
Investigating the Role of FABP4 in Diabetes and Obesity and the Influence of Age and Ethnicity: A Comprehensive Analysis of a Cohort from the KEDP-Study
 , ,
, ,  , , , ,
, , , , 
Abstract
:1. Introduction
2. Results
2.1. Study Sample
2.2. The Association between FABP4 Levels and Clinical Markers
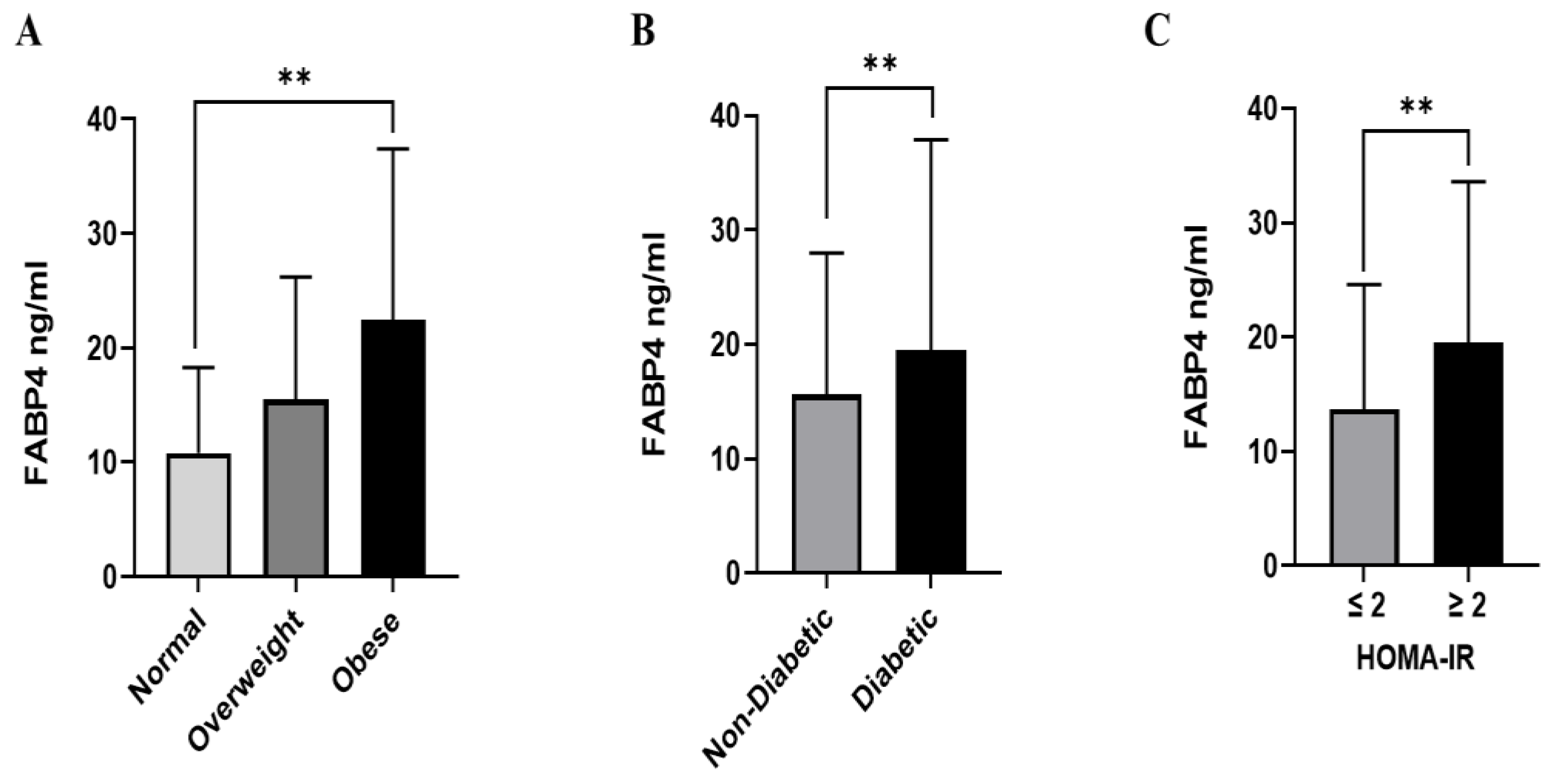
2.3. The Association between FABP4 Levels and Markers for Obesity
2.4. The Association between FABP4 Levels and the Glycemic Indices
3. Discussion
4. Methods and Materials
4.1. Participants and the Study Design
4.2. Anthropometry and Vital Signs Measurements
4.3. Laboratory Measurements
4.4. FABP4 Plasma Levels and R&D Custom Multiplexing Assay
4.5. Statistical Analysis
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Yang, J.; Liu, S.; Li, Y.; Fan, Z.; Meng, Y.; Zhou, B.; Zhang, G.; Zhan, H. FABP4 in macrophages facilitates obesity-associated pancreatic cancer progression via the NLRP3/IL-1beta axis. Cancer Lett. 2023, 575, 216403. [Google Scholar] [CrossRef]
- Bluher, M.; Aras, M.; Aronne, L.J.; Batterham, R.L.; Giorgino, F.; Ji, L.; Pietilainen, K.H.; Schnell, O.; Tonchevska, E.; Wilding, J.P.H. New insights into the treatment of obesity. Diabetes Obes. Metab. 2023, 25, 2058–2072. [Google Scholar] [CrossRef]
- Rubino, F.; Batterham, R.L.; Koch, M.; Mingrone, G.; le Roux, C.W.; Farooqi, I.S.; Farpour-Lambert, N.; Gregg, E.W.; Cummings, D.E. Lancet Diabetes & Endocrinology Commission on the Definition and Diagnosis of Clinical Obesity. Lancet Diabetes Endocrinol. 2023, 11, 226–228. [Google Scholar] [CrossRef]
- Safaei, M.; Sundararajan, E.A.; Driss, M.; Boulila, W.; Shapi’i, A. A systematic literature review on obesity: Understanding the causes & consequences of obesity and reviewing various machine learning approaches used to predict obesity. Comput. Biol. Med. 2021, 136, 104754. [Google Scholar] [CrossRef]
- Jia, W.; Liu, F. Obesity: Causes, consequences, treatments, and challenges. J. Mol. Cell Biol. 2021, 13, 463–465. [Google Scholar] [CrossRef] [PubMed]
- Masood, B.; Moorthy, M. Causes of obesity: A review. Clin. Med. 2023, 23, 284–291. [Google Scholar] [CrossRef]
- Liu, S.; Wu, D.; Fan, Z.; Yang, J.; Li, Y.; Meng, Y.; Gao, C.; Zhan, H. FABP4 in obesity-associated carcinogenesis: Novel insights into mechanisms and therapeutic implications. Front. Mol. Biosci. 2022, 9, 973955. [Google Scholar] [CrossRef]
- Wang, Y.; Yu, F.; Zheng, X.; Li, J.; Zhang, Z.; Zhang, Q.; Chen, J.; He, Y.; Yang, H.; Zhou, P. Balancing adipocyte production and lipid metabolism to treat obesity-induced diabetes with a novel proteoglycan from Ganoderma lucidum. Lipids Health Dis. 2023, 22, 120. [Google Scholar] [CrossRef] [PubMed]
- Williams, E.P.; Mesidor, M.; Winters, K.; Dubbert, P.M.; Wyatt, S.B. Overweight and Obesity: Prevalence, Consequences, and Causes of a Growing Public Health Problem. Curr. Obes. Rep. 2015, 4, 363–370. [Google Scholar] [CrossRef] [PubMed]
- Xu, A.; Wang, Y.; Xu, J.Y.; Stejskal, D.; Tam, S.; Zhang, J.; Wat, N.M.; Wong, W.K.; Lam, K.S. Adipocyte fatty acid-binding protein is a plasma biomarker closely associated with obesity and metabolic syndrome. Clin. Chem. 2006, 52, 405–413. [Google Scholar] [CrossRef] [PubMed]
- Tsai, H.-Y.; Wu, Y.-W.; Tseng, W.-K.; Leu, H.-B.; Yin, W.-H.; Lin, T.-H.; Chang, K.-C.; Wang, J.-H.; Yeh, H.-I.; Wu, C.-C.; et al. Circulating fatty-acid binding-protein 4 levels predict CV events in patients after coronary interventions. J. Formos. Med. Assoc. 2021, 120, 728–736. [Google Scholar] [CrossRef]
- Furuhashi, M.; Sakuma, I.; Morimoto, T.; Higashiura, Y.; Sakai, A.; Matsumoto, M.; Sakuma, M.; Shimabukuro, M.; Nomiyama, T.; Arasaki, O.; et al. Independent and Distinct Associations of FABP4 and FABP5 With Metabolic Parameters in Type 2 Diabetes Mellitus. Front. Endocrinol. 2020, 11, 575557. [Google Scholar] [CrossRef]
- Lee, C.H.; Cheung, C.Y.Y.; Woo, Y.C.; Lui, D.T.W.; Yuen, M.M.A.; Fong, C.H.Y.; Chow, W.S.; Xu, A.; Lam, K.S.L. Prospective associations of circulating adipocyte fatty acid-binding protein levels with risks of renal outcomes and mortality in type 2 diabetes. Diabetologia 2019, 62, 169–177. [Google Scholar] [CrossRef]
- Numao, S.; Uchida, R.; Kurosaki, T.; Nakagaichi, M. Carbohydrate ingestion does not suppress increases in fatty acid-binding protein 4 concentrations post-acute aerobic exercise in healthy men: A randomized crossover study. BMC Sports Sci. Med. Rehabil. 2024, 16, 63. [Google Scholar] [CrossRef]
- Chung, J.Y.; Hong, J.; Kim, H.J.; Song, Y.; Yong, S.B.; Lee, J.; Kim, Y.H. White adipocyte-targeted dual gene silencing of FABP4/5 for anti-obesity, anti-inflammation and reversal of insulin resistance: Efficacy and comparison of administration routes. Biomaterials 2021, 279, 121209. [Google Scholar] [CrossRef]
- Vorobjova, T.; Tagoma, A.; Talja, I.; Janson, H.; Kirss, A.; Uibo, R. FABP4 and I-FABP Levels in Pregnant Women Are Associated with Body Mass Index but Not Gestational Diabetes. J. Diabetes Res. 2022, 2022, 1089434. [Google Scholar] [CrossRef]
- von Eynatten, M.; Breitling, L.P.; Roos, M.; Baumann, M.; Rothenbacher, D.; Brenner, H. Circulating adipocyte fatty acid-binding protein levels and cardiovascular morbidity and mortality in patients with coronary heart disease: A 10-year prospective study. Arterioscler. Thromb. Vasc. Biol. 2012, 32, 2327–2335. [Google Scholar] [CrossRef]
- Kaess, B.M.; Enserro, D.M.; McManus, D.D.; Xanthakis, V.; Chen, M.H.; Sullivan, L.M.; Ingram, C.; O’Donnell, C.J.; Keaney, J.F.; Vasan, R.S.; et al. Cardiometabolic correlates and heritability of fetuin-A, retinol-binding protein 4, and fatty-acid binding protein 4 in the Framingham Heart Study. J. Clin. Endocrinol. Metab. 2012, 97, E1943–E1947. [Google Scholar] [CrossRef]
- Ning, H.; Tao, H.; Weng, Z.; Zhao, X. Plasma fatty acid-binding protein 4 (FABP4) as a novel biomarker to predict gestational diabetes mellitus. Acta Diabetol. 2016, 53, 891–898. [Google Scholar] [CrossRef]
- Garin-Shkolnik, T.; Rudich, A.; Hotamisligil, G.S.; Rubinstein, M. FABP4 attenuates PPARgamma and adipogenesis and is inversely correlated with PPARgamma in adipose tissues. Diabetes 2014, 63, 900–911. [Google Scholar] [CrossRef]
- Zhang, X.Z.; Tu, W.J.; Wang, H.; Zhao, Q.; Liu, Q.; Sun, L.; Yu, L. Circulating Serum Fatty Acid-Binding Protein 4 Levels Predict the Development of Diabetic Retinopathy in Type 2 Diabetic Patients. Am. J. Ophthalmol. 2018, 187, 71–79. [Google Scholar] [CrossRef]
- Nakamura, R.; Okura, T.; Fujioka, Y.; Sumi, K.; Matsuzawa, K.; Izawa, S.; Ueta, E.; Kato, M.; Taniguchi, S.I.; Yamamoto, K. Serum fatty acid-binding protein 4 (FABP4) concentration is associated with insulin resistance in peripheral tissues, A clinical study. PLoS ONE 2017, 12, e0179737. [Google Scholar] [CrossRef]
- Ota, H.; Furuhashi, M.; Ishimura, S.; Koyama, M.; Okazaki, Y.; Mita, T.; Fuseya, T.; Yamashita, T.; Tanaka, M.; Yoshida, H.; et al. Elevation of fatty acid-binding protein 4 is predisposed by family history of hypertension and contributes to blood pressure elevation. Am. J. Hypertens. 2012, 25, 1124–1130. [Google Scholar] [CrossRef]
- Terra, X.; Quintero, Y.; Auguet, T.; Porras, J.A.; Hernandez, M.; Sabench, F.; Aguilar, C.; Luna, A.M.; Del Castillo, D.; Richart, C. FABP 4 is associated with inflammatory markers and metabolic syndrome in morbidly obese women. Eur. J. Endocrinol. 2011, 164, 539–547. [Google Scholar] [CrossRef]
- Dadej, D.; Szczepanek-Parulska, E.; Ruchala, M. Interplay between Fatty Acid Binding Protein 4, Fetuin-A, Retinol Binding Protein 4 and Thyroid Function in Metabolic Dysregulation. Metabolites 2022, 12, 300. [Google Scholar] [CrossRef]
- Furuhashi, M.; Saitoh, S.; Shimamoto, K.; Miura, T. Fatty Acid-Binding Protein 4 (FABP4): Pathophysiological Insights and Potent Clinical Biomarker of Metabolic and Cardiovascular Diseases. Clin. Med. Insights Cardiol. 2014, 8, 23–33. [Google Scholar] [CrossRef]
- Polak, A.M.; Lebkowska, A.; Krentowska, A.; Buczynska, A.; Adamski, M.; Kretowski, A.J.; Kowalska, I.; Adamska, A. Elevated Serum Concentration of Adipocyte Fatty Acid-Binding Protein Correlates with the Markers of Abdominal Obesity Independently of Thyroid Hormones in Non-Obese Women with Polycystic Ovary Syndrome. J. Clin. Med. 2023, 12, 4610. [Google Scholar] [CrossRef]
- Tan, M.; Korkmaz, H.; Aydin, H.; Kumbul Doguc, D. FABP4 levels in hypothyroidism and its relationship with subclinical atherosclerosis. Turk. J. Med. Sci. 2019, 49, 1490–1497. [Google Scholar] [CrossRef]
- Chen, J.; Wu, K.; Lei, Y.; Huang, M.; Cheng, L.; Guan, H.; Lin, J.; Zhong, M.; Wang, X.; Zheng, Z. Inhibition of Fatty Acid beta-Oxidation by Fatty Acid Binding Protein 4 Induces Ferroptosis in HK2 Cells Under High Glucose Conditions. Endocrinol. Metab. 2023, 38, 226–244. [Google Scholar] [CrossRef]
- Berger, E.; Geloen, A. FABP4 Controls Fat Mass Expandability (Adipocyte Size and Number) through Inhibition of CD36/SR-B2 Signalling. Int. J. Mol. Sci. 2023, 24, 1032. [Google Scholar] [CrossRef]
- Djousse, L.; Bartz, T.M.; Ix, J.H.; Kochar, J.; Kizer, J.R.; Gottdiener, J.S.; Tracy, R.P.; Mozaffarian, D.; Siscovick, D.S.; Mukamal, K.J.; et al. Fatty acid-binding protein 4 and incident heart failure: The Cardiovascular Health Study. Eur. J. Heart Fail. 2013, 15, 394–399. [Google Scholar] [CrossRef]
- Su, H.Y.; Hsu, B.G.; Lin, Y.L.; Wang, C.H.; Lai, Y.H. Serum adipocyte fatty acid-binding protein level is positively associated with aortic stiffness in nondialysis chronic kidney disease patients: A cross-sectional study. Medicine 2022, 101, e29558. [Google Scholar] [CrossRef]
- Shi, Y.; Wang, C.C.; Wu, L.; Zhang, Y.; Xu, A.; Wang, Y. Pathophysiological Insight into Fatty Acid-Binding Protein-4: Multifaced Roles in Reproduction, Pregnancy, and Offspring Health. Int. J. Mol. Sci. 2023, 24, 12655. [Google Scholar] [CrossRef]
- Li, B.; Zamzam, A.; Syed, M.H.; Djahanpour, N.; Jain, S.; Abdin, R.; Qadura, M. Fatty acid binding protein 4 has prognostic value in peripheral artery disease. J. Vasc. Surg. 2023, 78, 719–726. [Google Scholar] [CrossRef]
- Saito, N.; Furuhashi, M.; Koyama, M.; Higashiura, Y.; Akasaka, H.; Tanaka, M.; Moniwa, N.; Ohnishi, H.; Saitoh, S.; Ura, N.; et al. Elevated circulating FABP4 concentration predicts cardiovascular death in a general population: A 12-year prospective study. Sci. Rep. 2021, 11, 4008. [Google Scholar] [CrossRef]
- Chan, K.H.; Song, Y.; Hsu, Y.H.; You, N.C.; Tinker, L.F.; Liu, S. Common genetic variants in fatty acid-binding protein-4 (FABP4) and clinical diabetes risk in the Women’s Health Initiative Observational Study. Obes. Silver Spring 2010, 18, 1812–1820. [Google Scholar] [CrossRef]
- Cabré, A.; Lázaro, I.; Girona, J.; Manzanares, J.M.; Marimón, F.; Plana, N.; Heras, M.; Masana, L. Plasma fatty acid binding protein 4 is associated with atherogenic dyslipidemia in diabetes. J. Lipid Res. 2008, 49, 1746–1751. [Google Scholar] [CrossRef]
- Alkandari, A.; Alarouj, M.; Elkum, N.; Sharma, P.; Devarajan, S.; Abu-Farha, M.; Al-Mulla, F.; Tuomilehto, J.; Bennakhi, A. Adult Diabetes and Prediabetes Prevalence in Kuwait: Data from the Cross-Sectional Kuwait Diabetes Epidemiology Program. J. Clin. Med. 2020, 9, 3420. [Google Scholar] [CrossRef]
- Genuth, S.M.; Palmer, J.P.; Nathan, D.M. Classification and Diagnosis of Diabetes. In Diabetes in America, 3rd ed.; Cowie, C.C., Casagrande, S.S., Menke, A., Cissell, M.A., Eberhardt, M.S., Meigs, J.B., Gregg, E.W., Eds.; National Institutes of Health: Bethesda, MD, USA, 2018. [Google Scholar]



{kind=link}
{kind=link}
| Characteristics | (%) or Median (IQR) |
|---|---|
| Gender, n (%) | |
| Male | 1161 (55.7%) |
| Female | 922 (44.3%) |
| Age, n (%) | |
| <40 | 750 (36.0%) |
| 40–50 | 680 (32.7%) |
| >50 | 653 (31.3%) |
| Ethnicity, n (%) | |
| Arab | 899 (46.6%) |
| South Asian | 666 (34.5%) |
| Southeast Asian | 364 (18.9%) |
| Diabetes status, n (%) | |
| Non-Diabetic | 1425 (69.2%) |
| Diabetic | 633 (30.8%) |
| BMI, n (%) | |
| Normal BMI | 441 (21.2%) |
| Overweight | 837 (40.2%) |
| Obese | 805 (38.6%) |
| HOMA-IR, n (%) | |
| HOMA-IR ≤ 2 | 969 (50.3%) |
| HOMA-IR > 2 | 958 (49.7%) |
| Hip circumference, median (IQR) | 102.3 (13) |
| Waist circumference, median (IQR) | 95 (15) |
| SBP, median (IQR) | 131 (26) |
| DBP, median (IQR) | 80 (16) |
| FBG, median (IQR) | 5.3 (1.7) |
| Insulin, median (IQR) | 7.9 (6.7) |
| TSH, median (IQR) | 1.53 (1.14) |
| FT4, median (IQR) | 11.78 (3.43) |
| FT3, median (IQR) | 4.76 (0.78) |
| Age, median (min, max) | 45 (18, 82) |
| HbA1c, median (IQR) | 5.8 (1.2) |
| TC, median IQR) | 5.1 (1.33) |
| AST, median (IQR) | 21 (8) |
| CRP, median (IQR) | 3 (2) |
| Characteristics | Number of Participants | FABP4 Levels (ng/mL) | p-Value |
|---|---|---|---|
| Gender | |||
| Male | 924 | 14.42 (10.9) | <0.001 a |
| Female | 762 | 18.83 (15.4) | |
| Age | |||
| <40 | 689 | 14.3 (11.9) | <0.001 b |
| 40–50 | 566 | 16.2 (12.9) | |
| >50 | 431 | 19.3 (15.9) | |
| Ethnicity | |||
| Arab | 715 | 18.0 (15.7) | <0.001 b |
| South Asian | 511 | 15.6 (10.8) | |
| Southeast Asian | 310 | 13.2 (10.8) | |
| Diabetes Status | |||
| Non-Diabetic | 1404 | 15.6 (12.4) | <0.001 a |
| Diabetic | 261 | 19.5 (18.4) | |
| BMI | |||
| Normal BMI | 387 | 10.8 (7.5) | <0.001 b |
| Overweight | 691 | 15.5 (10.7) | |
| Obese | 608 | 22.5 (14.9) | |
| HOMA-IR | |||
| HOMA-IR ≤ 2 | 890 | 13.7 (10.9) | <0.001 a |
| HOMA-IR > 2 | 644 | 19.5 (14.1) |
| Marker | FABP4 Level (r) | p-Value | Marker | FABP4 Level (r) | p-Value |
|---|---|---|---|---|---|
| Gender | −0.168 | <0.001 | HbA1c | 0.126 | <0.001 |
| Nationality | 0.144 | <0.001 | Insulin | 0.326 | <0.001 |
| Age | 0.228 | <0.001 | TC | 0.047 | <0.001 |
| BMI | 0.496 | <0.001 | TG | 0.159 | <0.001 |
| Hip circumference | 0.463 | <0.001 | HDL | −0.031 | <0.001 |
| Waist circumference | 0.436 | <0.001 | LDL | 0.022 | <0.001 |
| SBP | 0.079 | <0.001 | TSH | 0.088 | <0.001 |
| DBP | 0.111 | <0.001 | FT4 | 0.087 | <0.001 |
| FBG | 0.184 | <0.001 | FT3 | −0.110 | <0.001 |
| CRP | 0.316 | <0.001 | HOMA-IR | 0.333 | <0.001 |
| Marker | Unadjusted Median Regression β (95% CI) | p-Value | Adjusted Median Regression β (95% CI) * | p-Value |
|---|---|---|---|---|
| Male gender | −4.4 (−5.6, −3.2) | <0.001 | −3.85 (−4.92, −2.77) | <0.001 |
| Age | 0.21 (0.15, 0.27) | <0.001 | 0.14 (0.096, 0.183) | <0.001 |
| South Asian | −2.39 (−3.88, −0.89) | 0.002 | 1.52 (0.488, 2.54) | 0.004 |
| BMI | 0.915 (0.83, 1.0) | <0.001 | 0.74 (0.65, 0.84) | <0.001 |
| Insulin | 0.471 (0.27, 0.67) | <0.001 | 0.115 (0.091, 1.38) | <0.001 |
| TG | 1.9 (0.5, 3.3) | 0.007 | 0.676 (0.067, 1.29) | 0.030 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Abdalla, M.A.; Abubaker, J.; Abu-Farha, M.; Al-Khairi, I.; Cherian, P.; Qaddoumi, M.G.; Al-Rashed, F.; Thanaraj, T.A.; Albatineh, A.N.; Al-Mulla, F. Investigating the Role of FABP4 in Diabetes and Obesity and the Influence of Age and Ethnicity: A Comprehensive Analysis of a Cohort from the KEDP-Study. Int. J. Mol. Sci. 2024, 25, 4578. https://doi.org/10.3390/ijms25094578
Abdalla MA, Abubaker J, Abu-Farha M, Al-Khairi I, Cherian P, Qaddoumi MG, Al-Rashed F, Thanaraj TA, Albatineh AN, Al-Mulla F. Investigating the Role of FABP4 in Diabetes and Obesity and the Influence of Age and Ethnicity: A Comprehensive Analysis of a Cohort from the KEDP-Study. International Journal of Molecular Sciences. 2024; 25(9):4578. https://doi.org/10.3390/ijms25094578
Chicago/Turabian StyleAbdalla, Mohammed A., Jehad Abubaker, Mohamed Abu-Farha, Irina Al-Khairi, Preethi Cherian, Mohammad G. Qaddoumi, Fatema Al-Rashed, Thangavel Alphonse Thanaraj, Ahmed N. Albatineh, and Fahd Al-Mulla. 2024. "Investigating the Role of FABP4 in Diabetes and Obesity and the Influence of Age and Ethnicity: A Comprehensive Analysis of a Cohort from the KEDP-Study" International Journal of Molecular Sciences 25, no. 9: 4578. https://doi.org/10.3390/ijms25094578