Folate Intake and Methylenetetrahydrofolate Reductase Gene Polymorphisms as Predictive and Prognostic Biomarkers for Ovarian Cancer Risk

Abstract
:1. Introduction
2. Results and Discussion
2.1. Results
2.2. Discussion
3. Experimental Section
3.1. Study Subjects
3.2. Data Collection
3.3. Genotyping
3.4. Statistical Analysis
4. Conclusions
Acknowledgments
References
- Kristensen, G.B.; Trope, C. Epithelial ovarian carcinoma. Lancet 1997, 349, 113–117. [Google Scholar]
- Jin, F.; Shu, X.O.; Devesa, S.S.; Zheng, W.; Blot, W.J.; Gao, Y.T. Incidence trends for cancers of the breast, ovary, and corpus uteri in urban Shanghai, 1972–89. Cancer Causes Control 1993, 4, 355–360. [Google Scholar]
- La Vecchia, C. Epidemiology of ovarian cancer: A summary review. Eur. J. Cancer Prev 2001, 10, 125–129. [Google Scholar]
- Zhang, M.; Xie, X.; Lee, A.H.; Binns, C.W. Soy and isoflavone intake are associated with reduced risk of ovarian cancer in southeast China. Nutr. Cancer 2004, 49, 125–130. [Google Scholar]
- Aune, D.; Deneo-Pellegrini, H.; Ronco, A.L.; Boffetta, P.; Acosta, G.; Mendilaharsu, M.; de Stefani, E. Dietary folate intake and the risk of 11 types of cancer: A case-control study in Uruguay. Ann. Oncol 2010, 22, 444–451. [Google Scholar]
- Kim, Y.I. Will mandatory folic acid fortification prevent or promote cancer? Am. J. Clin. Nutr 2004, 80, 1123–1128. [Google Scholar]
- Larsson, S.C.; Giovannucci, E.; Wolk, A. Folate intake, MTHFR polymorphisms, and risk of esophageal, gastric, and pancreatic cancer: A meta-analysis. Gastroenterology 2006, 131, 1271–1283. [Google Scholar]
- Choi, S.W.; Mason, J.B. Folate and carcinogenesis: An integrated scheme. J. Nutr 2000, 13, 129–132. [Google Scholar]
- Gallus, S.; La Vecchia, C. Is there a link between diet and esophageal cancer? Nat. Clin. Pract. Gastroenterol. Hepatol 2007, 4, 2–3. [Google Scholar]
- Blount, B.C.; Mack, M.M.; Wehr, C.M.; MacGregor, J.T.; Hiatt, R.A.; Wang, G. Folate deficiency causes uracil misincorporation into human DNA and chromosome breakage: Implications for cancer and neuronal damage. Proc. Natl. Acad. Sci. USA 2007, 94, 3290–3295. [Google Scholar]
- Bailey, L.B.; Gregory, J.F., 3rd. Polymorphisms of methylenetetrahydrofolate reductase and other enzymes: Metabolic significance, risks and impact on folate requirement. J. Nutr. 1999, 129, 919–922. [Google Scholar]
- Frosst, P.; Blom, H.J.; Milos, R.; Goyette, P.; Sheppard, C.A.; Matthews, R.G.; Boers, G.J.; den Heijer, M.; Kluijtmans, L.A.; van den Heuvel, L.P.; et al. A candidate genetic risk factor for vascular disease: A commonmutation inmethylenetetrahydrofolate reductase. Nat. Genet 1995, 10, 111–113. [Google Scholar]
- Terry, K.L.; Tworoger, S.S.; Goode, E.L.; Gates, M.A.; Titus-Ernstoff, L.; Kelemen, L.E.; Sellers, T.A.; Hankinson, S.E.; Cramer, D.W. MTHFR polymorphisms in relation to ovarian cancer risk. Gynecol. Oncol 2010, 119, 319–324. [Google Scholar]
- Upadhyay, R.; Jain, M.; Kumar, S.; Ghoshal, U.C.; Mittal, B. Functional polymorphisms of cyclooxygenase-2 (COX-2) gene and risk for esophageal squamous cell carcinoma. Mutat. Res 2009, 663, 52–59. [Google Scholar]
- Upadhyay, R.; Jain, M.; Kumar, S.; Ghoshal, U.C.; Mittal, B. Association of interleukin-6 (−174G>C) promoter polymorphism with risk of squamous cell esophageal cancer and tumor location: An exploratory study. Clin. Immunol 2008, 128, 199–204. [Google Scholar]
- Jain, M.; Tilak, A.R.; Upadhyay, R.; Kumar, A.; Mittal, B. Microsomal epoxide hydrolase (EPHX1), slow (exon 3, 113His) and fast (exon 4, 139Arg) alleles confer susceptibility to squamous cell esophageal cancer. Toxicol. Appl. Pharmacol 2008, 230, 247–251. [Google Scholar]
- Wang, J.; Sasco, A.J.; Fu, C.; Xue, H.; Guo, G.; Hua, Z.; Zhou, Q.; Jiang, Q.; Xu, B. Aberrant DNA methylation of P16, MGMT, and hMLH1 genes in combination with MTHFR C677T genetic polymorphism in esophageal squamous cell carcinoma. Cancer Epidemiol. Biomark. Prev 2008, 17, 118–125. [Google Scholar]
- Mason, J.B. Folate, cancer risk, and the Greek god, Proteus: A tale of two chameleons. Nutr. Rev 2009, 67, 206–212. [Google Scholar]
- Webb, P.M.; Ibiebele, T.I.; Hughes, M.C.; Beesley, J.; van der Pols, J.C.; Chen, X.; Nagle, CM.; Bain, C.J.; Chenevix-Trench, G. Australian Cancer Study (Ovarian Cancer); Australian Ovarian Cancer Study Group. Folate and related micronutrients, folate-metabolising genes and risk of ovarian cancer. Eur. J. Clin. Nutr 2011, 65, 1133–1140. [Google Scholar]
- Harris, H.R.; Cramer, D.W.; Vitonis, A.F.; Depari, M.; Terry, K.L. Folate, vitamin B(6), vitamin B(12), methionine and alcohol intake in relation to ovarian cancer risk. Int. J. Cancer 2011, 22. [Google Scholar] [CrossRef]
- Ito, H.; Shinoda, M.; Hatooka, S.; Hirose, K.; Wakai, K.; Saito, T.; Wakai, K.; Saito, T.; Suzuki, T.; Maeda, T.; et al. Gene-environment interactions between alcohol drinking and the MTHFR C677T polymorphism impact on esophageal cancer risk: Results of a case-control study in Japan. Carcinogenesis 2005, 26, 1285–1290. [Google Scholar]
- Wang, Y.; Guo, W.; He, Y.; Chen, Z.; Wen, D.; Zhang, X.; Wang, N.; Li, Y.; Ge, H.; Zhang, J. Association of MTHFR C677T and SHMT(1) C1420T with susceptibility to ESCC and GCA in a high incident region of Northern China. Cancer Causes Control 2007, 18, 143–152. [Google Scholar]
- Goode, E.L.; Maurer, M.J.; Sellers, T.A.; Phelan, C.M.; Kalli, K.R.; Fridley, B.L.; Vierkant, R.A.; Armasu, S.M.; White, K.L.; Keeney, G.L.; et al. Inherited determinants of ovarian cancer survival. Clin. Cancer Res 2010, 16, 995–1007. [Google Scholar]
- Jakubowska, A.; Gronwald, J.; Menkiszak, J.; Górski, B.; Huzarski, T.; Byrski, T.; Edler, L.; Lubiński, J.; Scott, R.J.; Hamann, U. Methylenetetrahydrofolate reductase polymorphisms modify BRCA1-associated breast and ovarian cancer risks. Breast Cancer Res. Treat 2007, 104, 299–308. [Google Scholar]
- Zhang, Z.G.; Rustum, Y.M. Pharmacologic rationale for fluoropyrimidine-leucovorin combination: Biochemical mechanisms. Semin. Oncol 1992, 19, 46–50. [Google Scholar]
- Carlsson, G.; Hafström, L.O.; Spears, C.P.; Gustavsson, B.; Larsson, P.A. 5-fluorouracil (5-FU) and 5, 10-methylene tetrahydrofolate (5, 10-CH2FH4) as adjuvant therapy in an experimental rodent colon carcinoma model. Anticancer Res 1997, 17, 3671–3674. [Google Scholar]
- Cohen, V.; Panet-Raymond, V.; Sabbaghian, N.; Morin, I.; Batist, G.; Rozen, R. Methylenetetrahydrofolate reductase polymorphism in advanced colorectal cancer: A novel genomic predictor of clinical response to fluoropyrimidinebased chemotherapy. Clin. Cancer Res 2003, 9, 1611–1615. [Google Scholar]
- Lu, C.; Xie, H.; Wang, F.L.; Shen, H.B.; Wang, J.M. Diet folate, DNA methylation and genetic polymorphisms of MTHFR C677T in association in the prognosis of esophageal squamous cell carcinoma. BMC Cancer 2011, 11. [Google Scholar] [CrossRef]
- Sarbia, M.; Stahl, M.; von Weyhern, C.; Weirich, G.; Pühringer-Oppermann, F. The prognostic significance of genetic polymorphisms (methylenetetrahydrofolate reductase C677T, methionine synthase A2756G, thymidilate synthase tandem repeat polymorphism) in multimodally treated oesophageal squamous cell carcinoma. Br. J. Cancer 2006, 94, 203–207. [Google Scholar]
- Hunn, J.; Rodriguez, G.C. Ovarian cancer: Etiology, risk factors, and epidemiology. Clin. Obstet. Gynecol 2012, 55, 3–23. [Google Scholar]
- Sawabe, M.; Arai, T.; Araki, A.; Hosoi, T.; Kuchiba, A.; Tanaka, N.; Naito, T.; Oda, K.; Ikeda, S.; Muramatsu, M. Smoking confers a MTHFR 677C>T genotype-dependent risk for systemic atherosclerosis: Results from a large number of elderly autopsy cases that died in a community-based general geriatric hospital. J. Atheroscler. Thromb 2009, 16, 91–104. [Google Scholar]
- Tsai, C.W.; Hsu, C.F.; Tsai, M.H.; Tsou, Y.A.; Hua, C.H.; Chang, W.S.; Lin, C.C.; Bau, D.T. Methylenetetrahydrofolate reductase (MTHFR) genotype, smoking habit, metastasis and oral cancer in Taiwan. Anticancer Res 2011, 31, 2395–2399. [Google Scholar]
- Supic, G.; Jovic, N.; Kozomara, R.; Zeljic, K.; Magic, Z. Interaction between the MTHFR C677T polymorphism and alcohol—impact on oral cancer risk and multiple DNA methylation of tumor-related genes. J. Dent. Res 2011, 90, 65–70. [Google Scholar]



{kind=link}
{kind=link}
| Variable | Cases, N (%) | Controls, N (%) | p value |
|---|---|---|---|
| Age, years [mean, (sd)] | 47.2, 7.5 | 47.6, 8.1 | 0.30 |
| Smoking status | |||
| Smokers | 196 (91.2) | 204 (93.5) | 0.34 |
| Nonsmokers | 19 (8.8) | 14 (6.5) | |
| Drinking status | |||
| Drinkers | 169 (21.6) | 177 (18.8) | 0.50 |
| Nondrinkers | 46 (78.4) | 41 (81.2) | |
| Number of deliveries | |||
| 0 | 27 (12.6) | 12 (5.7) | <0.05 |
| 1 | 85 (39.6) | 79 (36.4) | |
| 2 | 83 (38.7) | 95 (43.7) | |
| ≥3 | 20 (9.1) | 31 (14.2) | |
| Menopausal status | |||
| Pre-menopausal | 105 (48.7) | 97 (44.3) | 0.37 |
| Post-menopausal | 110 (51.3) | 121 (55.7) | |
| Hormone replacement therapy | |||
| Never | 203 (94.5) | 212 (97.2) | 0.14 |
| Ever | 12 (5.5) | 6 (2.8) | |
| Oral contraceptive use | |||
| Never | 162 (75.3) | 140 (64.4) | <0.05 |
| Ever | 53 (24.7) | 78 (35.6) | |
| Ovarian cancer in first-degree relatives | |||
| Yes | 203 (94.4) | 217 (99.994) | <0.05 |
| No | 12 (5.6) | 1 (0.006) | |
| Tumor type | |||
| Invasive | 132 (61.6) | ||
| Borderline | 81 (37.5) | ||
| Unknown | 2 (0.9) | ||
| Chemotherapy | |||
| Yes | 154 (71.6) | ||
| No | 44 (20.5) | ||
| Radiotherapy | |||
| Yes | 13 (6.0) | ||
| No | 185 (86.0) | ||
| Genotype/Allele | Cases, N (%) | Controls, N (%) | OR 1 (95% CI) | OR 2 (95% CI) |
|---|---|---|---|---|
| MTHFR C677T | ||||
| CC | 102 (47.3) | 115 (52.8) | 1.0 (Reference) | 1.0 (Reference) |
| CT | 94 (43.9) | 92 (42.1) | 1.15 (0.76–1.74) | 1.48 (0.94–2.15) |
| TT | 19 (8.8) | 11 (5.1) | 1.94 (0.83–4.75) | 2.43 (1.32–6.32) |
| T allele | 113 (52.7) | 103 (47.2) | 1.24 (0.83–1.84) | 1.67 (0.99–3.27) |
| Daily folate consumption (μg/day) | ||||
| Mean (SE) | 257.4, 36.7 | 295.5, 28.6 | - | |
| <200 | 61 (28.6) | 46 (21.3) | 1.0 (Reference) | 1.0 (Reference) |
| 200–310 | 90 (41.7) | 95 (43.7) | 0.71 (0.43–1.19) | 0.66 (0.41–1.05) |
| >310 | 64 (29.7) | 76 (35) | 0.64 (0.37–1.09) | 0.54 (0.32–0.94) |
| N (%) | Mean Survival, 95% CI (months) | HR (95% CI), p value | |
|---|---|---|---|
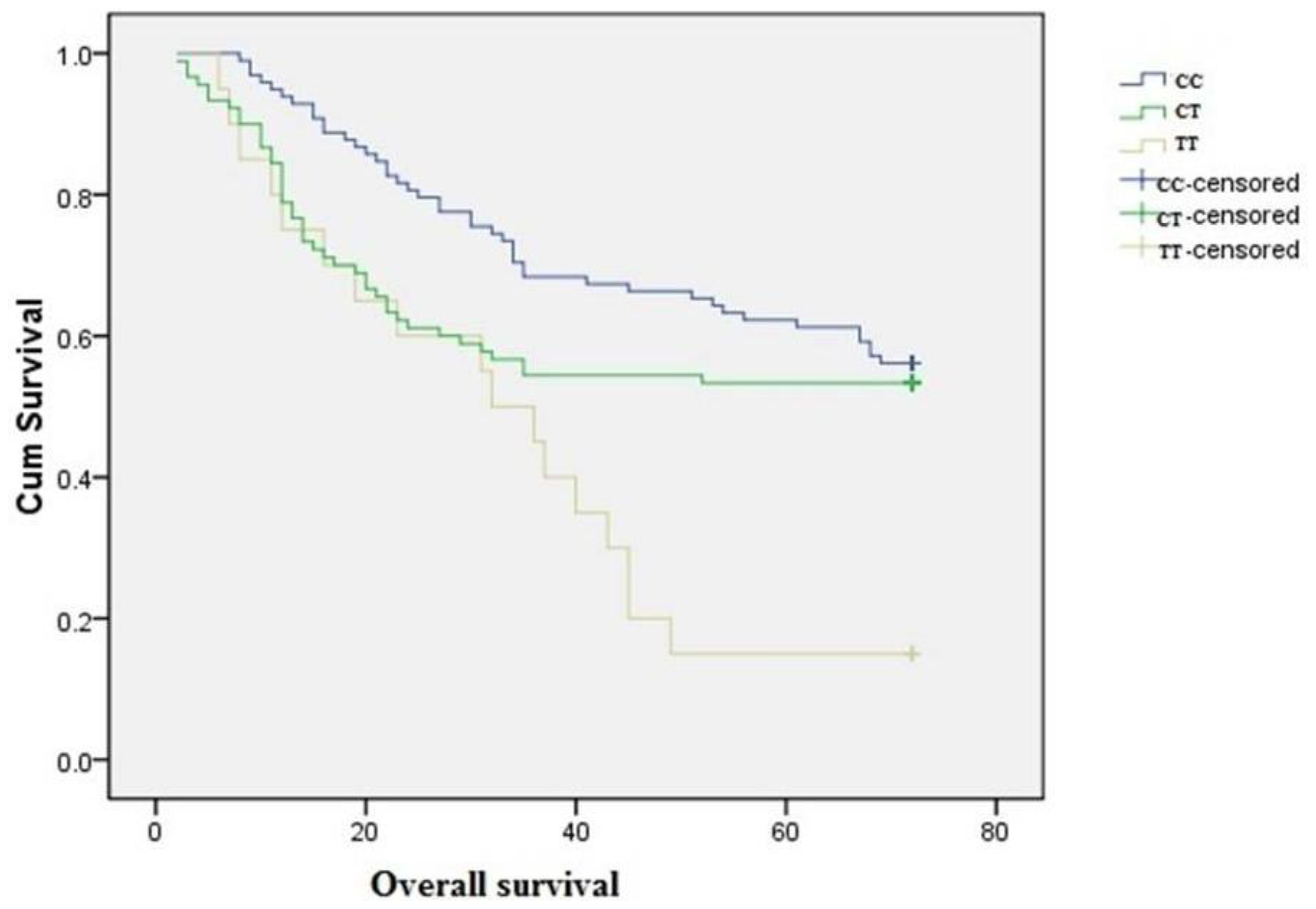
| MTHFR C677T | |||
| CC | 98 (47.2) | 54.5 (69.9–59.1) | 1.0 (reference) |
| CT | 90 (43.1) | 46.0 (40.1–51.9) | 1.34 (0.89–2.18), 0.11 |
| TT | 20 (9.7) | 33.8 (24.6–43.0) | 2.17 (1.20–4.79), <0.05 |
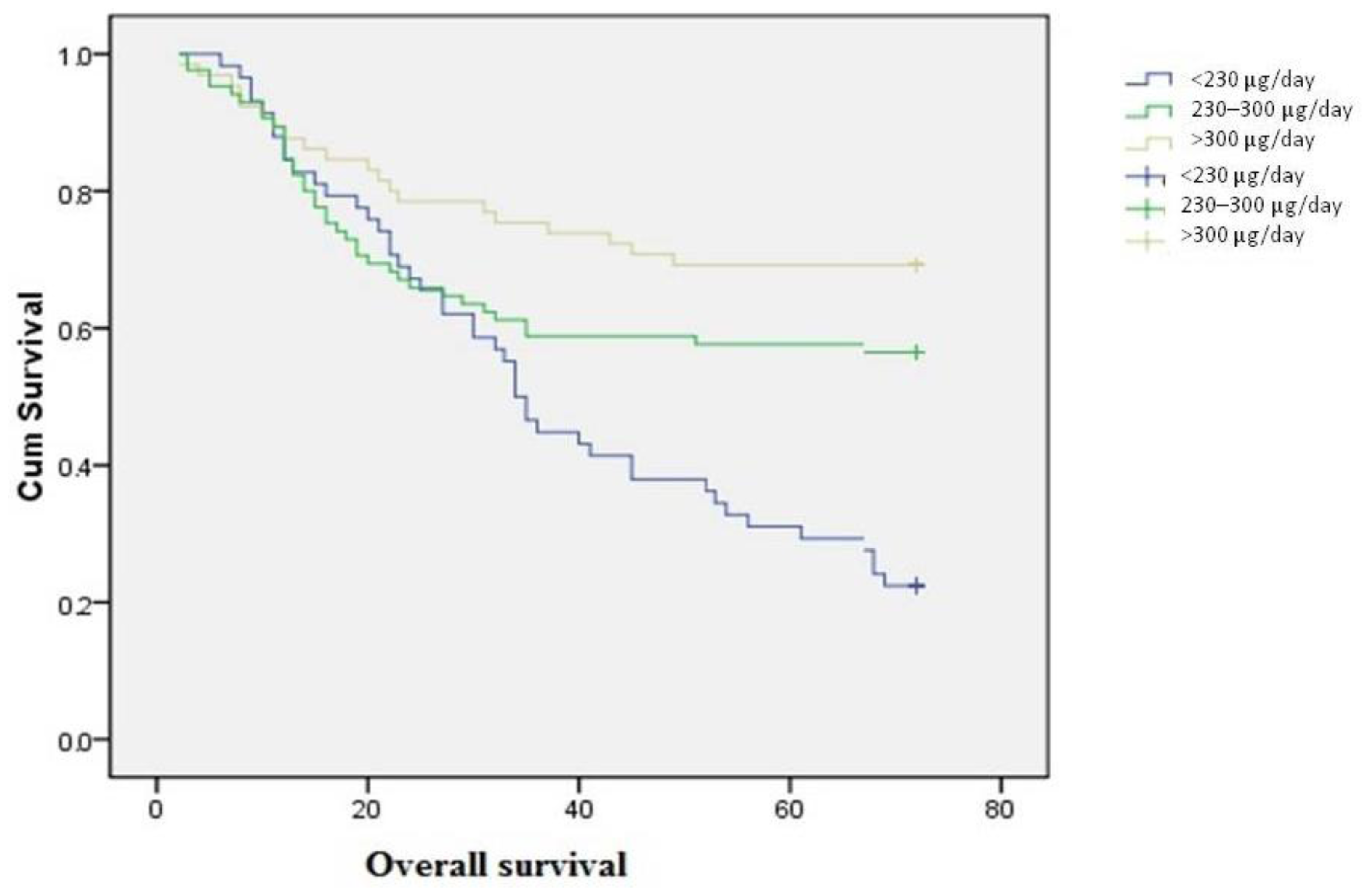
| Folate intake (μg/day) | |||
| <230 | 58 (27.9) | 40.5 (34.5–46.5) | 1.0 (reference) |
| 230–300 | 88 (42.2) | 48.8 (42.9–54.7) | 0.67 (0.40–1.03), 0.06 |
| >300 | 62 (29.9) | 56.2 (50.2–62.3) | 0.43 (0.33–0.88), <0.05 |
| Daily folate consumption | Genotype | ||||||||
|---|---|---|---|---|---|---|---|---|---|
| CC Cases (%) | Deaths N (%) | HR (95% CI) 1 | CT Cases | Deaths N (%) | HR (95% CI) 1 | TT Cases | Deaths N (%) | HR (95% CI) 1 | |
| <230 μg/day | 30 (30.6) | 23 (51.1) | 1.0 (Reference) | 20 (22.2) | 16 (38.1) | 1.0 (Reference) | 8 (40.0) | 6 (40.0) | 1.0 (Reference) |
| 230–300 μg/day | 33 (33.7) | 14 (31.1) | 0.56 (0.39–0.96) | 48 (53.3) | 18 (42.9) | 0.59 (0.42–1.27) | 7 (35.0) | 5 (33.3) | 1.25 (0.84–1.45) |
| >300 μg/day | 35 (35.7) | 8 (17.8) | 0.32 (0.27–0.82) | 22 (24.5) | 8 (19.0) | 0.45 (0.34–1.02) | 5 (25.0) | 4 (26.7) | 1.59 (0.93–2.24) |
© 2012 by the authors; licensee Molecular Diversity Preservation International, Basel, Switzerland. This article is an open-access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/3.0/).
Share and Cite
Zhang, L.; Liu, W.; Hao, Q.; Bao, L.; Wang, K. Folate Intake and Methylenetetrahydrofolate Reductase Gene Polymorphisms as Predictive and Prognostic Biomarkers for Ovarian Cancer Risk. Int. J. Mol. Sci. 2012, 13, 4009-4020. https://doi.org/10.3390/ijms13044009
Zhang L, Liu W, Hao Q, Bao L, Wang K. Folate Intake and Methylenetetrahydrofolate Reductase Gene Polymorphisms as Predictive and Prognostic Biomarkers for Ovarian Cancer Risk. International Journal of Molecular Sciences. 2012; 13(4):4009-4020. https://doi.org/10.3390/ijms13044009
Chicago/Turabian StyleZhang, Li, Wenxin Liu, Quan Hao, Lewen Bao, and Ke Wang. 2012. "Folate Intake and Methylenetetrahydrofolate Reductase Gene Polymorphisms as Predictive and Prognostic Biomarkers for Ovarian Cancer Risk" International Journal of Molecular Sciences 13, no. 4: 4009-4020. https://doi.org/10.3390/ijms13044009
APA StyleZhang, L., Liu, W., Hao, Q., Bao, L., & Wang, K. (2012). Folate Intake and Methylenetetrahydrofolate Reductase Gene Polymorphisms as Predictive and Prognostic Biomarkers for Ovarian Cancer Risk. International Journal of Molecular Sciences, 13(4), 4009-4020. https://doi.org/10.3390/ijms13044009