
The Role of the Neutrophil to Lymphocyte Ratio for Survival Outcomes in Patients with Metastatic Castration-Resistant Prostate Cancer Treated with Abiraterone

 , ,
, ,
Abstract
:1. Introduction
2. Results
2.1. Patient Characteristics
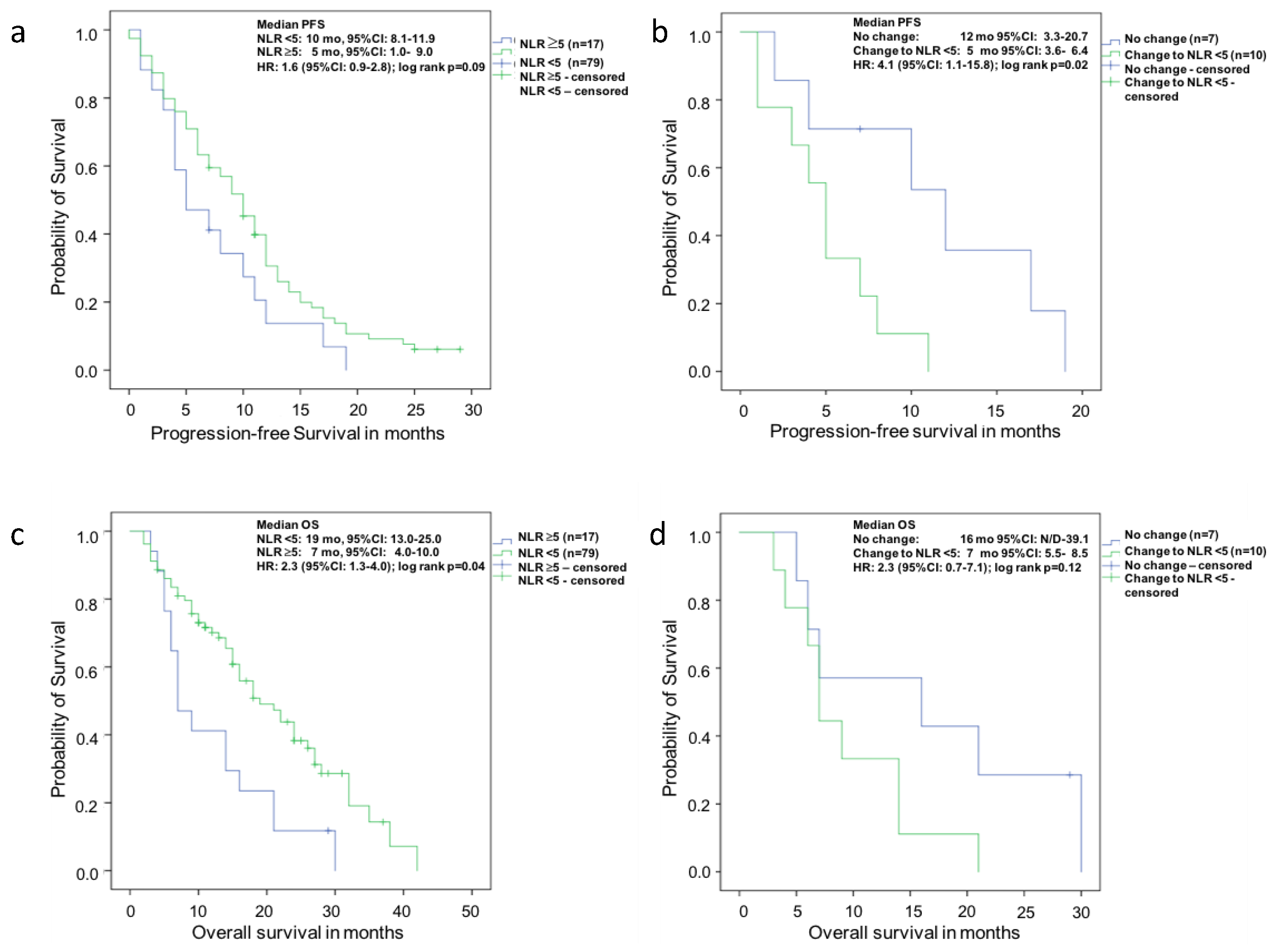
2.2. Prognostication of Survival Outcomes at Baseline
2.3. Prognostication of Survival Outcomes with Change of Neutrophil-to-Lymphocyte Ratio (NLR) to <5 in Patients with a Baseline NLR > 5 vs. no Change after Eight Weeks of Abiraterone
3. Discussion
4. Materials and Methods
4.1. Patients
4.2. Statistical Methods
5. Conclusions
Author Contributions
Conflicts of Interest
Abbreviations
| mCRPC | Metastatic castration resistant prostate cancer |
| OS | Overall survival |
| PD | Progressive disease |
| NLR | Neutrophil-to-lymphocyte ratio |
| PFS | Progression-free survival |
| PSA | Prostate specific antigen |
| IQR | Interquartile range |
| ALP | Alkaline phosphatase |
| LDH | Lactate dehydrogenase |
| ULN | Upper normal limit |
| PCWG2 | Prostate cancer working group 2 |
| HR | Hazard ratio |
| 95%CI | 95% confidence interval |
| ECOG | Eastern Collaborative Oncology Group Performance Status |
| CR | Complete remission |
| PR | Partial remission |
| SD | Stable disease |
References
- Ryan, C.J.; Smith, M.R.; Fizazi, K.; Saad, F.; Mulders, P.F.; Sternberg, C.N.; Miller, K.; Logothetis, C.J.; Shore, N.D.; Small, E.J.; et al. Abiraterone acetate plus prednisone versus placebo plus prednisone in chemotherapy-naive men with metastatic castration-resistant prostate cancer (COU-AA-302): Final overall survival analysis of a randomised, double-blind, placebo-controlled phase 3 study. Lancet Oncol. 2015, 16, 152–160. [Google Scholar] [CrossRef]
- Beer, T.M.; Tombal, B. Enzalutamide in metastatic prostate cancer before chemotherapy. N. Engl. J. Med. 2014, 371, 1755–1756. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kantoff, P.W.; Higano, C.S.; Shore, N.D.; Berger, E.R.; Small, E.J.; Penson, D.F.; Redfern, C.H.; Ferrari, A.C.; Dreicer, R.; Sims, R.B.; et al. Sipuleucel-T immunotherapy for castration-resistant prostate cancer. N. Engl. J. Med. 2010, 363, 411–422. [Google Scholar] [CrossRef] [PubMed]
- Fizazi, K.; Scher, H.I.; Molina, A.; Logothetis, C.J.; Chi, K.N.; Jones, R.J.; Staffurth, J.N.; North, S.; Vogelzang, N.J.; Saad, F.; et al. Abiraterone acetate for treatment of metastatic castration-resistant prostate cancer: Final overall survival analysis of the COU-AA-301 randomised, double-blind, placebo-controlled phase 3 study. Lancet Oncol. 2012, 13, 983–992. [Google Scholar] [CrossRef]
- Scher, H.I.; Fizazi, K.; Saad, F.; Taplin, M.E.; Sternberg, C.N.; Miller, K.; de Wit, R.; Mulders, P.; Chi, K.N.; Shore, N.D.; et al. Increased survival with enzalutamide in prostate cancer after chemotherapy. N. Engl. J. Med. 2012, 367, 1187–1197. [Google Scholar] [PubMed]
- De Bono, J.S.; Oudard, S.; Ozguroglu, M.; Hansen, S.; Machiels, J.P.; Kocak, I.; Gravis, G.; Bodrogi, I.; Mackenzie, M.J.; Shen, L.; et al. Prednisone plus cabazitaxel or mitoxantrone for metastatic castration-resistant prostate cancer progressing after docetaxel treatment: A randomised open-label trial. Lancet 2010, 376, 1147–1154. [Google Scholar] [CrossRef]
- Parker, C.; Nilsson, S.; Heinrich, D.; Helle, S.I.; O’Sullivan, J.M.; Fossa, S.D.; Chodacki, A.; Wiechno, P.; Logue, J.; Seke, M.; et al. α emitter radium-223 and survival in metastatic prostate cancer. N. Engl. J. Med. 2013, 369, 213–223. [Google Scholar] [CrossRef] [PubMed]
- Ryan, C.J.; Shah, S.; Efstathiou, E.; Smith, M.R.; Taplin, M.E.; Bubley, G.J.; Logothetis, C.J.; Kheoh, T.; Kilian, C.; Haqq, C.M.; et al. Phase II study of abiraterone acetate in chemotherapy-naive metastatic castration-resistant prostate cancer displaying bone flare discordant with serologic response. Clin. Cancer Res. 2011, 17, 4854–4861. [Google Scholar] [CrossRef] [PubMed]
- Hanahan, D.; Weinberg, R.A. Hallmarks of cancer: The next generation. Cell 2011, 144, 646–674. [Google Scholar] [CrossRef] [PubMed]
- Lorente, D.; Mateo, J.; Templeton, A.J.; Zafeiriou, Z.; Bianchini, D.; Ferraldeschi, R.; Bahl, A.; Shen, L.; Su, Z.; Sartor, O.; et al. Baseline neutrophil-lymphocyte ratio (NLR) is associated with survival and response to treatment with second-line chemotherapy for advanced prostate cancer independent of baseline steroid use. Ann. Oncol. 2015, 26, 750–755. [Google Scholar] [CrossRef] [PubMed]
- Luo, Y.; She, D.L.; Xiong, H.; Fu, S.J.; Yang, L. Pretreatment Neutrophil to Lymphocyte Ratio as a Prognostic Predictor of Urologic Tumors: A Systematic Review and Meta-Analysis. Medicine 2015, 94, e1670. [Google Scholar] [CrossRef] [PubMed]
- Xin-Ji, Z.; Yong-Gang, L.; Xiao-Jun, S.; Xiao-Wu, C.; Dong, Z.; Da-Jian, Z. The prognostic role of neutrophils to lymphocytes ratio and platelet count in gastric cancer: A meta-analysis. Int. J. Surg. 2015, 21, 84–91. [Google Scholar] [CrossRef] [PubMed]
- Yodying, H.; Matsuda, A.; Miyashita, M.; Matsumoto, S.; Sakurazawa, N.; Yamada, M.; Uchida, E. Prognostic significance of neutrophil-to-lymphocyte ratio and platelet-to-lymphocyte ratio in oncologic outcomes of esophageal cancer: A systematic review and meta-analysis. Ann. Surg. Oncol. 2016, 23, 646–654. [Google Scholar] [CrossRef] [PubMed]
- Keizman, D.; Gottfried, M.; Ish-Shalom, M.; Maimon, N.; Peer, A.; Neumann, A.; Rosenbaum, E.; Kovel, S.; Pili, R.; Sinibaldi, V.; et al. Pretreatment neutrophil-to-lymphocyte ratio in metastatic castration-resistant prostate cancer patients treated with ketoconazole: Association with outcome and predictive nomogram. Oncologist 2012, 17, 1508–1514. [Google Scholar] [CrossRef] [PubMed]
- Sonpavde, G.; Pond, G.R.; Armstrong, A.J.; Clarke, S.J.; Vardy, J.L.; Templeton, A.J.; Wang, S.L.; Paolini, J.; Chen, I.; Chow-Maneval, E.; et al. Prognostic impact of the neutrophil-to-lymphocyte ratio in men with metastatic castration-resistant prostate cancer. Clin. Genitourin. Cancer 2014, 12, 317–324. [Google Scholar] [CrossRef] [PubMed]
- Van Soest, R.J.; Templeton, A.J.; Vera-Badillo, F.E.; Mercier, F.; Sonpavde, G.; Amir, E.; Tombal, B.; Rosenthal, M.; Eisenberger, M.A.; Tannock, I.F.; et al. Neutrophil-to-lymphocyte ratio as a prognostic biomarker for men with metastatic castration-resistant prostate cancer receiving first-line chemotherapy: Data from two randomized phase III trials. Ann. Oncol. 2015, 26, 743–749. [Google Scholar] [CrossRef] [PubMed]
- Leibowitz-Amit, R.; Templeton, A.J.; Omlin, A.; Pezaro, C.; Atenafu, E.G.; Keizman, D.; Vera-Badillo, F.; Seah, J.A.; Attard, G.; Knox, J.J.; et al. Clinical variables associated with PSA response to abiraterone acetate in patients with metastatic castration-resistant prostate cancer. Ann. Oncol. 2014, 25, 657–662. [Google Scholar] [CrossRef] [PubMed]
- Donskov, F. Immunomonitoring and prognostic relevance of neutrophils in clinical trials. Semin. Cancer Biol 2013, 23, 200–207. [Google Scholar] [CrossRef] [PubMed]
- Guthrie, G.J.; Charles, K.A.; Roxburgh, C.S.; Horgan, P.G.; McMillan, D.C.; Clarke, S.J. The systemic inflammation-based neutrophil-lymphocyte ratio: Experience in patients with cancer. Crit. Rev. Oncol. Hematol. 2013, 88, 218–230. [Google Scholar] [CrossRef] [PubMed]
- Nakagawa, M.; Terashima, T.; D’Yachkova, Y.; Bondy, G.P.; Hogg, J.C.; van Eeden, S.F. Glucocorticoid-induced granulocytosis: Contribution of marrow release and demargination of intravascular granulocytes. Circulation 1998, 98, 2307–2313. [Google Scholar] [CrossRef] [PubMed]
- Facchini, G.; Caffo, O.; Ortega, C.; D’Aniello, C.; Di Napoli, M.; Cecere, S.C.; Della Pepa, C.; Crispo, A.; Maines, F.; Ruatta, F.; et al. Very Early PSA Response to Abiraterone in mCRPC Patients: A Novel Prognostic Factor Predicting Overall Survival. Front. Pharmacol. 2016, 7, 123. [Google Scholar] [CrossRef] [PubMed]
- Scher, H.I.; Halabi, S.; Tannock, I.; Morris, M.; Sternberg, C.N.; Carducci, M.A.; Eisenberger, M.A.; Higano, C.; Bubley, G.J.; Dreicer, R.; et al. Design and end points of clinical trials for patients with progressive prostate cancer and castrate levels of testosterone: Recommendations of the Prostate Cancer Clinical Trials Working Group. J. Clin. Oncol. 2008, 26, 1148–1159. [Google Scholar] [CrossRef] [PubMed]
- Eisenhauer, E.A.; Therasse, P.; Bogaerts, J.; Schwartz, L.H.; Sargent, D.; Ford, R.; Dancey, J.; Arbuck, S.; Gwyther, S.; Mooney, M.; et al. New response evaluation criteria in solid tumours: Revised RECIST guideline (version 1.1). Eur. J. Cancer 2009, 45, 228–247. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Variable | All | NLR <5 | NLR >5 | p |
|---|---|---|---|---|
| Patients (n) (%) | 96 | 79 (82.3) | 17 (17.7) | |
| Median NLR Baseline (ng/mL) (IQR) | 3.2 (2.5–4.5) | |||
| Age, median (years) (IQR) | 70.0 (63.0–76.3) | 70.0 (62.0–76.0) | 70.0 (65.0–78.0) | 0.60 |
| Median follow-up | 20.0 (11.0–28.0) | 17.5 (11.0–26.8) | 29.0 (29.0–29.0) | 0.28 |
| Median duration AA therapy (months) (IQR) | 10.0 (6.0–14.3) | 11.0 (7.0–15.0) | 7.0 (5.0–11.5) | 0.08 |
| GS ≥8 (n) (%) | 55 (59.8) | 46 (60.5) | 9 (56.3) | 0.75 |
| Lnn. Metastases (n) (%) | 61 (63.5) | 50 (63.3) | 11 (64.7) | 0.91 |
| Visceral Metastases (n) (%) | 27 (28.1) | 24 (30.4) | 3 (17.6) | 0.38 |
| Bone Metastases (n) (%) | 85 (88.5) | 69 (87.3) | 16 (94.1) | 0.68 |
| Pre CTX (n) (%) | 52 (54.2) | 44 (55.7) | 8 (47.1) | 0.52 |
| Post CTX (n) (%) | 44 (45.8) | 35 (44.3) | 9 (52.9) | |
| Patients died (n) (%) | 67 (69.8) | 51 (64.6) | 16 (94.1) | 0.02 |
| ECOG (all) (n) (%) | ||||
| 0 | 19 (20.0) | 16 (20.5) | 3 (17.6) | 0.91 |
| 1 | 57 (60.0) | 47 (60.3) | 10 (58.8) | |
| 2 | 19 (20.0) | 15 (19.2) | 4 (23.5) | |
| Antiresorptive therapy (n) (%) | 57 (59.4) | 47 (59.5) | 10 (58.8) | 0.96 |
| Zoledronic acid (n) (%) | 40 (41.7) | 33 (41.8) | 7 (41.2) | 0.96 |
| Denosumab (n) (%) | 19 (19.8) | 15 (19.0) | 4 (23.5) | 0.67 |
| Best clinical outcome (n) (%) | ||||
| CR | 1 (1.1) | 1 (1.3) | 0 (0) | 0.61 |
| PR | 54 (56.8) | 46 (59.0) | 8 (47.1) | |
| SD | 27 (28.4) | 20 (25.6) | 7 (41.2) | |
| PD | 13 (13.7) | 11 (14.1) | 2 (11.8) | |
| PSA red. ≥50% (n) (%) | 48 (50.0) | 42 (53.2) | 6 (35.3) | 0.18 |
| PSA red. ≥90% (n) (%) | 23 (24.0) | 22 (27.8) | 1 (5.9) | 0.06 |
| Median PSA Baseline (ng/mL) (IQR) | 134 (45–349) | 91 (35–334) | 224 (107–589) | 0.04 |
| Median LDH Baseline (U/L) (IQR) | 251 (210–358) | 240 (205–357) | 308 (245–386) | 0.04 |
| LDH BL >UNL (n) (%) | 62 (64.6) | 47 (59.5) | 15 (88.2) | 0.03 |
| Median ALP Baseline (U/L) (IQR) | 126 (86–296) | 126 (91–297) | 103 (77–266) | 0.43 |
| (a) Univariate Analysis PFS at Baseline | (b) Univariate Analysis of PFS in n = 17 Patients with Baseline NLR > 5 after Eight Weeks of Abiraterone | ||||
|---|---|---|---|---|---|
| Variable | HR (95%CI) | p | Variable | HR (95%CI) | p |
| ECOG | <0.01 | ECOG | 0.57 | ||
| 0–1 | 1 (reference) | 0–1 | 1 (reference) | ||
| 2 | 2.9 (1.7–4.9) | 2 | 1.4 (0.4–4.8) | ||
| LDH baseline >UNL | <0.01 | LDH baseline >UNL | 1 (reference) | 0.52 | |
| No | 1 (reference) | No | |||
| Yes | 2.6 (1.6–4.3) | Yes | 2.0 (0.3–15.4) | ||
| Visceral metastases | 0.02 | Visceral metastases | 0.85 | ||
| No | 1 (reference) | No | 1 (reference) | ||
| Yes | 2.2 (1.4–3.5) | Yes | 0.9 (0.2–3.3) | ||
| ALP baseline >UNL | 0.13 | ALP baseline >UNL | 0.55 | ||
| No | 1 (reference) | No | 1 (reference) | ||
| Yes | 1.4 (0.9–2.1) | Yes | 1.4 (0.5–3.9) | ||
| NLR | 0.11 | NLR | 0.04 | ||
| <5 | 1 (reference) | No change | 1 (reference) | ||
| >5 | 1.6 (0.9–2.8) | Change to <5 | 4.1 (1.1–15.8) | ||
| Abiraterone | 0.10 | PSA decline ≥50% | 0.14 | ||
| Pre-Docetaxel | 1 (reference) | Yes | 1 (reference) | ||
| Post-Docetaxel | 1.4 (0.9–2.2) | No | 2.7 (0.7–10.2) | ||
| Gleason Score | 0.10 | Abiraterone | 0.41 | ||
| <8 | 1 (reference) | Pre-Docetaxel | 1 (reference) | ||
| ≥8 | 1.5 (0.9–2.3) | Post-Docetaxel | 1.6 (0.5–4.6) | ||
| Lymphonodal metastases | 0.77 | Gleason Score | 0.63 | ||
| No | 1 (reference) | <8 | 1 (reference) | ||
| Yes | 0.9 (0.6–1.5) | ≥8 | 1.3 (0.4–3.9) | ||
| Bone Metastases | 0.82 | Lymphonodal metastases | 0.41 | ||
| No | 1 (reference) | No | 1 (reference) | ||
| Yes | 1.1 (0.5–2.2) | Yes | 0.6 (0.2–1.9) | ||
| (a) Univariate Analysis OS at Baseline | (b) Univariate Analysis of OS in n = 17 Patients with Baseline NLR >5 after Eight Weeks of Abiraterone | ||||
|---|---|---|---|---|---|
| Variable | HR (95%CI) | p | Variable | HR (95%CI) | p |
| ECOG | <0.01 | ECOG | 0.60 | ||
| 0–1 | 1 (reference) | 0–1 | 1 (reference) | ||
| 2 | 3.4 (1.9–6.0) | 2 | 1.4 (0.3–4.5) | ||
| LDH baseline >UNL | <0.01 | LDH baseline >UNL | 0.65 | ||
| No | 1 (reference) | No | 1 (reference) | ||
| Yes | 3.1 (1.7–5.8) | Yes | 0.7 (0.2–3.3) | ||
| Visceral metastases | 0.35 | Visceral metastases | 0.76 | ||
| No | 1 (reference) | No | 1 (reference) | ||
| Yes | 1.3 (0.8–2.2) | Yes | 0.8 (0.2–2.9) | ||
| ALP baseline >UNL | <0.01 | ALP baseline >UNL | 0.83 | ||
| No | 1 (reference) | No | 1 (reference) | ||
| Yes | 1.9 (1.2–3.2) | Yes | 0.9 (0.3–2.5) | ||
| NLR | <0.01 | NLR | 0.15 | ||
| <5 | 1 (reference) | No change | 1 (reference) | ||
| >5 | 2.3 (1.3–4.0) | Change to <5 | 2.3 (0.7–7.1) | ||
| Abiraterone | 0.06 | PSA decline ≥50% | 0.08 | ||
| Pre-Docetaxel | 1 (reference) | Yes | 1 (reference) | ||
| Post-Docetaxel | 1.6 (1.0–2.6) | No | 2.9 (0.9–9.4) | ||
| Gleason Score | 0.67 | Abiraterone | 0.38 | ||
| <8 | 1 (reference) | Pre-Docetaxel | 1 (reference) | ||
| ≥8 | 1.1 (0.7–1.9) | Post-Docetaxel | 1.6 (0.6–4.6) | ||
| Lymphonodal metastases | 0.35 | Gleason Score | 0.93 | ||
| No | 1 (reference) | <8 | 1 (reference) | ||
| Yes | 0.8 (0.5–1.3) | ≥8 | 1.1 (0.4–3.0) | ||
| Bone metastases | 0.62 | Lymphonodal metastases | 0.64 | ||
| No | 1 (reference) | No | 1 (reference) | ||
| Yes | 1.3 (0.5–3.2) | Yes | 0.8 (0.3–2.2) | ||
| (a) Multivariate Analysis PFS at Baseline | (c) Multivariate analysis of PFS in n =17 Patients with Baseline NLR >5 after Eight Weeks of Abiraterone | ||||
| Variable | HR (95%CI) | p | Variable | HR (95%CI) | p |
| ECOG | 0.01 | NLR | 0.11 | ||
| 0–1 | 1 (reference) | No change | 1 (reference) | ||
| 2 | 2.6 (1.5–4.5) | Change to <5 | 3.4 (0.8–15.2) | ||
| LDH baseline >UNL | 0.01 | PSA decline ≥50% | 0.14 | ||
| No | 1 (reference) | Yes | 1 (reference) | ||
| Yes | 2.2 (1.3–3.8) | No | 1.5 (0.3–6.4) | ||
| Visceral metastases | 0.04 | ||||
| No | 1 (reference) | ||||
| Yes | 1.7 (1.0–2.9) | ||||
| ALP baseline >UNL | 0.25 | ||||
| No | 1 (reference) | ||||
| Yes | 1.3 (0.8–2.1) | ||||
| NLR | 0.71 | ||||
| <5 | 1 (reference) | ||||
| >5 | 1.1 (0.6–2.0) | ||||
| (b) Multivariate analysis OS at baseline | (d) Multivariate Analysis of OS in n = 17 Patients with Baseline NLR >5 after Eight Weeks of Abiraterone | ||||
| Variable | HR (95%CI) | p | Variable | HR (95%CI) | p |
| ECOG | <0.01 | NLR | 0.47 | ||
| 0–1 | 1 (reference) | No change | 1 (reference) | ||
| 2 | 3.0 (1.6–5.5) | Change to <5 | 1.6 (0.5–5.6) | ||
| LDH baseline >UNL | 0.01 | PSA decline ≥50% | 0.25 | ||
| No | 1 (reference) | Yes | 1 (reference) | ||
| Yes | 2.4 (1.2–4.6) | No | 2.2 (0.6–8.1) | ||
| Visceral metastases | 0.56 | ||||
| No | 1 (reference) | ||||
| Yes | 1.2 (0.7–2.1) | ||||
| ALP baseline >UNL | 0.05 | ||||
| No | 1 (reference) | ||||
| Yes | 1.7 (1.0–2.9) | ||||
| NLR | 0.10 | ||||
| <5 | 1 (reference) | ||||
| >5 | 1.7 (0.9–3.0) | ||||
© 2017 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license ( http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Boegemann, M.; Schlack, K.; Thomes, S.; Steinestel, J.; Rahbar, K.; Semjonow, A.; Schrader, A.J.; Aringer, M.; Krabbe, L.-M. The Role of the Neutrophil to Lymphocyte Ratio for Survival Outcomes in Patients with Metastatic Castration-Resistant Prostate Cancer Treated with Abiraterone. Int. J. Mol. Sci. 2017, 18, 380. https://doi.org/10.3390/ijms18020380
Boegemann M, Schlack K, Thomes S, Steinestel J, Rahbar K, Semjonow A, Schrader AJ, Aringer M, Krabbe L-M. The Role of the Neutrophil to Lymphocyte Ratio for Survival Outcomes in Patients with Metastatic Castration-Resistant Prostate Cancer Treated with Abiraterone. International Journal of Molecular Sciences. 2017; 18(2):380. https://doi.org/10.3390/ijms18020380
Chicago/Turabian StyleBoegemann, Martin, Katrin Schlack, Stefan Thomes, Julie Steinestel, Kambiz Rahbar, Axel Semjonow, Andres Jan Schrader, Martin Aringer, and Laura-Maria Krabbe. 2017. "The Role of the Neutrophil to Lymphocyte Ratio for Survival Outcomes in Patients with Metastatic Castration-Resistant Prostate Cancer Treated with Abiraterone" International Journal of Molecular Sciences 18, no. 2: 380. https://doi.org/10.3390/ijms18020380