Glut1 and Glut3 as Potential Prognostic Markers for Oral Squamous Cell Carcinoma

Abstract
:1. Introduction
2. Results and Discussion
2.1. Patients’ Clinical Data
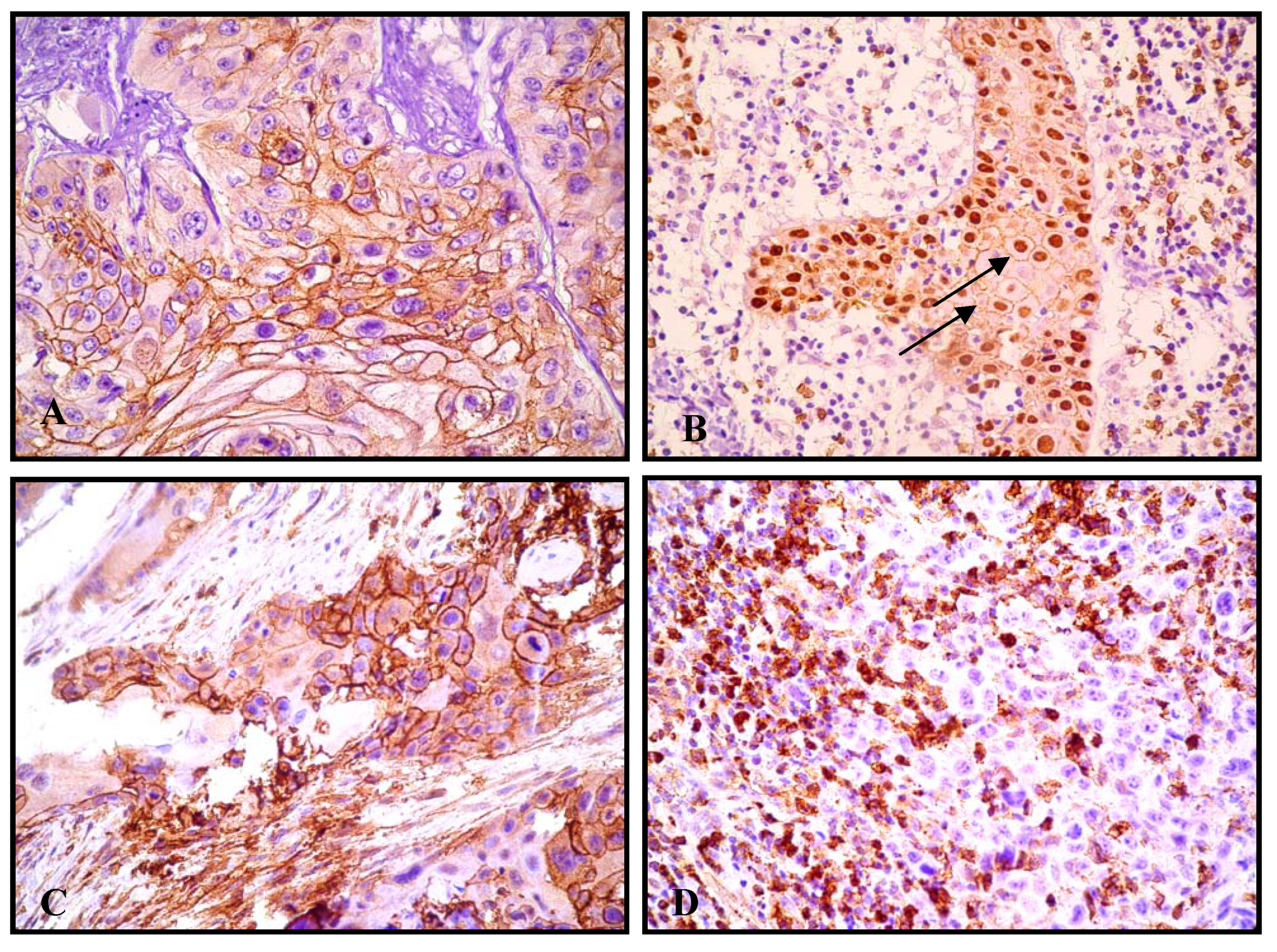
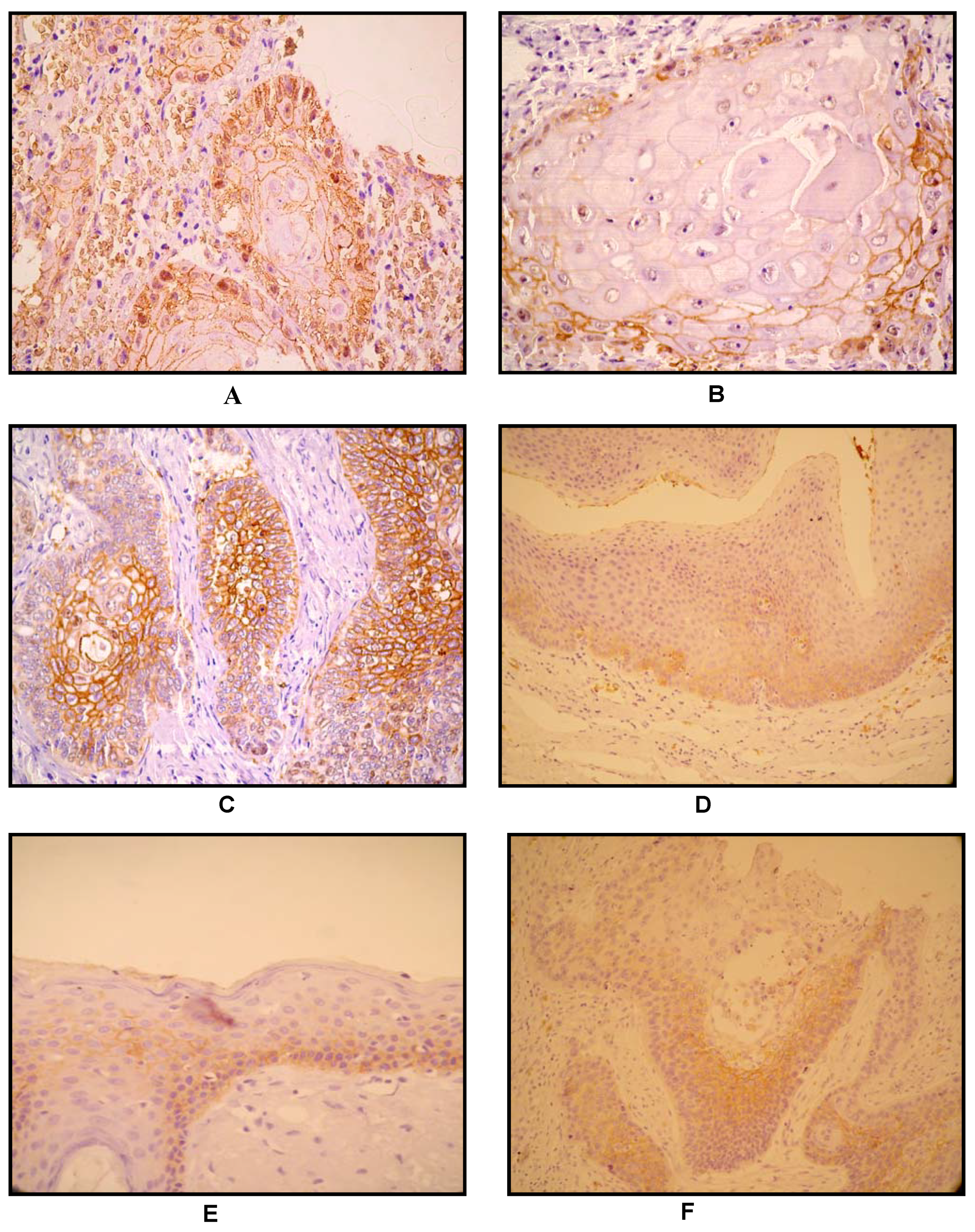
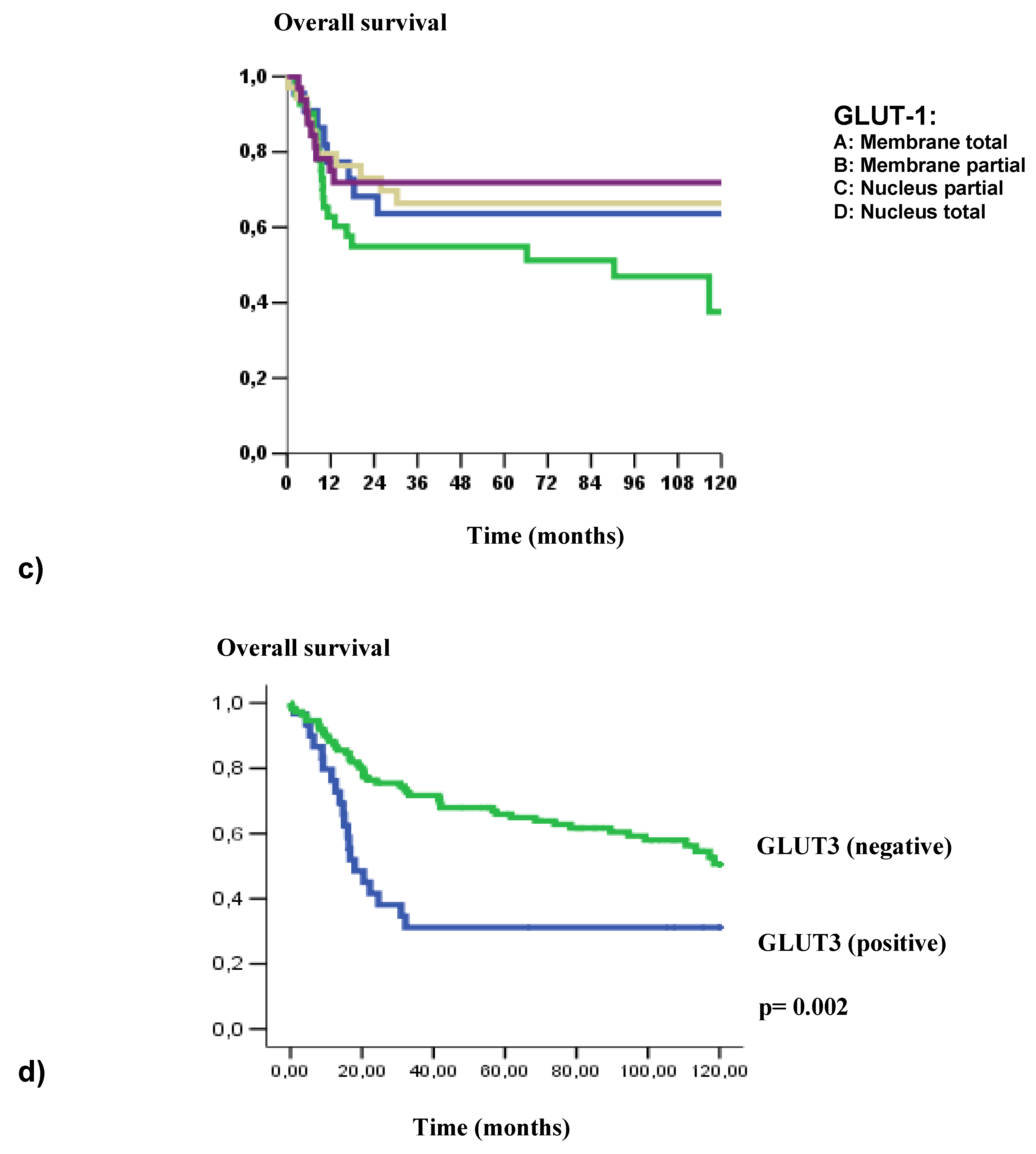
2.2. GLUT1 and GLUT3 Immunohistochemical Expression
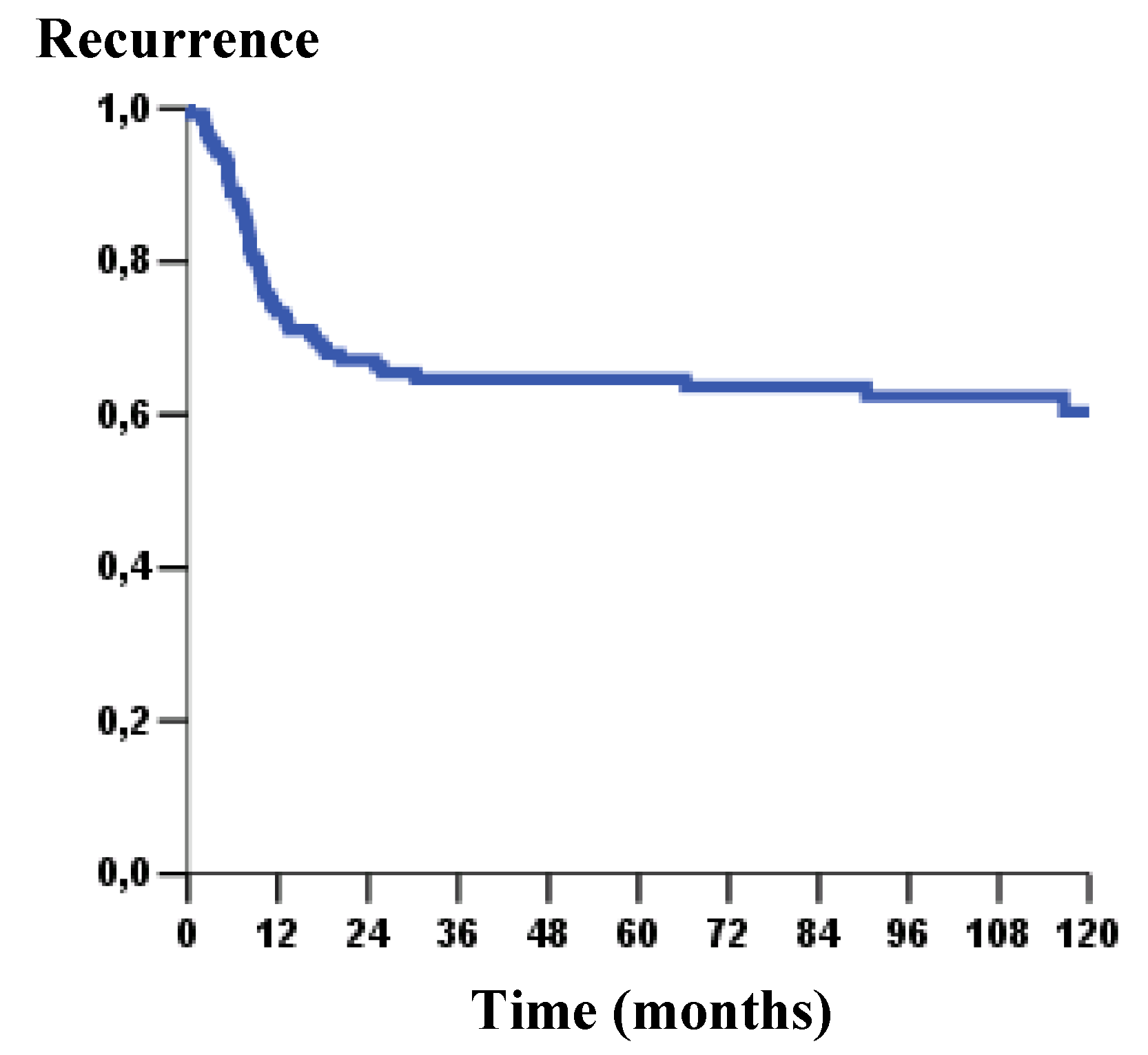
2.3. GLUT 1 and GLUT 3: Immunoexpression and Clinical-Pathological Parameters
3. Experimental
3.1. Patients
3.2. Tissue microarray construction (TMA)
3.3. Immunohistochemistry
3.4. Evaluation of stained sections: GLUT1 and GLUT3
3.5. Statistical analysis
4. Conclusions
Acknowledgements
References
- Kallinowski, F.; Schlenger, K.H.; Runkel, S.; Kloes, M.; Stohrer, M.; Okunieff, P.; Vaupel, P. Blood flow, metabolism, cellular microenvironment and growth rate of human tumor xenography. Cancer Res. 1989, 49, 3759–3764. [Google Scholar] [PubMed]
- Reisser, C.; Eichhorn, K.; Herold-Mende, C.; Born, A.I.; Bannasch, P. Expression of facilitative glucose transport proteins during development of squamous cell carcinomas of the head and neck. Int. J. Cancer 1999, 80, 194–198. [Google Scholar] [CrossRef]
- Haber, R.S.; Rathan, A.; Weiser, K.R.; Pritsker, A.; Itzkowitz, S.H.; Bodian, C.; Slater, G.; Weiss, A.; Burstein, D.E. GLUT 1 Glucose transporter Expression in colorectal carcinoma: a marker for poor prognosis. Cancer 1998, 17, 34–40. [Google Scholar] [CrossRef]
- Kunkel, M.; Reichert, T.E.; Benz, P.; Lehr, H.A.; Jeong, J.H.; Wieand, S.; Bartenstein, P.; Wagner, W.; Whiteside, T.L. Over expression of GLUT 1 and increased glucose metabolism in tumors are associated with a poor prognosis in patients with oral squamous cell carcinoma. Cancer 2003, 15, 1015–1024. [Google Scholar] [CrossRef] [PubMed]
- Baer, S.; Casaubon, L.; Schwartz, M.R.; Macrogliese, A.; Younes, M. GLUT 3 expression in biopsy specimens of laryngeal carcinoma is associated with poor survival. Laryngoscope 2002, 112, 393–396. [Google Scholar] [CrossRef] [PubMed]
- Airley, R.; Loncaster, J.; Davidson, S.; Bromley, M.; Roberts, S.; Patterson, A.; Hunter, R.; Stratford, I.; West, C. Glucose transporter GLUT 1 expression correlates with tumor hypoxia and predicts metastasis-free survival in advanced carcinoma of the cervix. Clin. Cancer Res. 2001, 7, 928–934. [Google Scholar] [PubMed]
- Burstein, D.E.; Nagi, C.; Kohtz, D.S.; Lumerman, H.; Wang, B.Y. Immunohistochemical detection of GLUT1, p63 and phosphorylated histone H1 in head and neck squamous intraepithelial neoplasia: evidence for aberrations in hypoxia-related, cell cycle-and stem – cell- regulatory pathways. Histopathology 2006, 48, 708–716. [Google Scholar] [CrossRef] [PubMed]
- Mochizuki, T.; Tsukamoto, E.; Kuge, Y.; Kanegae, K.; Zhao, S.; Hikosaka, K.; Hosokawa, M.; Kohanawa, M.; Tamaki, N. FDG uptake and glucose transporter subtype expressions in experimental tumor and inflammation models. J. Nucl. Med. 2001, 42, 1551–1555. [Google Scholar] [PubMed]
- Kato, H.; Takita, J.; Miyazaki, T.; Nakajima, M.; Fukai, Y.; Masuda, N.; Fukuchi, M.; Manda, R.; Ojima, H.; Tsukada, K.; Kuwano, H. GLUT 1 glucose transport expression in esophageal squamous cell carcinoma is associated with tumor aggressiveness. Anticancer Res. 2002, 22, 2635–2639. [Google Scholar] [PubMed]
- Mellanen, P.; Minn, H.; Grenman, R.; Harkonen, P. Expression of glucose transporters in head-and-neck tumors. Int. J. Cancer 1994, 56, 622–629. [Google Scholar] [CrossRef] [PubMed]
- Higashi, T.; Tamaki, N.; Honda, T.; Torizuka, T.; Kimura, T.; Inokuma, T.; Ohshio, G.; Hosotani, R.; Imamura, M.; Konishi, J. Expression of glucose transporters in human pancreatic tumors compared with increased FDG accumulation in PET study. J. Nucl. Med. 1997, 38, 1337–1344. [Google Scholar] [PubMed]
- Marom, E.M.; Aloia, T.A.; Moore, M.B.; Hara, M.; Herndon, J.E.; Harpole, D.H.; Goodman, P.C.; Patz, E.F. Correlation of FDG PET imaging with GLUT 1 and GLUT 3 expression in early-stage non-small cell lung cancer. Lung Cancer 2001, 33, 99–107. [Google Scholar] [CrossRef]
- Gjedde, A. Glucose metabolism. In Principles and Practice of Nuclear Medicine, 2th ed.; Wagner, H., Ed.; W B Saunders: Philadelphia, PA, USA, 1995; pp. 56–62. [Google Scholar]
- Oliver, R.J.; Woodwards, R.T.; Sloan, P.; Thakker, N.S.; Stratford, I.J.; Airley, R.E. Prognostic value of facilitative glucose transporter GLUT 1 in oral squamous cell carcinomas treated by surgical resection; results of EORTC Translational Research Fund studies. Eur. J. Cancer 2004, 40, 503–507. [Google Scholar] [CrossRef] [PubMed]
- Hermanek, P.; Sobin, L.H. (Eds.) UICC: TNM Classification of Malignant Tumors, 4th ed.; Springer: New York, NY, USA, 1987. [Google Scholar]
- Masanori, Y.; Naoki, O.; Hiroyuki, H.; Yoichi, K.; Yohei, M.; Tetsuji, I.; Yusuke, M.; Keiichi, T.; Takeo, M.; Osamura, R. Glucose transporter-1 expression in the thyroid gland: clinocopathological significance for papillary carcinoma. Oncol. Rep. 2005, 14, 1499–1504. [Google Scholar]
- Tohma, T.; Okazumi, S.; Makino, H.; Cho, A.; Mochizuki, R.; Shuto, K.; Kudo, H.; Matsubara, K.; Gunji, H.; Matsubara, H.; Ochiai, T. Over expression of glucose transporter 1 in esophageal squamous cell carcinomas: a marker for poor prognosis. Dis. Esophagus 2005, 18, 185–189. [Google Scholar] [CrossRef] [PubMed]
- Zhou, S.; Wang, S.; Wu, Q.; Fan, J.; Wang, Q. Expression of glucose transporter-1 and -3 in the head and neck carcinoma—the correlation of the expression with the biological behaviors. ORL J. Otorhinolaryngol. Relat. Spec. 2008, 70, 189–194. [Google Scholar] [CrossRef] [PubMed]
- Rocha, R.M.; Miller, K.; Soares, F.A.; Schenka, N.M.; Vassallo, J.; Gobbi, H. Biotin-free systems provide stronger immunohistochemical signal in oestrogen receptor evaluation of breast cancer. J. Clin. Pathol. 2009, 62, 699–704. [Google Scholar] [CrossRef] [PubMed]
Sample Availability: No samples are available. |







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Varible | Group | Cases (%) |
|---|---|---|
| Gender (n = 142) | Male Female | 112 (78.9) 30 (21.1) |
| Race (n = 142) | Caucasians Others | 122 (85.9) 20 (14.1) |
| Tabacco (n = 142) | No Light Moderate/Severe Ignored | 15 (10.6) 99 (69.7) 17 (12) 11 (7.7) |
| Alcohol (n = 142) | No Light Moderate/Severe Ignored | 27 (19.0) 89 (62.7) 15 (10.6) 11 (7.7) |
| Site (n = 142) | Tongue Gingiva Floor of the mouth Palate Jugal Retromolar | 54 (38) 20 (14.1) 42 (29.6) 1 (0.7) 6 (4.2) 19 (13.4) |
| Vascular Invision (n = 142) | No observed Yes Ignored | 75 (52.8) 53 (37.3) 14 (9.9) |
| Clinic Stage (n = 142) | I/II III/IV | 37 (26.1) 105 (73.9) |
| Recurrence (n = 142) | No Yes | 92 (64.8) 50 (35.2) |
| Site of Recurrence (n = 142) | Local Others Local/others No recurrence | 41 (28.8) 7 (4.9) 2 (1.4) 92 (64.8) |
| Status of last contact (n = 142) | Alive wth disease Alive wthout disease Death due to disease Death due to other causes Lost | 2 (1.4) 61 (43) 45 (31.7) 26 (18.3) 8 (5.6) |
| Variable (n = 135) | Category | GLUT-1/grouping | ||||
|---|---|---|---|---|---|---|
| M | MN/N OR N | p | ||||
| Gender | Male Female | 53(39.3) 15(11.1) | 54(40) 13(9.6) | 0.832 | ||
| Alcohol | No Light Moderate/severe | 14(11.3) 37(29.8) 11(8.9) | 11(8.9) 48(38.7) 3(2.4) | 0.042 | ||
| Staging | I/II III/IV | 19(14.1) 49(36.3) | 16(11.9) 51(37.8) | 0.695 | ||
| Vascular Embolization | No yes | 31(25.6) 29(24) | 38(31.4) 23(19) | 0.273 | ||
| Variable (n = 142) | Category | GLUT-3 | ||
|---|---|---|---|---|
| Positivo(%) | Negativo(%) | p | ||
| Gender | Male Female | 87(61.3) 25(17.6) | 25(17.6) 5(3.5) | 0.619 |
| Alcohol | No Light Moderate/severe | 3(2.3) 22(16.8) 3(2.3) | 24(18.3) 67(51.1) 12(9.2) | 0.316 |
| Tabacco | No Light Moderate/severe | 1(0.8) 24(18.3) 3(2.3) | 14(10.7) 75(57.3) 14(10.7) | 0.279 |
| Staging | I/II III/IV | 2(1,4) 28(19,7) | 35(24.6) 77(54.2) | 0.005 |
| Vascular Embolization | No yes | 10(7,8) 19(14,8) | 65(50.8) 34(26.6) | 0.005 |
| Variable | Category | HR (95% IC) | p valor |
|---|---|---|---|
| Vascular embolization | No | 1.0 (ref.) | |
| Yes | 2.165 (1.295–3.618) | 0.003 | |
| GLUT-1 | (group) | 1.0(ref.) | |
| GLUT-1/pattern | (group 1) | 2.066( 1.232–3.464) | 0.006 |
| GLUT-3 | Negative | 1.0 (ref.) | |
| Positive | 1.933(1.119–3.339) | 0.018 |
| Variable | Category | HR (95% IC) | p valor |
|---|---|---|---|
| staging | |||
| I/II | 1.0 (ref.) | ||
| III/IV | 3.304(1.407–7.762) | 0.006 |
© 2010 by the authors; licensee Molecular Diversity Preservation International, Basel, Switzerland. This article is an open-access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/3.0/).
Share and Cite
Ayala, F.R.R.; Rocha, R.M.; Carvalho, K.C.; Carvalho, A.L.; Da Cunha, I.W.; Lourenço, S.V.; Soares, F.A. Glut1 and Glut3 as Potential Prognostic Markers for Oral Squamous Cell Carcinoma. Molecules 2010, 15, 2374-2387. https://doi.org/10.3390/molecules15042374
Ayala FRR, Rocha RM, Carvalho KC, Carvalho AL, Da Cunha IW, Lourenço SV, Soares FA. Glut1 and Glut3 as Potential Prognostic Markers for Oral Squamous Cell Carcinoma. Molecules. 2010; 15(4):2374-2387. https://doi.org/10.3390/molecules15042374
Chicago/Turabian StyleAyala, Fernanda Rocha Rojas, Rafael Malagoli Rocha, Kátia Cândido Carvalho, André Lopes Carvalho, Isabela Werneck Da Cunha, Silvia Vanessa Lourenço, and Fernando Augusto Soares. 2010. "Glut1 and Glut3 as Potential Prognostic Markers for Oral Squamous Cell Carcinoma" Molecules 15, no. 4: 2374-2387. https://doi.org/10.3390/molecules15042374