Caloric Restriction and Its Effect on Blood Pressure, Heart Rate Variability and Arterial Stiffness and Dilatation: A Review of the Evidence

Abstract
:1. Introduction
2. Caloric Restriction: Effects on Lowering Systolic and Diastolic Blood Pressure
2.1. Multivariate Regression Correlates with Blood Pressure Lowering
2.2. Does a Baseline Diagnosis of Metabolic Syndrome Influence the Effectiveness of CR?
2.3. Does a Baseline Diagnosis of Hypertension or Pre-Hypertension Influence the Effectiveness of CR?
2.4. Does Ethnicity Influence the Effectiveness of CR in Blood Pressure Lowering?
2.5. Is DBP Slower to Respond to CR Than SBP?
3. Caloric Restriction: Effects on Lowering of Heart Rate
4. Caloric Restriction: Effects on Heart Rate Variability and Autonomic Nervous System Balance
5. Caloric Restriction: Effects on Pulse Wave Velocity
6. Caloric Restriction: Effects on Endothelium-Dependent Flow-Mediated Dilatation
Multivariate Regression Correlates with Endothelium-Dependent Flow-Mediated Dilatation Improvement
7. Caloric Restriction: Effects on Endothelium-Independent Flow-Mediated Dilatation
8. Summary of Findings
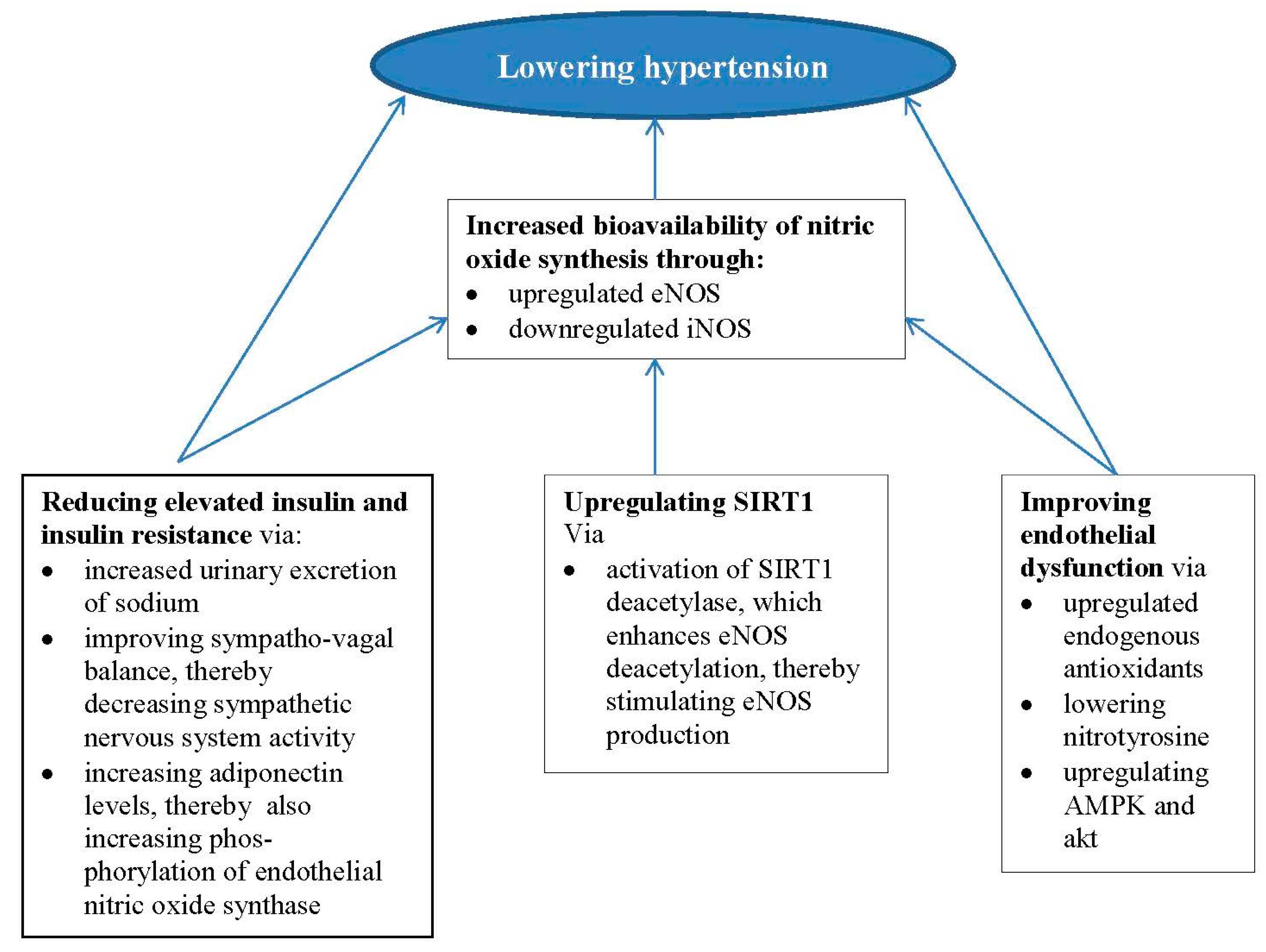
9. Potential Mechanisms
9.1. The Role of Insulin and Insulin Resistance
9.2. The Role of Endothelial Dysfunction
9.3. The Role of SIRT1
10. Conclusions
Conflicts of Interest
References
- Poulter, N.R.; Prabhakaran, D.; Caulfield, M. Hypertension. Lancet 2015, 386, 801–812. [Google Scholar] [CrossRef]
- Carretero, O.A.; Oparil, S. Essential hypertension. Part I: Definition and etiology. Circulation 2000, 101, 329–335. [Google Scholar] [CrossRef] [PubMed]
- Spelta, F.; Bertozzi, B.; Cominacini, L.; Fontana, L. Calorie restriction, endothelial function and blood pressure homeostasis. Vasc. Pharmacol. 2015, 65–66. [Google Scholar] [CrossRef] [PubMed]
- Blumenthal, J.A.; Babyak, M.A.; Sherwood, A.; Craighead, L.; Lin, P.H.; Johnson, J.; Watkins, L.L.; Wang, J.T.; Kuhn, C.; Feinglos, M.; et al. Effects of the dietary approaches to stop hypertension diet alone and in combination with exercise and caloric restriction on insulin sensitivity and lipids. Hypertension 2010, 55, 1199–1205. [Google Scholar] [CrossRef] [PubMed]
- Messerli, F.H.; Williams, B.; Ritz, E. Essential hypertension. Lancet 2007, 370, 591–603. [Google Scholar] [CrossRef]
- Mertens, I.L.; Van Gaal, L.F. Overweight, obesity, and blood pressure: The effects of modest weight reduction. Obes. Res. 2000, 8, 270–278. [Google Scholar] [CrossRef] [PubMed]
- Caetano, J.; Delgado Alves, J. Heart rate and cardiovascular protection. Eur. J. Intern. Med. 2015, 26, 217–222. [Google Scholar] [CrossRef] [PubMed]
- Stein, P.K.; Soare, A.; Meyer, T.E.; Cangemi, R.; Holloszy, J.O.; Fontana, L. Caloric restriction may reverse age-related autonomic decline in humans. Aging Cell 2012, 11, 644–650. [Google Scholar] [CrossRef] [PubMed]
- Hillis, G.S.; Woodward, M.; Rodgers, A.; Chow, C.K.; Li, Q.; Zoungas, S.; Patel, A.; Webster, R.; Batty, G.D.; Ninomiya, T.; et al. Resting heart rate and the risk of death and cardiovascular complications in patients with type 2 diabetes mellitus. Diabetologia 2012, 55, 1283–1290. [Google Scholar] [CrossRef] [PubMed]
- Hillis, G.S.; Hata, J.; Woodward, M.; Perkovic, V.; Arima, H.; Chow, C.K.; Zoungas, S.; Patel, A.; Poulter, N.R.; Mancia, G. Resting heart rate and the risk of microvascular complications in patients with type 2 diabetes mellitus. J. Am. Heart Assoc. 2012, 1, e002832. [Google Scholar] [CrossRef] [PubMed]
- Dekker, J.M.; Girman, C.; Rhodes, T.; Perkovic, V.; Arima, H.; Chow, C.K.; Zoungas, S.; Patel, A.; Poulter, N.R.; Mancia, G.; et al. Metabolic syndrome and 10-year cardiovascular disease risk in the Hoorn Study. Circulation 2005, 112, 666–673. [Google Scholar] [CrossRef] [PubMed]
- Mitchell, G.F.; Hwang, S.J.; Vasan, R.S.; Larson, M.G.; Pencina, M.J.; Hamburg, N.M.; Vita, J.A.; Levy, D.; Benjamin, E.J. Arterial stiffness and cardiovascular events: The framingham heart study. Circulation 2010, 121, 505–511. [Google Scholar] [CrossRef] [PubMed]
- Raitakari, O.T.; Celermajer, D.S. Testing for endothelial dysfunction. Ann. Med. 2000, 32, 293–304. [Google Scholar] [CrossRef] [PubMed]
- Green, D.J.; Jones, H.; Thijssen, D.; Cable, N.T.; Atkinson, G. Flow-Mediated Dilation and Cardiovascular Event Prediction—Does Nitric Oxide Matter? Hypertension 2011, 57, 363–369. [Google Scholar] [CrossRef] [PubMed]
- Klempel, M.C.; Kroeger, C.M.; Norkeviciute, E.; Goslawski, M.; Phillips, S.A.; Varady, K.A. Benefit of a low-fat over high-fat diet on vascular health during alternate day fasting. Nutr. Diabetes 2013, 3. [Google Scholar] [CrossRef] [PubMed]
- Neal, B.; MacMahon, S.; Chapman, N. Blood Pressure Lowering Treatment Trialists C. Effects of ACE inhibitors, calcium antagonists, and other blood-pressure-lowering drugs: Results of prospectively designed overviews of randomised trials. Blood Pressure Lowering Treatment Trialists’ Collaboration. Lancet 2000, 356, 1955–1964. [Google Scholar] [PubMed]
- Joint National Committee on Prevention, Evaluation, and Treatment of High Blood Pressure. The Seventh Report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure; NIH Publication 04-5230; US Department of Health and Human Services: Bethesda, MD, USA, 2004.
- Appel, L.J.; Moore, T.J.; Obarzanek, E.; Vollmer, W.M.; Svetkey, L.P.; Sacks, F.M.; Bray, G.A.; Vogt, T.M.; Cutler, J.A.; Windhauser, M.M.; et al. A clinical trial of the effects of dietary patterns on blood pressure. DASH Collaborative Research Group. N. Engl. J. Med. 1997, 336, 1117–1124. [Google Scholar] [CrossRef] [PubMed]
- Sacks, F.M.; Svetkey, L.P.; Vollmer, W.M.; Appel, L.J.; Bray, G.A.; Harsha, D.; Obarzanek, E.; Conlin, P.R.; Miller, E.R., 3rd; Simons-Morton, D.G.; et al. Effects on blood pressure of reduced dietary sodium and the Dietary Approaches to Stop Hypertension (DASH) diet. DASH-Sodium Collaborative Research Group. N. Engl. J. Med. 2001, 344, 3–10. [Google Scholar] [CrossRef] [PubMed]
- Raitakari, M.; Ilvonen, T.; Ahotupa, M.; Lehtimäki, T.; Harmoinen, A.; Suominen, P.; Elo, J.; Hartiala, J.; Raitakari, O.T. Weight reduction with very-low-caloric diet and endothelial function in overweight adults: Role of plasma glucose. Arterioscler. Thromb. Vasc. Biol. 2004, 24, 124–128. [Google Scholar] [CrossRef] [PubMed]
- Ruggenenti, P.; Abbate, M.; Ruggiero, B.; Rota, S.; Trillini, M.; Aparicio, C.; Parvanova, A.; Iliev, I.P.; Pisanu, G.; Perna, A.; et al. Renal and Systemic Effects of Calorie Restriction in Type-2 Diabetes Patients with Abdominal Obesity: A Randomized Controlled Trial. Diabetes 2017, 66, 75–86. [Google Scholar] [CrossRef] [PubMed]
- Li, C.; Sadraie, B.; Steckhan, N.; Kessler, C.; Stange, R.; Jeitler, M.; Michalsen, A. Effects of A One-week Fasting Therapy in Patients with Type-2 Diabetes Mellitus and Metabolic Syndrome—A Randomized Controlled Explorative Study. Exp. Clin. Endocrinol. Diabetes 2017. [Google Scholar] [CrossRef] [PubMed]
- Van Schinkel, L.D.; Bakker, L.E.; Jonker, J.T.; De Roos, A.; Pijl, H.; Meinders, A.E.; Jazet, I.M.; Lamb, H.J.; Smit, J.W. Cardiovascular flexibility in middle-aged overweight South Asians vs. white Caucasians: Response to short-term caloric restriction. Nutr. Metab. Cardiovasc. Dis. 2015, 25, 403–410. [Google Scholar] [CrossRef] [PubMed]
- Hong, K.; Li, Z.; Wang, H.J.; Elashoff, R.; Heber, D. Analysis of weight loss outcomes using VLCD in black and white overweight and obese women with and without metabolic syndrome. Int. J. Obes. 2005, 29, 436–442. [Google Scholar] [CrossRef] [PubMed]
- Jakobsdottir, S.; van Nieuwpoort, I.C.; van Bunderen, C.C.; de Ruiter, M.B.; Twisk, J.W.; Deijen, J.B.; Veltman, D.J.; Drent, M.L. Acute and short-term effects of caloric restriction on metabolic profile and brain activation in obese, postmenopausal women. Int. J. Obes. 2016, 40, 1671–1678. [Google Scholar] [CrossRef] [PubMed]
- Most, J.; Gilmore, L.A.; Smith, S.R.; Han, H.; Ravussin, E.; Redman, L.M. Significant Improvement in Cardiometabolic Health in Healthy Non-Obese Individuals during Caloric Restriction-induced Weight Loss and Weight Loss Maintenance. Am. J. Physiol. Endocrinol. Metab. 2017. [Google Scholar] [CrossRef] [PubMed]
- Li, C.; Ostermann, T.; Hardt, M.; Lüdtke, R.; Broecker-Preuss, M.; Dobos, G.; Michalsen, A. Metabolic and psychological response to 7-day fasting in obese patients with and without metabolic syndrome. Forschende Komplementarmedizin 2013, 20, 413–420. [Google Scholar] [CrossRef] [PubMed]
- Walford, R.L.; Mock, D.; Verdery, R.; MacCallum, T. Calorie restriction in biosphere 2: Alterations in physiologic, hematologic, hormonal, and biochemical parameters in humans restricted for a 2-year period. J. Gerontol. A Biol. Sci. Med. Sci. 2002, 57, B211–B224. [Google Scholar] [CrossRef] [PubMed]
- Erdem, Y.; Özkan, G.; Ulusoy, Ş.; Arıcı, M.; Derici, Ü.; Şengül, Ş.; Sindel, Ş.; Ertürk, Ş. Turkish Society of Hypertension and Renal Diseases. The effect of intermittent fasting on blood pressure variability in patients with newly diagnosed hypertension or prehypertension. J. Am. Soc. Hypertens. 2018, 12, 42–49. [Google Scholar] [CrossRef] [PubMed]
- Kawamura, M.; Adachi, T.; Nakajima, J.; Fujiwara, T.; Hiramori, K. Factors that affect calorie-sensitive and calorie-insensitive reduction in blood pressure during short-term calorie restriction in overweight hypertensive women. Hypertension 1996, 27, 408–413. [Google Scholar] [CrossRef] [PubMed]
- Case, C.C.; Jones, P.H.; Nelson, K.; O’Brian Smith, E.; Ballantyne, C.M. Impact of weight loss on the metabolic syndrome. Diabetes Obes. Metab. 2002, 4, 407–414. [Google Scholar] [CrossRef] [PubMed]
- Beleslin, B.; Cirić, J.; Zarković, M.; Vujović, S.; Trbojević, B.; Drezgić, M. The effects of three-week fasting diet on blood pressure, lipid profile and glucoregulation in extremely obese patients. Srpski Arhiv Za Celokupno Lekarstvo 2007, 135, 440–446. [Google Scholar] [CrossRef] [PubMed]
- Sasaki, S.; Higashi, Y.; Nakagawa, K.; Kimura, M.; Noma, K.; Sasaki, S.; Hara, K.; Matsuura, H.; Goto, C.; Oshima, T.; et al. A low-calorie diet improves endothelium-dependent vasodilation in obese patients with essential hypertension. Am. J. Hypertens. 2002, 15, 302–309. [Google Scholar] [CrossRef]
- Goldhamer, A.C.; Lisle, D.J.; Sultana, P.; Anderson, S.V.; Parpia, B.; Hughes, B.; Campbell, T.C. Medically supervised water-only fasting in the treatment of borderline hypertension. J. Altern. Complement. Med. 2002, 8, 643–650. [Google Scholar] [CrossRef] [PubMed]
- Goldhamer, A.; Lisle, D.; Parpia, B.; Anderson, S.V.; Campbell, T.C. Medically supervised water-only fasting in the treatment of hypertension. J. Manip. Physiol. Ther. 2001, 24, 335–339. [Google Scholar] [CrossRef] [PubMed]
- Ghachem, A.; Prudhomme, D.; Rabasa-Lhoret, R.; Brochu, M. Effects of a 6-month caloric restriction induced-weight loss program in obese postmenopausal women with and without the metabolic syndrome: A MONET study. Menopause 2017, 24, 908–915. [Google Scholar] [CrossRef] [PubMed]
- Volek, J.S.; Feinman, R.D. Carbohydrate restriction improves the features of Metabolic Syndrome. Metabolic Syndrome may be defined by the response to carbohydrate restriction. Nutr. Metab. 2005, 2, 31. [Google Scholar] [CrossRef] [PubMed]
- Nicoll, R. Reversal of obesity: The quest for the optimum dietary regimen. Int. J. Nutr. 2017, 2, 24. [Google Scholar] [CrossRef]
- Eshghinia, S.; Mohammadzadeh, F. The effects of modified alternate-day fasting diet on weight loss and CAD risk factors in overweight and obese women. J. Diabetes Metab. Disord. 2013, 12, 4. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hoddy, K.K.; Bhutani, S.; Phillips, S.A.; Varady, K.A. Effects of different degrees of insulin resistance on endothelial function in obese adults undergoing alternate day fasting. Nutr. Healthy Aging 2016, 4, 63–71. [Google Scholar] [CrossRef] [PubMed]
- Varady, K.A.; Bhutani, S.; Church, E.C.; Klempel, M.C. Short-term modified alternate-day fasting: A novel dietary strategy for weight loss and cardioprotection in obese adults. Am. J. Clin. Nutr. 2009, 90, 1138–1143. [Google Scholar] [CrossRef] [PubMed]
- Hoddy, K.K.; Kroeger, C.M.; Trepanowski, J.F.; Barnosky, A.; Bhutani, S.; Varady, K.A. Meal timing during alternate day fasting: Impact on body weight and cardiovascular disease risk in obese adults. Obesity 2014, 22, 2524–2531. [Google Scholar] [CrossRef] [PubMed]
- Bhutani, S.; Klempel, M.C.; Kroeger, C.M.; Trepanowski, J.F.; Varady, K.A. Alternate day fasting and endurance exercise combine to reduce body weight and favorably alter plasma lipids in obese humans. Obesity 2013, 21, 1370–1379. [Google Scholar] [CrossRef] [PubMed]
- Kessler, C.S.; Stange, R.; Schlenkermann, M.; Jeitler, M.; Michalsen, A.; Selle, A.; Raucci, F.; Steckhan, N. A nonrandomized controlled clinical pilot trial on 8 wk of intermittent fasting (24 h/wk). Nutrition 2017. [Google Scholar] [CrossRef] [PubMed]
- Harvie, M.N.; Pegington, M.; Mattson, M.P.; Frystyk, J.; Dillon, B.; Evans, G.; Cuzick, J.; Jebb, S.A.; Martin, B.; Cutler, R.G.; et al. The effects of intermittent or continuous energy restriction on weight loss and metabolic disease risk markers: A randomized trial in young overweight women. Int. J. Obes. 2011, 35, 714–727. [Google Scholar] [CrossRef] [PubMed]
- Meyer, T.E.; Kovács, S.J.; Ehsani, A.A.; Klein, S.; Holloszy, J.O.; Fontana, L. Long-term caloric restriction ameliorates the decline in diastolic function in humans. J. Am. Coll. Cardiol. 2006, 47, 398–402. [Google Scholar] [CrossRef] [PubMed]
- Fontana, L.; Meyer, T.E.; Klein, S.; Holloszy, J.O. Long-term calorie restriction is highly effective in reducing the risk for atherosclerosis in humans. Proc. Natl. Acad. Sci. USA 2004, 101, 6659–6663. [Google Scholar] [CrossRef] [PubMed]
- Williams, C.L.; Hayman, L.L.; Daniels, S.R.; Robinson, T.N.; Steinberger, J.; Paridon, S.; Bazzarre, T.; American Heart Association. Cardiovascular health in childhood: A statement for health professionals on atherosclerosis, hypertension, and obesity in the young (AHOY) of the Council on Cardiovascular Disease in the Young. Circulation 2002, 106, 143–160. [Google Scholar] [CrossRef] [PubMed]
- Klempel, M.C.; Kroeger, C.M.; Bhutani, S.; Trepanowski, J.F.; Varady, K.A. Intermittent fasting combined with calorie restriction is effective for weight loss and cardio-protection in obese women. Nutr. J. 2012, 11, 98. [Google Scholar] [CrossRef] [PubMed]
- Meckling, K.A.; Sherfey, R. A randomized trial of a hypocaloric high-protein diet, with and without exercise, on weight loss, fitness, and markers of the Metabolic Syndrome in overweight and obese women. Appl. Physiol. Nutr. Metab. 2007, 32, 743–752. [Google Scholar] [CrossRef] [PubMed]
- Klempel, M.C.; Kroeger, C.M.; Varady, K.A. Alternate day fasting (ADF) with a high-fat diet produces similar weight loss and cardio-protection as ADF with a low-fat diet. Metabolism 2013, 62, 137–143. [Google Scholar] [CrossRef] [PubMed]
- Trepanowski, J.F.; Kroeger, C.M.; Barnosky, A.; Klempel, M.C.; Bhutani, S.; Hoddy, K.K.; Gabel, K.; Freels, S.; Rigdon, J.; Rood, J.; et al. Effect of Alternate-Day Fasting on Weight Loss, Weight Maintenance, and Cardioprotection Among Metabolically Healthy Obese Adults: A Randomized Clinical Trial. JAMA Intern. Med. 2017. [Google Scholar] [CrossRef] [PubMed]
- De Jonge, L.; Moreira, E.A.; Martin, C.K.; Ravussin, E.; Pennington CALERIE Team. Impact of 6-month caloric restriction on autonomic nervous system activity in healthy, overweight, individuals. Obesity 2010, 18, 414–416. [Google Scholar] [CrossRef] [PubMed]
- Yassine, H.N.; Marchetti, C.M.; Krishnan, R.K.; Vrobel, T.R.; Gonzalez, F.; Kirwan, J.P. Effects of exercise and caloric restriction on insulin resistance and cardiometabolic risk factors in older obese adults—A randomized clinical trial. J. Gerontol. A Biol. Sci. Med. Sci. 2009, 64, 90–95. [Google Scholar] [CrossRef] [PubMed]
- Wycherley, T.P.; Brinkworth, G.D.; Noakes, M.; Buckley, J.D.; Clifton, P.M. Effect of caloric restriction with and without exercise training on oxidative stress and endothelial function in obese subjects with type 2 diabetes. Diabetes Obes. Metab. 2008, 10, 1062–1073. [Google Scholar] [CrossRef] [PubMed]
- Thomson, R.L.; Buckley, J.D.; Noakes, M.; Clifton, P.M.; Norman, R.J.; Brinkworth, G.D. The effect of a hypocaloric diet with and without exercise training on body composition, cardiometabolic risk profile, and reproductive function in overweight and obese women with polycystic ovary syndrome. J. Clin. Endocrinol. Metab. 2008, 93, 3373–3380. [Google Scholar] [CrossRef] [PubMed]
- Lefevre, M.; Redman, L.M.; Heilbronn, L.K.; Smith, J.V.; Martin, C.K.; Rood, J.C.; Greenway, F.L.; Williamson, D.A.; Smith, S.R.; Ravussin, E.; et al. Caloric restriction alone and with exercise improves CVD risk in healthy non-obese individuals. Atherosclerosis 2009, 203, 206–213. [Google Scholar] [CrossRef] [PubMed]
- Blumenthal, J.A.; Babyak, M.A.; Hinderliter, A.; Watkins, L.L.; Craighead, L.; Lin, P.-H.; Caccia, C.; Johnson, J.; Waugh, R.A.; Sherwood, A. Effects of the DASH diet alone and in combination with exercise and weight loss on blood pressure and cardiovascular biomarkers in men and women with high blood pressure: The ENCORE Study. Arch. Intern. Med. 2010, 170, 126–135. [Google Scholar] [CrossRef] [PubMed]
- Law, M.R.; Wald, N.J.; Morris, J.K.; Jordan, R.E. Value of low dose combination treatment with blood pressure lowering drugs: Analysis of 354 randomised trials. BMJ 2003, 326, 1427. [Google Scholar] [CrossRef] [PubMed]
- Nakano, Y.; Oshima, T.; Sasaki, S.; Higashi, Y.; Ozono, R.; Takenaka, S.; Miura, F.; Hirao, H.; Matsuura, H.; Chayama, K.; et al. Calorie restriction reduced blood pressure in obesity hypertensives by improvement of autonomic nerve activity and insulin sensitivity. J. Cardiovasc. Pharmacol. 2001, 38 (Suppl. S1), S69–S74. [Google Scholar] [CrossRef] [PubMed]
- Weiss, E.P.; Albert, S.G.; Reeds, D.N.; Kress, K.S.; McDaniel, J.L.; Klein, S.; Villareal, D.T. Effects of matched weight loss from calorie restriction, exercise, or both on cardiovascular disease risk factors: A randomized intervention trial. Am. J. Clin. Nutr. 2016, 104, 576–586. [Google Scholar] [CrossRef] [PubMed]
- Facchini, M.; Malfatta, F.; Salba, L.; Fontana, P.; Lafortuna, C.; Sartorio, A. Changes of autonomic cardiac profileafter a 3 week integrated body weight reduction program in severely obese patients. J. Endocrinol. Investig. 2003, 26, 138–142. [Google Scholar] [CrossRef] [PubMed]
- Herlihy, J.T.; Stacy, C.; Bertrand, H.A. Long-term calorie restriction enhances baroreflex responsiveness in Fischer 344 rats. Am. J. Physiol. 1992, 263, H1021–H1025. [Google Scholar] [CrossRef] [PubMed]
- Mager, D.E.; Wan, R.; Brown, M.; Cheng, A.; Wareski, P.; Abernethy, D.R.; Mattson, M.P. Caloric restriction and intermittent fasting alter spectral measures of heart rate and blood pressure variability in rats. FASEB J. 2006, 20, 631–637. [Google Scholar] [CrossRef] [PubMed]
- Petersen, K.S.; Blanch, N.; Keogh, J.B.; Clifton, P.M. Effect of weight loss on pulse wave velocity: Systematic review and meta-analysis. Arterioscler. Thromb. Vasc. Biol. 2015, 35, 243–252. [Google Scholar] [CrossRef] [PubMed]
- Donato, A.J.; Walker, A.E.; Magerko, K.A.; Bramwell, R.C.; Black, A.D.; Henson, G.D.; Lawson, B.R.; Lesniewski, L.A.; Seals, D.R. Life-long caloric restriction reduces oxidative stress and preserves nitric oxide bioavailability and function in arteries of old mice. Aging Cell 2013, 12, 772–783. [Google Scholar] [CrossRef] [PubMed]
- Khoo, J.; Piantadosi, C.; Duncan, R.; Worthley, S.G.; Jenkins, A.; Noakes, M.; Worthley, M.I.; Lange, K.; Wittert, G.A. Comparing effects of a low-energy diet and a high-protein low-fat diet on sexual and endothelial function, urinary tract symptoms, and inflammation in obese diabetic men. J. Sex. Med. 2011, 8, 2868–2875. [Google Scholar] [CrossRef] [PubMed]
- Clifton, P.M.; Keogh, J.B.; Foster, P.R.; Noakes, M. Effect of weight loss on inflammatory and endothelial markers and FMD using two low-fat diets. Int. J. Obes. 2005, 29, 1445–1451. [Google Scholar] [CrossRef] [PubMed]
- Volek, J.S.; Ballard, K.D.; Silvestre, R.; Judelson, D.A.; Quann, E.E.; Forsythe, C.E.; Fernandez, M.L.; Kraemer, W.J. Effects of dietary carbohydrate restriction versus low-fat diet on flow-mediated dilation. Metabolism 2009, 58, 1769–1777. [Google Scholar] [CrossRef] [PubMed]
- Green, D.J.; Maiorana, A.J.; Tschakovsky, M.E.; Pyke, K.E.; Weisbrod, C.J.; O’Driscoll, G. Relationship between changes in brachial artery flow-mediated dilation and basal release of nitric oxide in subjects with type 2 diabetes. Am. J. Physiol. Heart Circ. Physiol. 2006, 291, H1193–H1199. [Google Scholar] [CrossRef] [PubMed]
- Sakamoto, S.; Minami, K.; Niwa, Y.; Ohnaka, M.; Nakaya, Y.; Mizuno, A.; Kuwajima, M.; Shima, K. Effect of exercise training and food restriction on endothelium-dependent relaxation in the Otsuka Long-Evans Tokushima Fatty rat, a model of spontaneous NIDDM. Diabetes 1998, 47, 82–86. [Google Scholar] [CrossRef] [PubMed]
- Galvao, R.; Plavnik, F.L.; Ribeiro, F.F.; Ajzen, S.A.; Christofalo, D.M.; Kohlmann, O., Jr. Effects of different degrees of insulin sensitivity on endothelial function in obese patients. Arquivos Brasileiros Cardiologia 2012, 98, 45–51. [Google Scholar]
- Sciacqua, A.; Candigliota, M.; Ceravolo, R.; Scozzafava, A.; Sinopoli, F.; Corsonello, A.; Sesti, G.; Perticone, F. Weight loss in combination with physical activity improves endothelial dysfunction in human obesity. Diabetes Care 2003, 26, 1673–1678. [Google Scholar] [CrossRef] [PubMed]
- Reaven, G.M. Relationships among Insulin Resistance, Type 2 Diabetes, Essential Hypertension, and Cardiovascular Disease: Similarities and Differences. J. Clin. Hypertens. 2011, 13, 238–243. [Google Scholar] [CrossRef] [PubMed]
- Lima, N.K.; Abbasi, F.; Lamendola, C.; Reaven, G.M. Prevalence of insulin resistance and related risk factors for cardiovascular disease in patients with essential hypertension. Am. J. Hypertens. 2009, 22, 106–111. [Google Scholar] [CrossRef] [PubMed]
- Jung, C.H.; Jung, S.H.; Lee, B.; Rosenberg, M.; Reaven, G.M.; Kim, S.H. Relationship among age, insulin resistance, and blood pressure. J. Am. Soc. Hypertens. 2017, 11, 359–365. [Google Scholar] [CrossRef] [PubMed]
- Emdin, M.; Gastaldelli, A.; Muscelli, E.; Macerata, A.; Natali, A.; Camastra, S.; Ferrannini, E. Hyperinsulinemia and autonomic nervous system dysfunction in obesity: Effects of weight loss. Circulation 2001, 103, 513–519. [Google Scholar] [CrossRef] [PubMed]
- Arcaro, G.; Cretti, A.; Balzano, S.; Lechi, A.; Muggeo, M.; Bonora, E.; Bonadonna, R.C. Insulin causes endothelial dysfunction in humans: Sites and mechanisms. Circulation 2002, 105, 576–582. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.A.; Montagnani, M.; Koh, K.K.; Quon, M.J. Reciprocal relationships between insulin resistance and endothelial dysfunction: Molecular and pathophysiological mechanisms. Circulation 2006, 113, 1888–1904. [Google Scholar] [CrossRef] [PubMed]
- Kuboki, K.; Jiang, Z.Y.; Takahara, N.; Ha, S.W.; Igarashi, M.; Yamauchi, T.; Feener, E.P.; Herbert, T.P.; Rhodes, C.J.; King, G.L. Regulation of endothelial constitutive nitric oxide synthase gene expression in endothelial cells and in vivo: A specific vascular action of insulin. Circulation 2000, 101, 676–681. [Google Scholar] [CrossRef] [PubMed]
- Surdackii, A.; Nowicki, M.; Sandmann, J.; Tsikas, D.; Boeger, R.H.; Bode-Boeger, S.M.; Kruszelnicka-Kwiatkowska, O.; Kokot, F.; Dubiel, J.S.; Froelich, J.C. Reduced urinary secretion of nitric oxide metabolites and increased plasma levels of asymmetric dimethylarginine in men with essential hypertension. J. Cardiovasc. Pharmacol. 1999, 33, 652–658. [Google Scholar] [CrossRef]
- Stuhlinger, M.C.; Abbasi, F.; Chu, J.W.; Chu, J.W. Relationship between insulin resistance and an endogenous nitiric oxide synthase inhibitor. JAMA 2002, 287, 1420–1426. [Google Scholar] [CrossRef] [PubMed]
- Karaca, U.; Schram, M.T.; Houben, A.J.; Muris, D.M.; Stehouwer, C.D. Microvascular dysfunction as a link between obesity, insulin resistance and hypertension. Diabetes Res. Clin. Pract. 2014, 103, 382–387. [Google Scholar] [CrossRef] [PubMed]
- McCarty, M.F. A preliminary fast may potentiate response to a subsequent low-salt, low-fat vegan diet in the management of hypertension—Fasting as a strategy for breaking metabolic vicious cycles. Med. Hypotheses 2003, 60, 624–633. [Google Scholar] [CrossRef]
- Tuck, M.L. Obesity, the sympathetic nervous system and essential hypertension. Hypertension 1992, 19 (Suppl. SI), I-67–I-77. [Google Scholar] [CrossRef]
- Ikeda, T.; Gomi, T.; Hirawa, N.; Sakurai, J.; Yoshikawa, N. Improvement of insulin sensitivity contributes to blood pressure reduction after weight loss in hypertensive subjects with obesity. Hypertension 1996, 27, 1180–1186. [Google Scholar] [CrossRef] [PubMed]
- Chen, H.; Montagnani, M.; Funahashi, T.; Shimomura, I.; Quon, M.J. Adiponectin stimulates production of nitric oxide in vascular endothelial cells. J. Biol. Chem. 2003, 278, 45021–45026. [Google Scholar] [CrossRef] [PubMed]
- Anderson, E.A.; Mark, A.L. The vasodilator action of insulin. Implications for the insulin hypothesis of hypertension. Hypertension 1993, 21, 136–141. [Google Scholar] [CrossRef] [PubMed]
- Zavaroni, I.; Ardigo, D.; Rossi, P.C.; Zuccarelli, A.; Pacetti, E.; Monti, L.; Piatti, P.M.; Reaven, G.M. Relationship between plasma nitric oxide concentration and insulin resistance in essential hypertension. Am. J. Hypertens. 2004, 17, 549–552. [Google Scholar] [CrossRef] [PubMed]
- Dolinsky, V.W.; Dyck, J.R. Calorie restriction and resveratrol in cardiovascular health and disease. Biochim. Biophys. Acta 2011, 1812, 1477–1489. [Google Scholar] [CrossRef] [PubMed]
- Chou, S.H.; Lee, Y.C.; Huang, C.F.; Wang, Y.R.; Yu, H.P.; Lau, Y.T. Gender-specific effects of caloric restriction on the balance of vascular nitric oxide and superoxide radical. Cardiovasc. Res. 2010, 87, 751–759. [Google Scholar] [CrossRef] [PubMed]
- Zanetti, M.; Gortan Cappellari, G.; Burekovic, I.; Barazzoni, R.; Stebel, M.; Guarnieri, G. Caloric restriction improves endothelial dysfunction during vascular aging: Effects on nitric oxide synthase isoforms and oxidative stress in rat aorta. Exp. Gerontol. 2010, 45, 848–855. [Google Scholar] [CrossRef] [PubMed]
- Rippe, C.; Lesniewski, L.; Connell, M.; LaRocca, T.; Donato, A.; Seals, D. Short-term calorie restriction reverses vascular endothelial dysfunction in old mice by increasing nitric oxide and reducing oxidative stress. Aging Cell 2010, 9, 304–312. [Google Scholar] [CrossRef] [PubMed]
- Li, R.; Zhang, H.; Wang, W.; Wang, X.; Huang, Y.; Huang, C.; Gao, F. Vascular insulin resistance in prehypertensive rats: Role of PI3-kinase/Akt/eNOS signaling. Eur. J. Pharmacol. 2010, 628, 140–147. [Google Scholar] [CrossRef] [PubMed]
- García-Prieto, C.F.; Pulido-Olmo, H.; Ruiz-Hurtado, G.; Gil-Ortega, M.; Aranguez, I.; Rubio, M.A.; Ruiz-Gayo, M.; Somoza, B.; Fernández-Alfonso, M.S. Mild caloric restriction reduces blood pressure and activates endothelial AMPK-PI3K-Akt-eNOS pathway in obese Zucker rats. Vasc. Pharmacol. 2015, 65–66, 3–12. [Google Scholar] [CrossRef] [PubMed]
- Dolinsky, V.W.; Morton, J.S.; Oka, T.; Robillard-Frayne, I.; Bagdan, M.; Lopaschuk, G.D.; Des Rosiers, C.; Walsh, K.; Davidge, S.T.; Dyck, J.R. Calorie restriction prevents hypertension and cardiac hypertrophy in the spontaneously hypertensive rat. Hypertension 2010, 56, 412–421. [Google Scholar] [CrossRef] [PubMed]
- Korda, M.; Kubant, R.; Patton, S.; Malinski, T. Leptin induced endothelial dysfunction in obesity. Am. J. Physiol. Heart Circ. Physiol. 2008, 295, H1514–H1521. [Google Scholar] [CrossRef] [PubMed]
- Mattagajasingh, I.; Kim, C.S.; Naqvi, A.; Yamamori, T.; Hoffman, T.A.; Jung, S.B.; DeRicco, J.; Kasuno, K.; Irani, K. SIRT1 promotes endothelium-dependent vascular relaxation by activating endothelial nitric oxide synthase. Proc. Natl. Acad. Sci. USA 2007, 104, 14855–14860. [Google Scholar] [CrossRef] [PubMed]
- Gano, L.B.; Donato, A.J.; Pasha, H.M.; Hearon, C.M., Jr.; Sindler, A.L.; Seals, D.R. The SIRT1 activator SRT1720 reverses vascular endothelial dysfunction, excessive superoxide production, and inflammation with aging in mice. Am. J. Physiol. Heart Circ. Physiol. 2014, 307, H1754–H1763. [Google Scholar] [CrossRef] [PubMed]
- Ding, M.; Lei, J.; Qu, Y.; Zhang, H.; Xin, W.; Ma, F.; Liu, S.; Li, Z.; Jin, F.; Fu, E. Calorie Restriction Attenuates Monocrotaline-induced Pulmonary Arterial Hypertension in Rats. J. Cardiovasc. Pharmacol. 2015, 65, 562–570. [Google Scholar] [CrossRef] [PubMed]
- Shinmura, K.; Tamaki, K.; Ito, K.; Yan, X.; Yamamoto, T.; Katsumata, Y.; Matsuhashi, T.; Sano, M.; Fukuda, K.; Suematsu, M.; et al. Indispensable role of endothelial nitric oxide synthase in caloric restriction-induced cardioprotection against ischemia-reperfusion injury. Am. J. Physiol. Heart Circ. Physiol. 2015, 308, H894–H903. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Study Author and Reference | Type of Study | Subjects | CR or No. of Calories | Duration of Study | Significant Lowering of |
|---|---|---|---|---|---|
| Raitakari et al. [20] | Obs | Obese | 580 kcal/day | 6 weeks | SBP, DBP |
| Ruggenenti et al. [21] | RCT | Type 2 diabetics | 25% CR | 6 months | SBP, DBP, MAP |
| Hong et al. [24] | Obs | Some with MetS | 500–800 kcal/day | 12 weeks | SBP, DBP |
| Most et al. [26] | Obs | Normal weight | 25% CR | 24 months | SBP, DBP |
| Case et al. [31] | Obs | Obese, some with MetS | 600–800 kcal/day | Various | SBP, DBP |
| Beleslin et al. [32] | Obs | Morbid obesity | 500–800 kcal/day | 3 weeks | SBP, DBP |
| Goldhamer et al. [34] | Obs | Pre-hypertensive | Water fasting | 2 weeks | SBP, DBP |
| Goldhamer et al. [35] | Obs | Hypertensive | Water fasting | 10–11 days | SBP, DBP |
| Ghachem et al. [36] | Obs | Obese, post-menopausal females | CR, high carbohydrate, low fat | 6 months | No change |
| Hoddy et al. [40] | Obs | Obese | ADF 25% CR | 8 weeks | No change |
| Harvie et al. [45] | Obs | Overweight or obese | 25% CR 7 days/week or VLCD 2 days/week | 6 months | SBP, DBP in both groups |
| Study Author and Reference | Type of Study | Subjects | CR or No. of Calories | Duration of Study | Effect on HR and HRV |
|---|---|---|---|---|---|
| Stein et al. [8] | Obs | Healthy | 30% CR | 3–15 years | HR lower; HRV higher |
| Ruggenenti et al. [21] | RCT | Type 2 diabetics | 25% CR | 6 months | HR lower |
| Hoddy et al. [40] | Obs | Obese | ADF with 75% CR | 8 weeks | HR no change |
| Meyer et al. [46] | Obs | Healthy | 1672 kcal/day vs. 2445 kcal/day | Mean 6.5 years | HR no difference |
| Trepanowski et al. [52] | RCT | Obese | ADF with 75% CR, 25% CR or control | 6 months | HR no change |
| Study Author and Reference | Type of Study | Subjects | CR or No. of Calories | Duration of Study | Effect on Flow-Mediated Dilatation |
|---|---|---|---|---|---|
| Raitakari et al. [20] | Obs | Obese | 580 kcal/day | 6 weeks | Improved |
| Sasaki et al. [33] | Obs | Obese, hypertensive | 800 kcal/day | 2 weeks | Improved |
| Khoo et al. [67] | Obs | Diabetic, obese males | 1000 kcal/day | 8 weeks | Improved |
| Clifton et al. [68] | Obs | Overweight | Low fat/high carbohydrate CR | 3 months | No change |
| Volek et al. [69] | Obs | Overweight | 1500 kcal/day, low fat vs. low carbohydrate CR | 12 weeks | Improved in low carbohydrate CR |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nicoll, R.; Henein, M.Y. Caloric Restriction and Its Effect on Blood Pressure, Heart Rate Variability and Arterial Stiffness and Dilatation: A Review of the Evidence. Int. J. Mol. Sci. 2018, 19, 751. https://doi.org/10.3390/ijms19030751
Nicoll R, Henein MY. Caloric Restriction and Its Effect on Blood Pressure, Heart Rate Variability and Arterial Stiffness and Dilatation: A Review of the Evidence. International Journal of Molecular Sciences. 2018; 19(3):751. https://doi.org/10.3390/ijms19030751
Chicago/Turabian StyleNicoll, Rachel, and Michael Y. Henein. 2018. "Caloric Restriction and Its Effect on Blood Pressure, Heart Rate Variability and Arterial Stiffness and Dilatation: A Review of the Evidence" International Journal of Molecular Sciences 19, no. 3: 751. https://doi.org/10.3390/ijms19030751