Development, Relative Validity and Reproducibility of the Aus-SDS (Australian Short Dietary Screener) in Adults Aged 70 Years and above

 , , , ,
, , , , 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Study Population
2.3. Ethics Statement
2.4. Diet Screening Tool for Older People (Australian Short Dietary Screener, Aus-SDS)
2.5. Multiple Pass 24-h Recall Dietary Assessment
2.6. Data Analysis
3. Results
3.1. Sociodemographic, Medical and Anthropometrics Characteristics
3.2. Dietary Intake
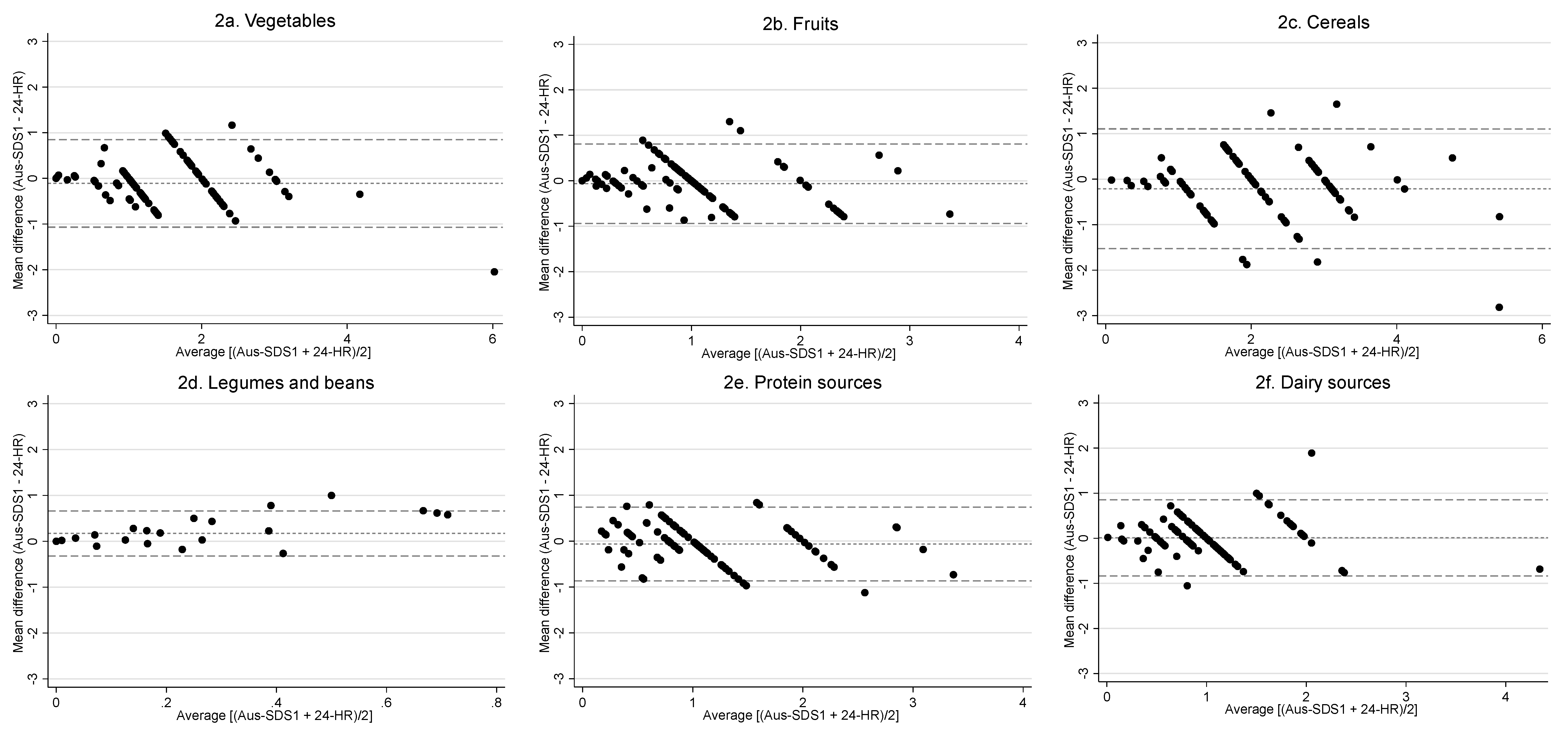
3.3. Relative Validity of the Aus-SDS
3.4. Reproducibility of the Aus-SDS
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Chang, A.Y.; Skirbekk, V.F.; Tyrovolas, S.; Kassebaum, N.J.; Dieleman, J.L. Measuring population ageing: An analysis of the Global Burden of Disease Study 2017. Lancet Public Health 2019, 4, e159–e167. [Google Scholar] [CrossRef] [Green Version]
- Australian Institute of Health and Welfare (AIHW). Australia’s Health. 2016. Available online: http://www.aihw.gov.au/australias-health/2016/ (accessed on 9 January 2020).
- World Health Organization. Diet, Nutrition, and the Prevention of Chronic Diseases: Report of a Joint WHO/FAO Expert Consultation; World Health Organization: Geneva, Switzerland, 2003; Volume 916. [Google Scholar]
- Afshin, A.; Sur, P.J.; Fay, K.A.; Cornaby, L.; Ferrara, G.; Salama, J.S.; Mullany, E.C.; Abate, K.H.; Abbafati, C.; Abebe, Z. Health effects of dietary risks in 195 countries, 1990–2017: A systematic analysis for the Global Burden of Disease Study 2017. Lancet 2019, 393, 1958–1972. [Google Scholar] [CrossRef] [Green Version]
- Drewnowski, A.; Shultz, J. Impact of aging on eating behaviors, food choices, nutrition, and health status. J. Nutr. Health Aging 2001, 5, 75–79. [Google Scholar] [PubMed]
- Senate Community Affairs References Committee. Effectiveness of the Aged Care Quality Assessment and Accreditation Framework for Protecting Residents from Abuse and Poor Practices, and Ensuring Proper Clinical and Medical Care Standards are Maintained and Practised: Interim Report. 2018. Available online: www.aph.gov.au/Parliamentary_Business/Committees/Senate/Community_Affairs/AgedCareQuality/Interim_report (accessed on 8 May 2020).
- Saunders, J.; Smith, T. Malnutrition: Causes and consequences. Clin. Med. (Northfield Il.) 2010, 10, 624. [Google Scholar] [CrossRef] [PubMed]
- Tapsell, L.C.; Neale, E.P.; Satija, A.; Hu, F.B. Foods, nutrients, and dietary patterns: Interconnections and implications for dietary guidelines. Adv. Nutr. 2016, 7, 445–454. [Google Scholar] [CrossRef]
- Govindaraju, T.; Sahle, B.W.; McCaffrey, T.A.; McNeil, J.J.; Owen, A.J. Dietary patterns and quality of life in older adults: A systematic review. Nutrients 2018, 10, 971. [Google Scholar] [CrossRef] [Green Version]
- Freeland-Graves, J.H.; Nitzke, S. Position of the academy of nutrition and dietetics: Total diet approach to healthy eating. J. Acad. Nutr. Diet. 2013, 113, 307–317. [Google Scholar] [CrossRef]
- National Health & Medical Research Council; Department of Health and Ageing. Eat for Health. In Australian Dietary Guidelines: Summary; Commonwealth of Australia: Canberra, Australia, 2013. Available online: https://www.eatforhealth.gov.au/sites/default/files/files/the_guidelines/n55_australian_dietary_guidelines.pdf (accessed on 9 January 2020).
- Iqbal, R.; Anand, S.; Ounpuu, S.; Islam, S.; Zhang, X.; Rangarajan, S.; Chifamba, J.; Al-Hinai, A.; Keltai, M.; Yusuf, S. Dietary patterns and the risk of acute myocardial infarction in 52 countries. Circulation 2008, 118, 1929–1937. [Google Scholar] [CrossRef] [Green Version]
- Russell, J.; Flood, V.; Rochtchina, E.; Gopinath, B.; Allman-Farinelli, M.; Bauman, A.; Mitchell, P. Adherence to dietary guidelines and 15-year risk of all-cause mortality. Br. J. Nutr. 2013, 109, 547–555. [Google Scholar] [CrossRef] [Green Version]
- Volkert, D.; Schrader, E. Dietary assessment methods for older persons: What is the best approach? Curr. Opin. Clin. Nutr. Metab. Care 2013, 16, 534–540. [Google Scholar] [CrossRef]
- Shim, J.-S.; Oh, K.; Kim, H.C. Dietary assessment methods in epidemiologic studies. Epidemiol. Health 2014, 36, e2014009. [Google Scholar] [CrossRef] [PubMed]
- Eysteinsdottir, T.; Thorsdottir, I.; Gunnarsdottir, I.; Steingrimsdottir, L. Assessing validity of a short food frequency questionnaire on present dietary intake of elderly Icelanders. Nutr. J. 2012, 11, 12. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Thompson, F.E.; Midthune, D.; Subar, A.F.; Kahle, L.L.; Schatzkin, A.; Kipnis, V. Performance of a short tool to assess dietary intakes of fruits and vegetables, percentage energy from fat and fibre. Public Health Nutr. 2004, 7, 1097–1106. [Google Scholar] [CrossRef] [PubMed]
- Cook, A.; Roberts, K.; O’Leary, F.; Allman-Farinelli, M.A. Comparison of single questions and brief questionnaire with longer validated food frequency questionnaire to assess adequate fruit and vegetable intake. Nutrition 2015, 31, 941–947. [Google Scholar] [CrossRef]
- Kris-Etherton, P.; Eissenstat, B.; Jaax, S.; Srinath, U.; Scott, L.; Rader, J.; Pearson, T. Validation for MEDFICTS, a dietary assessment instrument for evaluating adherence to total and saturated fat recommendations of the National Cholesterol Education Program Step 1 and Step 2 diets. J. Am. Diet. Assoc. 2001, 101, 81–86. [Google Scholar] [CrossRef]
- Blalock, S.J.; Norton, L.L.; Patel, R.A.; Cabral, K.; Thomas, C.L. Development and assessment of a short instrument for assessing dietary intakes of calcium and vitamin D. J. Am. Pharm. Assoc. 2003, 43, 685–693. [Google Scholar] [CrossRef]
- Robinson, S.; Jameson, K.; Bloom, I.; Ntani, G.; Crozier, S.; Syddall, H.; Dennison, E.; Cooper, C.; Sayer, A. Development of a short questionnaire to assess diet quality among older community-dwelling adults. J. Nutr. Health Aging 2017, 21, 247–253. [Google Scholar] [CrossRef]
- Bailey, R.L.; Miller, P.E.; Mitchell, D.C.; Hartman, T.J.; Lawrence, F.R.; Sempos, C.T.; Smiciklas-Wright, H. Dietary screening tool identifies nutritional risk in older adults. Am. J. Clin. Nutr. 2009, 90, 177–183. [Google Scholar] [CrossRef] [Green Version]
- Bland, J.M.; Altman, D. Statistical methods for assessing agreement between two methods of clinical measurement. Lancet 1986, 327, 307–310. [Google Scholar] [CrossRef]
- Jackson, K.A.; Byrne, N.M.; Magarey, A.M.; Hills, A.P. Minimizing random error in dietary intakes assessed by 24-h recall, in overweight and obese adults. Eur. J. Clin. Nutr. 2008, 62, 537–543. [Google Scholar] [CrossRef] [Green Version]
- Conway, J.M.; Ingwersen, L.A.; Moshfegh, A.J. Accuracy of dietary recall using the USDA five-step multiple-pass method in men: An observational validation study. J. Am. Diet. Assoc. 2004, 104, 595–603. [Google Scholar] [CrossRef] [PubMed]
- Bliss, R.M. Researchers produce innovation in dietary recall. Agric. Res. 2004, 52, 10–13. [Google Scholar]
- Australian Bureau of Statistics. Australian Health Survey Food model booklet. Canberra, Cat. No. 4363.0.55.001. 2010. Available online: https://www.ausstats.abs.gov.au/ausstats/subscriber.nsf/0/05E75E65AD98B1C0CA257CD20014B24B/$File/food%20model%20booklet.pdf (accessed on 9 January 2020).
- Food Standards Australia New Zealand. AUSNUT 2011–13—Australian Food Composition Database; FSANZ: Canberra, Australia, 2014. Available online: www.foodstandards.gov.au (accessed on 9 January 2020).
- Roe, M.; Bell, S.; Oseredczuk, M.; Christensen, T.; Westenbrink, S.; Pakkala, H.; Presser, K.; Finglas, P. Updated food composition database for nutrient intake. EFSA Supporting Publ. 2013, 10, 355E. [Google Scholar] [CrossRef] [Green Version]
- Australian Bureau of Statistics. Australian Health Survey: Users’ Guide, 2011–2013, Discretionary Foods, Cat. No. 4363.0.55.001. Available online: http://www.abs.gov.au/ausstats/[email protected]/Lookup/4363.0.55.001Chapter65062011-13 (accessed on 9 January 2020).
- Giles, G.G.; Ireland, P.D. Dietary Questionnaire for Epidemiological Studies (Version 3.2); Cancer Council Victoria: Melbourne, Australia, 1996. [Google Scholar]
- Giavarina, D. Understanding bland altman analysis. Biochem. Med. 2015, 25, 141–151. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lei, L.; Rangan, A.; Flood, V.M.; Louie, J.C.Y. Dietary intake and food sources of added sugar in the Australian population. Br. J. Nutr. 2016, 115, 868–877. [Google Scholar] [CrossRef] [Green Version]
- Pomerleau, J.; Lock, K.; Knai, C.; McKee, M. Effectiveness of Interventions and Programmes Promoting Fruit and Vegetable Intake; WHO: Geneva, Switzerland, 2005. [Google Scholar]
- Masson, L.F.; MCNeill, G.; Tomany, J.; Simpson, J.; Peace, H.S.; Wei, L.; Grubb, D.; Bolton-Smith, C. Statistical approaches for assessing the relative validity of a food-frequency questionnaire: Use of correlation coefficients and the kappa statistic. Public Health Nutr. 2003, 6, 313–321. [Google Scholar] [CrossRef]
- Shatenstein, B.; Payette, H. Evaluation of the relative validity of the short diet questionnaire for assessing usual consumption frequencies of selected nutrients and foods. Nutrients 2015, 7, 6362–6374. [Google Scholar] [CrossRef] [Green Version]
- Pisani, P.; Faggiano, F.; Krogh, V.; Palli, D.; Vineis, P.; Berrino, F. Relative validity and reproducibility of a food frequency dietary questionnaire for use in the Italian EPIC centres. Int. J. Epidemiol. 1997, 26, S152. [Google Scholar] [CrossRef] [Green Version]
- Whitton, C.; Ho, J.C.Y.; Rebello, S.A.; van Dam, R.M. Relative validity and reproducibility of dietary quality scores from a short diet screener in a multi-ethnic Asian population. Public Health Nutr. 2018, 21, 2735–2743. [Google Scholar] [CrossRef]
- Ibiebele, T.I.; Parekh, S.; Mallitt, K.-a.; Hughes, M.C.; O’Rourke, P.K.; Webb, P.M. Reproducibility of food and nutrient intake estimates using a semi-quantitative FFQ in Australian adults. Public Health Nutr. 2009, 12, 2359–2365. [Google Scholar] [CrossRef]
- Rolstad, S.; Adler, J.; Rydén, A. Response burden and questionnaire length: Is shorter better? A review and meta-analysis. Value Health 2011, 14, 1101–1108. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tonkin, E.; Kennedy, D.; Golley, R.; Byrne, R.; Rohit, A.; Kearns, T.; Hanieh, S.; Biggs, B.-A.; Brimblecombe, J. The relative validity of the menzies remote short-item dietary assessment tool (MRSDAT) in aboriginal Australian children aged 6–36 months. Nutrients 2018, 10, 590. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bartholome, L.T.; Peterson, R.E.; Raatz, S.K.; Raymond, N.C. A comparison of the accuracy of self-reported intake with measured intake of a laboratory overeating episode in overweight and obese women with and without binge eating disorder. Eur. J. Nutr. 2013, 52, 193–202. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Manjer, J.; Carlsson, S.; Elmståhl, S.; Gullberg, B.; Janzon, L.; Lindström, M.; Mattisson, I.; Berglund, G. The Malmö Diet and Cancer Study: Representativity, cancer incidence and mortality in participants and non-participants. Eur. J. Cancer Prev. 2001, 10, 489–499. [Google Scholar] [CrossRef] [Green Version]
- Dijkstra, W.; Smit, J.H.; Comijs, H.C. Using social desirability scales in research among the elderly. Qual. Quant. 2001, 35, 107–115. [Google Scholar] [CrossRef]
- Shahar, D.; Yerushalmi, N.; Lubin, F.; Froom, P.; Shahar, A.; Kristal-Boneh, E. Seasonal variations in dietary intake affect the consistency of dietary assessment. Eur. J. Epidemiol. 2001, 17, 129–133. [Google Scholar] [CrossRef]
- De la Fuente-Arrillaga, C.; Ruiz, Z.V.; Bes-Rastrollo, M.; Sampson, L.; Martinez-Gonzalez, M.A. Reproducibility of an FFQ validated in Spain. Public Health Nutr. 2010, 13, 1364–1372. [Google Scholar] [CrossRef]
- Vereecken, C.A.; Maes, L. A Belgian study on the reliability and relative validity of the Health Behaviour in School-Aged Children food-frequency questionnaire. Public Health Nutr. 2003, 6, 581–588. [Google Scholar] [CrossRef] [Green Version]



{kind=link}
{kind=link}
| Variables | Participant (n = 100) | ||
|---|---|---|---|
| Mean | SD | ||
| Age (years) | 76.8 | 4.5 | |
| Height, cm | 168.1 | 10.2 | |
| Weight, kg | 75.9 | 14.2 | |
| BMI (kg/m2) | 26.7 | 3.8 | |
| Number | |||
| Gender | |||
| Male | 52 | ||
| Female | 48 | ||
| Education | |||
| High school or less | 35 | ||
| More than high school | 65 | ||
| Smoking status | |||
| Current | 2 | ||
| Former | 49 | ||
| Never | 49 | ||
| Alcohol use | |||
| Current | 80 | ||
| Former | 7 | ||
| Never | 13 | ||
| Annual income | |||
| <$35,000 | 59 | ||
| ≥$35,000 | 33 | ||
| Prefer not to say | 8 | ||
| Household composition | |||
| Single person household | 26 | ||
| Multi-person household | 74 | ||
| Medical history | |||
| Heart disease | 27 | ||
| Diabetes | 14 | ||
| High cholesterol | 55 | ||
| Visited nutritionist or dietitian in previous year | 11 | ||
| Medication use | |||
| Cholesterol lowering | 63 | ||
| Blood pressure lowering | 58 | ||
| Glucose lowering | 8 | ||
| Food Group | Aus-SDS1 | Aus-SDS2 | 24-HRs | |||
|---|---|---|---|---|---|---|
| Mean (SD) | Median (IQR) | Mean (SD) | Median (IQR) | Mean (SD) | Median (IQR) | |
| Vegetables | 1.53 (0.90) | 1.00 (1.00, 2.00) | 1.52 (0.90) | 1.00 (1.00, 2.00) | 1.64 (1.01) | 1.42 (1.02, 2.30) |
| Fruit | 1.02 (0.64) | 1.00 (0.78, 1.00) | 1.12 (0.72) | 1.00 (0.78, 1.50) | 1.09 (0.77) | 0.94 (0.52, 1.58) |
| Cereal | 2.11 (1.05) | 2.00 (1.00, 3.00) | 2.16 (1.06) | 2.00 (0.01, 3.00) | 2.32 (1.13) | 2.28 (1.59, 3.16) |
| Legumes and beans | 0.20 (0.27) | 0.07 (0.02, 0.28) | 0.21 (0.32) | 0.07 (0.02, 0.28) | 0.03 (0.10) | 0.00 (0.00, 0.00) |
| Protein sources * | 1.08 (0.63) | 1.00 (0.78, 1.00) | 1.04 (0.59) | 1.00 (0.78, 1.00) | 1.14 (0.74) | 1.03 (0.61, 1.53) |
| Dairy sources † | 1.03 (0.62) | 1.00 (0.78, 1.00) | 1.12 (0.72) | 1.00 (0.78, 1.50) | 1.02 (0.64) | 0.92 (0.59, 1.33) |
| Food Group | Comparison of Aus-SDS1 vs. 24-HRs | ||||
|---|---|---|---|---|---|
| Spearman R (95% CI) | κ Coefficient (95% CI) | Mean Difference * (95% CI) in Intakes between Aus-SDS1 and 24-HRs | p Value ** | 95% LOA | |
| Vegetables | 0.82 (0.75, 0.88) | 0.58 (0.46, 0.70) | −0.11 (−0.20, −0.01) | 0.023 | −1.07, 0.85 |
| Fruit | 0.64 (0.50, 0.74) | 0.44 (0.28, 0.57) | −0.06 (−0.15, 0.02) | 0.142 | −0.94, 0.81 |
| Cereal | 0.84 (0.78, 0.89) | 0.51 (0.39, 0.64) | −0.21 (−0.34, −0.08) | 0.002 | −1.53, 1.11 |
| Legumes and beans | 0.82 (0.75, 0.88) | 0.12 (0.03, 0.22) | 0.17 (0.12, 0.22) | <0.001 | −0.32, 0.66 |
| Protein sources † | 0.83 (0.75, 0.88) | 0.64 (0.51, 0.75) | −0.06 (−0.14, 0.02) | 0.118 | −0.87, 0.74 |
| Dairy sources ‡ | 0.71 (0.60, 0.80) | 0.44 (0.31, 0.58) | 0.01 (−0.07, 0.09) | 0.817 | −0.83, 0.85 |
| Food Group | Comparison of Aus-SDS1 vs. Aus-SDS2 | ||||
|---|---|---|---|---|---|
| Spearman R (95% CI) | κ Coefficient (95% CI) | Mean Difference * (95% CI) in Intakes between Aus-SDS1 and Aus-SDS2 | p Value ** | 95% LOA | |
| Vegetable | 0.91 (0.88, 0.94) | 0.82 (0.71, 0.90) | −0.02 (−0.09, 0.06) | 0.694 | −0.78, 0.75 |
| Fruit | 0.95 (0.92, 0.96) | 0.89 (0.81, 0.97) | 0.10 (0.03, 0.16) | 0.004 | −0.55, 0.74 |
| Cereal | 0.84 (0.77, 0.89) | 0.69 (0.57, 0.79) | 0.05 (−0.07, 0.17) | 0.401 | −1.13, 1.23 |
| Legumes and beans | 0.86 (0.80, 0.90) | 0.68 (0.55, 0.80) | 0.01 (−0.02, 0.04) | 0.501 | −0.31, 0.32 |
| Protein sources † | 0.86 (0.80, 0.90) | 0.68 (0.54, 0.78) | −0.04 (−0.13, 0.06) | 0.443 | −0.94, 0.87 |
| Dairy sources ‡ | 0.91 (0.87, 0.94) | 0.85 (0.75, 0.93) | 0.09 (0.02, 0.17) | 0.018 | −0.68, 0.86 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gadowski, A.M.; McCaffrey, T.A.; Heritier, S.; Curtis, A.J.; Nanayakkara, N.; Zoungas, S.; Owen, A.J. Development, Relative Validity and Reproducibility of the Aus-SDS (Australian Short Dietary Screener) in Adults Aged 70 Years and above. Nutrients 2020, 12, 1436. https://doi.org/10.3390/nu12051436
Gadowski AM, McCaffrey TA, Heritier S, Curtis AJ, Nanayakkara N, Zoungas S, Owen AJ. Development, Relative Validity and Reproducibility of the Aus-SDS (Australian Short Dietary Screener) in Adults Aged 70 Years and above. Nutrients. 2020; 12(5):1436. https://doi.org/10.3390/nu12051436
Chicago/Turabian StyleGadowski, Adelle M., Tracy A. McCaffrey, Stephane Heritier, Andrea J. Curtis, Natalie Nanayakkara, Sophia Zoungas, and Alice J. Owen. 2020. "Development, Relative Validity and Reproducibility of the Aus-SDS (Australian Short Dietary Screener) in Adults Aged 70 Years and above" Nutrients 12, no. 5: 1436. https://doi.org/10.3390/nu12051436