
Exploration of the Esophageal Mucosal Barrier in Non-Erosive Reflux Disease

 ,
, 
Abstract
:1. Introduction
2. Results
2.1. Study Population Characteristics
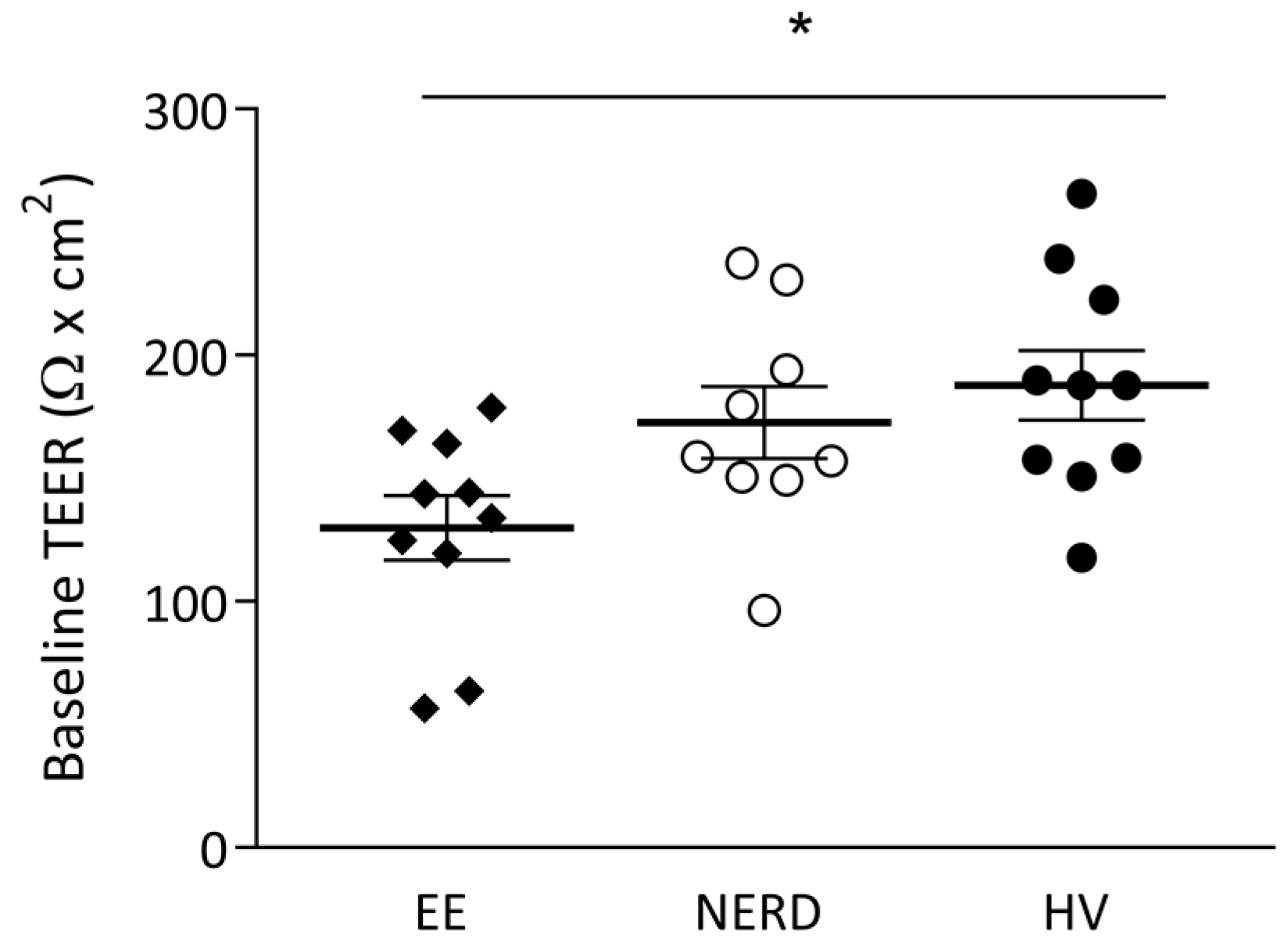
2.2. Ussing Chamber Experiment
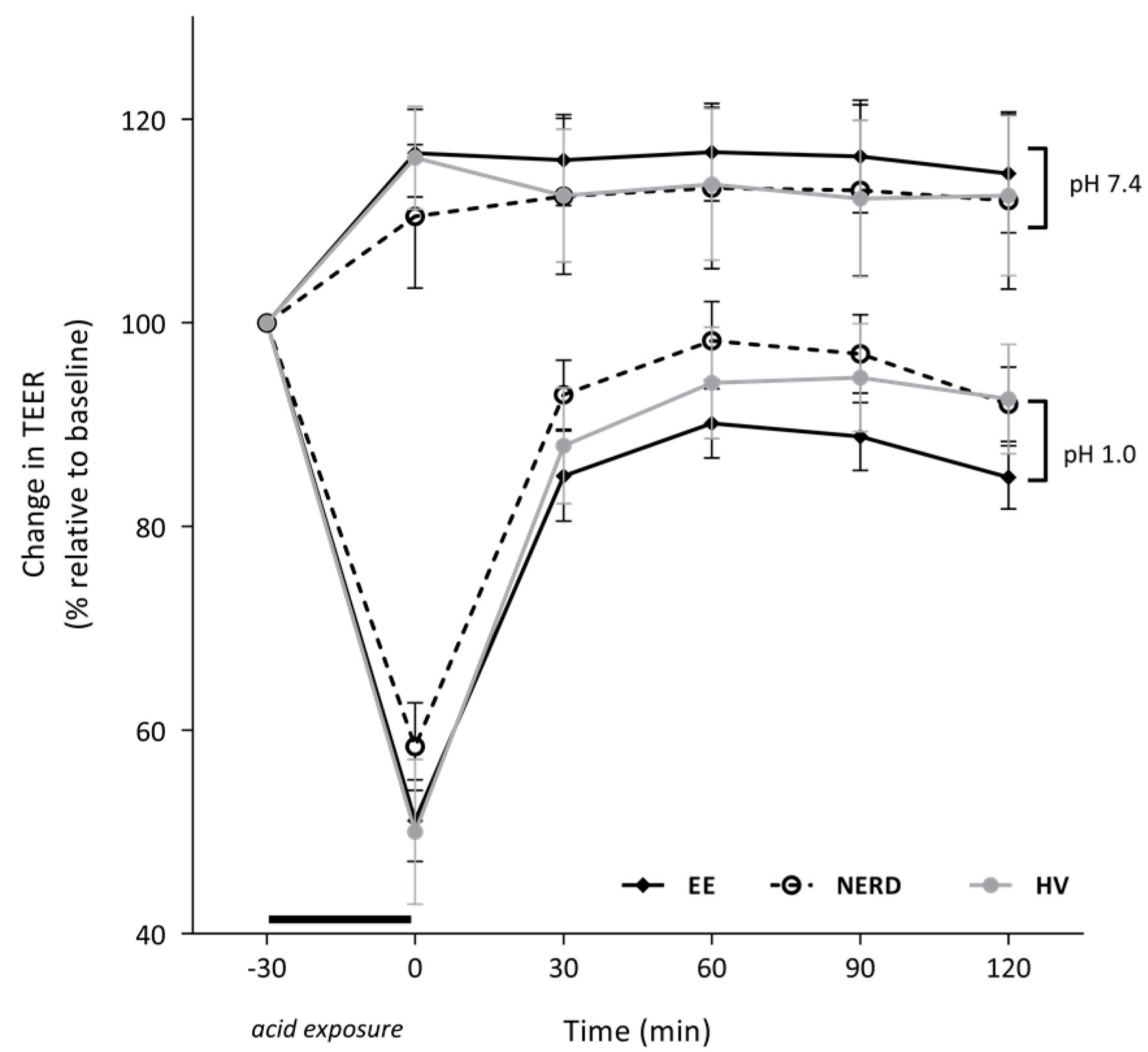
2.3. In Vitro Acid Exposure
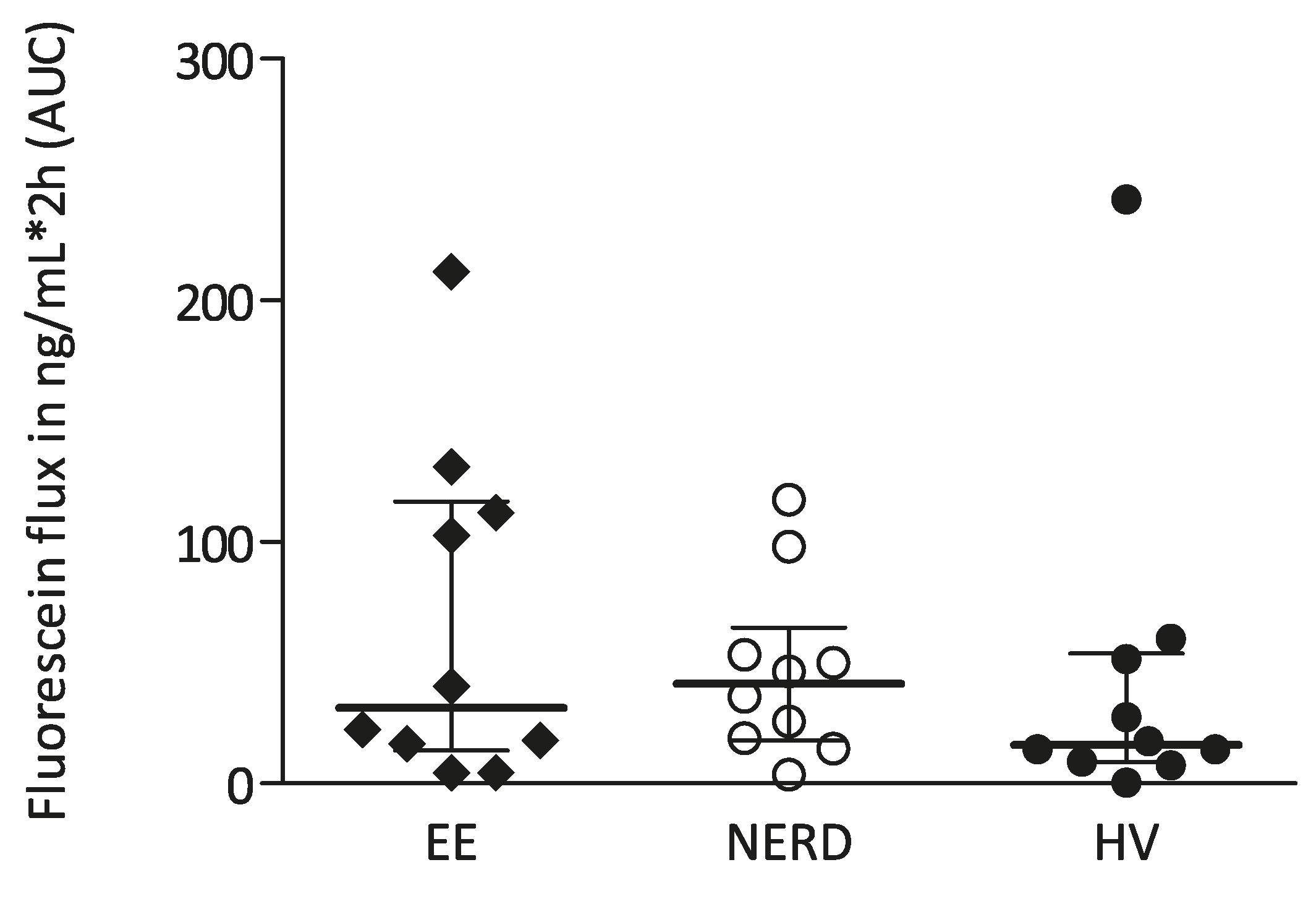
2.4. Mucosal Permeability
2.5. Tight Junction Gene Transcription
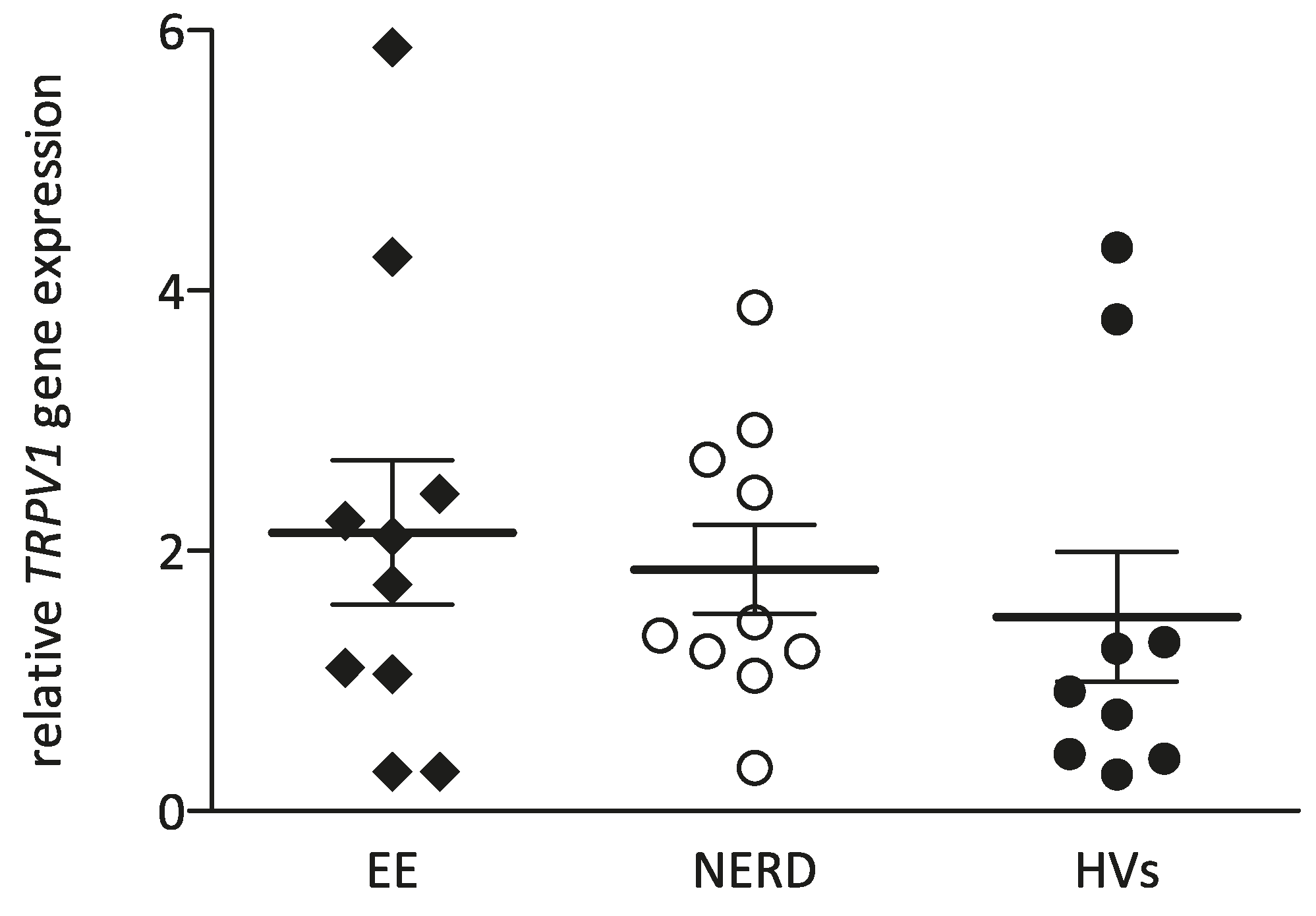
2.6. TRPV1 Gene Transcription
2.7. Associations and Correlations of Measurements
3. Discussion
4. Materials and Methods
4.1. Subjects
4.2. Study Protocol
4.3. GERD Symptom Evaluation
4.4. Ussing Chamber Experiment
4.5. Tight Junction Protein and TRPV1 Gene Transcription
4.6. Data and Statistical Analysis
5. Conclusions
Supplementary Materials
Author Contributions
Conflicts of Interest
References
- Barlow, W.J.; Orlando, R.C. The pathogenesis of heartburn in nonerosive reflux disease: A unifying hypothesis. Gastroenterology 2005, 128, 771–778. [Google Scholar] [CrossRef] [PubMed]
- Tack, J. Is there a unifying role for visceral hypersensitivity and irritable bowel syndrome in non-erosive reflux disease? Digestion 2008, 78, 42–45. [Google Scholar] [CrossRef] [PubMed]
- Knowles, C.H.; Aziz, Q. Visceral hypersensitivity in non-erosive reflux disease. Gut 2008, 57, 674–683. [Google Scholar] [CrossRef] [PubMed]
- Tobey, N.A.; Carson, J.L.; Alkiek, R.A.; Orlando, R.C. Dilated intercellular spaces: A morphological feature of acid reflux—Damaged human esophageal epithelium. Gastroenterology 1996, 111, 1200–1205. [Google Scholar] [CrossRef] [PubMed]
- Caviglia, R.; Ribolsi, M.; Maggiano, N.; Gabbrielli, A.M.; Emerenziani, S.; Guarino, M.P.; Carotti, S.; Habib, F.I.; Rabitti, C.; Cicala, M. Dilated intercellular spaces of esophageal epithelium in nonerosive reflux disease patients with physiological esophageal acid exposure. Am. J. Gastroenterol. 2005, 100, 543–548. [Google Scholar] [CrossRef] [PubMed]
- Farre, R.; Fornari, F.; Blondeau, K.; Vieth, M.; de Vos, R.; Bisschops, R.; Mertens, V.; Pauwels, A.; Tack, J.; Sifrim, D. Acid and weakly acidic solutions impair mucosal integrity of distal exposed and proximal non-exposed human oesophagus. Gut 2010, 59, 164–169. [Google Scholar] [CrossRef] [PubMed]
- Bredenoord, A.J. Mechanisms of reflux perception in gastroesophageal reflux disease: A review. Am. J. Gastroenterol. 2012, 107, 8–15. [Google Scholar] [CrossRef] [PubMed]
- Farre, R. Pathophysiology of gastro-esophageal reflux disease: A role for mucosa integrity? Neurogastroenterol. Motil. 2013, 25, 783–799. [Google Scholar] [CrossRef] [PubMed]
- Nagahara, A.; Miwa, H.; Minoo, T.; Hojo, M.; Kawabe, M.; Osada, T.; Kurosawa, A.; Asaoka, D.; Terai, T.; Ohkusa, T.; et al. Increased esophageal sensitivity to acid and saline in patients with nonerosive gastro-esophageal reflux disease. J. Clin. Gastroenterol. 2006, 40, 891–895. [Google Scholar] [CrossRef] [PubMed]
- Reddy, H.; Staahl, C.; Arendt-Nielsen, L.; Gregersen, H.; Drewes, A.M.; Funch-Jensen, P. Sensory and biomechanical properties of the esophagus in non-erosive reflux disease. Scand. J. Gastroenterol. 2007, 42, 432–440. [Google Scholar] [CrossRef] [PubMed]
- Trimble, K.C.; Pryde, A.; Heading, R.C. Lowered oesophageal sensory thresholds in patients with symptomatic but not excess gastro-oesophageal reflux: Evidence for a spectrum of visceral sensitivity in gord. Gut 1995, 37, 7–12. [Google Scholar] [CrossRef] [PubMed]
- Kindt, S.; Vos, R.; Blondeau, K.; Tack, J. Influence of intra-oesophageal capsaicin instillation on heartburn induction and oesophageal sensitivity in man. Neurogastroenterol. Motil. 2009, 21, 1032–1082. [Google Scholar] [CrossRef] [PubMed]
- Harnett, K.M.; Rieder, F.; Behar, J.; Biancani, P. Viewpoints on acid-induced inflammatory mediators in esophageal mucosa. J. Neurogastroenterol. Motil. 2010, 16, 374–388. [Google Scholar] [CrossRef] [PubMed]
- Yoshida, N.; Kuroda, M.; Suzuki, T.; Kamada, K.; Uchiyama, K.; Handa, O.; Takagi, T.; Yoshikawa, T.; Kuramoto, H. Role of nociceptors/neuropeptides in the pathogenesis of visceral hypersensitivity of nonerosive reflux disease. Dig. Dis. Sci. 2013, 58, 2237–2243. [Google Scholar] [CrossRef] [PubMed]
- Xu, X.; Li, Z.; Zou, D.; Yang, M.; Liu, Z.; Wang, X. High expression of calcitonin gene-related peptide and substance p in esophageal mucosa of patients with non-erosive reflux disease. Dig. Dis. Sci. 2013, 58, 53–60. [Google Scholar] [CrossRef] [PubMed]
- Cheng, L.; de la Monte, S.; Ma, J.; Hong, J.; Tong, M.; Cao, W.; Behar, J.; Biancani, P.; Harnett, K.M. HCl-activated neural and epithelial vanilloid receptors (TRPV1) in cat esophageal mucosa. Am. J. Physiol. Gastrointest. Liver Physiol. 2009, 297, G135–G143. [Google Scholar] [CrossRef] [PubMed]
- Weijenborg, P.W.; Smout, A.J.; Verseijden, C.; van Veen, H.A.; Verheij, J.; de Jonge, W.J.; Bredenoord, A.J. Hypersensitivity to acid is associated with impaired esophageal mucosal integrity in patients with gastroesophageal reflux disease with and without esophagitis. Am. J. Gastroenterol. Gastrointest. Liver Physiol. 2014, 307, 323–329. [Google Scholar] [CrossRef] [PubMed]
- Kandulski, A.; Jechorek, D.; Caro, C.; Weigt, J.; Wex, T.; Monkemuller, K.; Malfertheiner, P. Histomorphological differentiation of non-erosive reflux disease and functional heartburn in patients with ppi-refractory heartburn. Aliment. Pharmacol. Ther. 2013, 38, 643–651. [Google Scholar] [CrossRef] [PubMed]
- Ribolsi, M.; Perrone, G.; Caviglia, R.; Gentile, M.; Emerenziani, S.; Luca Guarino, M.P.; Petitti, T.; Cicala, M. Intercellular space diameters of the oesophageal epithelium in NERD patients: Head to head comparison between light and electron microscopy analysis. Dig. Liver Dis. 2009, 41, 9–14. [Google Scholar] [CrossRef] [PubMed]
- Caviglia, R.; Ribolsi, M.; Gentile, M.; Rabitti, C.; Emerenziani, S.; Guarino, M.P.; Petitti, T.; Cicala, M. Dilated intercellular spaces and acid reflux at the distal and proximal oesophagus in patients with non-erosive gastro-oesophageal reflux disease. Aliment. Pharmacol. Ther. 2007, 25, 629–636. [Google Scholar] [CrossRef] [PubMed]
- Farre, R.; Blondeau, K.; Clement, D.; Vicario, M.; Cardozo, L.; Vieth, M.; Mertens, V.; Pauwels, A.; Silny, J.; Jimenez, M.; et al. Evaluation of oesophageal mucosa integrity by the intraluminal impedance technique. Gut 2011, 60, 885–892. [Google Scholar] [CrossRef] [PubMed]
- Woodland, P.; Lee, C.; Duraisamy, Y.; Farre, R.; Dettmar, P.; Sifrim, D. Assessment and protection of esophageal mucosal integrity in patients with heartburn without esophagitis. Am. J. Gastroenterol. 2013, 108, 535–543. [Google Scholar] [CrossRef] [PubMed]
- Farre, R. Evaluating the esophageal epithelial integrity: More complex than it seems. Am. J. Gastroenterol. 2016, 111, 295–296. [Google Scholar] [CrossRef] [PubMed]
- Jovov, B.; Que, J.; Tobey, N.A.; Djukic, Z.; Hogan, B.L.; Orlando, R.C. Role of E-cadherin in the pathogenesis of gastroesophageal reflux disease. Am. J. Gastroenterol. 2011, 106, 1039–1047. [Google Scholar] [CrossRef] [PubMed]
- Bjorkman, E.; Casselbrant, A.; Lundberg, S.; Fandriks, L. In vitro assessment of epithelial electrical resistance in human esophageal and jejunal mucosae and in caco-2 cell layers. Scand. J. Gastroenterol. 2012, 47, 1321–1333. [Google Scholar] [CrossRef] [PubMed]
- Mancini, V.; Ribolsi, M.; Gentile, M.; de’Angelis, G.; Bizzarri, B.; Lindley, K.J.; Cucchiara, S.; Cicala, M.; Borrelli, O. Oesophageal mucosal intercellular space diameter and reflux pattern in childhood erosive and non-erosive reflux disease. Dig. Liver Dis. 2012, 44, 981–987. [Google Scholar] [CrossRef] [PubMed]
- Kandulski, A.; Weigt, J.; Caro, C.; Jechorek, D.; Wex, T.; Malfertheiner, P. Esophageal intraluminal baseline impedance differentiates gastroesophageal reflux disease from functional heartburn. Clin. Gastroenterol. Hepatol. 2015, 13, 1075–1081. [Google Scholar] [CrossRef] [PubMed]
- Ates, F.; Yuksel, E.S.; Higginbotham, T.; Slaughter, J.C.; Mabary, J.; Kavitt, R.T.; Garrett, C.G.; Francis, D.; Vaezi, M.F. Mucosal impedance discriminates GERD from non-GERD conditions. Gastroenterology 2015, 148, 334–343. [Google Scholar] [CrossRef] [PubMed]
- Shan, J.; Oshima, T.; Fukui, H.; Watari, J.; Miwa, H. Acidic deoxycholic acid and chenodeoxycholic acid induce interleukin-8 production through p38 mitogen-activated protein kinase and protein kinase a in a squamous epithelial model. J. Gastroenterol. Hepatol. 2013, 28, 823–828. [Google Scholar] [CrossRef] [PubMed]
- Shan, J.; Oshima, T.; Muto, T.; Yasuda, K.; Fukui, H.; Watari, J.; Nakanishi, K.; Miwa, H. Epithelial-derived nuclear IL-33 aggravates inflammation in the pathogenesis of reflux esophagitis. J. Gastroenterol. 2015, 50, 414–423. [Google Scholar] [CrossRef] [PubMed]
- Isomoto, H.; Saenko, V.A.; Kanazawa, Y.; Nishi, Y.; Ohtsuru, A.; Inoue, K.; Akazawa, Y.; Takeshima, F.; Omagari, K.; Miyazaki, M.; et al. Enhanced expression of interleukin-8 and activation of nuclear factor κB in endoscopy-negative gastroesophageal reflux disease. Am. J. Gastroenterol. 2004, 99, 589–597. [Google Scholar] [CrossRef] [PubMed]
- Monkemuller, K.; Wex, T.; Kuester, D.; Fry, L.C.; Peitz, U.; Beyer, M.; Roessner, A.; Malfertheiner, P. Interleukin-1β and interleukin-8 expression correlate with the histomorphological changes in esophageal mucosa of patients with erosive and non-erosive reflux disease. Digestion 2009, 79, 186–195. [Google Scholar] [PubMed]
- Altomare, A.; Ma, J.; Guarino, M.P.; Cheng, L.; Rieder, F.; Ribolsi, M.; Fiocchi, C.; Biancani, P.; Harnett, K.; Cicala, M. Platelet-activating factor and distinct chemokines are elevated in mucosal biopsies of erosive compared with non-erosive reflux disease patients and controls. Neurogastroenterol. Motil. 2012, 24, 463–943. [Google Scholar] [CrossRef] [PubMed]
- Fass, R. Non-erosive reflux disease (NERD) and erosive esophagitis—A spectrum of disease or special entities? Z. Gastroenterol. 2007, 45, 1156–1163. [Google Scholar] [CrossRef] [PubMed]
- Rinsma, N.F.; Farre, R.; Bouvy, N.D.; Masclee, A.A.; Conchillo, J.M. The effect of endoscopic fundoplication and proton pump inhibitors on baseline impedance and heartburn severity in GERD patients. Neurogastroenterol. Motil. 2015, 27, 220–228. [Google Scholar] [CrossRef] [PubMed]
- Kessing, B.F.; Bredenoord, A.J.; Weijenborg, P.W.; Hemmink, G.J.; Loots, C.M.; Smout, A.J. Esophageal acid exposure decreases intraluminal baseline impedance levels. Am. J. Gastroenterol. 2011, 106, 2093–2097. [Google Scholar] [CrossRef] [PubMed]
- Pardon, N; Blondeau, K; Vanheel, H; Vicario, M; Vanuytsel, T; Keita, A; Tack, J; Farré, R. In vivo and in vitro evaluation of esophageal mucosal integrity in healthy humans and GERD patients. Gastroenterology 2012, 142, S146–S147. [Google Scholar] [CrossRef]
- Woodland, P.; Al-Zinaty, M.; Yazaki, E.; Sifrim, D. In vivo evaluation of acid-induced changes in oesophageal mucosa integrity and sensitivity in non-erosive reflux disease. Gut 2013, 62, 1256–1261. [Google Scholar] [CrossRef] [PubMed]
- Guarino, M.P.; Cheng, L.; Ma, J.; Harnett, K.; Biancani, P.; Altomare, A.; Panzera, F.; Behar, J.; Cicala, M. Increased TRPV1 gene expression in esophageal mucosa of patients with non-erosive and erosive reflux disease. Neurogastroenterol. Motil. 2010, 22, 746–751. [Google Scholar] [CrossRef] [PubMed]
- Matthews, P.J.; Aziz, Q.; Facer, P.; Davis, J.B.; Thompson, D.G.; Anand, P. Increased capsaicin receptor TRPV1 nerve fibres in the inflamed human oesophagus. Eur. J. Gastroenterol. Hepatol. 2004, 16, 897–902. [Google Scholar] [CrossRef] [PubMed]
- Bhat, Y.M.; Bielefeldt, K. Capsaicin receptor (TRPV1) and non-erosive reflux disease. Eur. J. Gastroenterol. Hepatol. 2006, 18, 263–270. [Google Scholar] [CrossRef] [PubMed]
- Fujino, K.; de la Fuente, S.G.; Takami, Y.; Takahashi, T.; Mantyh, C.R. Attenuation of acid induced oesophagitis in VR-1 deficient mice. Gut 2006, 55, 34–40. [Google Scholar] [CrossRef] [PubMed]
- Szallasi, A.; Nilsson, S.; Farkas-Szallasi, T.; Blumberg, P.M.; Hokfelt, T.; Lundberg, J.M. Vanilloid (capsaicin) receptors in the rat: Distribution in the brain, regional differences in the spinal cord, axonal transport to the periphery, and depletion by systemic vanilloid treatment. Brain Res. 1995, 703, 175–183. [Google Scholar] [CrossRef]
- Matsumoto, K.; Hosoya, T.; Ishikawa, E.; Tashima, K.; Amagase, K.; Kato, S.; Murayama, T.; Horie, S. Distribution of transient receptor potential cation channel subfamily v member 1-expressing nerve fibers in mouse esophagus. Histochem. Cell Biol. 2014, 142, 635–644. [Google Scholar] [CrossRef] [PubMed]
- Bhalla, V.; Liu, J.; Puckett, J.L.; Mittal, R.K. Symptom hypersensitivity to acid infusion is associated with hypersensitivity of esophageal contractility. Am. J. Physiol. Gastrointest. Liver Physiol. 2004, 287, 65–71. [Google Scholar] [CrossRef] [PubMed]
- Pehlivanov, N.; Liu, J.; Mittal, R.K. Sustained esophageal contraction: A motor correlate of heartburn symptom. Am. J. Physiol. Gastrointest. Liver Physiol. 2001, 281, 743–751. [Google Scholar]
- Woodland, P.; Aktar, R.; Mthunzi, E.; Lee, C.; Peiris, M.; Preston, S.L.; Blackshaw, L.A.; Sifrim, D. Distinct afferent innervation patterns within the human proximal and distal esophageal mucosa. Am. J. Physiol. Gastrointest. Liver Physiol. 2015, 308, 525–531. [Google Scholar] [CrossRef] [PubMed]
- Shaw, M.J.; Talley, N.J.; Beebe, T.J.; Rockwood, T.; Carlsson, R.; Adlis, S.; Fendrick, A.M.; Jones, R.; Dent, J.; Bytzer, P. Initial validation of a diagnostic questionnaire for gastroesophageal reflux disease. Am. J. Gastroenterol. 2001, 96, 52–57. [Google Scholar] [CrossRef] [PubMed]
- Keszthelyi, D.; Troost, F.J.; Jonkers, D.M.; Helyes, Z.; Hamer, H.M.; Ludidi, S.; Vanhoutvin, S.; Venema, K.; Dekker, J.; Szolcsanyi, J.; et al. Alterations in mucosal neuropeptides in patients with irritable bowel syndrome and ulcerative colitis in remission: A role in pain symptom generation? Eur. J. Pain 2013, 17, 1299–1306. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| EE n = 11 | NERD n = 10 | HV n = 10 | |
|---|---|---|---|
| Age (range) years | 63 (45–77) | 48 (28–70) | 35 (21–65) |
| Male:female ratio | 6:5 | 7:3 | 5:5 |
| Esophagitis on study endoscopy | 11/11 | 0/10 | 0/10 |
| PPI-use | 11/11 | 10/10 | 0/10 |
| Heartburn score (SD) | 2.8 (1.6) | 2.7 (2.3) | 0 (SD 0) |
| Regurgitation score (SD) | 2.6 (1.5) | 2.3 (2.0) | 0 (SD 0) |
| Pathologic acid exposure time (>4%) on 24-h MII-pH monitoring | n/a | 6/10 | n/a |
| EE | NERD | HVs | p-Value | |
|---|---|---|---|---|
| Claudin-1 | 1.28 (0.32) | 1.80 (0.29) | 1.25 (0.28) | 0.35 |
| Claudin-4 | 0.93 (0.15) | 1.02 (0.34) | 0.93 (0.21) | 0.88 |
| Occludin | 1.70 (0.35) | 1.92 (0.35) | 1.47 (0.17) | 0.53 |
| E-cadherin | 1.25 (0.38) | 1.18 (0.37) | 1.23 (0.23) | 0.99 |
| ZO-1 | 2.42 (0.38) | 2.02 (0.37) | 1.99 (0.23) | 0.61 |
© 2017 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rinsma, N.F.; Farré, R.; Troost, F.J.; Elizalde, M.; Keszthelyi, D.; Helyes, Z.; Masclee, A.A.; Conchillo, J.M. Exploration of the Esophageal Mucosal Barrier in Non-Erosive Reflux Disease. Int. J. Mol. Sci. 2017, 18, 1091. https://doi.org/10.3390/ijms18051091
Rinsma NF, Farré R, Troost FJ, Elizalde M, Keszthelyi D, Helyes Z, Masclee AA, Conchillo JM. Exploration of the Esophageal Mucosal Barrier in Non-Erosive Reflux Disease. International Journal of Molecular Sciences. 2017; 18(5):1091. https://doi.org/10.3390/ijms18051091
Chicago/Turabian StyleRinsma, Nicolaas F., Ricard Farré, Fred J. Troost, Montserrat Elizalde, Daniel Keszthelyi, Zsuzsanna Helyes, Ad A. Masclee, and José M. Conchillo. 2017. "Exploration of the Esophageal Mucosal Barrier in Non-Erosive Reflux Disease" International Journal of Molecular Sciences 18, no. 5: 1091. https://doi.org/10.3390/ijms18051091
APA StyleRinsma, N. F., Farré, R., Troost, F. J., Elizalde, M., Keszthelyi, D., Helyes, Z., Masclee, A. A., & Conchillo, J. M. (2017). Exploration of the Esophageal Mucosal Barrier in Non-Erosive Reflux Disease. International Journal of Molecular Sciences, 18(5), 1091. https://doi.org/10.3390/ijms18051091