
Comparing the Risk of Infusion-Related Reactions and Tolerability in Patients Given Cetirizine or Diphenhydramine Prior to Ocrelizumab Infusion (PRECEPT)
Abstract
:1. Introduction
2. Methods
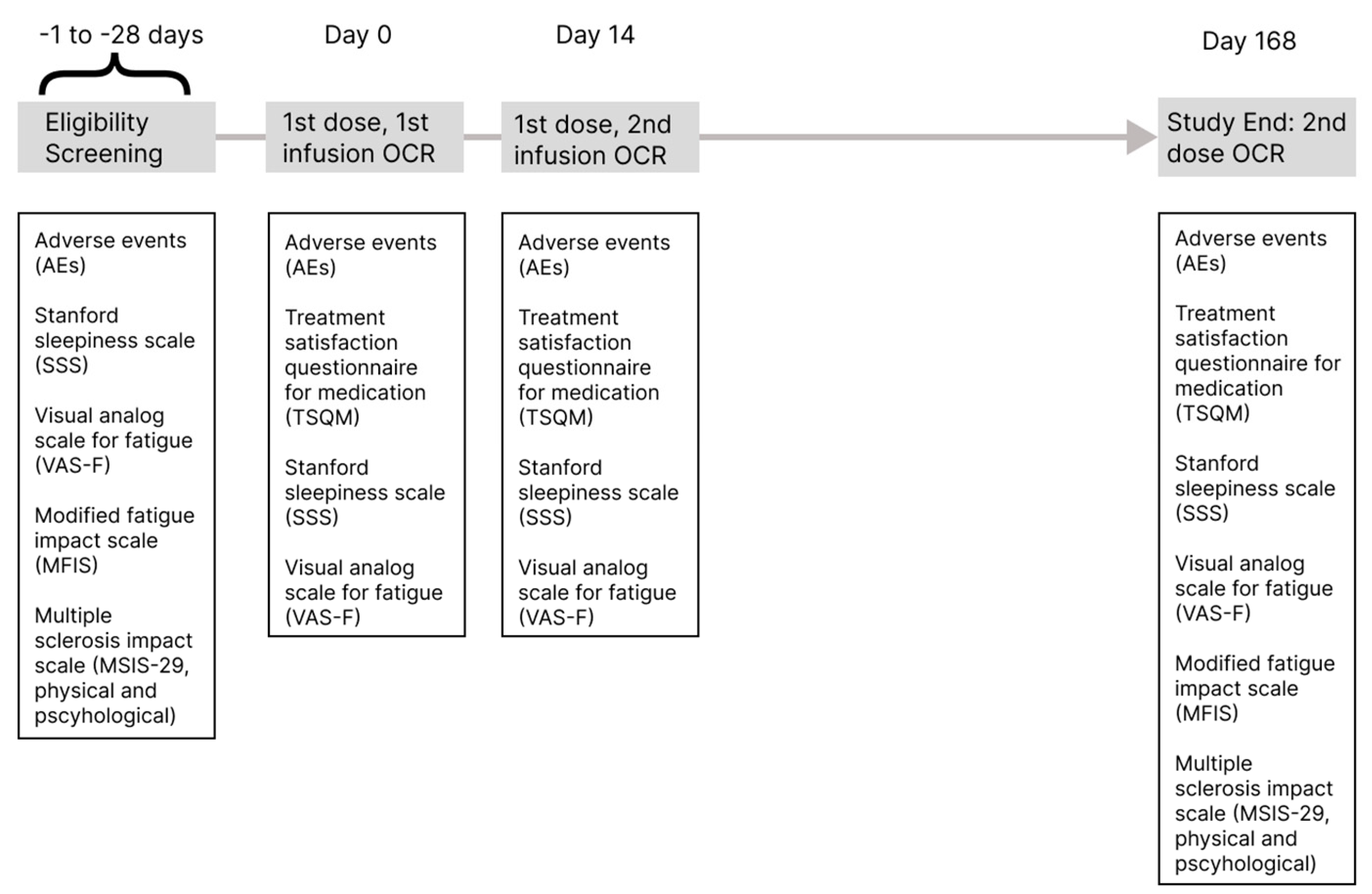
2.1. Trial Design
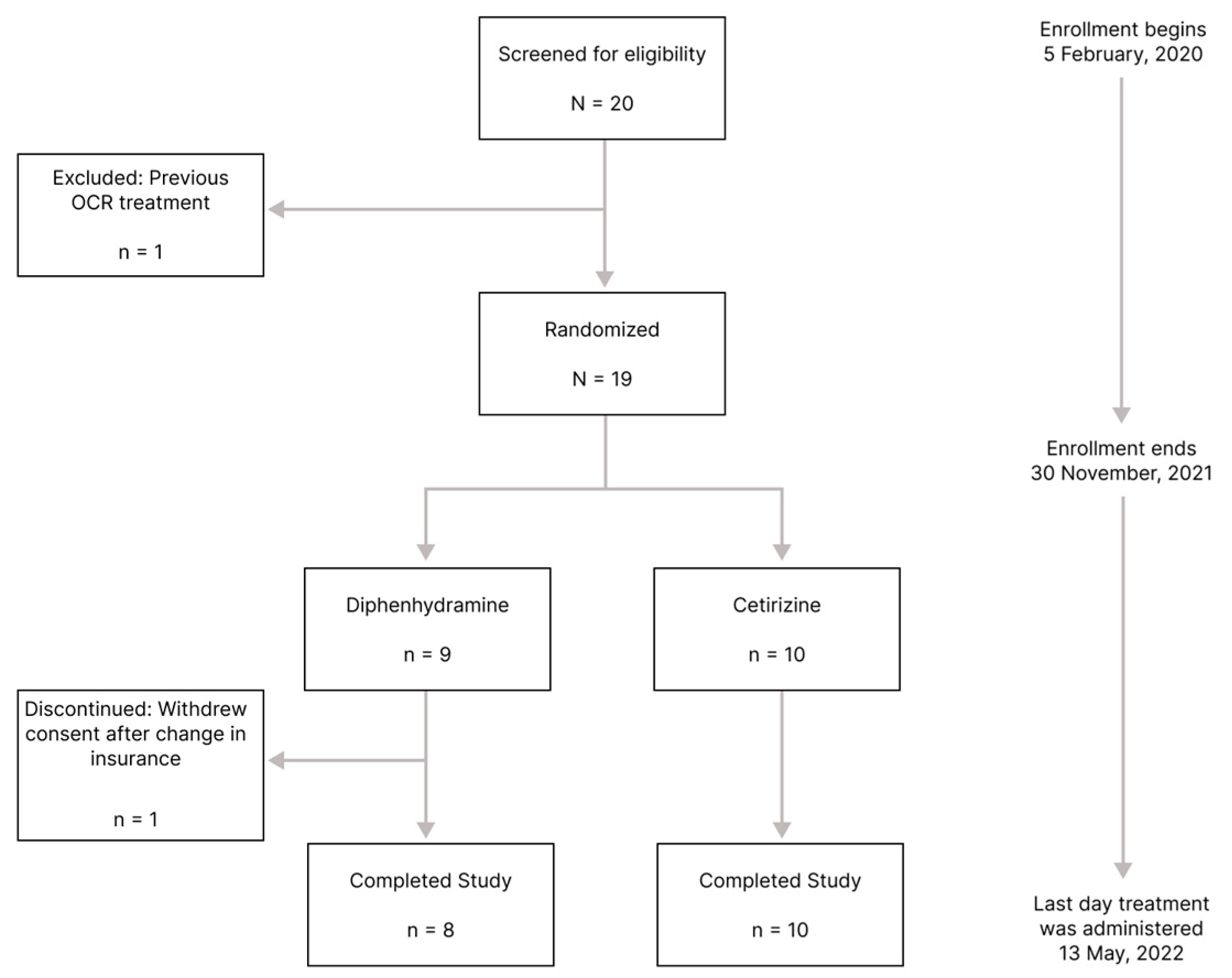
2.2. Participants and Setting
2.3. Interventions
2.4. Variables and Outcomes
2.4.1. Adverse Events
2.4.2. Neurological Exams and Patient-Reported Outcomes
2.5. Sample Size
2.6. Randomization, Allocation, and Blinding
2.7. Statistical Methods
3. Results
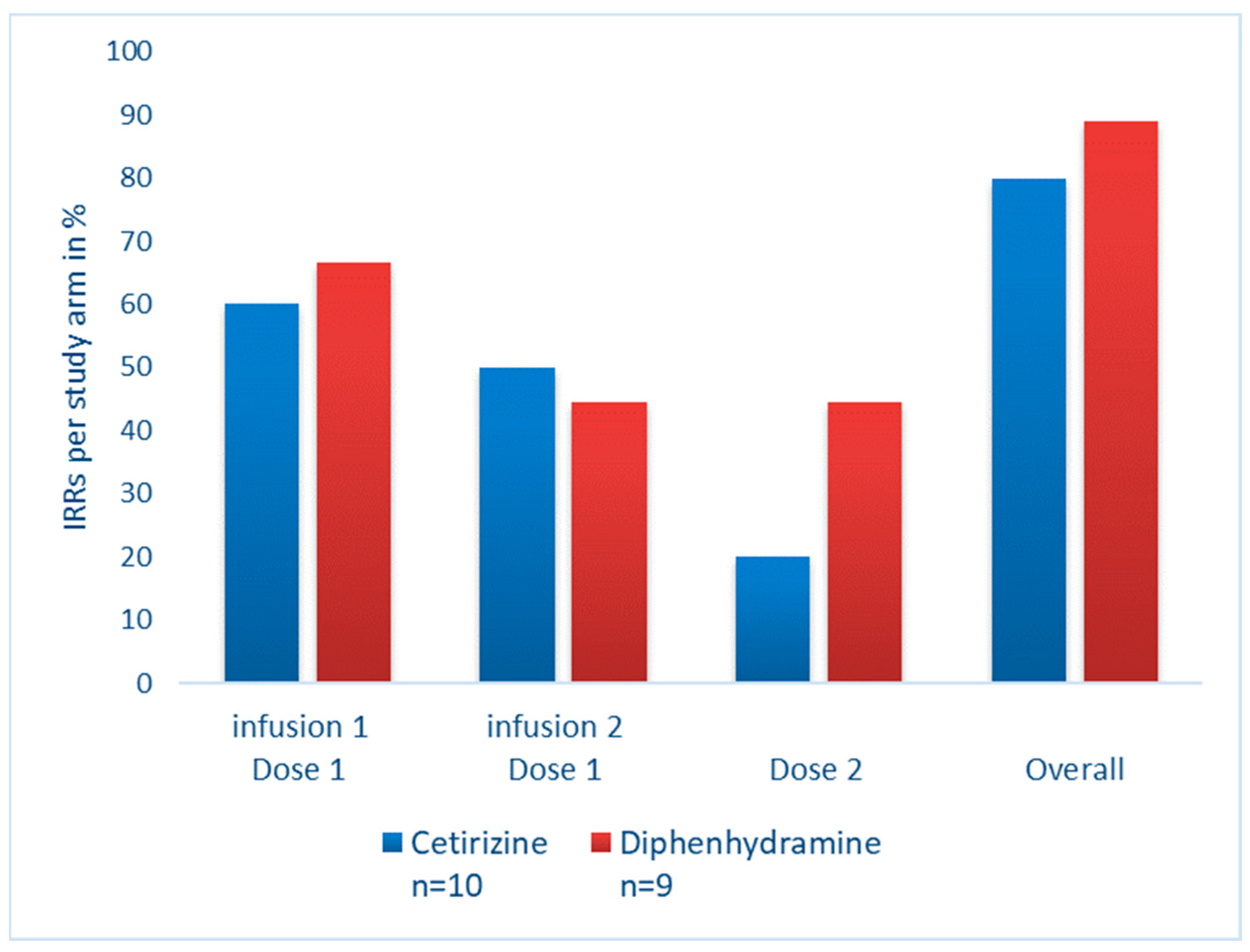
3.1. Treatment Outcomes
3.2. Incidence of Adverse Events
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Hauser, S.L.; Bar-Or, A.; Comi, G.; Giovannoni, G.; Hartung, H.-P.; Hemmer, B.; Lublin, F.; Montalban, X.; Rammohan, K.W.; Selmaj, K.; et al. Ocrelizumab versus Interferon Beta-1a in Relapsing Multiple Sclerosis. N. Engl. J. Med. 2017, 376, 221–234. [Google Scholar] [CrossRef]
- Montalban, X.; Hauser, S.L.; Kappos, L.; Arnold, D.L.; Bar-Or, A.; Comi, G.; de Seze, J.; Giovannoni, G.; Hartung, H.-P.; Hemmer, B.; et al. Ocrelizumab versus Placebo in Primary Progressive Multiple Sclerosis. N. Engl. J. Med. 2017, 376, 209–220. [Google Scholar] [CrossRef] [PubMed]
- Blaiss, M.S.; Bernstein, J.A.; Kessler, A.; Pines, J.M.; Camargo, C.A.; Fulgham, P.; Haumschild, R.; Rupp, K.; Tyler, T.; Moellman, J. The Role of Cetirizine in the Changing Landscape of IV Antihistamines: A Narrative Review. Adv. Ther. 2022, 39, 178–192. [Google Scholar] [CrossRef] [PubMed]
- ALMuhizi, F.; De Las Vecillas Sanchez, L.; Gilbert, L.; Copaescu, A.M.; Isabwe, G.A.C. Premedication Protocols to Prevent Hypersensitivity Reactions to Chemotherapy: A Literature Review. Clin. Rev. Allergy Immunol. 2022, 62, 534–547. [Google Scholar] [CrossRef] [PubMed]
- Holmes, J.P.; Peguero, J.A.; Garland, R.C.; North, J.; Young, S.; Brent, L.D.; Joseph-Ridge, N. Intravenous Cetirizine vs Intravenous Diphenhydramine for the Prevention of Hypersensitivity Infusion Reactions: Results of an Exploratory Phase 2 Study. J. Infus. Nurs. 2021, 44, 315–322. [Google Scholar] [CrossRef] [PubMed]
- Conte, W.L.; Arndt, N.; Cipriani, V.P.; Dellaria, A.; Javed, A. Reduction in ocrelizumab-induced infusion reactions by a modified premedication protocol. Mult. Scler. Relat. Disord. 2019, 27, 397–399. [Google Scholar] [CrossRef] [PubMed]
- Ocrevus: Highlights of Prescribing Information [Internet]. Available online: https://www.accessdata.fda.gov/drugsatfda_docs/label/2020/761053s022lbl.pdf (accessed on 17 March 2023).
- Mayer, L.; Kappos, L.; Racke, M.K.; Rammohan, K.; Traboulsee, A.; Hauser, S.L.; Julian, L.; Köndgen, H.; Li, C.; Napieralski, J.; et al. Ocrelizumab infusion experience in patients with relapsing and primary progressive multiple sclerosis: Results from the phase 3 randomized OPERA I, OPERA II, and ORATORIO studies. Mult. Scler. Relat. Disord. 2019, 30, 236–243. [Google Scholar] [CrossRef] [PubMed]
- Akgün, K.; Behrens, J.; Schriefer, D.; Ziemssen, T. Acute Effects of Ocrelizumab Infusion in Multiple Sclerosis Patients. Int. J. Mol. Sci. 2022, 23, 13759. [Google Scholar] [CrossRef] [PubMed]
- Doessegger, L.; Banholzer, M.L. Clinical development methodology for infusion-related reactions with monoclonal antibodies. Clin. Transl. Immunol. 2015, 4, e39. [Google Scholar] [CrossRef] [PubMed]
- Tan, Y.Y.; Papez, V.; Chang, W.H.; Mueller, S.H.; Denaxas, S.; Lai, A.G. Comparing clinical trial population representativeness to real-world populations: An external validity analysis encompassing 43,895 trials and 5,685,738 individuals across 989 unique drugs and 286 conditions in England. Lancet Healthy Longev. 2022, 3, e674–e689. [Google Scholar] [CrossRef] [PubMed]
- Kimby, E. Tolerability and safety of rituximab (MabThera). Cancer Treat. Rev. 2005, 31, 456–473. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Arm | |||||
|---|---|---|---|---|---|
| Relapsing or Progressive MS | Total (N = 19) 1 | Cetirizine (n = 10, 53%) 1 | Diphenhydramine (n = 9, 47%) 1 | p-Value 2 | |
| Age at MS symptoms onset (years) | 33.9 [19.4, 56.4] | 33.7 [29.5, 47.0] | 33.9 [30.0, 36.5] | 0.87 | |
| Age at MS diagnosis (years) | 34.6 [19.8, 63.1] | 34.5 [29.6, 47.1] | 36.7 [30.1, 45.3] | 0.99 | |
| From MS symptoms onset to MS diagnosis (weeks) | 8.6 [0, 465] | 7.4 [2.5, 25.9] | 8.6 [5.4, 209] | 0.27 | |
| Age at OCR start (years) | 47.5 [29.0, 63.2] | 48.2 [38.0, 54.0] | 46.3 [39.8, 52.2] | 0.97 | |
| Gender, n (%) | Female | 15 (78.9%) | 9 (90.0%) | 6 (66.7%) | 0.30 |
| Race, n (%) | Asian | 1 (5.3%) | 1 (10.0%) | 0 (0.0%) | 0.99 |
| Black or African American | 2 (10.5%) | 1 (10.0%) | 1 (11.1%) | ||
| Other | 1 (5.3%) | 0 (0%) | 1 (11.1%) | ||
| White | 15 (78.9%) | 8 (80.0%) | 7 (77.8%) | ||
| Ethnicity, n (%) | Hispanic or Latino | 1 (5.3%) | 1 (10.0%) | 0 (0%) | 0.99 |
| Not Hispanic or Latino | 18 (94.7%) | 9 (90.0%) | 9 (100%) | ||
| Education, n (%) | High school | 2 (10.5%) | 1 (10.0%) | 1 (11.1%) | 0.17 |
| Trade school | 1 (5.3%) | 0 (0%) | 1 (11.1%) | ||
| Associate’s degree | 5 (26.3%) | 1 (10.0%) | 4 (44.4%) | ||
| Bachelor’s degree | 8 (42.1%) | 5 (50.0%) | 3 (33.3%) | ||
| Graduate school | 3 (15.8%) | 3 (30.0%) | 0 (0.0%) | ||
| Employment, n (%) | Disabled | 2 (10.5%) | 1 (10.0%) | 1 (11.1%) | 0.10 |
| Full-time | 12 (63.2%) | 5 (50.0%) | 7 (77.8%) | ||
| Not working | 4 (21.1%) | 4 (40.0%) | 0 (0.0%) | ||
| Retired | 1 (5.3%) | 0 (0%) | 1 (11.1%) | ||
| MS type, n (%) | PPMS | 1 (5.3%) | 0 (0%) | 1 (11.1%) | 0.09 |
| RRMS | 16 (84.2%) | 10 (100%) | 6 (66.7%) | ||
| SPMS | 2 (10.5%) | 0 (0%) | 2 (22.2%) | ||
| Reason for OCR start, n (%) | Breakthrough disease activity on previous treatment | 8 (42.1%) | 5 (50.0%) | 3 (33.3%) | 0.60 |
| Convenience | 2 (10.5%) | 0 (0%) | 2 (22.2%) | ||
| First-line therapy | 5 (26.3%) | 3 (30.0%) | 2 (22.2%) | ||
| Risk reduction from prior treatment | 3 (15.8%) | 1 (10.0%) | 2 (22.2%) | ||
| Side effects of prior treatment | 1 (5.3%) | 1 (10.0%) | 0 (0.0%) | ||
| V1, Screening | p-Val 2 | V2, Baseline, Randomization, OCR1a | p-Val 2 | V3, OCR1b | p-Val 2 | V4, OCR2 | p-Val 2 | ||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Arm | Arm | Arm | Arm | ||||||||||
| Cetirizine (n = 10, 53%) 1 | Diphenhydramine (n = 9, 47%) 1 | Differences between Arms | Cetirizine (n = 10, 53%) 1 | Diphenhydramine (n = 9, 47%) 1 | Differences between Arms | Cetirizine (n = 10, 53%) 1 | Diphenhydramine (n = 9, 47%) 1 | Differences between Arms | Cetirizine (n = 10, 56%) 1 | Diphenhydramine (n = 8, 44%) 1 | Differences between Arms | ||
| VAS-F | Fatigue | 2.36 (2.50) | 3.13 (1.65) | 0.30 | 1.92 (2.13) | 4.10 (2.19) | 0.03 | 1.94 (1.12) | 3.95 (1.94) | 0.04 | 2.12 (2.12) | 3.52 (1.08) | 0.09 |
| Energy | 6.02 (2.80) | 5.36 (2.34) | 0.50 | 6.28 (2.56) | 5.20 (1.35) | 0.40 | 6.08 (1.80) | 4.63 (1.98) | 0.13 | 5.82 (2.43) | 5.33 (2.66) | 0.70 | |
| SSS | 1.90 (1.60) | 2.67 (0.71) | 0.02 | 1.90 (0.88) | 3.11 (1.27) | 0.20 | 2.00 (0.67) | 3.13 (1.13) | 0.30 | 2.33 (1.00) | 2.50 (0.84) | 0.03 | |
| V1, Screening | V4, OCR2 | p-Value 2 | ||||
|---|---|---|---|---|---|---|
| Arm | Arm | |||||
| Cetirizine (n = 10, 53%) 1 | Diphenhydramine (n = 9, 47%) 1 | Cetirizine (n = 10, 56%) 1 | Diphenhydramine (n = 8, 44%) 1 | Differences between Arm Means | ||
| MFIS | Physical | 9.20 (12.4) | 15.2 (8.98) | 8.90 (12.2) | 11.6 (9.24) | 0.24 |
| Cognitive | 9.10 (10.8) | 14.1 (8.21) | 7.60 (9.85) | 9.63 (9.40) | 0.57 | |
| Psychosocial | 2.00 (3.23) | 3.11 (2.80) | 1.80 (3.08) | 2.63 (1.85) | 0.15 | |
| Total | 20.3 (24.7) | 32.4 (15.4) | 18.3 (22.2) | 23.9 (15.9) | 0.32 | |
| MSIS-29 | MSIS29 Physical | 13.7 (25.9) | 27.0 (19.9) | 6.38 (9.31) | 19.7 (25.7) | 0.13 |
| MSIS29 Psychological | 16.3 (22.6) | 28.8 (21.4) | 12.3 (14.1) | 13.0 (10.2) | 0.90 | |
| V2, Baseline, Randomization, OCR1a | p-Value 2 | V3, OCR1b | p-Value 2 | V4, OCR2 | p-Value 2 | |||||
|---|---|---|---|---|---|---|---|---|---|---|
| Arm | Arm | Arm | ||||||||
| Cetirizine (n = 10, 53%) 1 | Diphenhydramine (n = 9, 47%) 1 | Cetirizine (n = 10, 53%) 1 | Diphenhydramine (n = 9, 47%) 1 | Cetirizine (n = 10, 56%) 1 | Diphenhydramine (n = 8, 44%) 1 | |||||
| TSQM | Global Satisfaction | 90.8 (9.99) | 88.0 (15.7) | 0.50 | 93.3 (11.7) | 88.6 (14.7) | 0.60 | 99.1 (2.67) | 91.7 (13.9) | 0.20 |
| Effectiveness | 86.7 (11.2) | 78.7 (18.2) | 0.50 | 91.7 (14.2) | 78.1 (14.0) | 0.08 | 93.5 (10.0) | 87.5 (15.6) | 0.30 | |
| Side Effects | 100 (0) | 94.4 (11.0) | 0.20 | 100 (0) | 92.7 (10.4) | 0.07 | 96.3 (11.0) | 95.8 (6.98) | 0.40 | |
| Convenience | 96.1 (5.89) | 87.6 (13.9) | 0.50 | 95.6 (7.33) | 90.3 (11.0) | 0.07 | 95.7 (10.9) | 94.4 (7.04) | 0.40 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Smoot, K.; Marginean, H.; Gervasi-Follmar, T.; Chen, C. Comparing the Risk of Infusion-Related Reactions and Tolerability in Patients Given Cetirizine or Diphenhydramine Prior to Ocrelizumab Infusion (PRECEPT). Medicina 2024, 60, 659. https://doi.org/10.3390/medicina60040659
Smoot K, Marginean H, Gervasi-Follmar T, Chen C. Comparing the Risk of Infusion-Related Reactions and Tolerability in Patients Given Cetirizine or Diphenhydramine Prior to Ocrelizumab Infusion (PRECEPT). Medicina. 2024; 60(4):659. https://doi.org/10.3390/medicina60040659
Chicago/Turabian StyleSmoot, Kyle, Horia Marginean, Tiffany Gervasi-Follmar, and Chiayi Chen. 2024. "Comparing the Risk of Infusion-Related Reactions and Tolerability in Patients Given Cetirizine or Diphenhydramine Prior to Ocrelizumab Infusion (PRECEPT)" Medicina 60, no. 4: 659. https://doi.org/10.3390/medicina60040659