
Time Series Analysis of the Impact of Meteorological Conditions and Air Quality on the Number of Medical Visits for Hypertension in Haikou City, China
Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Sources
2.2. Research Methods
2.2.1. Descriptive Analysis
2.2.2. Generalized Additive Model
2.2.3. Distributed Lag Nonlinear Model
2.2.4. Relative Risk
3. Results
3.1. Descriptive Statistical Analysis
3.2. The Impact of Meteorological Conditions and Air Quality on the Number of Medical Visits for Hypertension
4. Discussion
5. Conclusions
- (1)
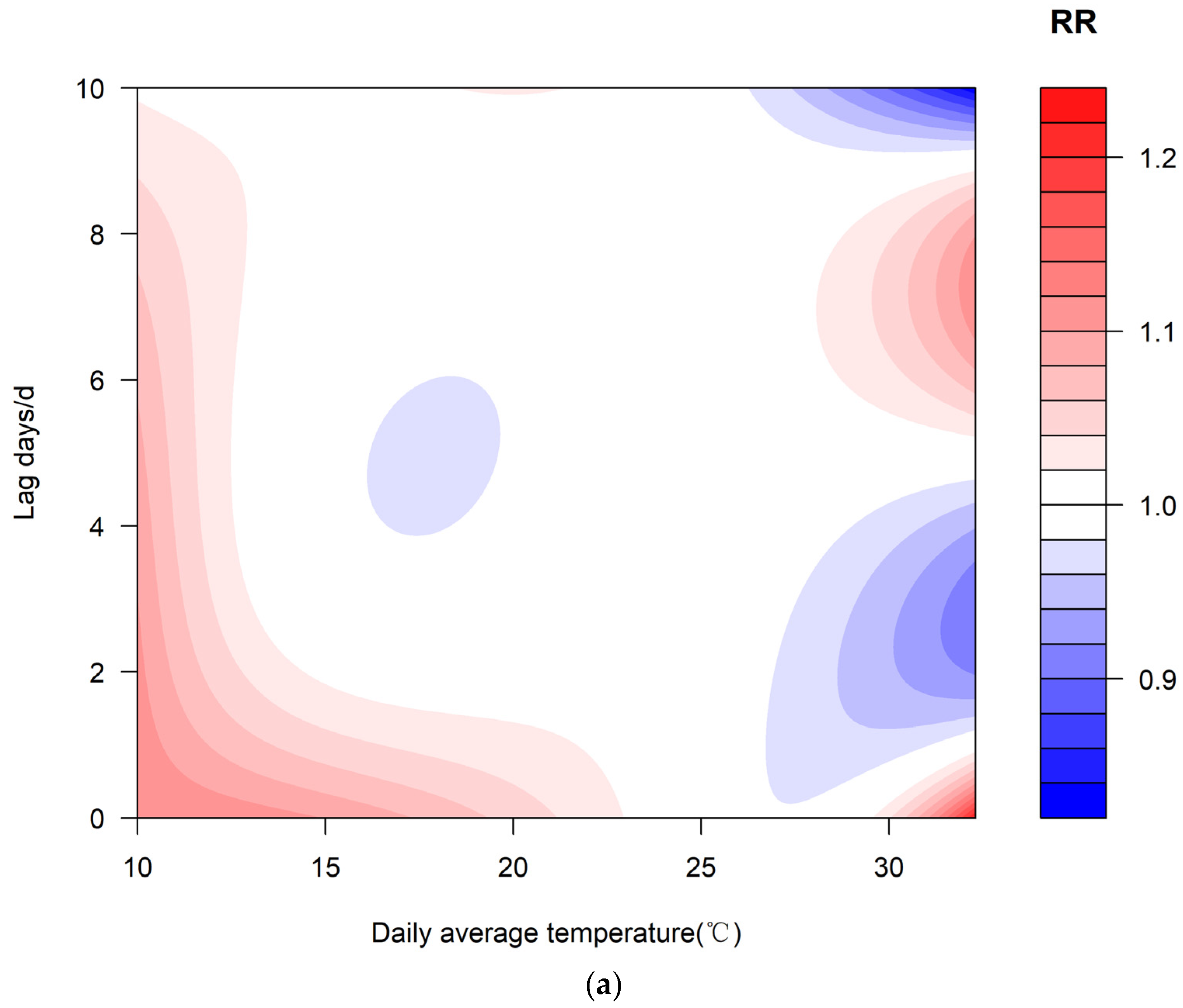
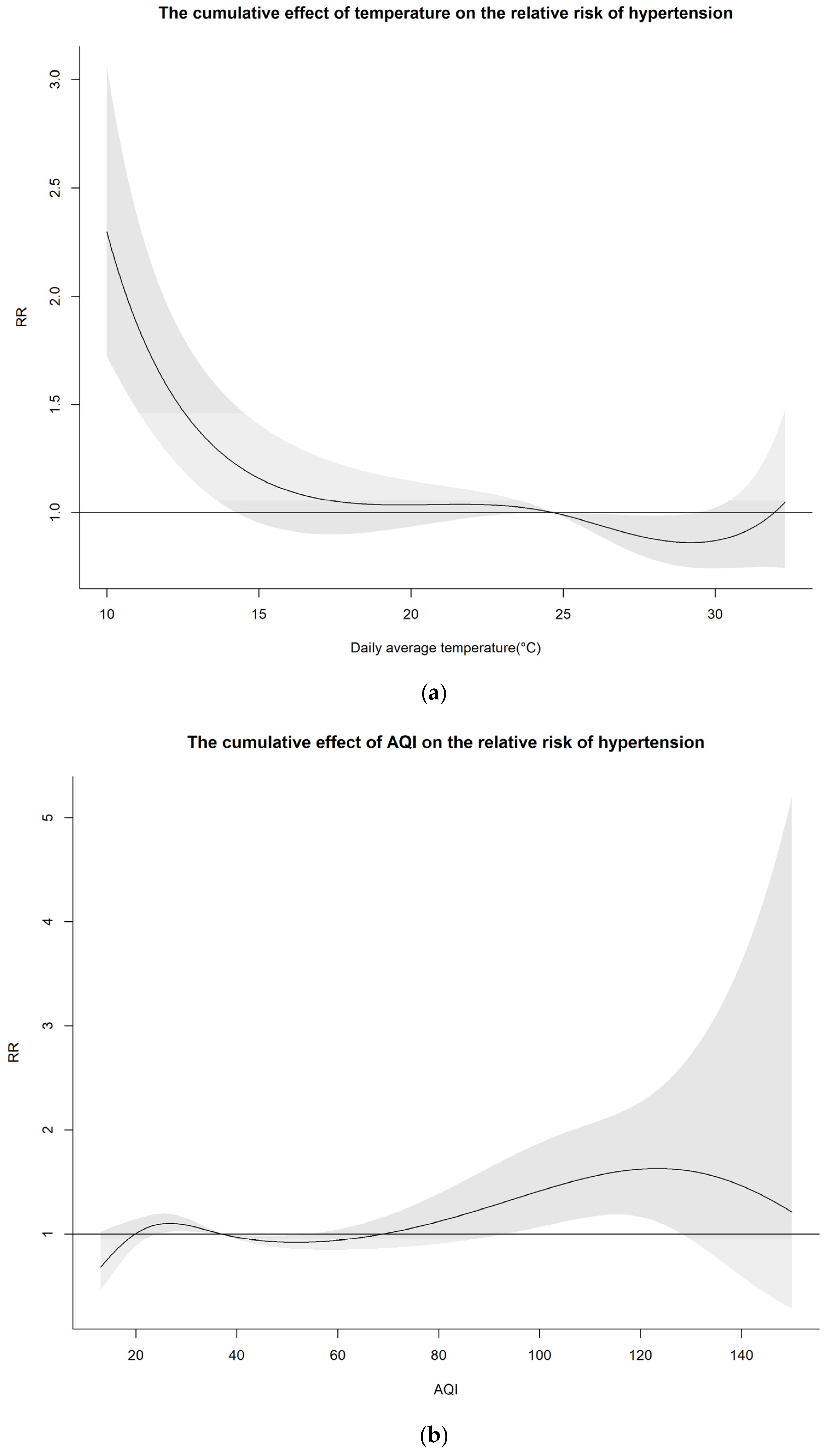
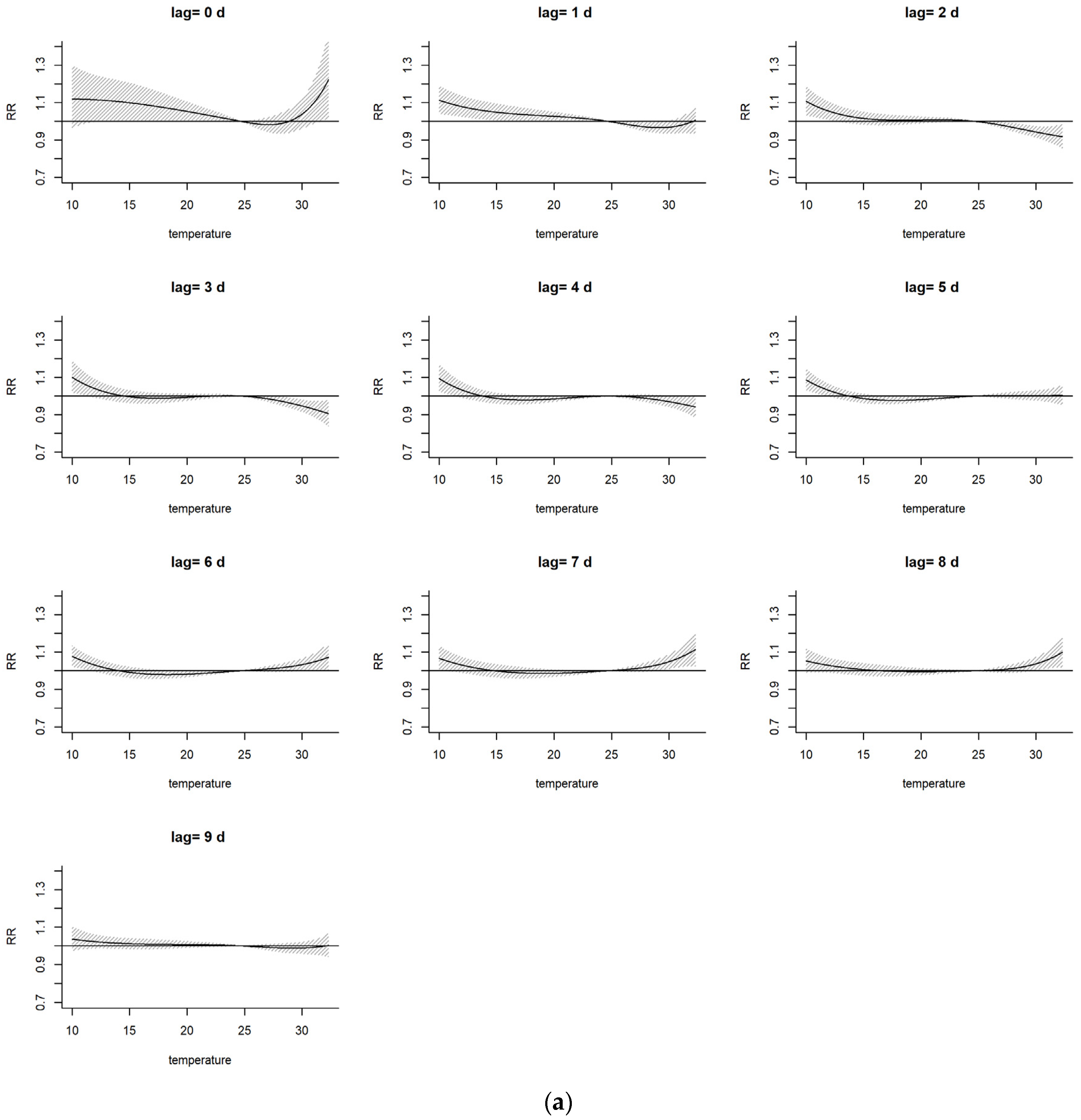
- The effect of temperature on the risk of hypertension was dominated by the cold effect, which was associated with a greater risk of hypertension, with a lag of 1 to 10 days from September 2016 to April 2018. When the temperature decreased to 10 °C, the cumulative effect on the RR of hypertension reached its highest value on the day when the low temperature occurred (RR = 2.30 and the 95% confidence interval = 1.723~3.061). Additionally, the RR increased by 1.30 times and passed the test for significance.
- (2)
- The impact of the air-quality effect on the risk of hypertension is mainly dominated by the low-quality-air effect (AQI less than 100), with a lag period of 0 to 8 days. When the AQI increased to approximately 124, the RR was the highest (RR was 1.63 and the 95% confidence interval was 1.104–2.408), and the RR increased by 63% and passed the test for significance.
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Hu, S.T.; Gao, R.L.; Liu, L.S.; Zhu, M.L.; Wang, W. Summary of the 2018 Report on Cardiovascular Diseases in China. Chin. Circ. J. 2019, 34, 209–220. [Google Scholar]
- Dai, Y.T.; Yu, F.Y.; Chang, P.; Zhang, L.; Yang, X. Weather conditions of hypertension incidence and its forecast model in Dezhou, Shandong province. J. Meteorol. Environ. 2012, 28, 79–82. [Google Scholar]
- Ma, S.C. Research on Effect of Cold Air from Northwest China on Hypertension Diseases and Its Mechanism. Master’s Thesis, Nanjing University of Information Science & Technology, Nanjing, China, 2012. [Google Scholar]
- Zhang, Y.; Xin, J.Y.; Ma, P.; Feng, X.Y.; Zhang, X.L.; Wang, S.G.; Zhang, J.X.; Wang, H.M.; Zheng, C.J. Interaction effects between ambient temperature and PM2.5 and O3 on mortality in Chengdu. China Environ. Sci. 2021, 41, 3887–3895. [Google Scholar] [CrossRef]
- Kotecki, P.; Więckowska, B.; Stawińska-Witoszyńska, B. The Impact of Meteorological Parameters and Seasonal Changes on Reporting Patients with Selected Cardiovascular Diseases to Hospital Emergency Departments: A Pilot Study. Int. J. Environ. Res. Public Health 2023, 20, 4838. [Google Scholar] [CrossRef] [PubMed]
- Ho, J.Y. Early-Life Environmental Exposures and Height, Hypertension, and Cardiovascular Risk Factors Among Older Adults in India. Biodemography Soc. Biol. 2015, 61, 121–146. [Google Scholar] [CrossRef]
- Di Pilla, M.; Bruno, R.M.; Stea, F.; Massetti, L.; Taddei, S.; Ghiadoni, L.; Modesti, P.A. Impact of seasonality and air pollutants on carotid-femoral pulse wave velocity and wave reflection in hypertensive patients. PLoS ONE 2017, 12, e0172550. [Google Scholar] [CrossRef]
- Yackerson, N.S.; Bromberg, L.; Adler, B.; Aizenberg, A. Possible effects of changes in the meteorological state over semi-arid areas on the general well-being of weather-sensitive patients. Environ. Health 2012, 11, 26. [Google Scholar] [CrossRef]
- Liu, Y.; Dong, J.; Zhai, G. Association between air pollution and hospital admissions for hypertension in Lanzhou, China. Environ. Sci. Pollut. Res. Int. 2022, 29, 11976–11989. [Google Scholar] [CrossRef]
- Wu, G.; Cai, M.; Wang, C.; Zou, H.; Wang, X.; Hua, J.; Lin, H. Ambient air pollution and incidence, progression to multimorbidity and death of hypertension, diabetes, and chronic kidney disease: A national prospective cohort. Sci. Total Environ. 2023, 881, 163406. [Google Scholar] [CrossRef]
- Hou, J.; Gu, J.; Liu, X.; Tu, R.; Dong, X.; Li, R.; Mao, Z.; Huo, W.; Chen, G.; Pan, M.; et al. Long-term exposure to air pollutants enhanced associations of obesity with blood pressure and hypertension. Clin. Nutr. 2021, 40, 1442–1450. [Google Scholar] [CrossRef]
- Fuks, K.B.; Weinmayr, G.; Basagaña, X.; Gruzieva, O.; Hampel, R.; Oftedal, B.; Sørensen, M.; Wolf, K.; Aamodt, G.; Aasvang, G.M.; et al. Long-term exposure to ambient air pollution and traffic noise and incident hypertension in seven cohorts of the European study of cohorts for air pollution effects (ESCAPE). Eur. Heart J. 2017, 38, 983–990. [Google Scholar] [CrossRef]
- Zhang, J.; Zhang, F.; Xin, C.; Duan, Z.; Wei, J.; Zhang, X.; Han, S.; Niu, Z. Associations of long-term exposure to air pollution, physical activity with blood pressure and prevalence of hypertension: The China Health and Retirement Longitudinal Study. Front. Public Health 2023, 11, 1137118. [Google Scholar] [CrossRef]
- Meng, X.Y.; Zheng, S.; Wei, X.F.; Nie, Y.H.; Wang, M.Z.; Mi, X.Y.; Li, H.Y.; Bai, Y.N. Effects of cold waves on hospital admissions for hypertension in Jinchang, Gansu Province: A case-crossover study. J. Environ. Occup. Med. 2020, 37, 36–43. [Google Scholar] [CrossRef]
- Wei, J.N.; Xue, S.L.; Lu, D.Y.; Qiao, X.F.; Shang, J. Association between daily admission of patients with hypertension and air pollutants. Chin. Prev. Med. 2018, 19, 101–105. [Google Scholar] [CrossRef]
- Wu, H. Risk Assessment of Ozone and Meteorological Factors on Cardiovascular and Cerebrovascular Mortality in the Population: A Time Series Study Based on 7-Year Cause of Death Registration Data in Nanchang City, Jiangxi Province. Master’s Thesis, Nanchang University, Nanchang, China, 2023. [Google Scholar] [CrossRef]
- Lin, S.; Luo, M.; Walker, R.J.; Liu, X.; Hwang, S.A.; Chinery, R. Extreme high temperatures and hospital admissions for respiratory and cardiovascular diseases. Epidemiology 2009, 20, 738–746. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.Y. The impact of environmental factors, meteorology and air pollution factors on the number of deaths from cardiovascular and cerebrovascular diseases during the high temperature in Wuhan from 2014 to 2019. Public Health Prev. Med. 2023, 6, 40–43. [Google Scholar] [CrossRef]
- Zhang, S.Y.; Wang, B.J.; Xie, J.F.; Qin, Y.M. Study and analysis of relationship between CVD and weather conditions and the establishment of medical forecast in Jilin province. Med. Mon. 2010, 36, 106–110. [Google Scholar]
- World Health Organization. Air Quality Guidelines: Global Update 2005:Particulate Matter, Ozone, Nitrogen Dioxide, and Sulfur Dioxide; World Health Organization: Geneva, Switzerland, 2006. [Google Scholar]
- Nuvolone, D.; Balzi, D.; Pepe, P.; Chini, M.; Scala, D.; Giovannini, F.; Cipriani, F.; Barchielli, A. Ozone short-term exposure and acute coronary events: A multicities study in Tuscany (Italy). Environ. Res. 2013, 126, 17–23. [Google Scholar] [CrossRef]
- Goodman, J.E.; Prueitt, R.L.; Sax, S.N.; Lynch, H.N.; Zu, K.; Lemay, J.C.; King, J.M.; Venditti, F.J. Weight-of-evidence evaluation of short-term ozone exposure and cardiovascular effects. Crit. Rev. Toxicol. 2014, 44, 725–790. [Google Scholar] [CrossRef]
- Guo, R.N.; Zheng, H.Z.; Ou, C.Q.; Huang, L.Q.; Zhou, Y.; Zhang, X.; Liang, C.K.; Lin, J.Y.; Zhong, H.J.; Song, T.; et al. Impact of Influenza on Outpatient Visits, Hospitalizations, and Deaths by Using a Time Series Poisson Generalized Additive Model. PLoS ONE 2016, 11, e0149468. [Google Scholar] [CrossRef]
- Luo, P.; Wang, D.; Luo, J.; Li, S.; Li, M.M.; Chen, H.; Duan, Y.; Fan, J.; Cheng, Z.; Zhao, M.M.; et al. Relationship between air pollution and childhood atopic dermatitis in Chongqing, China: A time-series analysis. Front. Public Health 2022, 10, 990464. [Google Scholar] [CrossRef]
- Li, Y.; Wang, B.; Wang, S.; Xu, S.; Li, S.; He, H.; Niu, J.; Luo, B. Ambient temperature, humidity, and urinary system diseases: A population-based study in Western China. Environ. Sci. Pollut. Res. Int. 2022, 29, 28637–28646. [Google Scholar] [CrossRef]
- Luo, L.; He, K.; Wu, W.; Taylor, J.M. Using information criteria to select smoothing parameters when analyzing survival data with time-varying coefficient hazard models. Stat. Methods Med. Res. 2023, 32, 1664–1679. [Google Scholar] [CrossRef]
- Gasparrini, A.; Armstrong, B.; Kenward, M.G. Distributed lag non-linear models. Stat. Med. 2010, 29, 2224–2234. [Google Scholar] [CrossRef] [PubMed]
- Kriit, H.K.; Andersson, E.M.; Carlsen, H.K.; Andersson, N.; Ljungman, P.L.S.; Pershagen, G.; Segersson, D.; Eneroth, K.; Gidhagen, L.; Spanne, M.; et al. Using Distributed Lag Non-Linear Models to Estimate Exposure Lag-Response Associations between Long-Term Air Pollution Exposure and Incidence of Cardiovascular Disease. Int. J. Environ. Res. Public Health 2022, 19, 2630. [Google Scholar] [CrossRef]
- Wu, Y.; Liang, M.; Liang, Q.; Yang, X.; Sun, Y. A distributed lag non-linear time-series study of ambient temperature and healthcare-associated infections in Hefei, China. Int. J. Environ. Health Res. 2023, 33, 258–267. [Google Scholar] [CrossRef]
- Schwartz, J. The distributed lag between air pollution and daily deaths. Epidemiology 2000, 11, 320–326. [Google Scholar] [CrossRef] [PubMed]
- Zhao, J.; Zhang, Y.; Ni, Y.; He, J.; Wang, J.; Li, X.; Guo, Y.; Li, C.; Zhang, W.; Cui, Z. Effect of ambient temperature and other environmental factors on stroke emergency department visits in Beijing: A distributed lag non-linear model. Front. Public Health 2022, 10, 1034534. [Google Scholar] [CrossRef] [PubMed]
- Noordzij, M.; van Diepen, M.; Caskey, F.C.; Jager, K.J. Relative risk versus absolute risk: One cannot be interpreted without the other. Nephrol. Dial. Transplant. 2017, 32 (Suppl. S2), ii13–ii18. [Google Scholar] [CrossRef]
- Huang, S.L. Study on the Correlation between Gaseous Pollutants and Death of Cardiovascular and Cerebrovascular Diseases in Shenyang from 2014 to 2018. Master Thesis, China Medical University, Shenyang, China, 2023. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Meteorological Elements | Average Air Pressure | Maximum Air Pressure | Lowest Air Pressure | Average Temperature | Maximum Temperature | Minimum Temperature | Vapor Pressure | Relative Humidity | Precipitation | Average Wind Speed | Temperature Change Range |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Number of visits | 0.15 * | 0.15 * | 0.14 * | −0.18 ** | −0.16 ** | −0.19 ** | −0.19 * | −0.05 | −0.07 | 0.04 | −0.01 |
| Air quality indicators | AQI | PM2.5 | PM10 | SO2 | NO2 | CO | O3 | ||||
| Number of doctors | 0.10 ** | 0.11 ** | 0.13 ** | 0.02 | 0.09 * | 0.08 * | 0.04 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zhang, M.; Zhang, Y.; Zhang, J.; Lin, S. Time Series Analysis of the Impact of Meteorological Conditions and Air Quality on the Number of Medical Visits for Hypertension in Haikou City, China. Atmosphere 2024, 15, 370. https://doi.org/10.3390/atmos15030370
Zhang M, Zhang Y, Zhang J, Lin S. Time Series Analysis of the Impact of Meteorological Conditions and Air Quality on the Number of Medical Visits for Hypertension in Haikou City, China. Atmosphere. 2024; 15(3):370. https://doi.org/10.3390/atmos15030370
Chicago/Turabian StyleZhang, Mingjie, Yajie Zhang, Jinghong Zhang, and Shaowu Lin. 2024. "Time Series Analysis of the Impact of Meteorological Conditions and Air Quality on the Number of Medical Visits for Hypertension in Haikou City, China" Atmosphere 15, no. 3: 370. https://doi.org/10.3390/atmos15030370