

Home Indoor Environmental Quality and Attention Deficit Hyperactivity Disorder


Abstract
1. Introduction
2. Materials and Methods
3. Data Analyses and Results
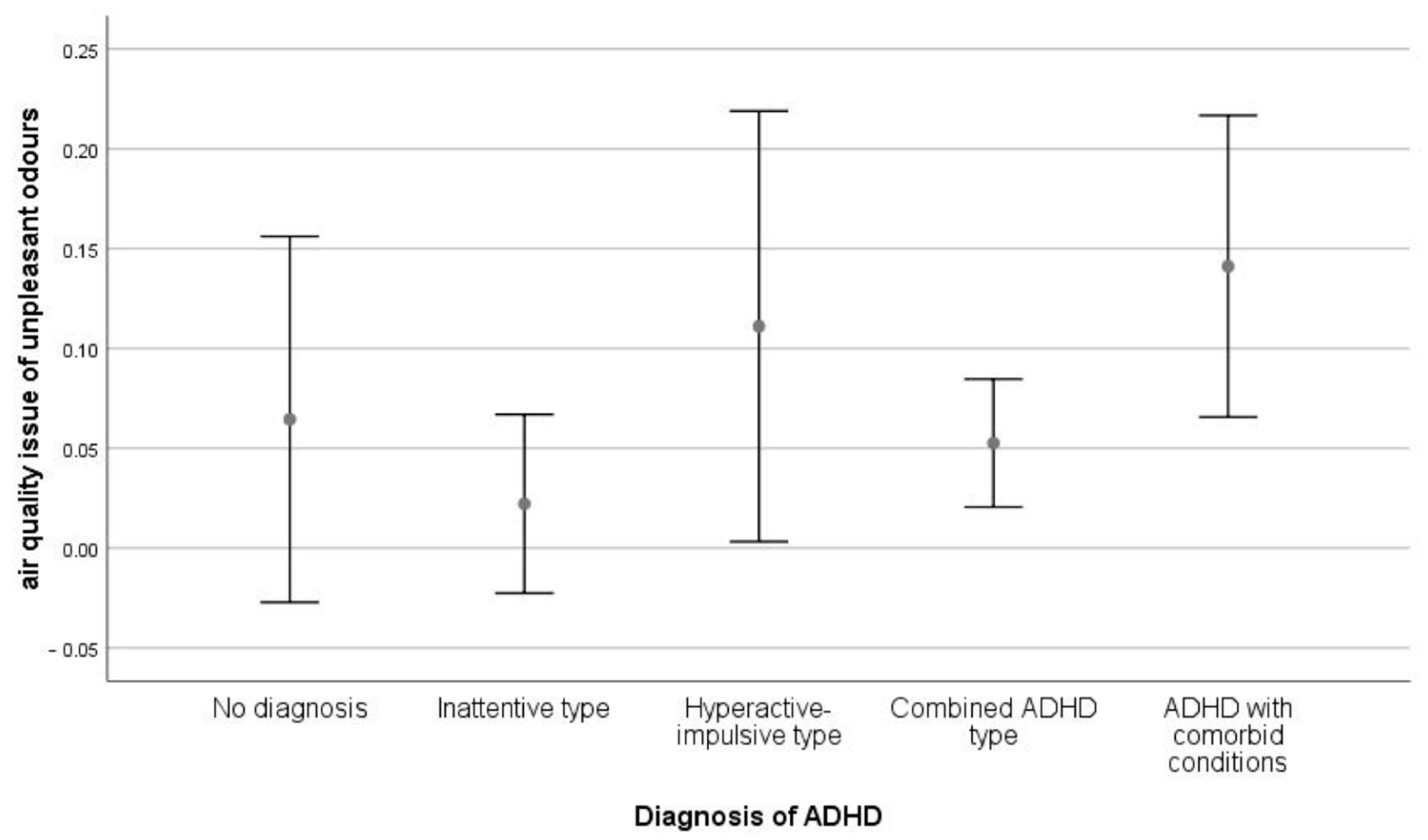
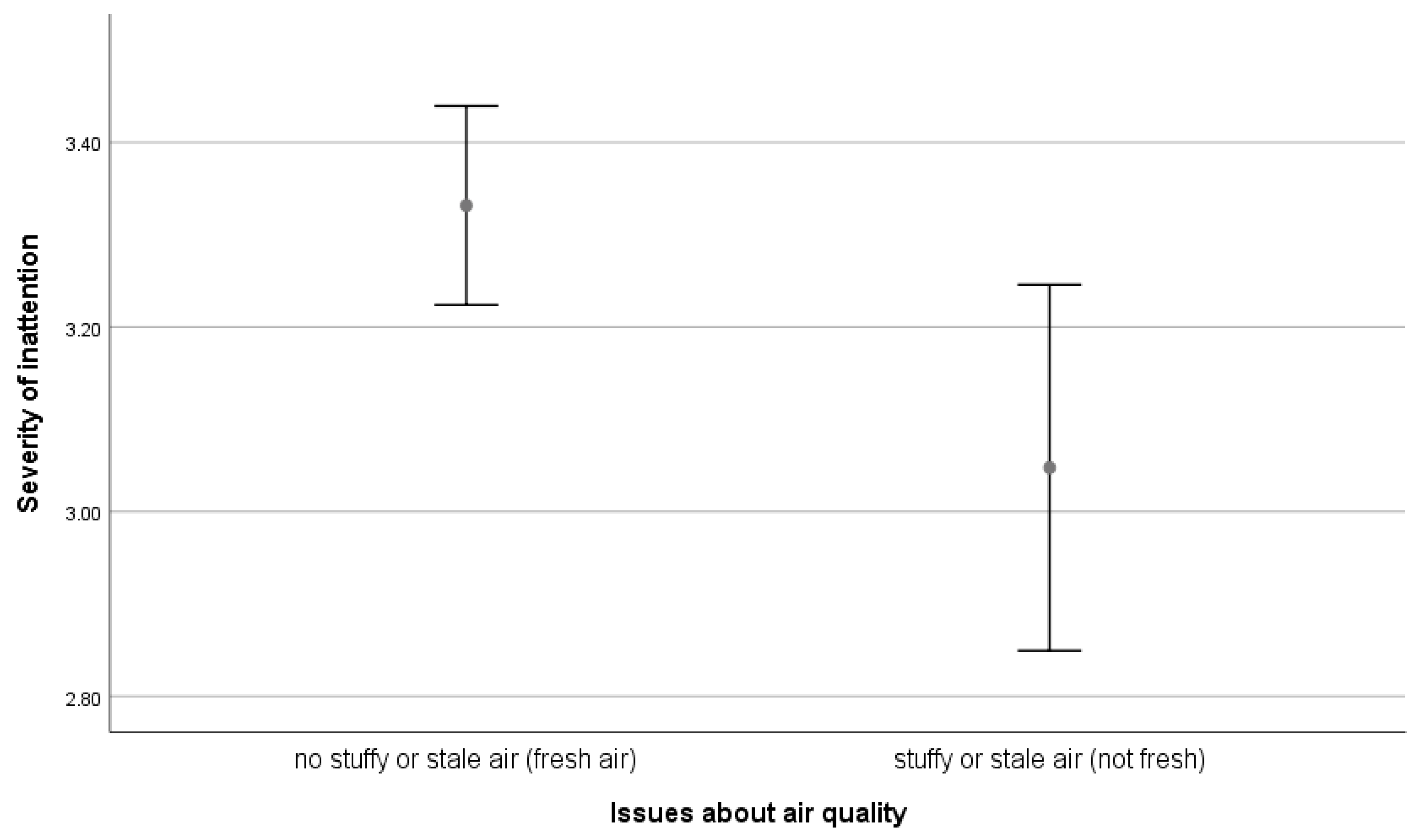
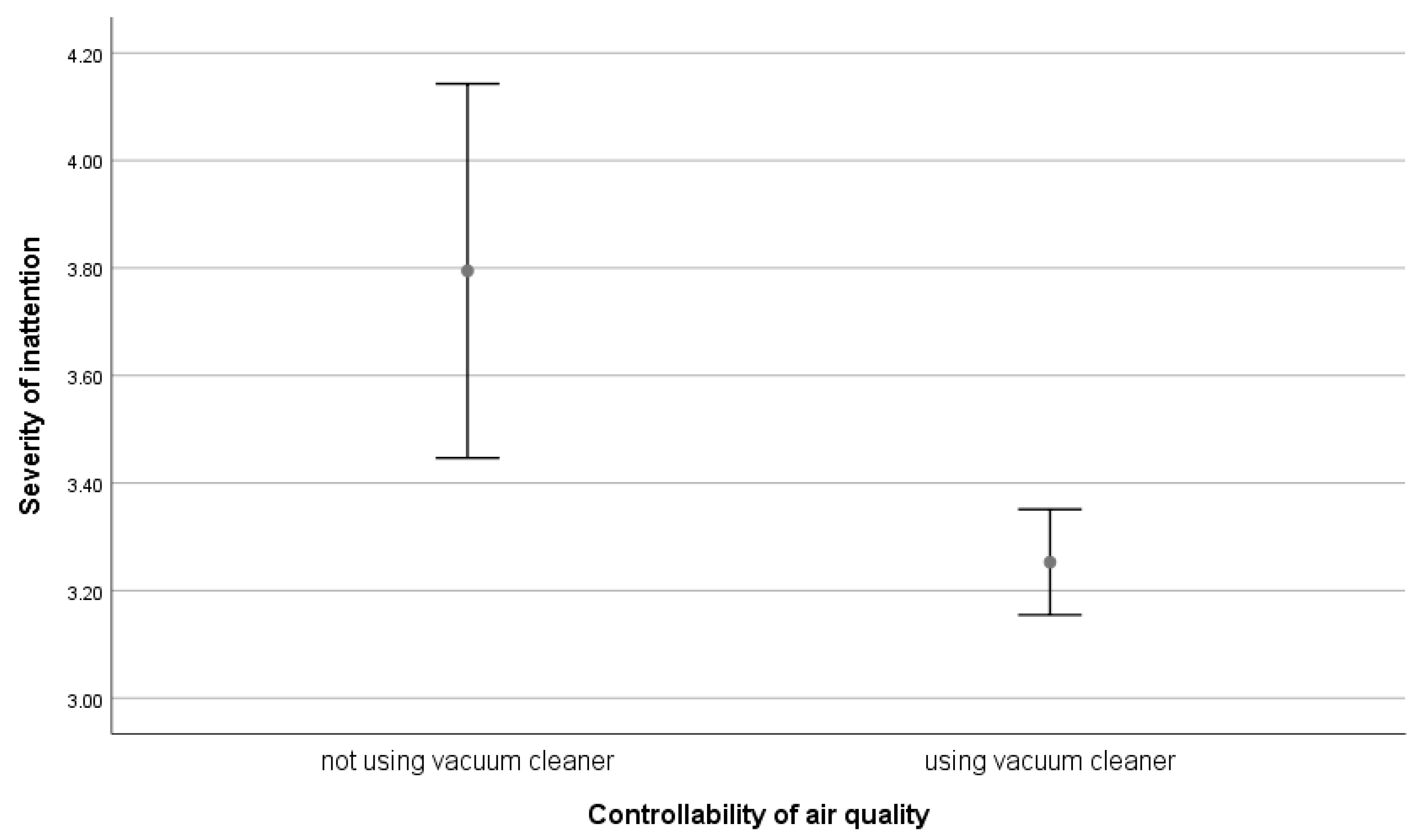
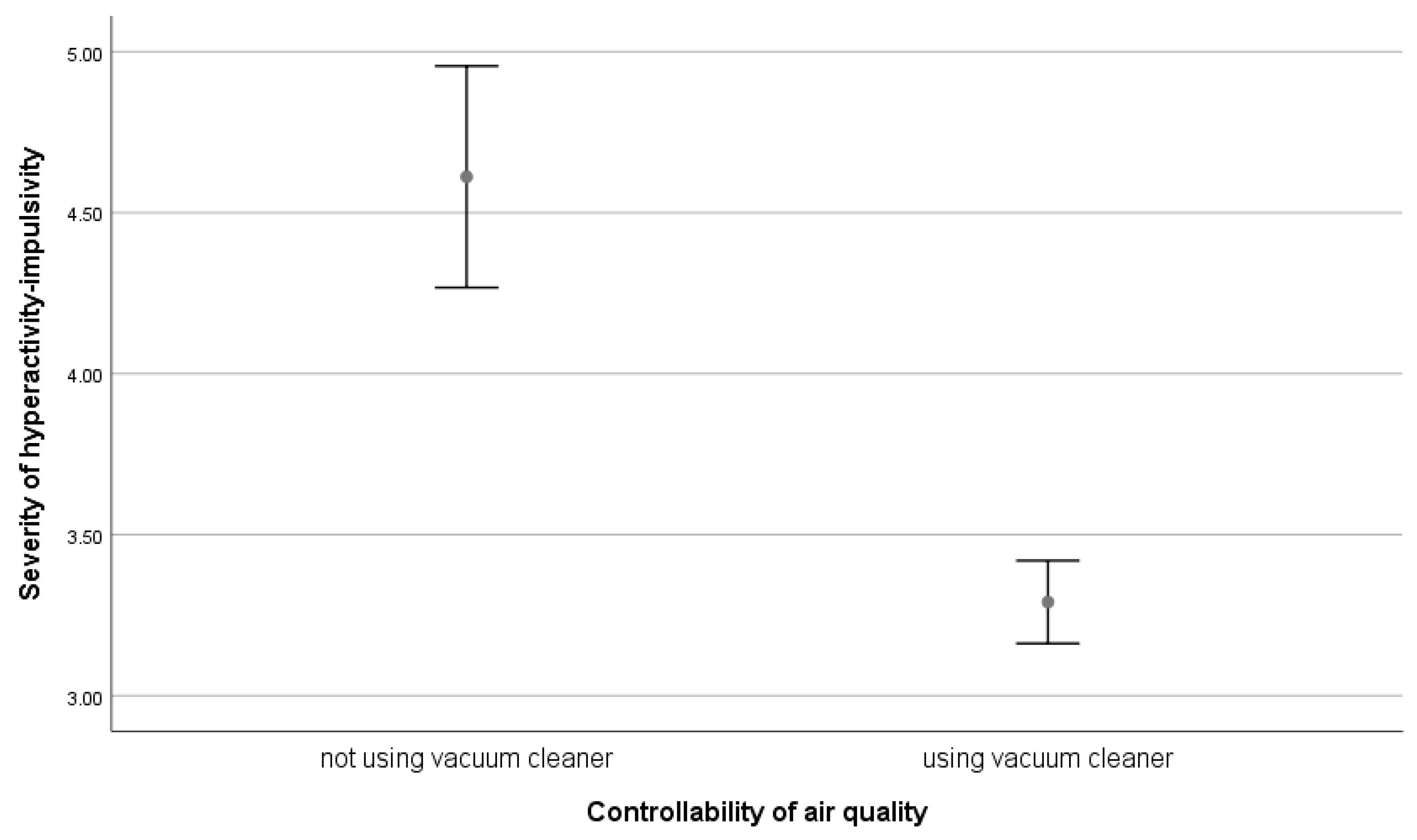
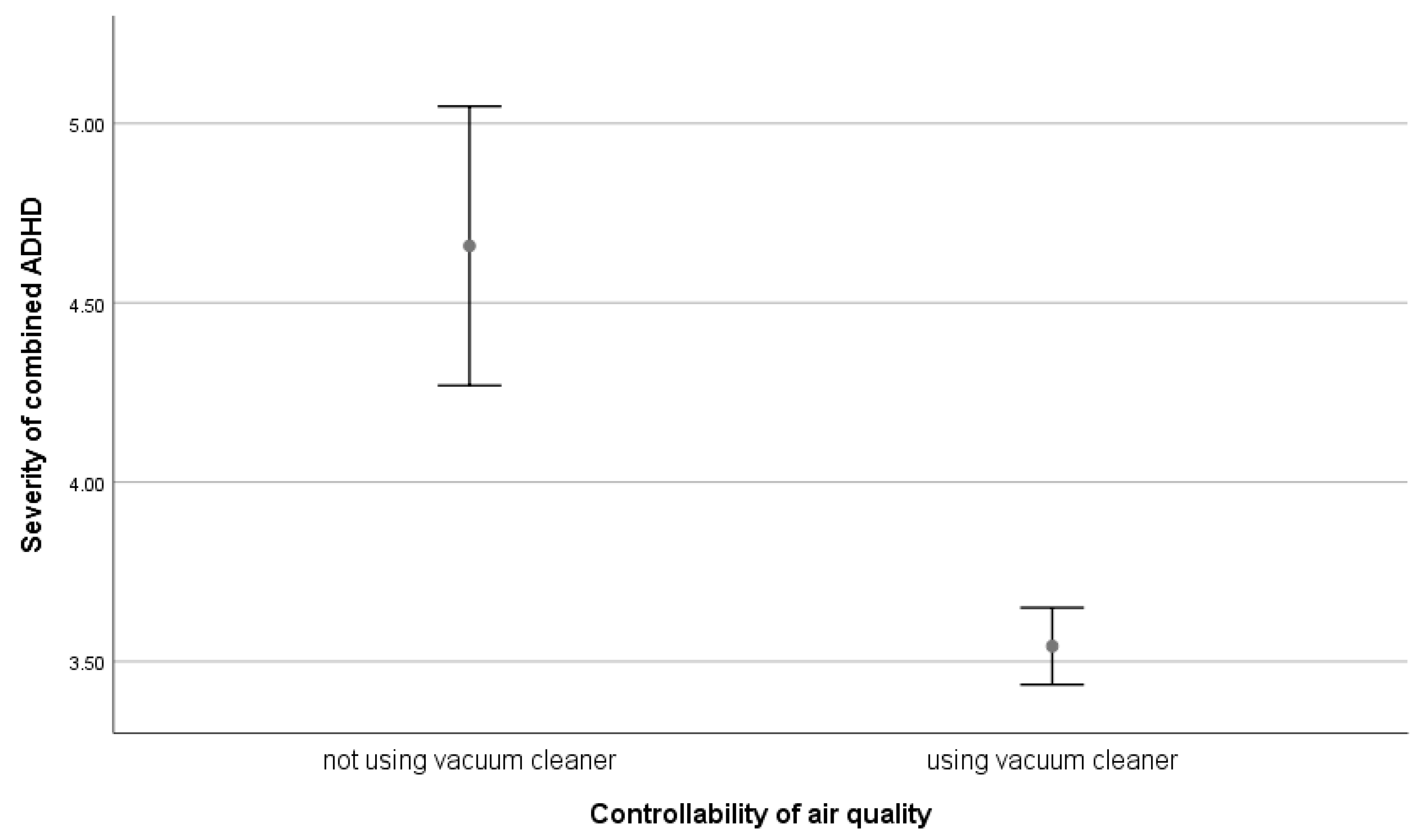
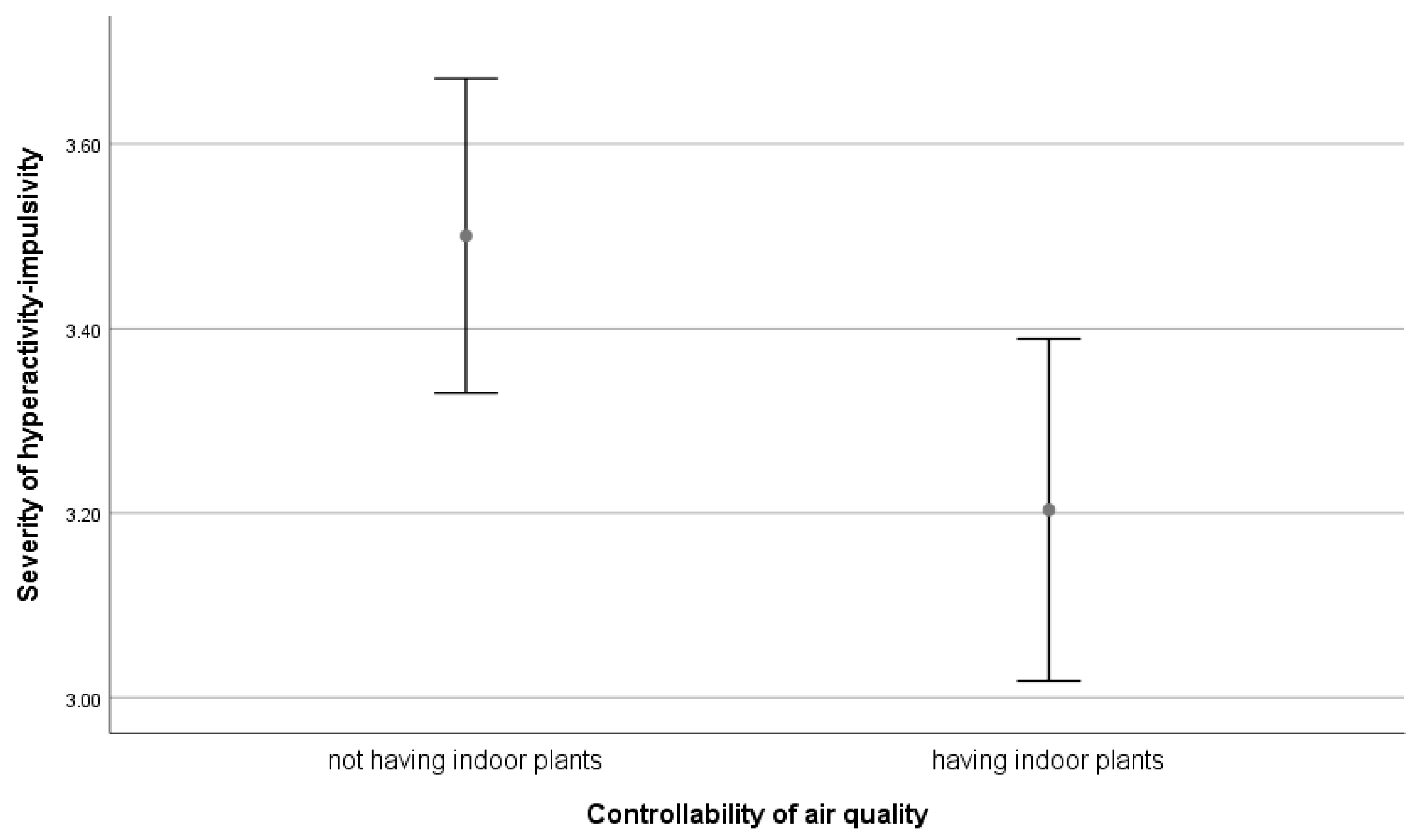
3.1. ADHD and Air Quality
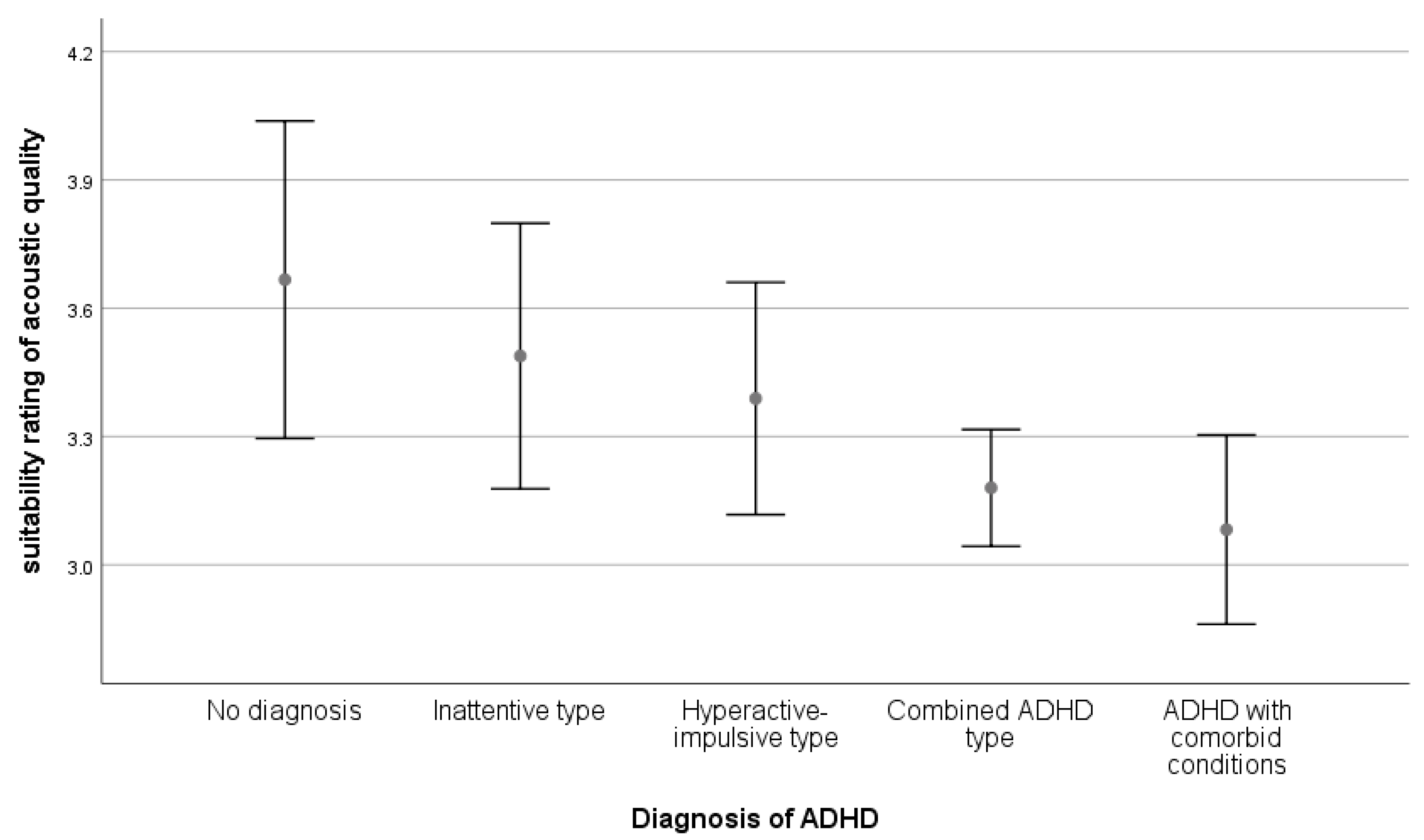
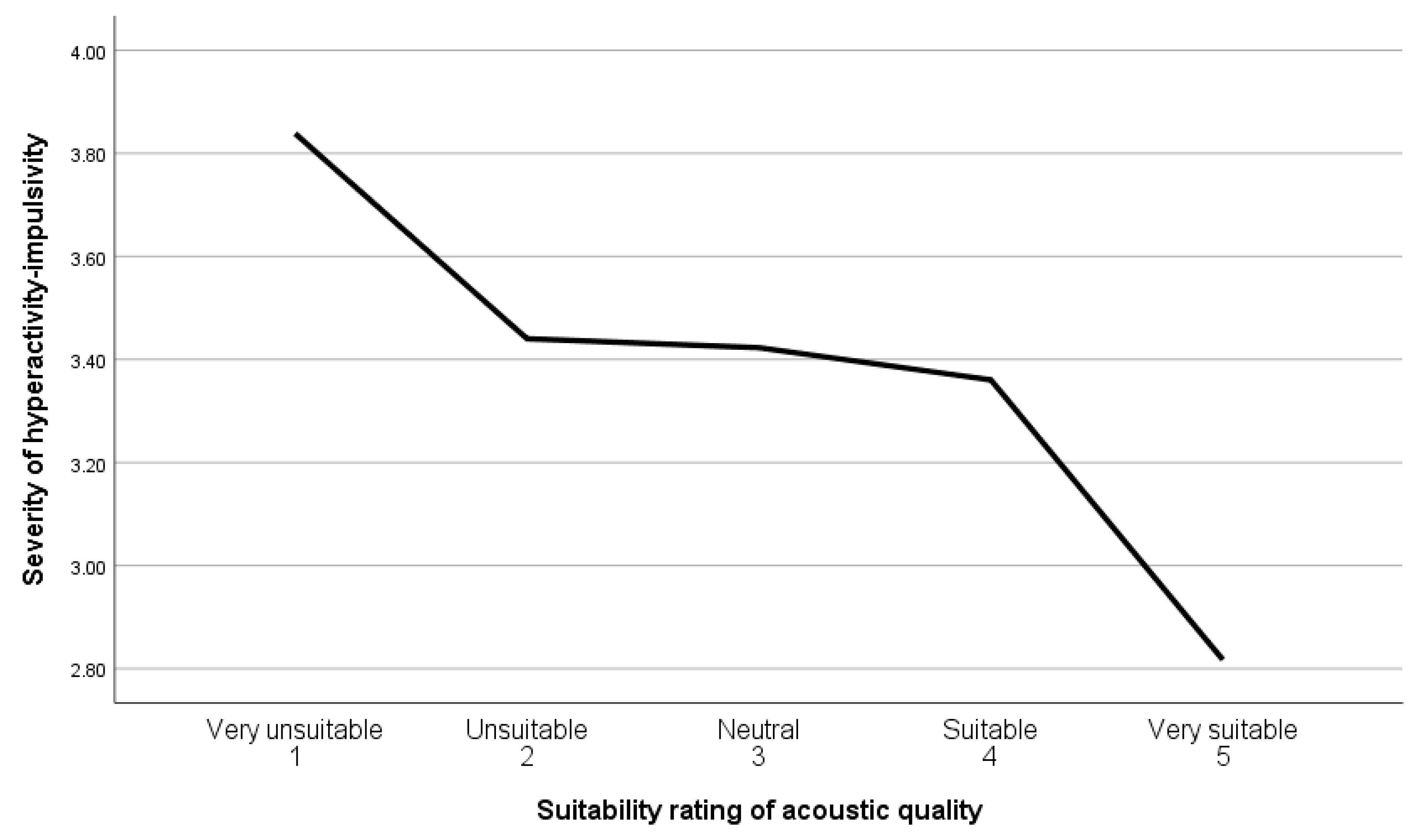
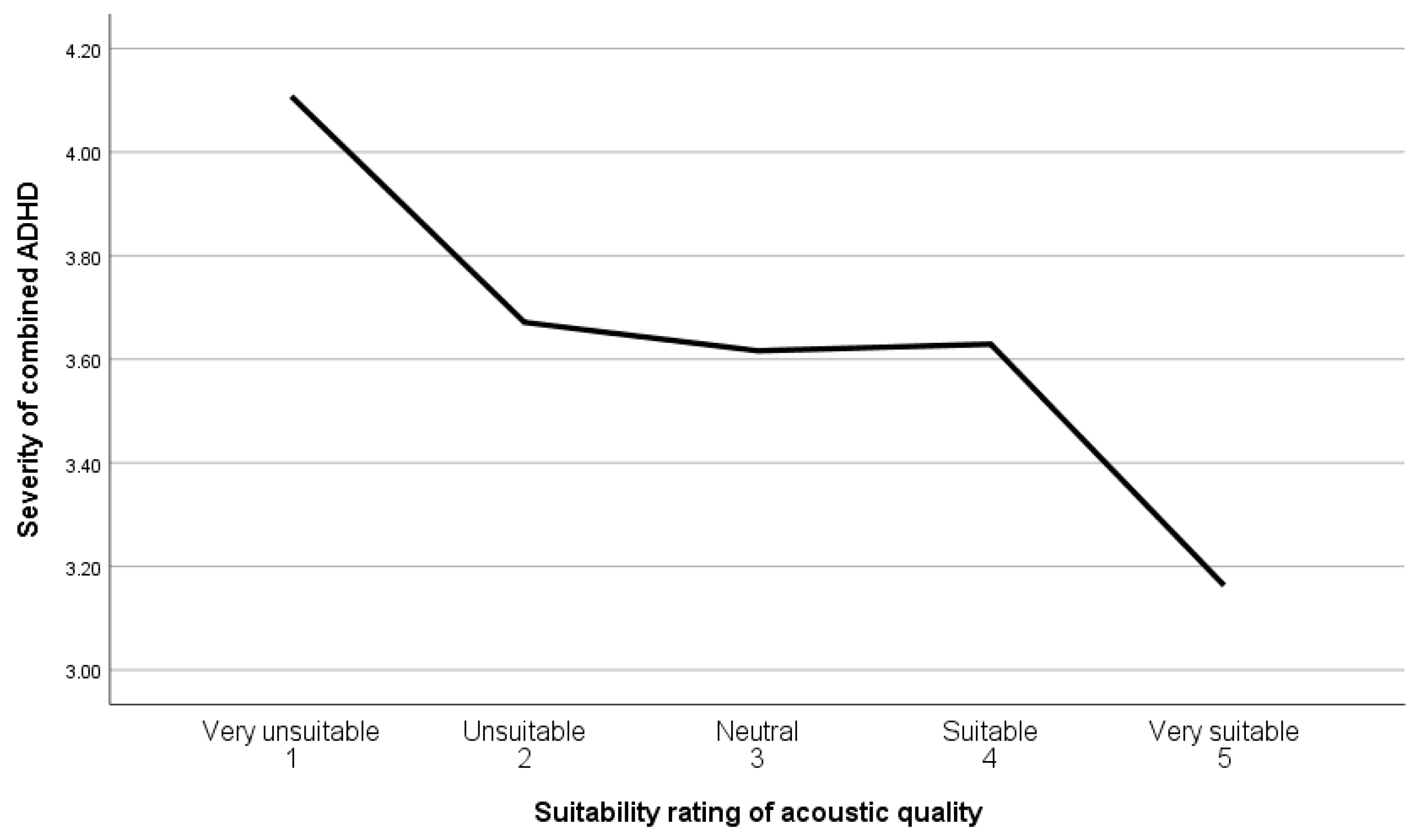
3.2. ADHD and Acoustic Quality
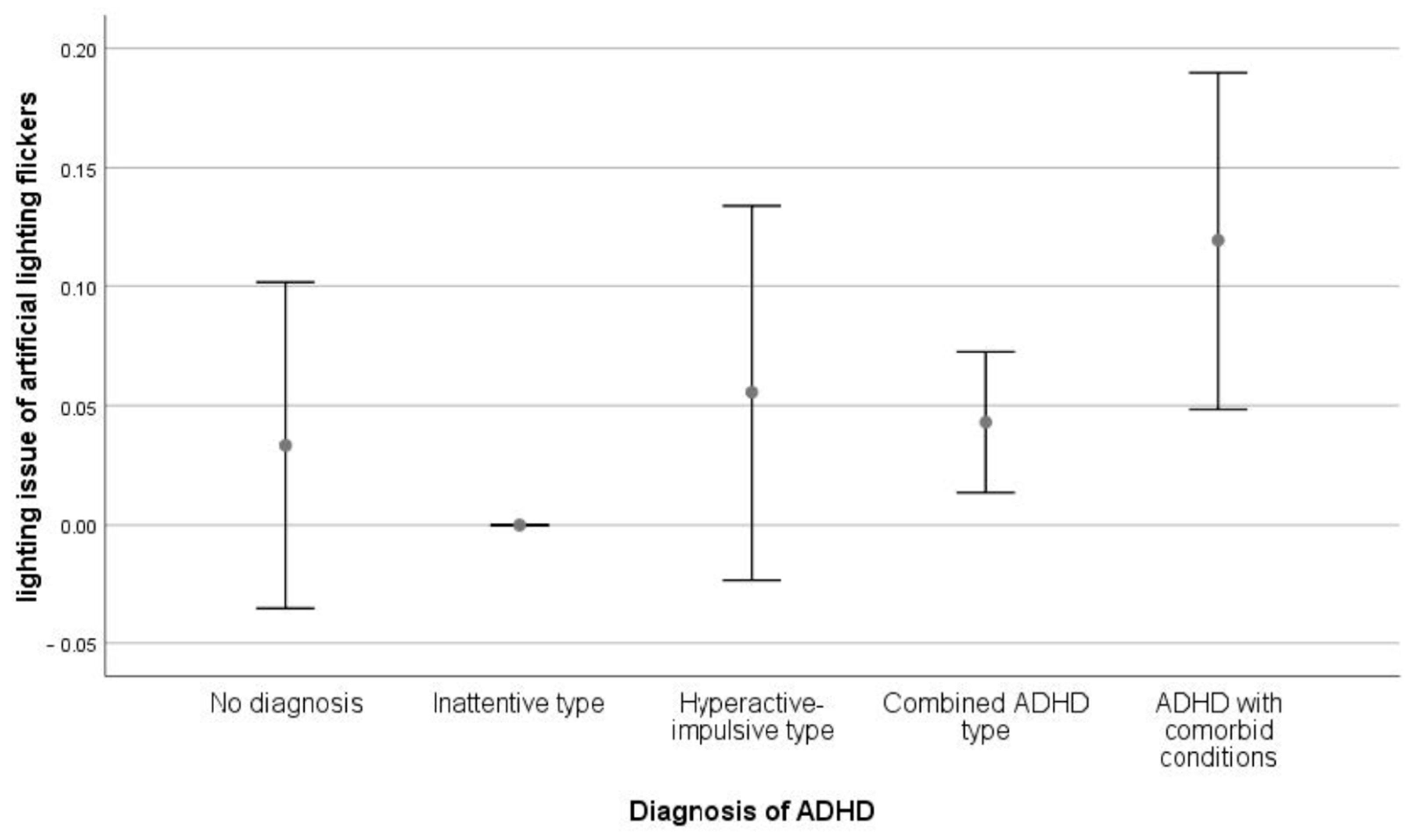
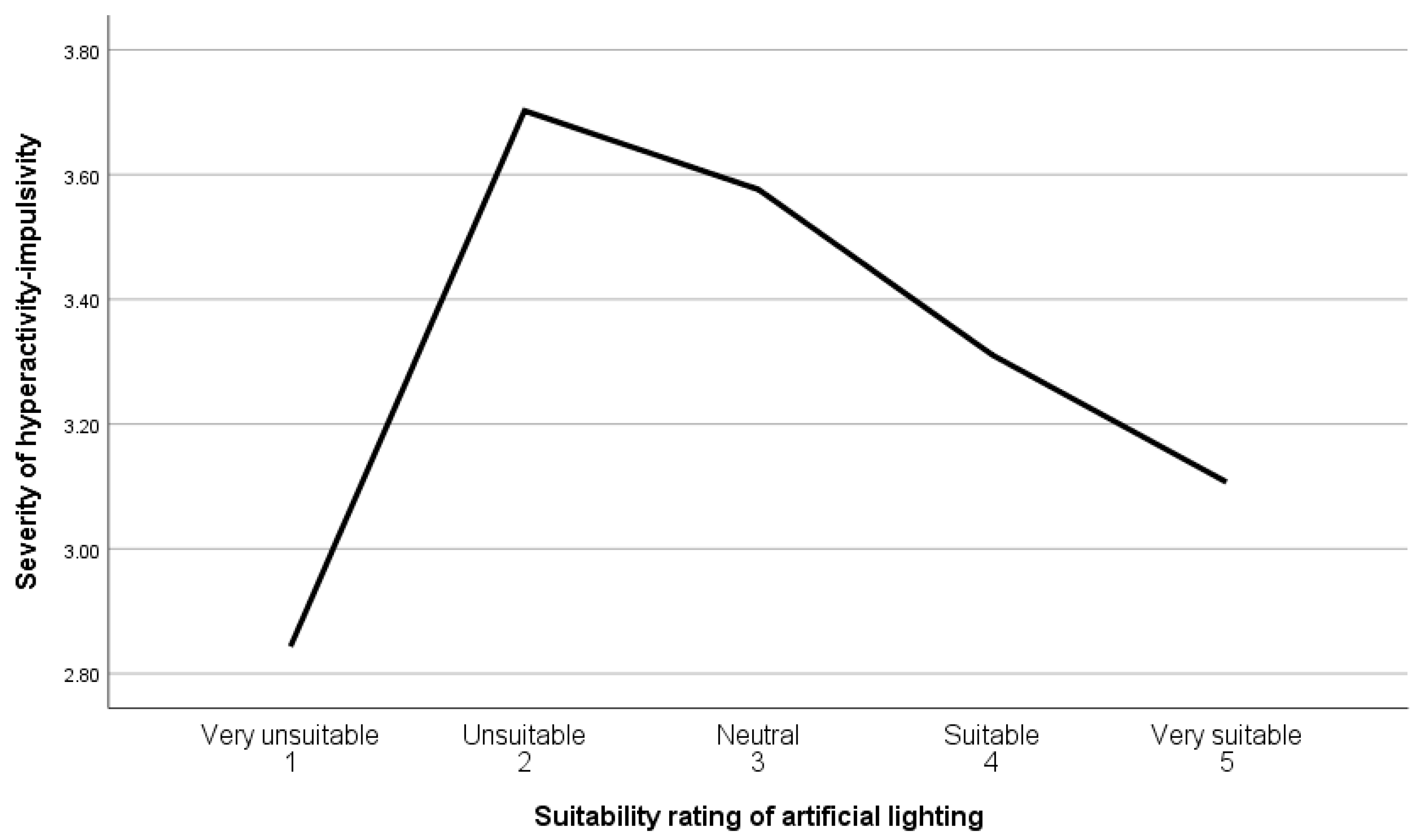
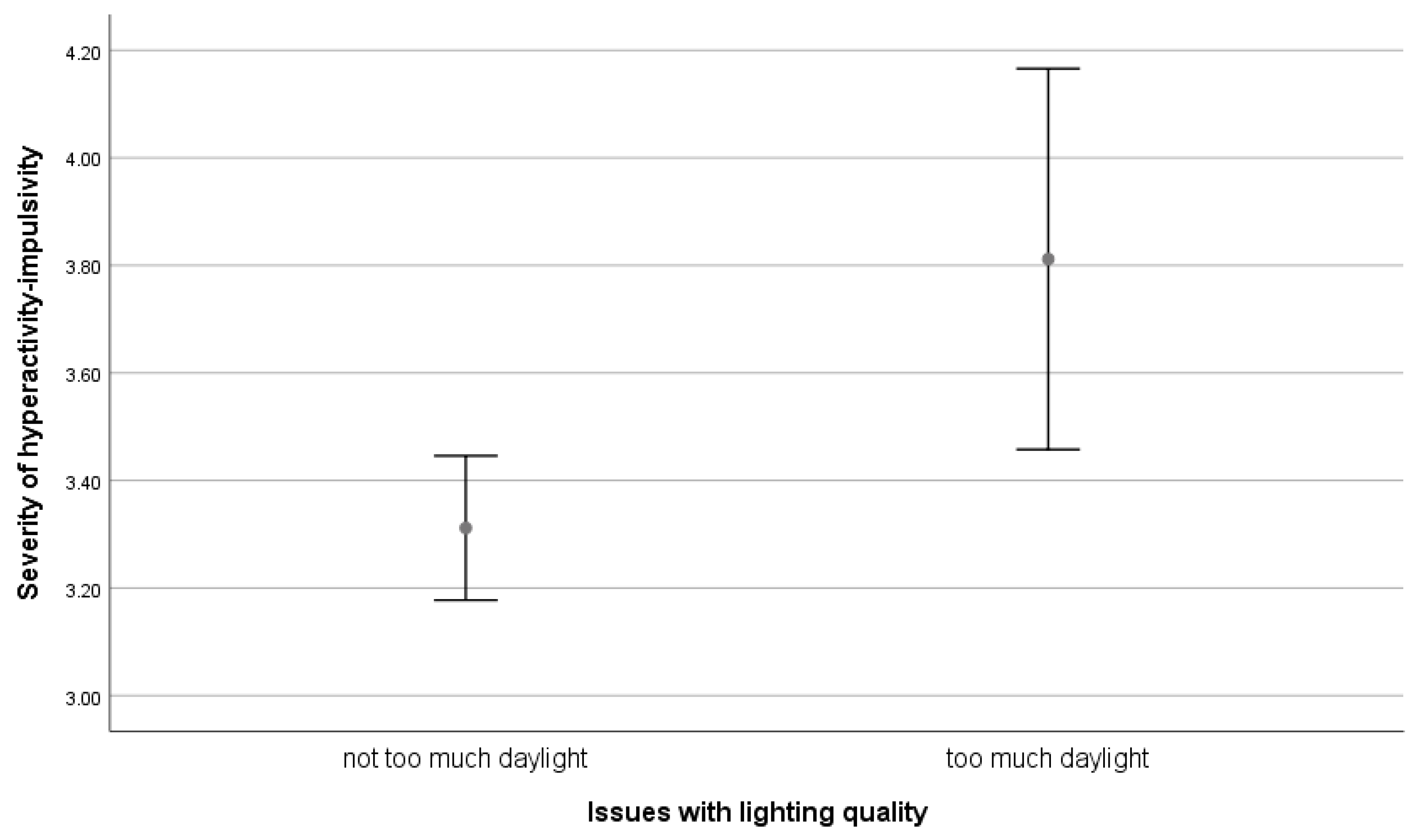
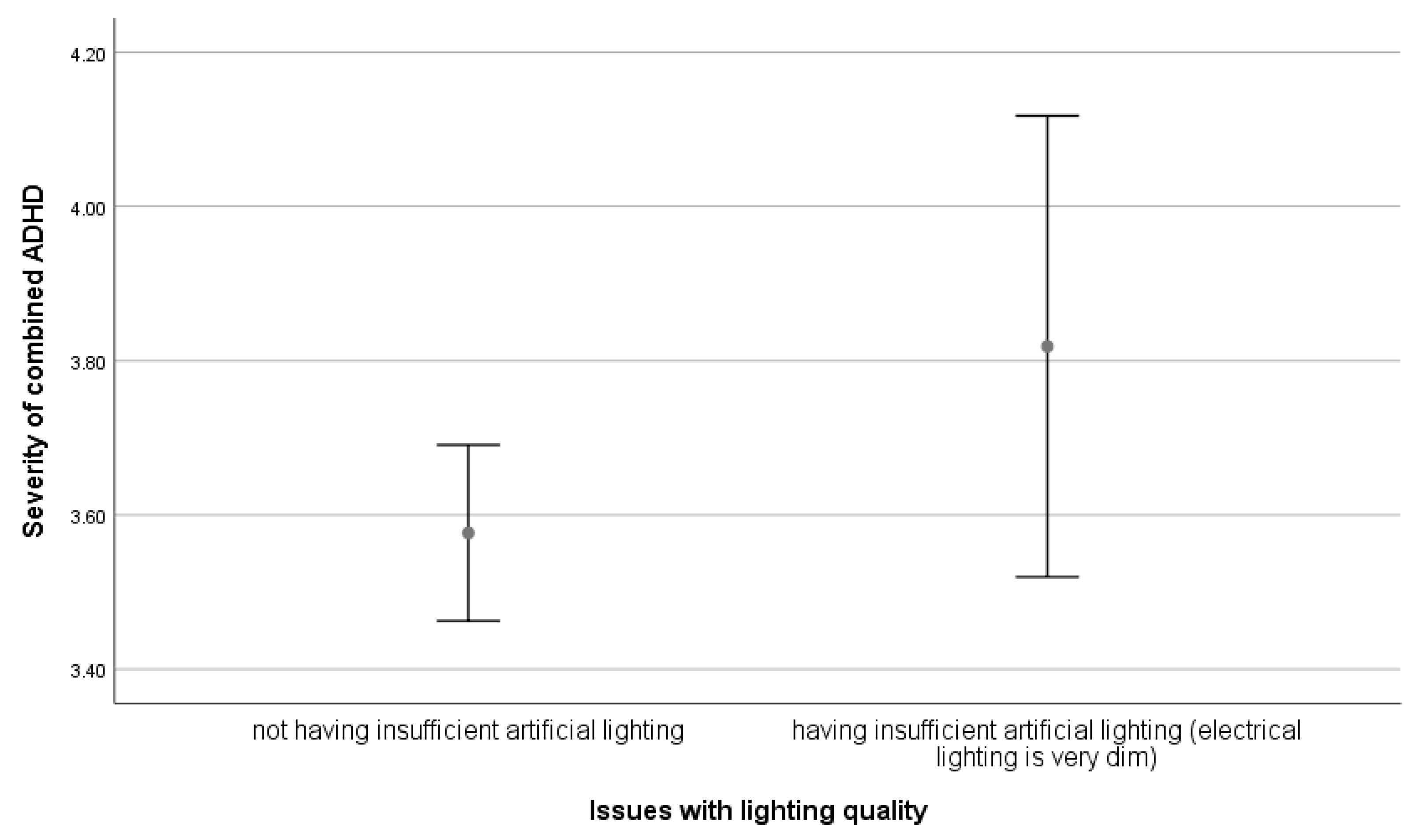
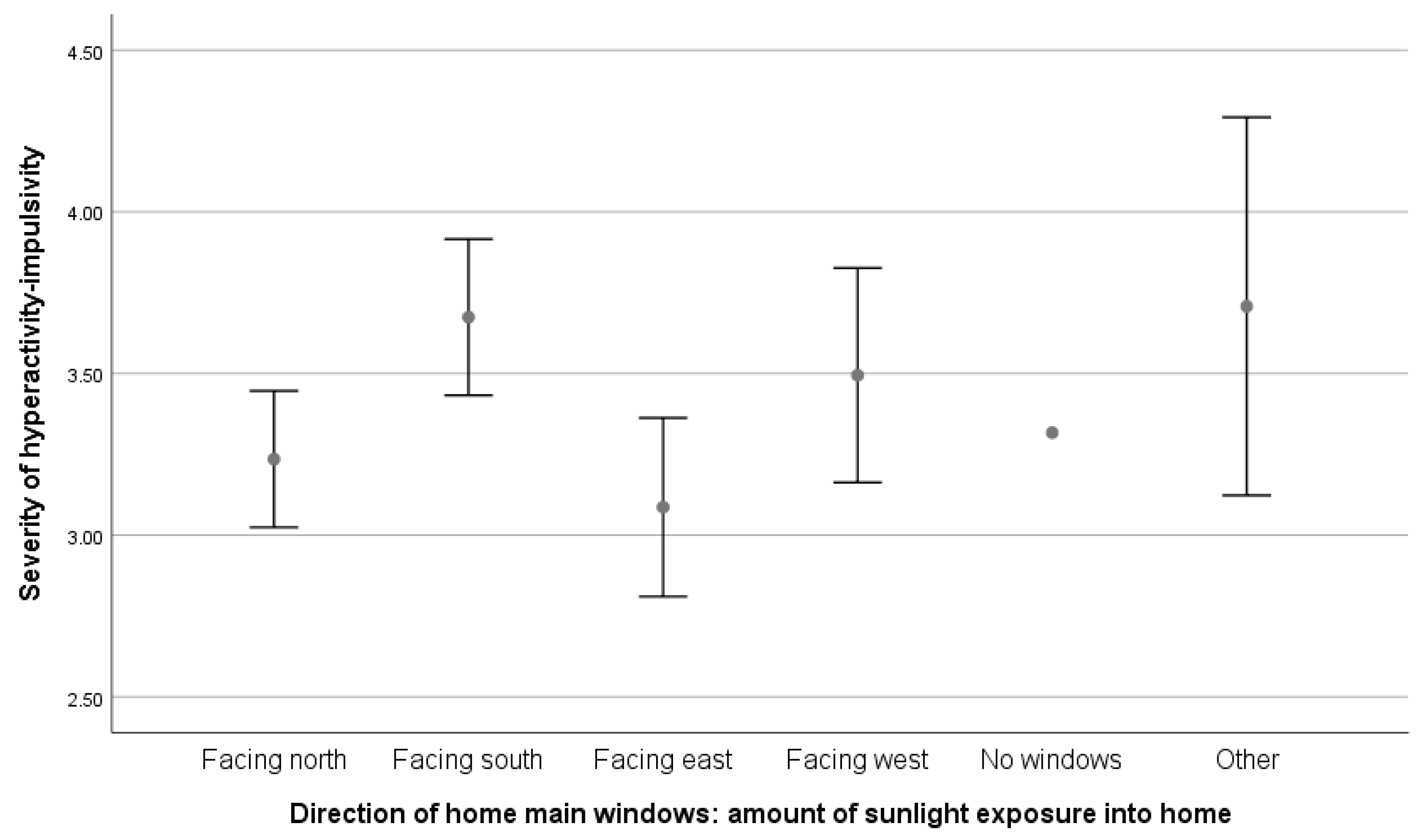
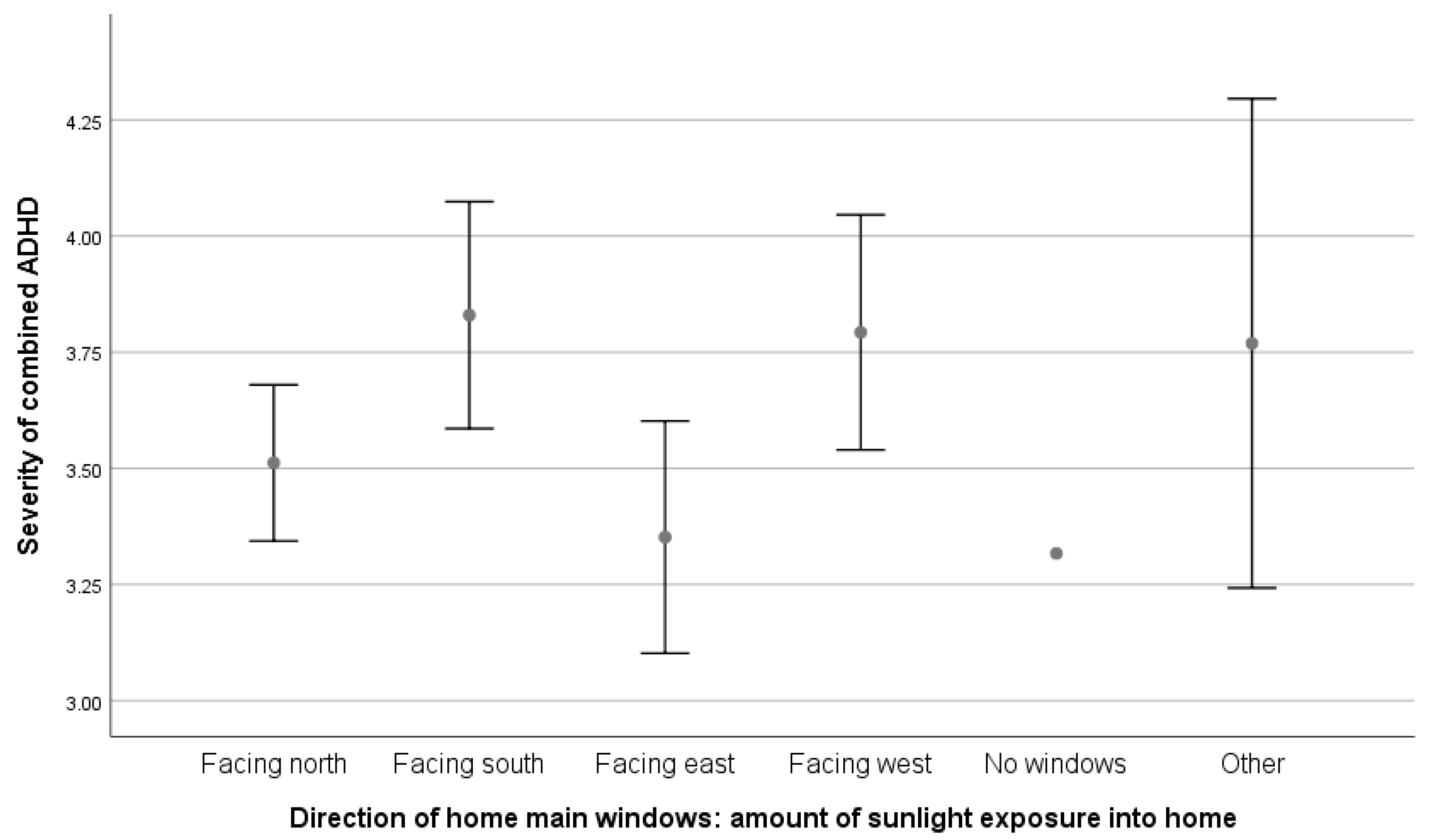
3.3. ADHD and Lighting Quality
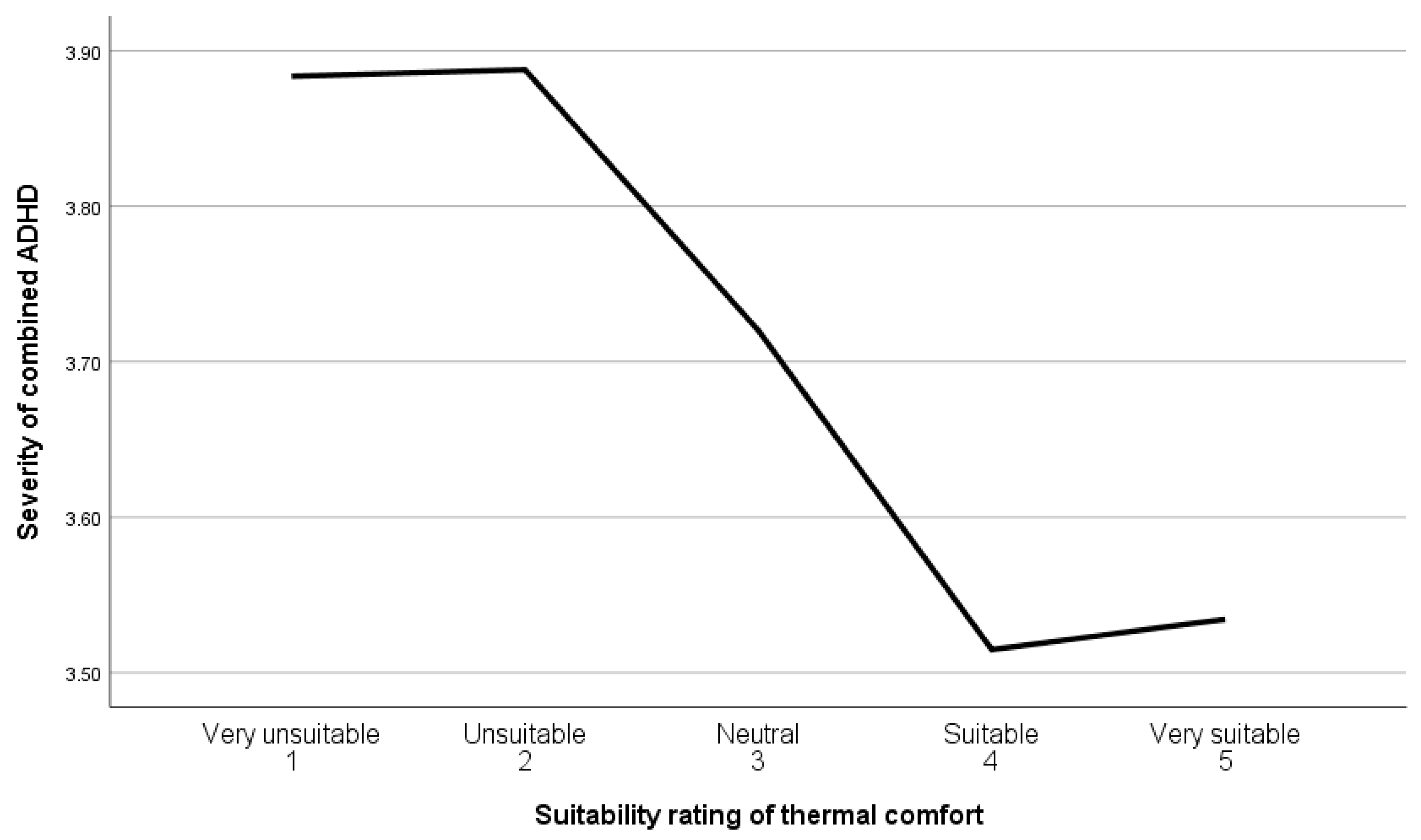
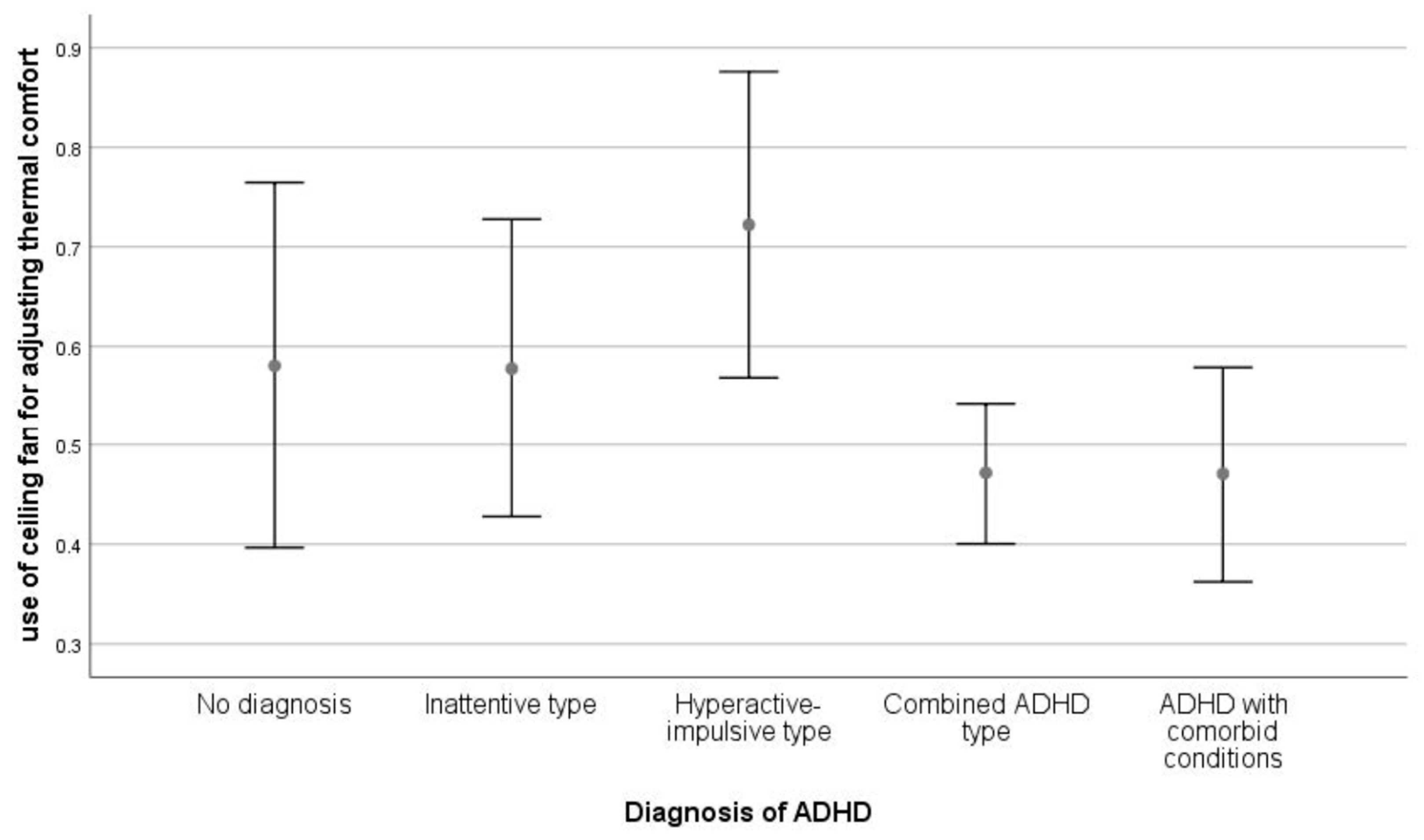
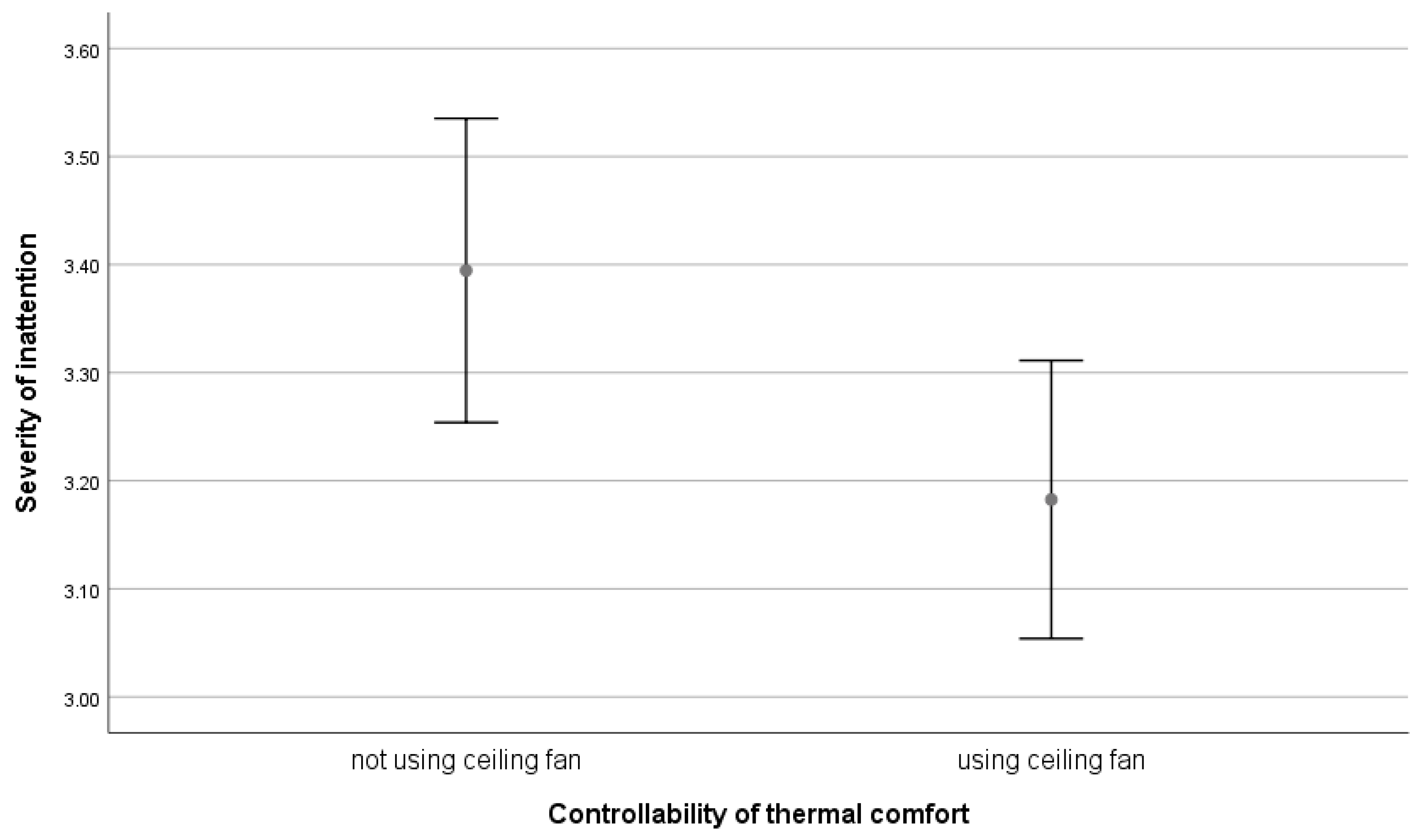
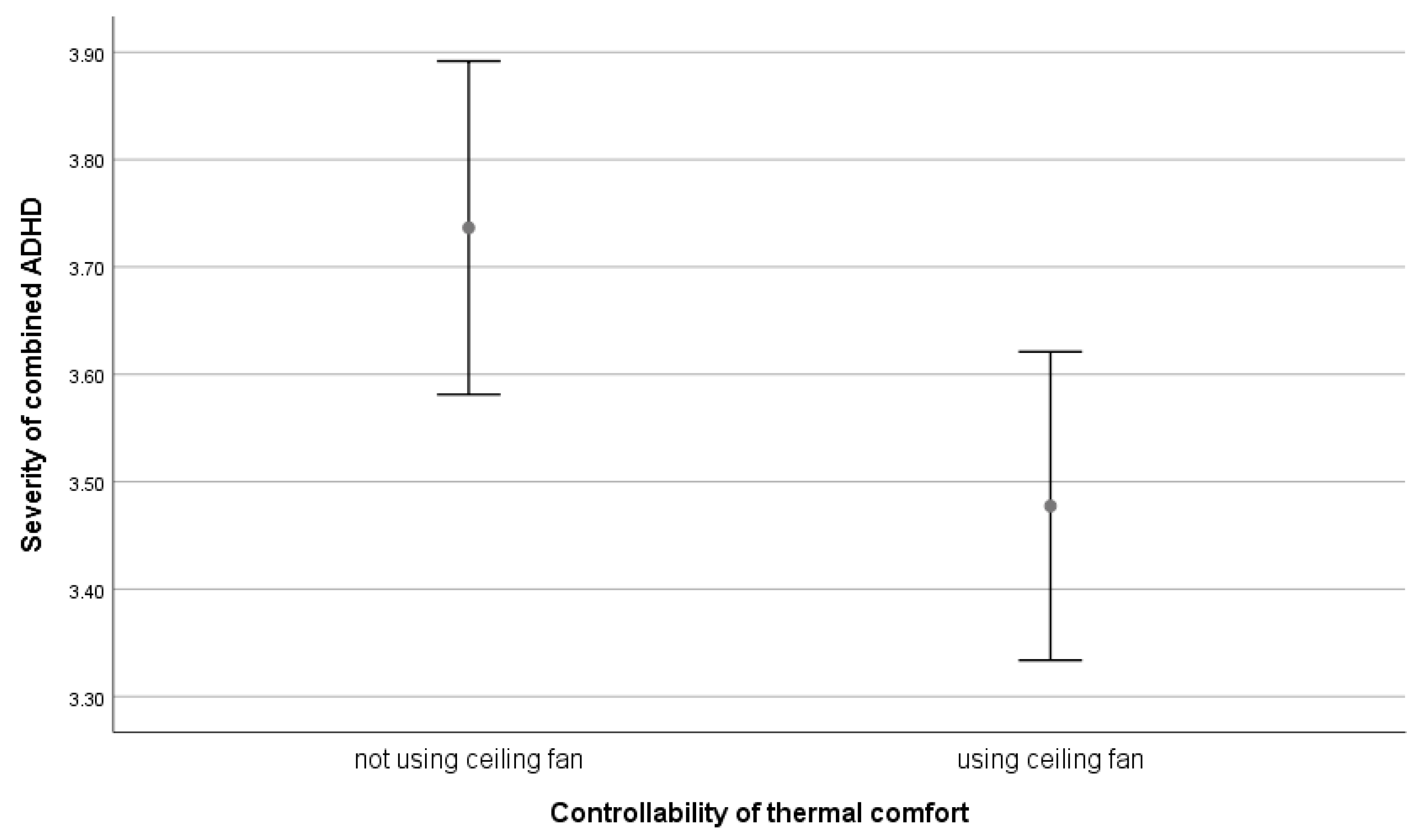
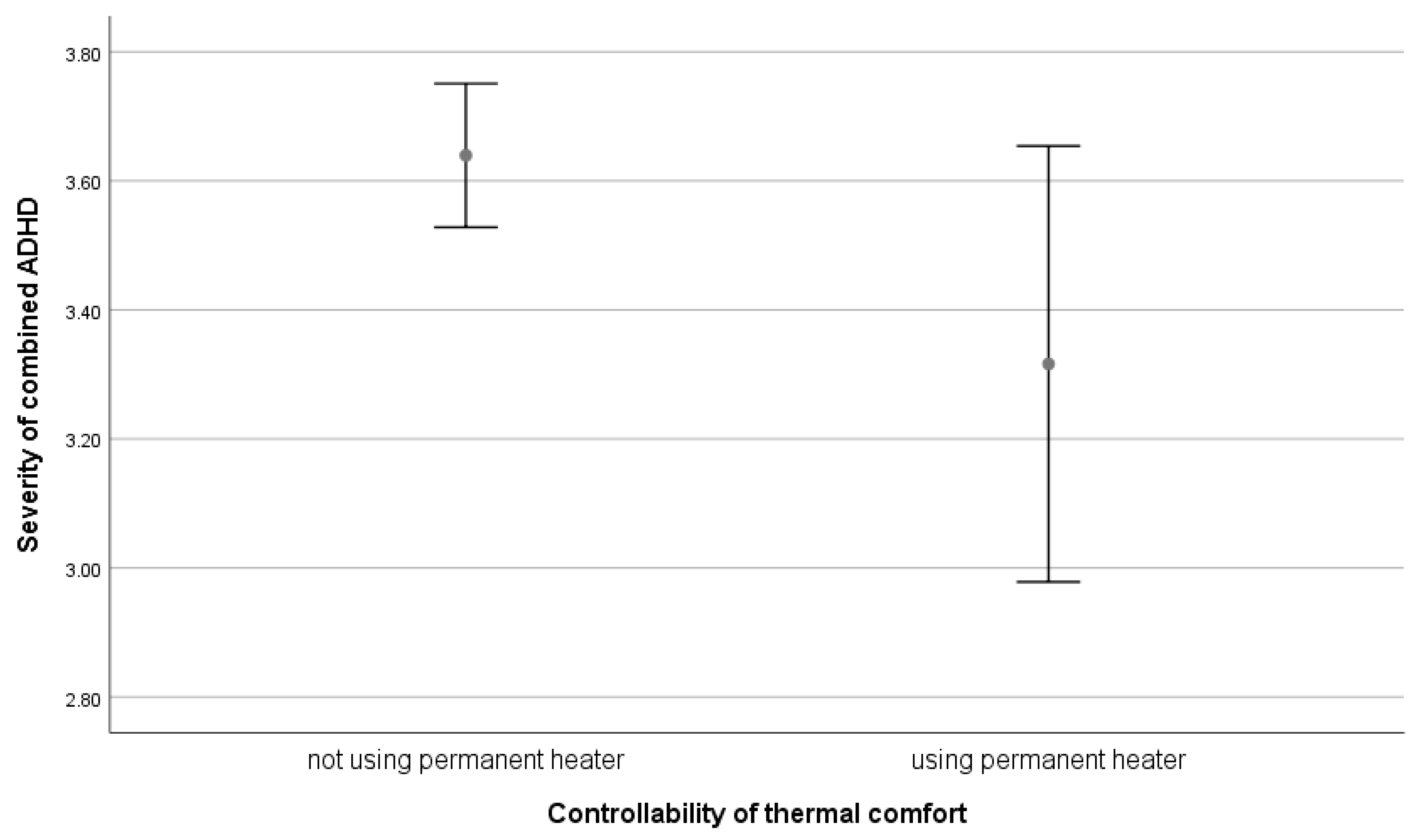
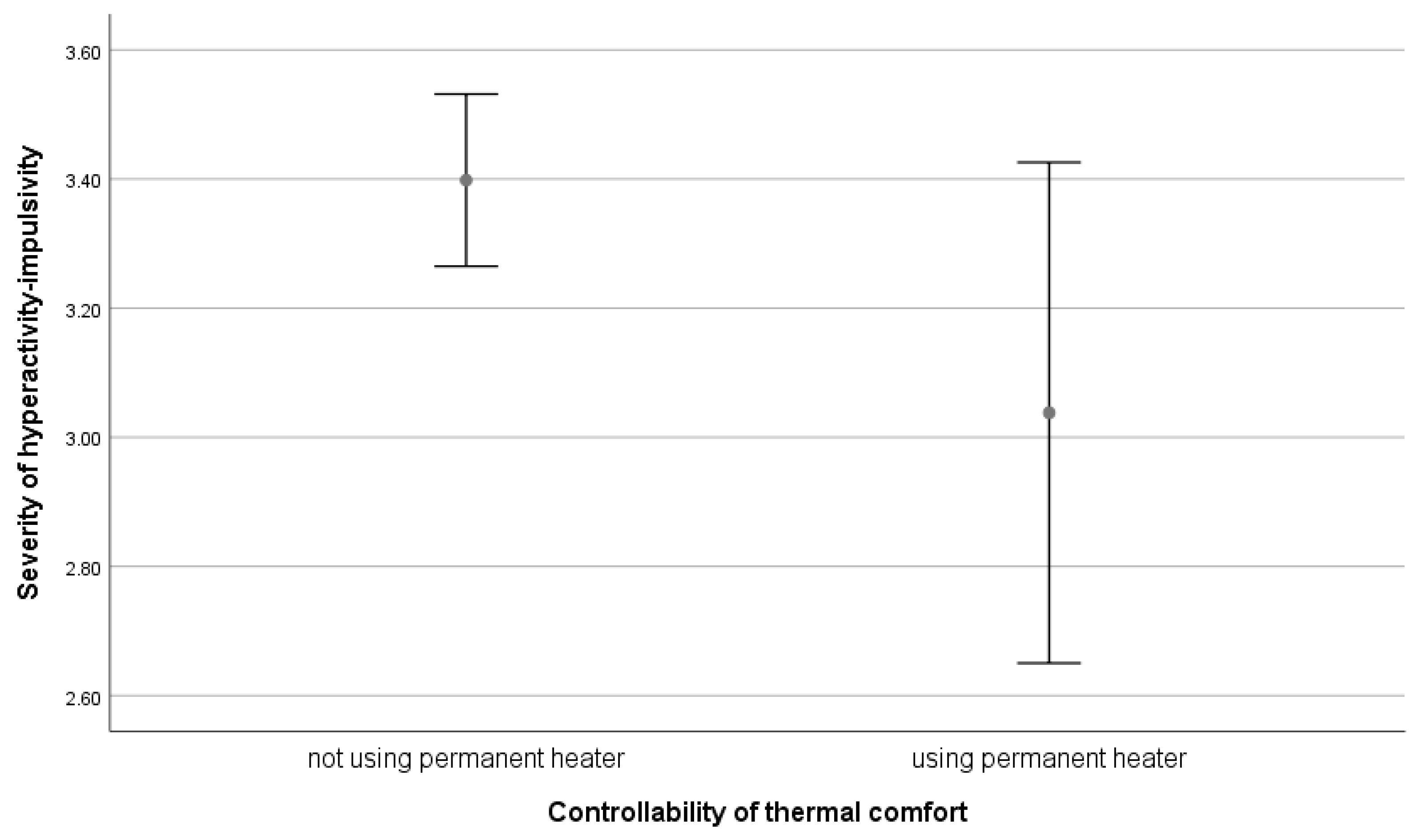
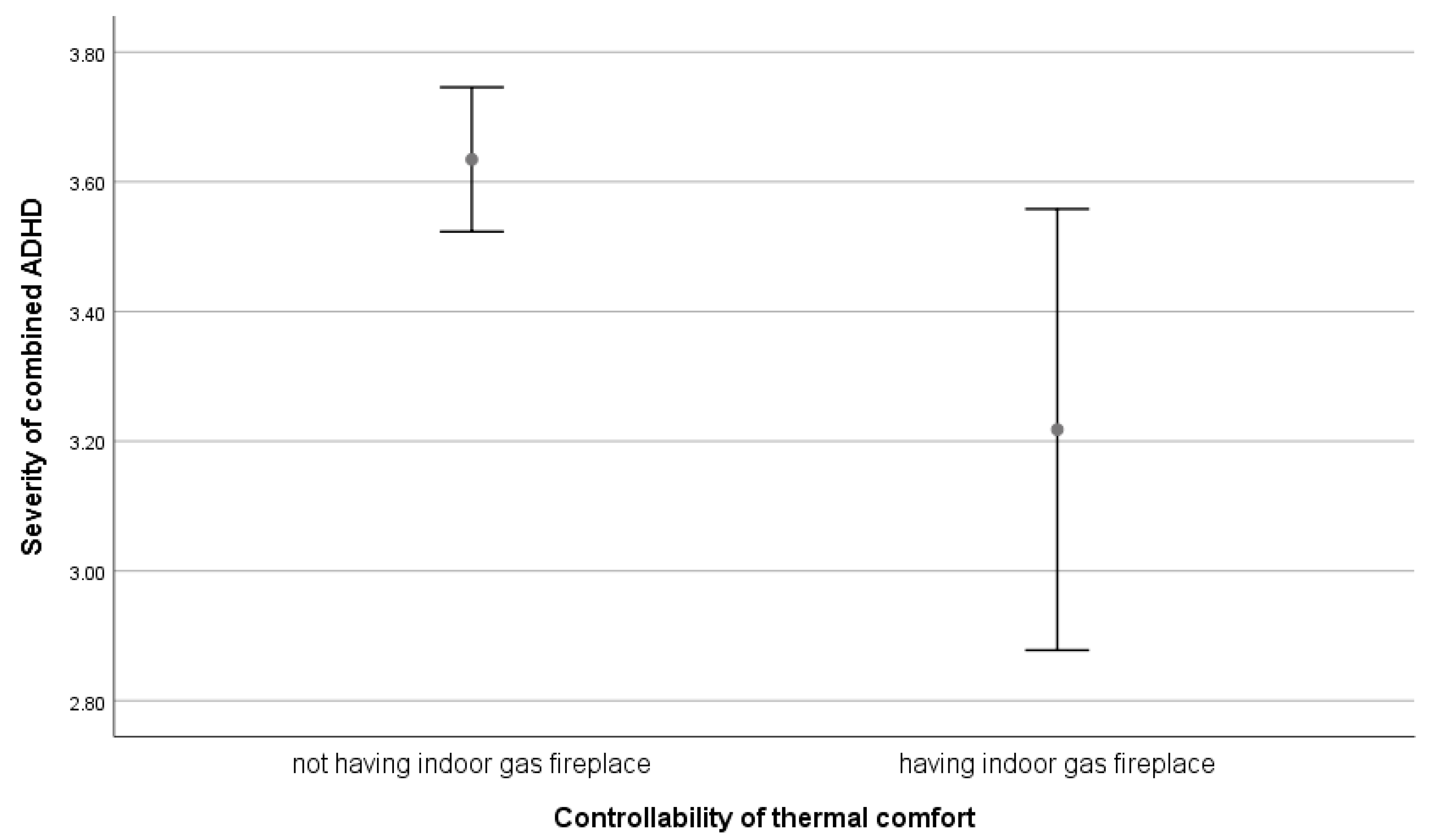
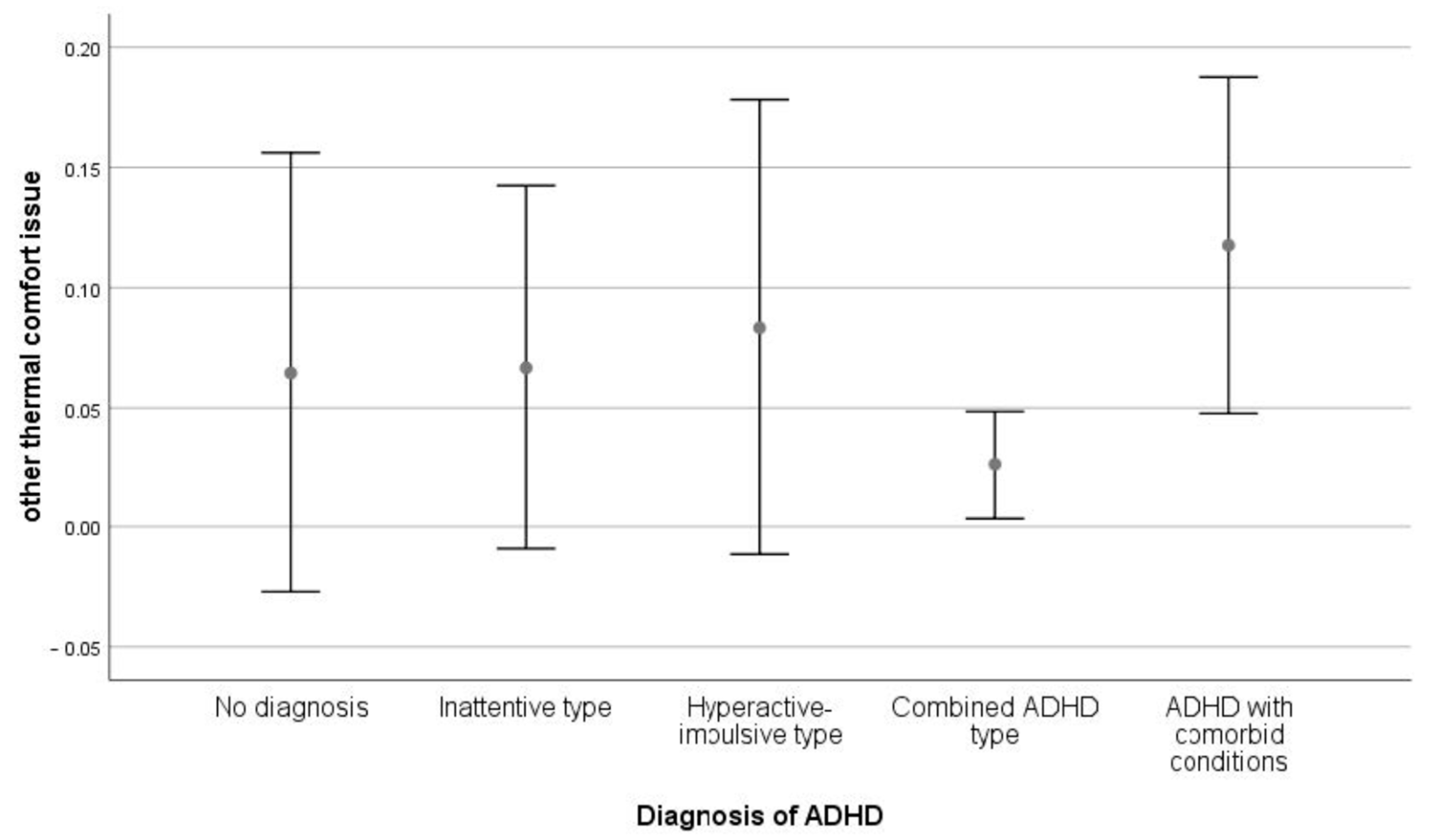
3.4. ADHD and Thermal Comfort
3.5. The Contribution of IEQ to the Prediction of ADHD
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A. ADHD and Air Quality






Appendix B. ADHD and Acoustic Quality



Appendix C. ADHD and Lighting Quality








Appendix D. ADHD and Thermal Comfort








References
- Bluyssen, P.M.; Cox, C. Indoor environment quality and upgrading of European office buildings. Energy Build. 2002, 34, 155–162. [Google Scholar] [CrossRef]
- Fisk, J.W. How IEQ affects health, productivity. ASHRAE J. 2002, 44, 56–60. [Google Scholar]
- Yoon, S.-H. An Integrative Approach: Environmental Quality (EQ) Evaluation in Residential Buildings, in Architecture. Ph.D. Thesis, The University of Michigan, Ann Arbor, MI, USA, 2008. [Google Scholar]
- Al Horr, Y.; Arif, M.; Kaushik, A.; Mazroei, A.; Katafygiotou, M.; Elsarrag, E. Occupant productivity and office indoor environment quality: A review of the literature. Build. Environ. 2016, 105, 369–389. [Google Scholar] [CrossRef]
- Woo, J.H. Towards Sustainable Workplaces: Effects of Indoor Environmental Quality on Occupant Comfort and Work Performance. Ph.D. Thesis, The University of New South Wales, Sydney, NSW, Australia, 2010. [Google Scholar]
- Ansari, M.; Ahmadi Yousefabad, S. Potential threats of COVID-19 on quarantined families. Public Health 2020, 183, 1. [Google Scholar] [CrossRef] [PubMed]
- Cheshmehzangi, A. Housing and health evaluation related to general comfort and indoor thermal comfort satisfaction during the COVID-19 lockdown. J. Hum. Behav. Soc. Environ. 2021, 31, 184–209. [Google Scholar] [CrossRef]
- Department of Climate Change Energy the Environment and Water. Indoor Air. Available online: https://www.dcceew.gov.au/environment/protection/air-quality/indoor-air#:~:text=It%20is%20generally%20recognised%20that,more%20of%20their%20time%20indoors (accessed on 31 October 2022).
- National Research Council. Indoor Air Pollutants; National Academy Press: Washington, DC, USA, 1981. [Google Scholar]
- Mendell, M.J.; Heath, G.A. Do indoor pollutants and thermal conditions in schools influence student performance? A critical review of the literature. Indoor Air 2005, 15, 27–52. [Google Scholar] [CrossRef] [PubMed]
- Wherry, J.H. The influence of home on school success. J. Princ. 2004, 84, 6–7. [Google Scholar]
- Wyon, D.P.; Wargocki, P. How Indoor Environment Affects Performance. ASHRAE J. 2013, 55, 46–52. [Google Scholar]
- Faustman, E.M.; Silbernagel, S.M.; Fenske, R.A.; Burbacher, T.M.; Ponce, R.A. Mechanisms underlying Children’s susceptibility to environmental toxicants. Env. Health Perspect 2000, 108 (Suppl. S1), 13–21. [Google Scholar] [CrossRef]
- McCurdy, L.E.; Winterbottom, K.E.; Mehta, S.S.; Roberts, J.R. Using Nature and Outdoor Activity to Improve Children’s Health. Curr. Probl. Pediatr. Adolesc. Health Care 2010, 40, 102–117. [Google Scholar] [CrossRef]
- Burns, N. Negotiating difference: Disabled people’s experiences of housebuilders. Hous. Stud. 2004, 19, 765–780. [Google Scholar] [CrossRef]
- Heylighen, A. Sustainable and inclusive design: A matter of knowledge? Local Environ. 2008, 13, 531–540. [Google Scholar] [CrossRef]
- Imrie, R. Architects’ Conceptions of the Human Body. Environ. Plan. D Soc. Space 2003, 21, 47–65. [Google Scholar] [CrossRef]
- Barber, S.; Grubbs, L.; Cottrell, B. Self-Perception in Children with Attention Deficit/Hyperactivity Disorder. J. Pediatr. Nurs. 2005, 20, 235–245. [Google Scholar] [CrossRef]
- Remschmidt, H. Global consensus on ADHD/HKD. Europ.Child Adolesc. Psych 2005, 14, 127–137. [Google Scholar] [CrossRef]
- APA. Diagnostic and Statistical Manual of Mental Disorders, 4th ed.; American Psychiatric Association: Washington, DC, USA, 1994. [Google Scholar]
- Bruce, B.; Thernlund, G.; Nettelbladt, U. ADHD and language impairment: A study of the parent questionnaire FTF (Five to Fifteen). Europ.Child Adolesc. Psych. 2006, 15, 52–60. [Google Scholar] [CrossRef] [PubMed]
- Barkley, R.A.; Murphy, K.R.; Fischer, M. ADHD in Adults: What the Science Says; The Guilford Press: New York, NY, USA, 2010. [Google Scholar]
- Barkley, R.A. Attention-Deficit Hyperactivity Disorder: A Handbook for Diagnosis and Treatment, 3rd ed.; The Guilford Press: New York, NY, USA, 2006; pp. 3–785. [Google Scholar]
- Biederman, J.; Newcomb, J.; Sprich, S. Comorbidity of attention deficit hyperactivity disorder with conduct, depressive, anxiety, and other disorders. Am. J. Psychiatry 1991, 148, 564–577. [Google Scholar]
- Bartholomew, K.; Owens, J. Sleep and ADHD: A review. Med. Health Rhode Isl. 2006, 89, 91–93. [Google Scholar]
- National Resource Center on ADHD. ADHD, Sleep, and Sleep Disorders. Available online: https://adhdaustralia.org.au/wp-content/uploads/2015/08/ADHD-Sleep-and-Sleep-Disorders-5D.pdf (accessed on 12 August 2019).
- Antshel, K.M.; Zhang-James, Y.; Faraone, S.V. The comorbidity of ADHD and autism spectrum disorder. Expert Rev. Neurother. 2013, 13, 1117–1128. [Google Scholar] [CrossRef] [PubMed]
- Geng, G. Investigation of teachers’ verbal and non-verbal strategies for managing Attention Deficit Hyperactivity Disorder (ADHD) students’ behaviours within a classroom environment. Aust. J. Teach. Educ. 2011, 36, 2. [Google Scholar] [CrossRef]
- CDC. Attention Deficit/Hyperactivity disorder (ADHD). Available online: www.cdc.gov/ncbddd/adhd/research.html (accessed on 27 October 2022).
- Polanczyk, G.; De Lima, M.S.; Horta, B.L.; Biederman, J.; Rohde, L.A. The worldwide prevalence of ADHD: A systematic review and metaregression analysis. Am. J. Psychiatry 2007, 164, 942–948. [Google Scholar] [CrossRef]
- Thomas, R.; Sanders, S.; Doust, J.; Beller, E.; Glasziou, P. Prevalence of Attention-Deficit/Hyperactivity Disorder: A Systematic Review and Meta-analysis. Am. Acad. Pediatr. 2015, 135, e994–e1001. [Google Scholar] [CrossRef] [PubMed]
- Zentall, S.S. Theory- and Evidence-Based Strategies for Children with Attentional Problems. Psychol. Schs. 2005, 42, 821–836. [Google Scholar] [CrossRef]
- Thapar, A.; van den Bree, M.; Fowler, T.; Langley, K.; Whittinger, N. Predictors of antisocial behaviour in children with attention deficit hyperactivity disorder. Europ.Child Adolesc. Psych. 2006, 15, 118–125. [Google Scholar] [CrossRef] [PubMed]
- Green, K. ADHD Light Sensitivity: The Link with Hypersensitivity & Sensory Processing. TheraSpecs. 2018, Volume 2019. Available online: https://www.theraspecs.com/blog/adhd-light-sensitivity-hypersensitivity-sensory-processing/ (accessed on 7 December 2022).
- Low, K. Understanding Hypersensitivity in ADHD. verywellmind, 11 December 2022. Available online: https://www.verywellmind.com/sensitivities-and-adhd-20473 (accessed on 7 December 2022).
- Bailie, R.; Stevens, M.; McDonald, E.; Brewster, D.; Guthridge, S. Exploring cross-sectional associations between common childhood illness, housing and social conditions in remote Australian Aboriginal communities. BMC Public Health 2010, 10, 147. [Google Scholar] [CrossRef]
- Shaw, M. Housing and Public Health. Annu. Rev. Public Health 2004, 25, 397–418. [Google Scholar] [CrossRef] [PubMed]
- Fisk, W.J.; Rosenfeld, A.H. Estimates of Improved Productivity and Health from Better Indoor Environments. Indoor Air 1997, 7, 158–172. [Google Scholar] [CrossRef]
- Wigle, D.T. Child Health and the Environment; Oxford University Press: Oxford, NY, USA, 2003. [Google Scholar]
- Wells, N.M.; Evans, G.W.; Yang, Y. Environments and health: Planning decisions as public-health decisions. J. Archit. Plan. Res. 2010, 27, 124–143. [Google Scholar]
- Matte, T.D.; Jacobs, D.E. Housing and health—Current issues and implications for research and programs. J. Urban Health 2000, 77, 7–25. [Google Scholar] [CrossRef]
- Krieger, J.; Higgins, D.L. Housing and Health: Time Again for Public Health Action. ScienceDaily 2002, 92, 758–768. [Google Scholar] [CrossRef]
- Bell, I.; Baldwin, C.; Schottenfeld, R. Psychological sequelae of hazardous materials exposure. In Clinical Environmental Health and Toxic Exposures, 2nd ed.; Sullivan, J., Krieger, G., Eds.; Lippincott Williams and Wilkins: Philadelphia, PA, USA, 2001; pp. 404–412. [Google Scholar]
- Araki, S. Neurobehavioral Methods and Effects in Occupational and Environmental Health; Academic Press: New York, NY, USA, 1994. [Google Scholar]
- Needleman, H.L.; Schell, A.; Bellinger, D.; Leviton, A.; Allred, E.N. The Long-Term Effects of Exposure to Low Doses of Lead in Childhood: An 11-Year Follow-up Report. N. Engl. J. Med. 1990, 322, 83–88. [Google Scholar] [CrossRef]
- Needleman, H.L.; Gunnoe, C.; Leviton, A.; Reed, R.; Peresie, H.; Maher, C.; Barrett, P. Deficits in Psychologic and Classroom Performance of Children with Elevated Dentine Lead Levels. N. Engl. J. Med. 1979, 300, 689–695. [Google Scholar] [CrossRef]
- Sciarillo, W.G.; Alexander, G.; Farrell, K.P. Lead exposure and child behavior. Am. J. Public Health 1992, 82, 1356–1360. [Google Scholar] [CrossRef] [PubMed]
- Yousef, S.; Eapen, V.; Zoubeidi, T.; Kosanovic, M.; Mabrouk, A.A.; Adem, A. Learning disorder and blood concentration of heavy metals in the United Arab Emirates. Asian J. Psychiatry 2013, 6, 394–400. [Google Scholar] [CrossRef] [PubMed]
- Yousef, S.; Adem, A.; Zoubeidi, T.; Kosanovic, M.; Mabrouk, A.A.; Eapen, V. Attention Deficit Hyperactivity Disorder and Environmental Toxic Metal Exposure in the United Arab Emirates. J. Trop. Pediatr. 2011, 57, 457–460. [Google Scholar] [CrossRef] [PubMed]
- Choi, W.-J.; Kwon, H.-J.; Lim, M.H.; Lim, J.-A.; Ha, M. Blood lead, parental marital status and the risk of attention-deficit/hyperactivity disorder in elementary school children: A longitudinal study. Psychiatry Res. 2016, 236, 42–46. [Google Scholar] [CrossRef]
- Dong, T.; Hu, W.; Zhou, X.; Lin, H.; Lan, L.; Hang, B.; Lv, W.; Geng, Q.; Xia, Y. Prenatal exposure to maternal smoking during pregnancy and attention-deficit/hyperactivity disorder in offspring: A meta-analysis. Reprod. Toxicol. 2018, 76, 63–70. [Google Scholar] [CrossRef]
- Schneider, M. Do School Facilities Affect Academic Outcomes? In Proceedings of the National Clearinghouse for Educational Facilities, Washington, DC, USA, 1 November 2002; p. 25. [Google Scholar]
- Myhrvold, A.; Olsen, E.; Lauridsen, O. Indoor environment in schools–pupils health and performance in regard to CO2 concentrations. Indoor Air 1996, 96, 369–371. [Google Scholar]
- Lercher, P.; Evans, G.; Meis, M.; Kofler, W. Ambient neighbourhood noise and children’s mental health. Occup. Environ. Med. 2002, 59, 380–386. [Google Scholar] [CrossRef]
- Bullinger, M.; Hygge, S.; Evans, G.W.; Meis, M.; Mackensen, S.V. The Psychological Cost of Aircraft Noise for Children*. Zentralblatt für Hygiene und Umweltmedizin 1999, 202, 127–138. [Google Scholar] [CrossRef] [PubMed]
- Knipschild, P.; Oudshoorn, N. VII. Medical effects of aircraft noise: Drug survey. Int. Arch. Occup. Environ. Health 1977, 40, 197–200. [Google Scholar] [CrossRef] [PubMed]
- Enmarker, I.; Boman, E. Noise annoyance responses of middle school pupils and teachers. J. Environ. Psychol. 2004, 24, 527–536. [Google Scholar] [CrossRef]
- Lercher, P.; Evans, G.W.; Meis, M. Ambient Noise and Cognitive Processes among Primary Schoolchildren. Environ. Behav. 2003, 35, 725–735. [Google Scholar] [CrossRef]
- Hygge, S.; Boman, E.; Enmarker, I. The effects of road traffic noise and meaningful irrelevant speech on different memory systems. Scand. J. Psychol. 2003, 44, 13–21. [Google Scholar] [CrossRef]
- Norlander, T.; Moås, L.; Archer, T. Noise and Stress in Primary and Secondary School Children: Noise Reduction and Increased Concentration Ability Through a Short but Regular Exercise and Relaxation Program. Sch. Eff. Sch. Improv. 2005, 16, 91–99. [Google Scholar] [CrossRef]
- Tufvesson, C. Concentration Difficulties in the School Environment—With Focus on Children with ADHD, Autism and Down’s Syndrome; Lund University: Lund, Sweden, 2007. [Google Scholar]
- Mostafa, M. Housing Adaptation for Adults with Autistic Spectrum Disorder. Open House Int. 2010, 35, 37–48. [Google Scholar] [CrossRef]
- Evans, G.W. The built environment and mental health. J. Urban Health 2003, 80, 536–555. [Google Scholar] [CrossRef]
- McAllister, K.; Maguire, B. Design considerations for the autism spectrum disorder-friendly Key Stage 1 classroom. Support Learn. 2012, 27, 103–112. [Google Scholar] [CrossRef]
- McAllister, K. The ASD Friendly Classroom–Design Complexity, Challenge and Characteristics. In Proceedings of the Design and Complexity—Design Research Society International Conference, Montreal, QU, Canada, 7–9 July 2010. [Google Scholar]
- Küller, R. Planning for Good Indoor Lighting; Lund University: Lund, Sweden, 2004; p. 20. [Google Scholar]
- Colman, R.S.; Frankel, F.; Ritvo, E.; Freeman, B.J. The effects of fluorescent and incandescent illumination upon repetitive behaviors in autistic children. J. Autism Child. Schizophr. 1976, 6, 157–162. [Google Scholar] [CrossRef] [PubMed]
- Küller, R. The Influence of Light on Circarhythms in Humans. J. Physiol. Anthropol. Appl. Hum. Sci. 2002, 21, 87–91. [Google Scholar] [CrossRef]
- Vogel, C.L. Classroom Design for Living and Learning with Autism. Autism Asperger’s Dig. 2008, 7, 30–39. [Google Scholar]
- Beaver, C. Autism-friendly environments. Autism File 2010, 34, 82–85. [Google Scholar]
- Vázquez, F.S.; Torres, A.S. Autism and Architecture. In Recent Advances in Autism Spectrum Disorders; Fitzgerald, M., Ed.; Trinity College: Dublin, Ireland, 2013; Volume 2, pp. 177–186. [Google Scholar]
- Hewitt, J.; Hewitson, C.; O’Toole, G.; Haywood, N. Sensory Access in Higher Education: Guidance Report; Equality Challenge Unit: London, UK, 2009. [Google Scholar]
- Ott, J.N. Influence of Fluorescent Lights on Hyperactivity and Learning Disabilities. J Learn. Disabil. 1976, 9, 417–422. [Google Scholar] [CrossRef]
- Rybak, Y.E.; McNeely, H.E.; Mackenzie, B.E.; Jain, U.R.; Levitan, R.D. An open trial of light therapy in adult attention-deficit/hyperactivity disorder. J. Clin. Psychiatry 2006, 67, 1527–1535. [Google Scholar] [CrossRef] [PubMed]
- Arns, M.; van der Heijden, K.B.; Arnold, L.E.; Kenemans, J.L. Geographic Variation in the Prevalence of Attention-Deficit/Hyperactivity Disorder: The Sunny Perspective. Biol. Psychiatry 2013, 74, 585–590. [Google Scholar] [CrossRef]
- Tufvesson, C.; Tufvesson, J. The building process as a tool towards an all-inclusive school. A Swedish example focusing on children with defined concentration difficulties such as ADHD, autism and Down’s syndrome. J. Hous. Built Environ. 2009, 24, 47–66. [Google Scholar] [CrossRef]
- Wilson, A. Productivity and green buildings. EBN 2004, 13, 10–15. [Google Scholar]
- Bonnefoy, X.R.; Annesi-Maesano, I.; Aznar, L.M.; Braubach, M.; Croxford, B.; Davidson, M.; Ezratty, V.; Fredouille, J.; GonzalezGross, M.; Kamp, I.V.; et al. Review of evidence on housing and health: Background document. In the Fourth Ministerial Conference on Environment and Health; World Health Organisation: Budapest, Hungary, 2004. [Google Scholar]
- Bluyssen, P.M.; Zhang, D.; Kurvers, S.; Overtoom, M.; Ortiz-Sanchez, M. Self-reported health and comfort of school children in 54 classrooms of 21 Dutch school buildings. Build. Environ. 2018, 138, 106–123. [Google Scholar] [CrossRef]
- King, J.; Marans, R.W. The Physical Environment and the Learning Process: A Survey of Recent Research; Institute for Social Research, University of Michigan Architectural Research Laboratory: Ann Arbor, MI, USA, 1979; p. 85. [Google Scholar]
- DuPaul, G.J.; Power, T.J.; Anastopoulos, A.D.; Reid, R. ADHD Rating Scale-IV (for Children and Adolescents): Checklists, Norms, and Clinical Interpretation; Guilford Publications: New York, NY, USA, 1998. [Google Scholar]
- Mostafa, M. An Architecture for Autism: Concepts of Design Intervention for the Autistic User. Archnet-IJAR: Int. J. Archit. Res. 2008, 2, 189–211. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Research Variables | Central Tendency | Dispersion | Distribution | |||||
|---|---|---|---|---|---|---|---|---|
| Mean | Median | Mode | Std. Deviation | Variance | Range | Skewness | Kurtosis | |
| ADHD Diagnosis | 2.63 | 3.00 | 3.00 | 1.17 | 1.37 | 4 | −0.925 | −0.054 |
| IA Severity | 3.29 | 3.31 | 3.66 | 0.951 | 0.905 | 4.52 | 0.148 | −0.038 |
| HI Severity | 3.34 | 3.47 | 3.66 | 1.24 | 1.55 | 5.83 | −0.475 | 0.089 |
| COM Severity | 3.59 | 3.47 | 5.29 | 1.04 | 1.09 | 4.74 | 0.077 | −0.677 |
| IEQ | 3.66 | 3.60 | 3.60 | 0.643 | 0.414 | 3.20 | −0.059 | −0.239 |
| Air Quality | ADHD Severity | N | df | F | Mean Difference | Std. Error | Sig. |
|---|---|---|---|---|---|---|---|
| Stuffy or stale air | Inattention | 387 | 1 | 4.91 | 0.275 | 0.124 | 0.027 |
| Vacuum cleaner | Inattention | 386 | 1 | 6.92 | 0.638 | 0.242 | 0.009 |
| Hyperactivity-impulsivity | 385 | 1 | 18.56 | 1.379 | 0.320 | 0.000 | |
| Combined ADHD | 386 | 1 | 20.97 | 1.202 | 0.262 | 0.000 | |
| Indoor plants | Hyperactivity-impulsivity | 385 | 1 | 3.74 | 0.251 | 0.130 | 0.054 |
| Acoustic Quality | ADHD Diagnosis and Severity of Symptoms | N | df | F | Pearson Correlation (2-Tailed) | Mean | Std. Deviation | Std. Error | Sig. |
|---|---|---|---|---|---|---|---|---|---|
| Suitability of acoustic quality | Control group (no ADHD) | 378 | 4 | 3.13 | - | 3.67 | 0.994 | 0.182 | 0.015 |
| ADHD with comorbid conditions | 3.18 | 0.951 | 0.069 | ||||||
| Severity of hyperactivity-impulsivity | 382 | - | - | −0.118 | - | - | - | 0.021 | |
| Severity of combined ADHD | 383 | - | - | −0.115 | - | - | - | 0.024 |
| Lighting Quality | ADHD Severity | N | df | F | Pearson Correlation (2-Tailed) | Mean Difference | Std. Error | Sig. |
|---|---|---|---|---|---|---|---|---|
| Suitability of artificial lighting quality | Hyperactivity-impulsivity | 368 | - | - | −0.118 | - | - | 0.024 |
| Reflection or glare | Hyperactivity-impulsivity | 378 | 1 | 4.88 | - | −0.420 | 0.190 | 0.028 |
| Too much daylight | Hyperactivity-impulsivity | 378 | 1 | 7.14 | - | −0.555 | 0.208 | 0.008 |
| Combined ADHD | 379 | 1 | 6.03 | - | −0.435 | 0.177 | 0.015 | |
| Insufficient artificial lighting | Combined ADHD | 379 | 1 | 3.52 | - | −0.315 | 0.168 | 0.062 |
| Windows’ placement facing south vs. east * | Hyperactivity-impulsivity | 377 | 5 | 2.41 | - | 0.588 | 0.203 | 0.004 |
| Combined ADHD | 377 | 5 | 2.35 | - | 0.478 | 0.172 | 0.006 | |
| Windows’ placement facing south vs. north * | Hyperactivity-impulsivity | 377 | 5 | 2.41 | - | 0.439 | 0.179 | 0.014 |
| Combined ADHD | 377 | 5 | 2.35 | - | 0.318 | 0.151 | 0.036 | |
| Windows’ placement facing east vs. west * | Hyperactivity-impulsivity | 377 | 5 | 2.41 | - | −0.408 | 0.203 | 0.045 |
| Combined ADHD | 377 | 5 | 2.35 | - | −0.441 | 0.171 | 0.010 |
| Thermal Comfort | ADHD Severity | N | df | F | Pearson Correlation (2-Tailed) | Mean Difference | Std. Error | Sig. |
|---|---|---|---|---|---|---|---|---|
| Suitability of thermal comfort | Combined ADHD | 390 | - | - | −0.105 | - | - | 0.038 |
| Ceiling fan | Inattention | 390 | 1 | 5.19 | - | 0.227 | 0.100 | 0.023 |
| Combined ADHD | 390 | 1 | 5.63 | - | 0.261 | 0.110 | 0.018 | |
| Permanent heater | Combined ADHD | 390 | 1 | 4.46 | - | 0.365 | 0.173 | 0.035 |
| Hyperactivity-impulsivity | 389 | 1 | 3.83 | - | 0.403 | 0.206 | 0.051 | |
| Indoor gas fireplace | Combined ADHD | 386 | 1 | 5.41 | - | 0.417 | 0.179 | 0.021 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Alizadeh, S.; Bridge, C.E.; Judd, B.H.; Eapen, V. Home Indoor Environmental Quality and Attention Deficit Hyperactivity Disorder. Sustainability 2023, 15, 2899. https://doi.org/10.3390/su15042899
Alizadeh S, Bridge CE, Judd BH, Eapen V. Home Indoor Environmental Quality and Attention Deficit Hyperactivity Disorder. Sustainability. 2023; 15(4):2899. https://doi.org/10.3390/su15042899
Chicago/Turabian StyleAlizadeh, Sima, Catherine E. Bridge, Bruce H. Judd, and Valsamma Eapen. 2023. "Home Indoor Environmental Quality and Attention Deficit Hyperactivity Disorder" Sustainability 15, no. 4: 2899. https://doi.org/10.3390/su15042899
APA StyleAlizadeh, S., Bridge, C. E., Judd, B. H., & Eapen, V. (2023). Home Indoor Environmental Quality and Attention Deficit Hyperactivity Disorder. Sustainability, 15(4), 2899. https://doi.org/10.3390/su15042899