsini, P.; Gemignani, F.; et al. Increased Creatine Kinase May Predict A Worse COVID-19 Outcome. J. Clin. Med. 2021, 10, 1734. [Google Scholar] [CrossRef]
- Malik, G.R.; Wolfe, A.R.; Soriano, R.; Rydberg, L.; Wolfe, L.F.; Deshmukh, S.; Ko, J.H.; Nussbaum, R.P.; Dreyer, S.D.; Jayabalan, P.; et al. Injury-prone: Peripheral nerve injuries associated with prone positioning for COVID-19-related acute respiratory distress syndrome. Br. J. Anaesth. 2020, 125, e478–e480. [Google Scholar] [CrossRef]
- Frithiof, R.; Rostami, E.; Kumlien, E.; Virhammar, J.; Fallmar, D.; Hultstrom, M.; Lipcsey, M.; Ashton, N.; Blennow, K.; Zetterberg, H.; et al. Critical illness polyneuropathy, myopathy and neuronal biomarkers in COVID-19 patients: A prospective study. Clin. Neurophysiol. 2021, 132, 1733–1740. [Google Scholar] [CrossRef]
- Guerrero, J.I.; Barragan, L.A.; Martinez, J.D.; Montoya, J.P.; Pena, A.; Sobrino, F.E.; Tovar-Spinoza, Z.; Ghotme, K.A. Central and peripheral nervous system involvement by COVID-19: A systematic review of the pathophysiology, clinical manifestations, neuropathology, neuroimaging, electrophysiology, and cerebrospinal fluid findings. BMC Infect. Dis. 2021, 21, 515. [Google Scholar] [CrossRef]
- Needham, E.; Newcombe, V.; Michell, A.; Thornton, R.; Grainger, A.; Anwar, F.; Warburton, E.; Menon, D.; Trivedi, M.; Sawcer, S. Mononeuritis multiplex: An unexpectedly frequent feature of severe COVID-19. J. Neurol. 2021, 268, 2685–2689. [Google Scholar] [CrossRef]
- Vandenbroucke, J.P.; von Elm, E.; Altman, D.G.; Gotzsche, P.C.; Mulrow, C.D.; Pocock, S.J.; Poole, C.; Schlesselman, J.J.; Egger, M.; STROBE Initiative. Strengthening the Reporting of Observational Studies in Epidemiology (STROBE): Explanation and elaboration. Ann. Intern. Med. 2007, 147, W163–W194. [Google Scholar] [CrossRef] [Green Version]
- Graham, B.L.; Steenbruggen, I.; Miller, M.R.; Barjaktarevic, I.Z.; Cooper, B.G.; Hall, G.L.; Hallstrand, T.S.; Kaminsky, D.A.; McCarthy, K.; McCormack, M.C.; et al. Standardization of Spirometry 2019 Update. An Official American Thoracic Society and European Respiratory Society Technical Statement. Am. J. Respir. Crit. Care Med. 2019, 200, e70–e88. [Google Scholar] [CrossRef]
- Graham, B.L.; Brusasco, V.; Burgos, F.; Cooper, B.G.; Jensen, R.; Kendrick, A.; MacIntyre, N.R.; Thompson, B.R.; Wanger, J. Executive Summary: 2017 ERS/ATS standards for single-breath carbon monoxide uptake in the lung. Eur. Respir. J. 2017, 49, 16E0016. [Google Scholar] [CrossRef] [Green Version]
- Holland, A.E.; Spruit, M.A.; Troosters, T.; Puhan, M.A.; Pepin, V.; Saey, D.; McCormack, M.C.; Carlin, B.W.; Sciurba, F.C.; Pitta, F.; et al. An official European Respiratory Society/American Thoracic Society technical standard: Field walking tests in chronic respiratory disease. Eur. Respir. J. 2014, 44, 1428–1446. [Google Scholar] [CrossRef]
- Mahler, D.A.; Horowitz, M.B. Perception of breathlessness during exercise in patients with respiratory disease. Med. Sci. Sports Exerc. 1994, 26, 1078–1081. [Google Scholar] [CrossRef]
- Delorme, C.; Houot, M.; Rosso, C.; Carvalho, S.; Nedelec, T.; Maatoug, R.; Pitron, V.; Gassama, S.; Sambin, S.; Bombois, S.; et al. The wide spectrum of COVID-19 neuropsychiatric complications within a multidisciplinary centre. Brain Commun. 2021, 3, fcab135. [Google Scholar] [CrossRef]
- Rifino, N.; Censori, B.; Agazzi, E.; Alimonti, D.; Bonito, V.; Camera, G.; Conti, M.Z.; Foresti, C.; Frigeni, B.; Gerevini, S.; et al. Neurologic manifestations in 1760 COVID-19 patients admitted to Papa Giovanni XXIII Hospital, Bergamo, Italy. J. Neurol. 2021, 268, 2331–2338. [Google Scholar] [CrossRef]
- Saif, A.; Pick, A. Polyneuropathy following COVID-19 infection: The rehabilitation approach. BMJ Case Rep. 2021, 14, e242330. [Google Scholar] [CrossRef]
- Toscano, G.; Palmerini, F.; Ravaglia, S.; Ruiz, L.; Invernizzi, P.; Cuzzoni, M.G.; Franciotta, D.; Baldanti, F.; Daturi, R.; Postorino, P.; et al. Guillain-Barre Syndrome Associated with SARS-CoV-2. N. Engl. J. Med. 2020, 382, 2574–2576. [Google Scholar] [CrossRef]
- Manganotti, P.; Bellavita, G.; Tommasini, V.; D’Acunto, L.; Fabris, M.; Cecotti, L.; Furlanis, G.; Sartori, A.; Bonzi, L.; Buoite Stella, A.; et al. Cerebrospinal fluid and serum interleukins 6 and 8 during the acute and recovery phase in COVID-19 neuropathy patients. J. Med. Virol. 2021, 93, 5432–5437. [Google Scholar] [CrossRef]
- Carberry, N.; Badu, H.; Ulane, C.M.; Beckley, A.; Rosenberg, S.J.; Brenner, K.; Brannagan, T.H., III. Mononeuropathy Multiplex After COVID-19. J. Clin. Neuromuscul. Dis. 2021, 23, 24–30. [Google Scholar] [CrossRef]
- Daia, C.; Scheau, C.; Neagu, G.; Andone, I.; Spanu, A.; Popescu, C.; Stoica, S.I.; Verenca, M.C.; Onose, G. Nerve conduction study and electromyography findings in patients recovering from Covid-19-Case report. Int. J. Infect. Dis. 2021, 103, 420–422. [Google Scholar] [CrossRef]
- Gholami, M.; Safari, S.; Ulloa, L.; Motaghinejad, M. Neuropathies and neurological dysfunction induced by coronaviruses. J. Neurovirol. 2021, 27, 380–396. [Google Scholar] [CrossRef]
- Romero-Sanchez, C.M.; Diaz-Maroto, I.; Fernandez-Diaz, E.; Sanchez-Larsen, A.; Layos-Romero, A.; Garcia-Garcia, J.; Gonzalez, E.; Redondo-Penas, I.; Perona-Moratalla, A.B.; Del Valle-Perez, J.A.; et al. Neurologic manifestations in hospitalized patients with COVID-19: The ALBACOVID registry. Neurology 2020, 95, e1060–e1070. [Google Scholar] [CrossRef]
- Studart-Neto, A.; Guedes, B.F.; Tuma, R.L.E.; Camelo Filho, A.E.; Kubota, G.T.; Iepsen, B.D.; Moreira, G.P.; Rodrigues, J.C.; Ferrari, M.M.H.; Carra, R.B.; et al. Neurological consultations and diagnoses in a large, dedicated COVID-19 university hospital. Arq. Neuropsiquiatr. 2020, 78, 494–500. [Google Scholar] [CrossRef]
- Franz, C.K.; Murthy, N.K.; Malik, G.R.; Kwak, J.W.; D’Andrea, D.; Wolfe, A.R.; Farr, E.; Stearns, M.A.; Deshmukh, S.; Tavee, J.O.; et al. Acquired peripheral nerve injuries associated with severe COVID-1. medRxiv 2021. [Google Scholar] [CrossRef]
- Latronico, N.; Bolton, C.F. Critical illness polyneuropathy and myopathy: A major cause of muscle weakness and paralysis. Lancet Neurol. 2011, 10, 931–941. [Google Scholar] [CrossRef]
- De Jonghe, B.; Sharshar, T.; Lefaucheur, J.P.; Authier, F.J.; Durand-Zaleski, I.; Boussarsar, M.; Cerf, C.; Renaud, E.; Mesrati, F.; Carlet, J.; et al. Paresis acquired in the intensive care unit: A prospective multicenter study. JAMA 2002, 288, 2859–2867. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Suh, J.; Mukerji, S.S.; Collens, S.I.; Padera, R.F., Jr.; Pinkus, G.S.; Amato, A.A.; Solomon, I.H. Skeletal Muscle and Peripheral Nerve Histopathology in COVID-19. Neurology 2021, 97, e849–e858. [Google Scholar] [CrossRef] [PubMed]
- Lucchese, G.; Floel, A. SARS-CoV-2 and Guillain-Barre syndrome: Molecular mimicry with human heat shock proteins as potential pathogenic mechanism. Cell Stress Chaperones 2020, 25, 731–735. [Google Scholar] [CrossRef]
- Keddie, S.; Pakpoor, J.; Mousele, C.; Pipis, M.; Machado, P.M.; Foster, M.; Record, C.J.; Keh, R.Y.S.; Fehmi, J.; Paterson, R.W.; et al. Epidemiological and cohort study finds no association between COVID-19 and Guillain-Barre syndrome. Brain 2021, 144, 682–693. [Google Scholar] [CrossRef]
- Natoli, S.; Oliveira, V.; Calabresi, P.; Maia, L.F.; Pisani, A. Does SARS-Cov-2 invade the brain? Translational lessons from animal models. Eur. J. Neurol. 2020, 27, 1764–1773. [Google Scholar] [CrossRef]
- Kayacan, O.; Beder, S.; Deda, G.; Karnak, D. Neurophysiological changes in COPD patients with chronic respiratory insufficiency. Acta Neurol. Belg. 2001, 101, 160–165. [Google Scholar]
- Ulubay, G.; Ulasli, S.S.; Bozbas, S.S.; Ozdemirel, T.; Karatas, M. Effects of peripheral neuropathy on exercise capacity and quality of life in patients with chronic obstructive pulmonary diseases. Arch. Med. Sci. 2012, 8, 296–302. [Google Scholar] [CrossRef]
- Paliwal, V.K.; Garg, R.K.; Gupta, A.; Tejan, N. Neuromuscular presentations in patients with COVID-19. Neurol. Sci. 2020, 41, 3039–3056. [Google Scholar] [CrossRef]


{kind=link}
| Clinical Variables | Total Sample n = 102 | Normal n = 59 | Mononeuropathy n = 18 | Polyneuropathy n = 25 |
|---|---|---|---|---|
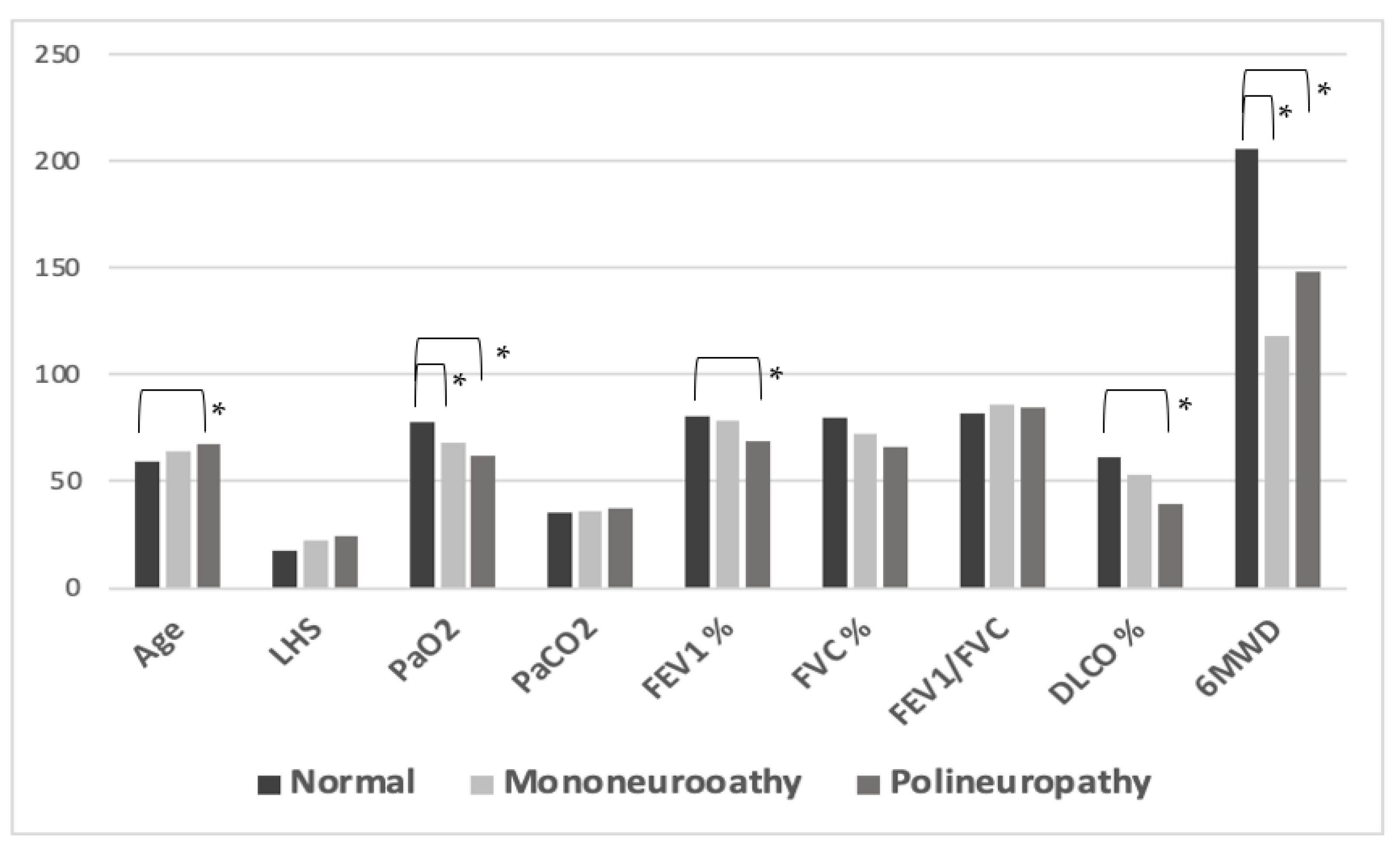
| Age, years | 62.5 (40–87) | 59 (40–80) | 62.5 (48–86) | 67 (52–87) |
| Males, n (%) | 84 (82.4) | 47 (79.7) | 15 (83.3) | 22 (88) |
| Hypertension, n (%) | 49 (48) | 26 (44.1) | 8 (44.4) | 15 (60) |
| Hypercholesterolemia, n (%) | 5 (5.9) | 1 (1.7) | 3 (16.7) | 2 (8) |
| History of cardiovascular events, n (%) | 12 (11.8) | 4 (6.8) | 3 (16.7) | 5 (20) |
| Obesity, n (%) | 24 (23.5) | 3 (5.1) | 9 (50) | 12 (48) |
| History of neurological events, n (%) | 9 (8.8) | 1 (1.7) | 4 (22.2) | 4 (16) |
| LHS (days) | 19 (0–68) | 18 (0–50) | 21 (0–48) | 24 (0–68) |
| WHO, class of severity III/IV (n) | 39/63 | 19/40 | 10/8 | 10/15 |
| Non invasive ventilation, n (%) | 30 (29.4) | 19 (32.2) | 4 (22.2) | 7 (28) |
| High flow oxygen therapy, n (%) | 26 (25.5) | 14 (23.7) | 7 (38.9) | 5 (20) |
| PaO2, mmHg | 71 (44–99) | 79 (49–99) | 66.7 (47–91) | 61.3 (44–80) |
| PaCO2, mmHg | 36 (25–46) | 36 (25–43) | 35.5 (29–43) | 37 (25–46) |
| FEV1, %predicted | 75 (34–114) | 79 (34–114) | 74.5 (54–104) | 64 (53–102) |
| FVC, %predicted | 76 (39–113) | 78 (39–113) | 69 (50–100) | 68.5 (44–86) |
| FEV1/FVC | 84 (40–100) | 83.5 (40–100) | 86 (79–91) | 85 (72–93) |
| DLCO, %predicted | 51.5 (20–110) | 57 (28–110) | 46 (25–99) | 32 (20–75) |
| 6MWD, metres | 208 (0–365) | 225 (0–365) | 75 (0–338) | 177 (30–210) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Balbi, P.; Saltalamacchia, A.; Lullo, F.; Fuschillo, S.; Ambrosino, P.; Moretta, P.; Lanzillo, B.; Maniscalco, M. Peripheral Neuropathy in Patients Recovering from Severe COVID-19: A Case Series. Medicina 2022, 58, 523. https://doi.org/10.3390/medicina58040523
Balbi P, Saltalamacchia A, Lullo F, Fuschillo S, Ambrosino P, Moretta P, Lanzillo B, Maniscalco M. Peripheral Neuropathy in Patients Recovering from Severe COVID-19: A Case Series. Medicina. 2022; 58(4):523. https://doi.org/10.3390/medicina58040523
Chicago/Turabian StyleBalbi, Pietro, Annamaria Saltalamacchia, Francesco Lullo, Salvatore Fuschillo, Pasquale Ambrosino, Pasquale Moretta, Bernardo Lanzillo, and Mauro Maniscalco. 2022. "Peripheral Neuropathy in Patients Recovering from Severe COVID-19: A Case Series" Medicina 58, no. 4: 523. https://doi.org/10.3390/medicina58040523
APA StyleBalbi, P., Saltalamacchia, A., Lullo, F., Fuschillo, S., Ambrosino, P., Moretta, P., Lanzillo, B., & Maniscalco, M. (2022). Peripheral Neuropathy in Patients Recovering from Severe COVID-19: A Case Series. Medicina, 58(4), 523. https://doi.org/10.3390/medicina58040523