
Comparison of GFAP and UCH-L1 Measurements Using Two Automated Immunoassays (i-STAT® and Alinity®) for the Management of Patients with Mild Traumatic Brain Injury: Preliminary Results from a French Single-Center Approach
 , , and
, , and
Abstract
:1. Introduction
2. Results
2.1. Patient Characteristics
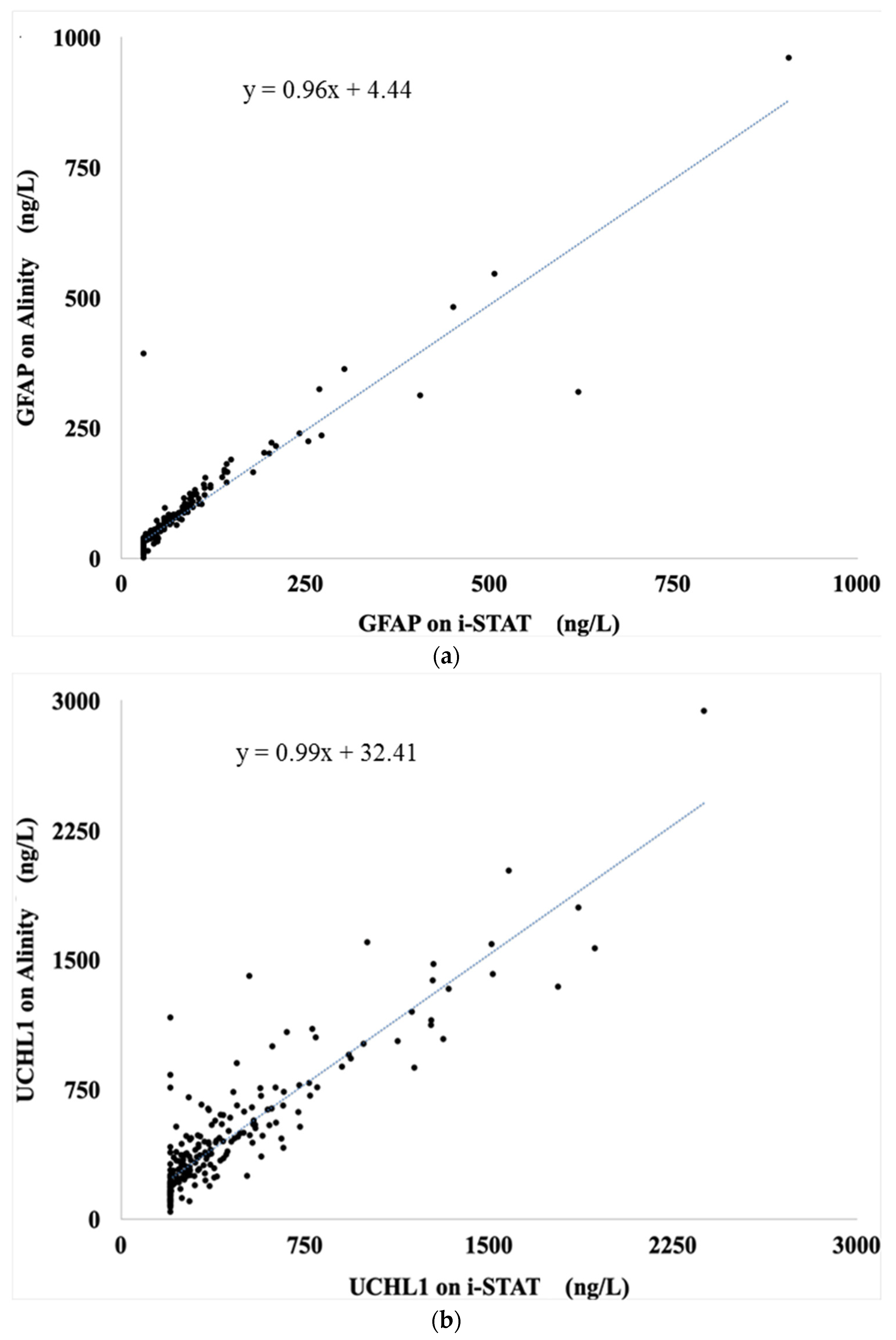
2.2. Analytical Correlation and Concordance
2.2.1. GFAP
2.2.2. UCH-L1
2.3. Biomarker Levels According to Imaging Findings on CT-Scan
2.3.1. i-STAT® Analyzer
2.3.2. Alinity® i Analyzer
2.4. Clinical Concordance for the Combined Test “GFAP + UCH-L1”
3. Discussion
4. Materials and Methods
4.1. Study Design and Patients
4.2. GFAP and UCH-L1 Assays
4.2.1. i-STAT® Analyzer
4.2.2. Alinity® Analyzer
4.3. Cranial Computed Tomography Scan
4.4. Statistical Analysis
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Oris, C.; Kahouadji, S.; Durif, J.; Bouvier, D.; Sapin, V. S100B, Actor and Biomarker of Mild Traumatic Brain Injury. Int. J. Mol. Sci. 2023, 24, 6602. [Google Scholar] [CrossRef] [PubMed]
- Haydel, M.J.; Blaudeau, E. Indications for Computed Tomography in Patients with Minor Head Injury. N. Engl. J. Med. 2000, 342, 100–105. [Google Scholar] [CrossRef] [PubMed]
- Sharp, A.L.; Nagaraj, G.; Rippberger, E.J.; Shen, E.; Swap, C.J.; Silver, M.A.; McCormick, T.; Vinson, D.R.; Hoffman, J.R. Computed Tomography Use for Adults With Head Injury: Describing Likely Avoidable Emergency Department Imaging Based on the Canadian CT Head Rule. Acad. Emerg. Med. 2017, 24, 22–30. [Google Scholar] [CrossRef] [PubMed]
- Hopman, J.H.; Santing, J.A.L.; Foks, K.A.; Verheul, R.J.; van der Linden, C.M.; van den Brand, C.L.; Jellema, K. Biomarker S100B in Plasma a Screening Tool for Mild Traumatic Brain Injury in an Emergency Department. Brain Inj. 2023, 37, 47–53. [Google Scholar] [CrossRef] [PubMed]
- Oris, C.; Pereira, B.; Durif, J.; Simon-Pimmel, J.; Castellani, C.; Manzano, S.; Sapin, V.; Bouvier, D. The Biomarker S100B and Mild Traumatic Brain Injury: A Meta-Analysis. Pediatrics 2018, 141, e20180037. [Google Scholar] [CrossRef] [PubMed]
- Astrand, R.; Rosenlund, C.; Undén, J. Scandinavian Guidelines for Initial Management of Minor and Moderate Head Trauma in Children. BMC Med. 2016, 14, 33. [Google Scholar] [CrossRef]
- Gil-Jardiné, C.; Payen, J.-F.; Bernard, R.; Bobbia, X.; Bouzat, P.; Catoire, P.; Chauvin, A.; Claessens, Y.-E.; Douay, B.; Dubucs, X.; et al. Management of Patients Suffering from Mild Traumatic Brain Injury 2023. Anaesth. Crit. Care Pain Med. 2023, 42, 101260. [Google Scholar] [CrossRef] [PubMed]
- Undén, J.; Romner, B. Can Low Serum Levels of S100B Predict Normal CT Findings after Minor Head Injury in Adults?: An Evidence-Based Review and Meta-Analysis. J. Head. Trauma. Rehabil. 2010, 25, 228–240. [Google Scholar] [CrossRef] [PubMed]
- Biberthaler, P.; Linsenmeier, U.; Pfeifer, K.-J.; Kroetz, M.; Mussack, T.; Kanz, K.-G.; Hoecherl, E.F.J.; Jonas, F.; Marzi, I.; Leucht, P.; et al. Serum S-100B Concentration Provides Additional Information Fot the Indication of Computed Tomography in Patients after Minor Head Injury: A Prospective Multicenter Study. Shock 2006, 25, 446–453. [Google Scholar] [CrossRef]
- Allouchery, G.; Moustafa, F.; Roubin, J.; Pereira, B.; Schmidt, J.; Raconnat, J.; Pic, D.; Sapin, V.; Bouvier, D. Clinical Validation of S100B in the Management of a Mild Traumatic Brain Injury: Issues from an Interventional Cohort of 1449 Adult Patients. Clin. Chem. Lab. Med. (CCLM) 2018, 56, 1897–1904. [Google Scholar] [CrossRef]
- Laribi, S.; Kansao, J.; Borderie, D.; Collet, C.; Deschamps, P.; Ababsa, R.; Mouniam, L.; Got, L.; Leon, A.; Thoannes, H.; et al. S100B Blood Level Measurement to Exclude Cerebral Lesions after Minor Head Injury: The Multicenter STIC-S100 French Study. Clin. Chem. Lab. Med. 2014, 52, 527–536. [Google Scholar] [CrossRef] [PubMed]
- Okonkwo, D.O.; Puffer, R.C.; Puccio, A.M.; Yuh, E.L.; Yue, J.K.; Diaz-Arrastia, R.; Korley, F.K.; Wang, K.K.W.; Sun, X.; Taylor, S.R.; et al. Point-of-Care Platform Blood Biomarker Testing of Glial Fibrillary Acidic Protein versus S100 Calcium-Binding Protein B for Prediction of Traumatic Brain Injuries: A Transforming Research and Clinical Knowledge in Traumatic Brain Injury Study. J. Neurotrauma 2020, 37, 2460–2467. [Google Scholar] [CrossRef] [PubMed]
- Bazarian, J.J.; Biberthaler, P.; Welch, R.D.; Lewis, L.M.; Barzo, P.; Bogner-Flatz, V.; Gunnar Brolinson, P.; Büki, A.; Chen, J.Y.; Christenson, R.H.; et al. Serum GFAP and UCH-L1 for Prediction of Absence of Intracranial Injuries on Head CT (ALERT-TBI): A Multicentre Observational Study. Lancet Neurol. 2018, 17, 782–789. [Google Scholar] [CrossRef] [PubMed]
- Janigro, D.; Mondello, S.; Posti, J.P.; Unden, J. GFAP and S100B: What You Always Wanted to Know and Never Dared to Ask. Front. Neurol. 2022, 13, 835597. [Google Scholar] [CrossRef] [PubMed]
- Bazarian, J.J.; Welch, R.D.; Caudle, K.; Jeffrey, C.A.; Chen, J.Y.; Chandran, R.; McCaw, T.; Datwyler, S.A.; Zhang, H.; McQuiston, B. Accuracy of a Rapid GFAP/UCH-L1 Test for the Prediction of Intracranial Injuries on Head CT after Mild Traumatic Brain Injury. Acad. Emerg. Med. 2021, 28, 1308–1317. [Google Scholar] [CrossRef] [PubMed]
- Oris, C.; Bouillon-Minois, J.-B.; Kahouadji, S.; Pereira, B.; Dhaiby, G.; Defrance, V.B.; Durif, J.; Schmidt, J.; Moustafa, F.; Bouvier, D.; et al. S100B vs. “GFAP and UCH-L1” Assays in the Management of MTBI Patients. Clin. Chem. Lab. Med. (CCLM) 2023, 62, 891–899. [Google Scholar] [CrossRef] [PubMed]
- Azizi, S.; Hier, D.B.; Allen, B.; Obafemi-Ajayi, T.; Olbricht, G.R.; Thimgan, M.S.; Wunsch, D.C. A Kinetic Model for Blood Biomarker Levels After Mild Traumatic Brain Injury. Front. Neurol. 2021, 12, 668606. [Google Scholar] [CrossRef] [PubMed]
- Thelin, E.P.; Zeiler, F.A.; Ercole, A.; Mondello, S.; Büki, A.; Bellander, B.-M.; Helmy, A.; Menon, D.K.; Nelson, D.W. Serial Sampling of Serum Protein Biomarkers for Monitoring Human Traumatic Brain Injury Dynamics: A Systematic Review. Front. Neurol. 2017, 8, 300. [Google Scholar] [CrossRef]
- Biberthaler, P.; Musaelyan, K.; Krieg, S.; Meyer, B.; Stimmer, H.; Zapf, J.; von Matthey, F.; Chandran, R.; Marino, J.A.; Beligere, G.; et al. Evaluation of Acute Glial Fibrillary Acidic Protein and Ubiquitin C-Terminal Hydrolase-L1 Plasma Levels in Traumatic Brain Injury Patients with and without Intracranial Lesions. Neurotrauma Rep. 2021, 2, 617–625. [Google Scholar] [CrossRef]
- Oris, C.; Bouillon-Minois, J.-B.; Pinguet, J.; Kahouadji, S.; Durif, J.; Meslé, V.; Pereira, B.; Schmidt, J.; Sapin, V.; Bouvier, D. Predictive Performance of Blood S100B in the Management of Patients Over 65 Years Old With Mild Traumatic Brain Injury. J. Gerontol. Ser. A 2021, 76, 1471–1479. [Google Scholar] [CrossRef]
- Koivikko, P.; Posti, J.P.; Mohammadian, M.; Lagerstedt, L.; Azurmendi, L.; Hossain, I.; Katila, A.J.; Menon, D.; Newcombe, V.F.J.; Hutchinson, P.J.; et al. Potential of Heart Fatty-Acid Binding Protein, Neurofilament Light, Interleukin-10 and S100 Calcium-Binding Protein B in the Acute Diagnostics and Severity Assessment of Traumatic Brain Injury. Emerg. Med. J. 2022, 39, 206–212. [Google Scholar] [CrossRef] [PubMed]
- Ward, M.D.; Weber, A.; Merrill, V.D.; Welch, R.D.; Bazarian, J.J.; Christenson, R.H. Predictive Performance of Traumatic Brain Injury Biomarkers in High-Risk Elderly Patients. J. Appl. Lab. Med. 2020, 5, 608. [Google Scholar] [CrossRef] [PubMed]
- Korley, F.K.; Datwyler, S.A.; Jain, S.; Sun, X.; Beligere, G.; Chandran, R.; Marino, J.A.; McQuiston, B.; Zhang, H.; Caudle, K.L.; et al. Comparison of GFAP and UCH-L1 Measurements from Two Prototype Assays: The Abbott i-STAT and ARCHITECT Assays. Neurotrauma Rep. 2021, 2, 193–199. [Google Scholar] [CrossRef] [PubMed]
- Zimmer, L.; McDade, C.; Beyhaghi, H.; Purser, M.; Textoris, J.; Krause, A.; Blanc, E.; Pavlov, V.; Earnshaw, S. Cost-Effectiveness of Blood-Based Brain Biomarkers for Screening Adults with Mild Traumatic Brain Injury in the French Health Care Setting. J. Neurotrauma 2023, 40, 706–719. [Google Scholar] [CrossRef] [PubMed]
- Richter, S.; Czeiter, E.; Amrein, K.; Mikolic, A.; Verheyden, J.; Wang, K.; Maas, A.I.R.; Steyerberg, E.; Büki, A.; Menon, D.K.; et al. Prognostic Value of Serum Biomarkers in Patients With Moderate-Severe Traumatic Brain Injury, Differentiated by Marshall Computer Tomography Classification. J. Neurotrauma 2023, 40, 2297–2310. [Google Scholar] [CrossRef] [PubMed]
- for the BE FAST III Study Group; Luger, S.; Jæger, H.S.; Dixon, J.; Bohmann, F.O.; Schaefer, J.; Richieri, S.P.; Larsen, K.; Hov, M.R.; Bache, K.G.; et al. Diagnostic Accuracy of Glial Fibrillary Acidic Protein and Ubiquitin Carboxy-Terminal Hydrolase-L1 Serum Concentrations for Differentiating Acute Intracerebral Hemorrhage from Ischemic Stroke. Neurocrit Care 2020, 33, 39–48. [Google Scholar] [CrossRef]
- Lewis, L.M.; Papa, L.; Bazarian, J.J.; Weber, A.; Howard, R.; Welch, R.D. Biomarkers May Predict Unfavorable Neurological Outcome after Mild Traumatic Brain Injury. J. Neurotrauma 2020, 37, 2624–2631. [Google Scholar] [CrossRef]
- Altman, D.G. Practical Statistics for Medical Research; Chapman and Hall: London, UK, 1991. [Google Scholar]



{kind=link}
{kind=link}
| Demographic Characteristics and Clinically Relevant Information | |
|---|---|
| Total | 230 |
| Sex ratio (M/F) | 1.2 |
| Mean age in years (min; max; IQR) | 66.2 (18.2; 101.2; 33.9–82.8) |
| Mean sampling time in minutes (min; max; IQR) | 100.5 (25; 720; 75–162) |
| GCS at admission, n (%) | |
| 13 | 1 (0.3) |
| 14 | 9 (4) |
| 15 | 220 (95.7) |
| Clinical outcome, n (%) | |
| Discharged | 194 (84.3) |
| Hospitalized for surveillance | 35 (15.3) |
| Death | 1 (0.4) |
| CT+ patients, n (%) | |
| Subdural hematoma | 5 (2.2) |
| Subarachnoid hemorrhage | 6 (2.6) |
| GFAP | UCH-L1 | |
|---|---|---|
| i-STAT® (ng/L), median | 43 | 282 |
| (min; max; IQR) | (30; 907; 30–76) | (200; 2376; 200–472) |
| Alinity® i (ng/L), median | 46.3 | 350 |
| (min; max; IQR) | (1; 961; 23–85) | (42; 2940; 200–548) |
| p-Value | 0.17 | 0.14 |
| Lin (95% CI) | 0.93 (0.91–0.95) | 0.89 (0.87–0.92) |
| % of agreement | 94 | 86 |
| Kappa (95% CI) | 0.88 (0.82–0.94) | 0.70 (0.60–0.79) |
| i-STAT® | |||
| ICL− (n = 219) | ICL+ (n = 11) | p-Value | |
| GFAP in ng/L median (min; max; IQR) | 41 (30; 507; 30–74) | 85 (30; 907; 59–179) | 0.003 |
| UCH-L1 in ng/L median (min; max; IQR) | 279 (200; 2376; 200–471) | 312 (200; 1931; 281–540) | 0.20 |
| Alinity® i | |||
| ICL− (n = 219) | ICL+ (n = 11) | p-Value | |
| GFAP in ng/L median (min; max; IQR) | 44 (1;546; 23–83) | 87 (29; 961; 71.1–165) | 0.005 |
| UCH-L1 in ng/L median (min; max; IQR) | 342 (42; 2940; 197–548) | 469 (187; 1603; 282–570) | 0.14 |
| GFAP + UCH-L1 (i-STAT®) | GFAP + UCH-L1 (Alinity® i) | p-Value | |
|---|---|---|---|
| SE (95% CI) | 100% (75.1–100%) | 100% (72–100%) | 1 |
| SP (95% CI) | 28.8% (22.9–35.3%) | 29.7% (23.7–36.2%) | 0.68 |
| PPV (95% CI) | 6.6% (3.3–11.5%) | 6.7% (3.3–11.5%) | 0.98 |
| NPV (95% CI) | 100% (94.3–100%) | 100% (94.5–100%) | 1 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Oris, C.; Khatib-Chahidi, C.; Pereira, B.; Bailly Defrance, V.; Bouvier, D.; Sapin, V. Comparison of GFAP and UCH-L1 Measurements Using Two Automated Immunoassays (i-STAT® and Alinity®) for the Management of Patients with Mild Traumatic Brain Injury: Preliminary Results from a French Single-Center Approach. Int. J. Mol. Sci. 2024, 25, 4539. https://doi.org/10.3390/ijms25084539
Oris C, Khatib-Chahidi C, Pereira B, Bailly Defrance V, Bouvier D, Sapin V. Comparison of GFAP and UCH-L1 Measurements Using Two Automated Immunoassays (i-STAT® and Alinity®) for the Management of Patients with Mild Traumatic Brain Injury: Preliminary Results from a French Single-Center Approach. International Journal of Molecular Sciences. 2024; 25(8):4539. https://doi.org/10.3390/ijms25084539
Chicago/Turabian StyleOris, Charlotte, Clara Khatib-Chahidi, Bruno Pereira, Valentin Bailly Defrance, Damien Bouvier, and Vincent Sapin. 2024. "Comparison of GFAP and UCH-L1 Measurements Using Two Automated Immunoassays (i-STAT® and Alinity®) for the Management of Patients with Mild Traumatic Brain Injury: Preliminary Results from a French Single-Center Approach" International Journal of Molecular Sciences 25, no. 8: 4539. https://doi.org/10.3390/ijms25084539