Infectious Disease Management through Point-of-Care Personalized Medicine Molecular Diagnostic Technologies

{kind=link}
Abstract
:1. Introduction
2. Personalized Medicine for Infectious Diseases?
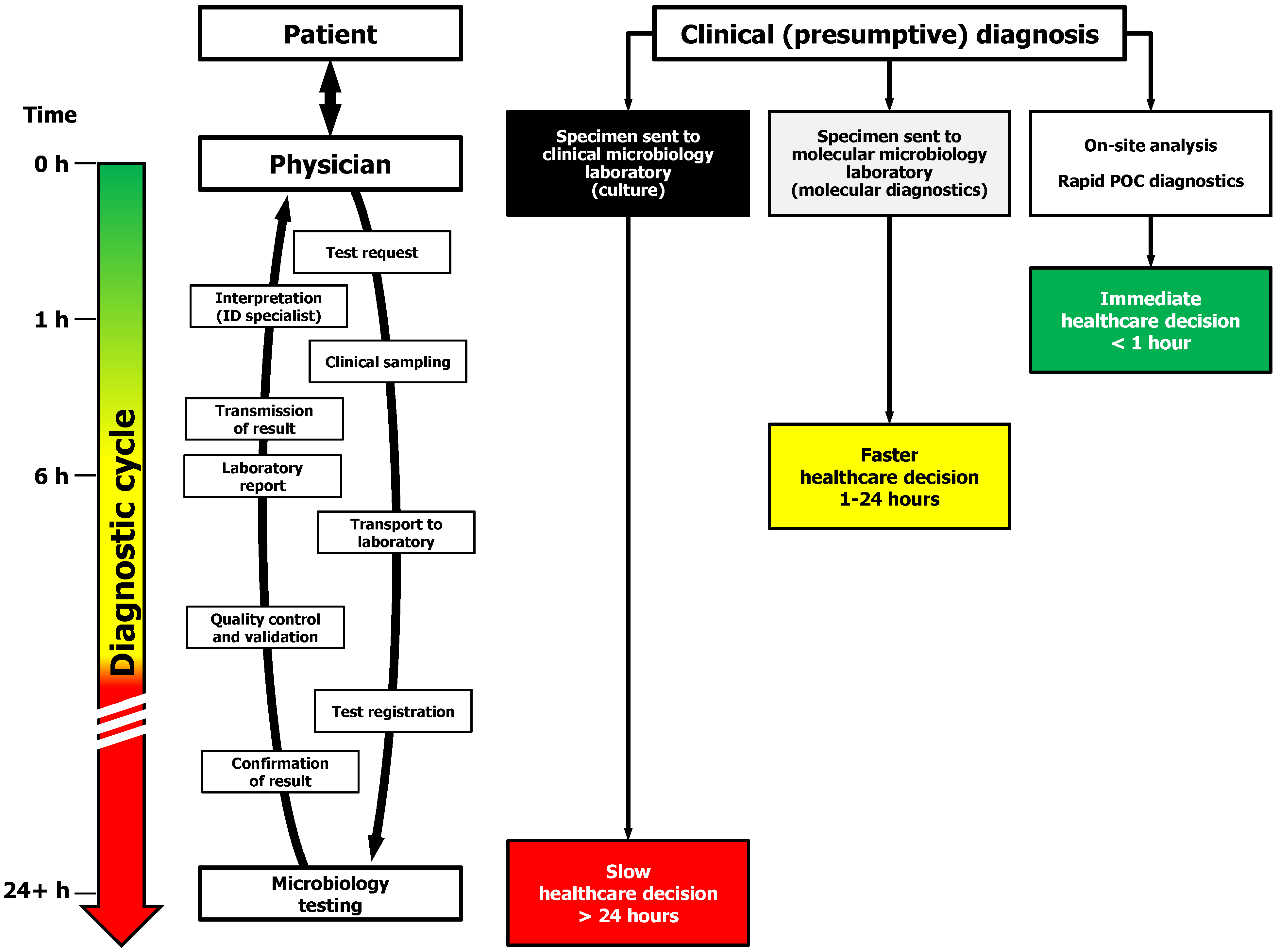
3. Infectious Disease Management in the Molecular Medicine Era—Shortening the Diagnostic Cycle

4. Molecular Tools for POC or near POC Diagnostics of Infectious Diseases
- (1)
- sample preparation shall enable the concentration of microbes and/or the recovery of intracellular pathogens. Indeed, achieving this should prevent the detection of (soluble) DNA liberated by dead or damaged pathogens exposed to antibiotics and improve the probability of detection of a microbial target against a lesser background of human DNA. The significance of microbial DNAemia is seldom raised against the utilization of PCR in clinical microbiology but, for the management of life-threatening infections, we concur with Bauer and Reinhart [78] in the sense that "... presence of a pathogen-associated DNA amplicon is a meaningful event in severe sepsis and warrants further investigation as to its suitability to guide anti-infective therapy". Alternatively, DNA from dead cells could be inactivated by compounds such as EMA or PMA (ethidium or propidium monoazide) [79]. However, EMA can penetrate the membrane of viable cells, EMA uptake is species-dependent, and there are drawbacks with PMA utilization [80];
- (2)
- the recovery of pathogens and nucleic acid extraction from a relatively large sample volume, for example 1 to 30 mL in the case of neonatal or human bloodstream infections is a major challenge that might require some external sample pretreatment, in order to deliver a concentrated subsample containing the target analyte(s) more easily subjected to the amplification and detection processes;
- (3)
- nucleic acid extraction or purification must enable the removal of PCR inhibitors known to hinder the performance of enzymatic components, and;
- (4)
- strict precautions to control the cross-contamination of personnel and equipment by amplification products that would negatively affect the performance and clinical validity of the test.
5. Applications and Anticipated Impact of POC or near POC Diagnostics of Infectious Diseases
5.1. Hospital-Acquired Infections
5.2. Bloodstream Infections and Sepsis
5.3. Influenza and Severe Respiratory Tract Infections
5.4. Other Clinical Indications and Strategic Suggestions for POC or near POC Testing Implementation
6. Regulatory, Ethical, and Financial Challenges to POC or near POC Testing for Infectious Diseases
7. Conclusions
Conflict of Interest
References
- Arnold, A.; Brouse, S.D.; Pitcher, W.D.; Hall, R.G., II. Empiric Therapy for Gram-Negative Pathogens in Nosocomial and Health Care-Associated Pneumonia: Starting with the End in Mind. J. Intensive Care Med. 2010, 25, 259–270. [Google Scholar]
- Jabes, D. The Antibiotic R&D Pipeline: An Update. Curr. Opin. Microbiol. 2011, 14, 564–569. [Google Scholar]
- Micek, S.T.; Welch, E.C.; Khan, J.; Pervez, M.; Doherty, J.A.; Reichley, R.M.; Hoppe-Bauer, J.; Dunne, W.M.; Kollef, M.H. Resistance to Empiric Antimicrobial Treatment Predicts Outcome in Severe Sepsis Associated with Gram-Negative Bacteremia. J. Hosp. Med. 2011, 6, 405–410. [Google Scholar]
- Nicolau, D.P. Current Challenges in the Management of the Infected Patient. Curr. Opin. Infect. Dis. 2011, 24 (suppl. 1), S1–S10. [Google Scholar]
- Pogue, J.M.; Marchaim, D.; Kaye, D.; Kaye, K.S. Revisiting "Older" Antimicrobials in the Era of Multidrug Resistance. Pharmacotherapy 2011, 31, 912–921. [Google Scholar]
- Griffith, M.M.; Gross, A.E.; Sutton, S.H.; Bolon, M.K.; Esterly, J.S.; Patel, J.A.; Postelnick, M.J.; Zembower, T.R.; Scheetz, M.H. The Impact of Anti-Infective Drug Shortages on Hospitals in the United States: Trends and Causes. Clin. Infect. Dis. 2012, 54, 684–691. [Google Scholar] [CrossRef]
- Morens, D.M.; Folkers, G.K.; Fauci, A.S. Emerging Infections: a Perpetual Challenge. Lancet Infect. Dis. 2008, 8, 710–719. [Google Scholar]
- Abrahams, E.; Ginsburg, G.S.; Silver, M. The Personalized Medicine Coalition. Am. J. Pharmacogenomics 2005, 5, 345–355. [Google Scholar]
- Ginsburg, G.S.; Willard, H.F. Genomic and Personalized Medicine: Foundations and Applications. Transl. Res. 2009, 154, 277–287. [Google Scholar]
- Walk, E.E. Improving the Power of Diagnostics in the Era of Targeted Therapy and Personalized Healthcare. Curr. Opin. Drug Discov. Dev. 2010, 13, 226–234. [Google Scholar]
- The Case for Personalized Medicine; Personalized Medicine Coalition: Washington, DC, USA, 2011, 3rd edition Available online: http://www.personalizedmedicinecoalition.org (accessed in November 2011).
- Chan, I.S.; Ginsburg, G.S. Personalized Medicine: Progress and Promise. Annu. Rev. Genomics Hum. Genet. 2011, 12, 217–244. [Google Scholar]
- Klouche, M.; Schröder, U. Methods for Diagnosis of Bloodstream Infections. Clin. Chem, Lab. Med. 2008, 46, 888–908. [Google Scholar] [CrossRef]
- Lehmann, L.E.; Herpichboehm, B.; Kost, G.J.; Kollef, M.H.; Stüber, F. Cost and Mortality Prediction using Polymerase Chain Reaction Pathogen Detection in Sepsis: Evidence from Three Observational Trials. Crit. Care 2010, 14, R186. [Google Scholar] [CrossRef] [Green Version]
- Olano, J.P.; Walker, D.H. Diagnosing Emerging and Reemerging Infectious Diseases. Arch. Pathol. Lab. Med. 2011, 135, 83–91. [Google Scholar]
- Bissonnette, L.; Bergeron, M.G. Next Revolution in the Molecular Theranostics of Infectious Diseases: Microfabricated Systems for Personalized Medicine. Expert Rev. Mol. Diagn. 2006, 6, 433–450. [Google Scholar]
- Millar, B.C.; Xu, J.; Moore, J.E. Molecular Diagnostics of Medically Important Infections. Curr. Issues Mol. Biol. 2007, 9, 21–40. [Google Scholar]
- Bergeron, M.G.; Ke, D.; Ménard, C.; Picard, F.J.; Gagnon, M.; Bernier, M.; Ouellette, M.; Roy, P.H.; Marcoux, S.; Fraser, W.D. Rapid Detection of Group B Streptococci in Pregnant Women at Delivery. N. Engl. J. Med. 2000, 343, 175–179. [Google Scholar]
- Scicchitano, L.M.; Bourbeau, P.P. Comparative Evaluation of the AccuProbe Group B Streptococcus Culture Test, the BD GeneOhm Strep B Assay, and Culture for Detection of Group B Streptococci in Pregnant Wome. J. Clin. Microbiol. 2009, 47, 3021–3023. [Google Scholar]
- Cunningham, R.; Jenks, P.; Northwood, J.; Wallis, M.; Ferguson, S.; Hunt, S. Effect on MRSA Transmission of Rapid PCR Testing of Patients Admitted to Critical Care. J. Hosp. Infect. 2007, 65, 24–28. [Google Scholar]
- Uçkay, I.; Sax, H.; Iten, A.; Camus, V.; Renzi, G.; Schrenzel, J.; Perrier, A.; Pittet, D. Effect of Screening for Methicillin-Resistant Staphylococcus aureus Carriage by Polymerase Chain Reaction on the Duration of Unnecessary Preemptive Contact Isolation. Infect. Control Hosp. Epidemiol. 2008, 29, 1077–1079. [Google Scholar] [CrossRef]
- Dalla Valle, C.; Pasca, M.R.; De Vitis, D.; Marzani, F.C.; Emmi, V.; Marone, P. Control of MRSA Infection and Colonisation in an Intensive Care Unit by GeneOhm MRSA Assay and Culture Methods. BMC Infect. Dis. 2009, 9, 137. [Google Scholar]
- Snyder, J.W.; Munier, G.K.; Johnson, C.L. Comparison of the BD GeneOhm Methicillin-Resistant Staphylococcus aureus (MRSA) PCR Assay to Culture by Use of BBL CHROMagar MRSA for Detection of MRSA in Nasal Surveillance Cultures from Intensive Care Unit Patients. J. Clin. Microbiol. 2010, 48, 1305–1309. [Google Scholar] [CrossRef]
- Hassan, H.; Shorman, M. Evaluation of the BD GeneOhm MRSA and VanR Assays as a Rapid Screening Tool for Detection of Methicillin-Resistant Staphylococcus aureus and Vancomycin-Resistant Enterococci in a Tertiary Hospital in Saudi Arabia. Int. J. Microbiol. 2011, 2011, 861514. [Google Scholar]
- Munson, E.; Bilbo, D.; Paul, M.; Napierala, M.; Hryciuk, J.E. Modifications of Commercial Toxigenic Clostridium difficile PCR Resulting in Improved Economy and Workflow Efficiency. J. Clin. Microbiol. 2011, 49, 2279–2282. [Google Scholar] [CrossRef]
- Selvaraju, S.B.; Gripka, M.; Estes, K.; Nguyen, A.; Jackson, M.A.; Selvarangan, R. Detection of Toxigenic Clostridium difficile in Pediatric Stool Samples: an Evaluation of Quik Check Complete Antigen Assay, BD GeneOhm Cdiff PCR, and ProGastro Cd PCR Assays. Diagn. Microbiol. Infect. Dis. 2011, 71, 224–229. [Google Scholar] [CrossRef]
- Pandit, A.; Mackay, W.G.; Steel, C.; van Loon, A.M.; Schuurman, R. HIV-1 Drug Resistance Genotyping Quality Assessment: Results of the ENVA7 Genotyping Proficiency Programme. J. Clin. Virol. 2008, 43, 401–406. [Google Scholar]
- Cepheid Home Page. Available online: http://www.cepheid.com (accessed in May 2012).
- Van Rie, A.; Page-Shipp, L.; Scott, L.; Sanne, I.; Stevens, W. Xpert® MTB/RIF for Point-of-Care Diagnosis of TB in High-HIV Burden, Resource-Limited Countries: Hype or Hope? Expert Rev. Mol. Diagn. 2010, 10, 937–946. [Google Scholar] [CrossRef]
- Donald, P.R.; Sirgel, F.A.; Venter, A.; Parkin, D.P.; Seifart, H.I.; van de Wal, B.W.; Werely, C.; van Helden, P.D.; Maritz, J.S. The Influence of Human N-Acetyltransferase Genotype on the Early Bactericidal Activity of Isoniazid. Clin. Infect. Dis. 2004, 39, 1425–1430. [Google Scholar]
- Kinzig-Schippers, M.; Tomalik-Scharte, D.; Jetter, A.; Scheidel, B.; Jakob, V.; Rodamer, M.; Cascorbi, I.; Doroshyenko, O.; Sörgel, F.; Fuhr, U. Should We Use N-Acetyltransferase Type 2 Genotyping to Personalize Isoniazid Doses? Antimicrob. Agents Chemother. 2005, 49, 1733–1738. [Google Scholar]
- Donald, P.R.; Parkin, D.P.; Seifart, H.I.; Schaaf, H.S.; van Helden, P.D.; Werely, C.J.; Sirgel, F.A.; Venter, A.; Maritz, J.S. The Influence of Dose and N-Acetyltransferase-2 (NAT2) Genotype and Phenotype on the Pharmacokinetics and Pharmacodynamics of Isoniazid. Eur. J. Clin. Pharmacol. 2007, 63, 633–639. [Google Scholar] [CrossRef]
- Betsou, F.; Parida, S.K.; Guillerm, M. Infectious Diseases Biobanking as a Catalyst Towards Personalized Medicine: Mycobacterium tuberculosis Paradigm. Tuberculosis 2011, 91, 524–532. [Google Scholar] [CrossRef]
- Faulstich, K.; Haberstroh, K. Handheld and Portable Test Systems for Decentralized Testing: from Lab to Marketplace. Proc. SPIE 2009, 7306, 73060H1–73060H8. [Google Scholar]
- Schimke, I. Quality and Timeliness in Medical Laboratory Testing. Anal. Bioanal. Chem. 2009, 393, 1499–1504. [Google Scholar]
- Kumar, A.; Roberts, D.; Wood, K.E.; Light, B.; Parrillo, J.E.; Sharma, S.; Suppes, R.; Feinstein, D.; Zanotti, S.; Taiberg, L.; Gurka, D.; Kumar, A.; Cheang, M. Duration of Hypotension before Initiation of Antimicrobial Therapy is the Critical Determinant of Survival in Human Septic Shock. Crit. Care Med. 2006, 34, 1589–1596. [Google Scholar]
- Lin, J.-N.; Lai, C.-H.; Chen, Y.-H.; Chang, L.-L.; Lu, P.-L.; Tsai, S.-S.; Lin, H.-L.; Lin, H.-H. Characteristics and Outcomes of Polymicrobial Bloodstream Infections in the Emergency Department: A Matched Case-Control Study. Acad. Emerg. Med. 2010, 17, 1072–1079. [Google Scholar]
- McGeer, A.; Green, K.A.; Plevneshi, A.; Shigayeva, A.; Siddiqi, N.; Raboud, J.; Low, D.E.; Toronto Invasive Bacterial Diseases Network. Antiviral Therapy and Outcomes of Influenza Requiring Hospitalization in Ontario, Canada. Clin. Infect. Dis. 45, 1568–1575.
- Klotz, S.A.; Chasin, B.S.; Powell, B.; Gaur, N.K.; Lipke, P.N. Polymicrobial Bloodstream Infections Involving Candida Species: Analysis of Patients and Review of the Literature. Diagn. Microbiol. Infect. Dis. 2007, 59, 401–406. [Google Scholar] [CrossRef]
- Brunstein, J.D.; Cline, C.L.; McKinney, S.; Thomas, E. Evidence from Multiplex Molecular Assays for Complex Multipathogen Interactions in Acute Respiratory Infections. J. Clin. Microbiol. 2008, 46, 97–102. [Google Scholar] [CrossRef]
- Rogers, G.B.; Hoffman, L.R.; Whiteley, M.; Daniels, T.W.; Carroll, M.P.; Bruce, K.D. Revealing the Dynamics of Polymicrobial Infections: Implications for Antibiotic Therapy. Trends Microbiol. 2010, 18, 357–364. [Google Scholar]
- Leggieri, N.; Rida, A.; François, P.; Schrenzel, J. Molecular Diagnosis of Bloodstream Infections: Planning to (Physically) Reach the Bedside. Curr. Opin. Infect. Dis. 2010, 23, 311–319. [Google Scholar]
- Nougairede, A.; Ninove, L.; Zandotti, C.; de Lamballerie, X.; Gazin, C.; Drancourt, M.; La Scola, B.; Raoult, D.; Charrel, R.N. Point of Care Strategy for Rapid Diagnosis of Novel A/H1N1 Influenza Virus. PLoS One 2010, 5, e9215. [Google Scholar]
- Cohen-Bacrie, S.; Ninove, L.; Nougairède, A.; Charrel, R.; Richet, H.; Minodier, P.; Badiaga, S.; Noël, G.; La Scola, B.; de Lamballerie, X.; Drancourt, M.; Raoult, D. Revolutionizing Clinical Microbiology Laboratory Organization in Hospitals with In Situ Point-of-Care. PLoS One 2011, 6, e22403. [Google Scholar]
- Bergeron, M.G. Revolutionizing the Practice of Medicine through Rapid (<1 h) DNA-Based Diagnostics. Clin. Invest. Med. 2008, 31, E265–E271. [Google Scholar]
- Association for Molecular Pathology. FDA-Cleared/Approved Molecular Diagnostics Tests (database). Available online: http://www.amp.org/FDATable/FDATable.doc (accessed in February 2012).
- BD Diagnostics GeneOhm Home Page. Available online: http://www.bd.com/geneohm (accessed in May 2012).
- Luminex Home Page. Available online: http://www.luminexcorp.com (accessed in May 2012).
- Benson, R.; Tondella, M.L.; Bhatnagar, J.; Carvalho, M.daG.S.; Sampson, J.S.; Talkington, D.F.; Whitney, A.M. ; Mothershed, E.; McGee, L.; Carlone, G.; McClee, V.; Guarner, J.; Zaki, S.; Dejsiri, S.; Cronin, K.; Han, J.; Fields, B.S. Development and Evaluation of a Novel Multiplex PCR Technology for Molecular Differential Detection of Bacterial Respiratory Disease Pathogens. J. Clin. Microbiol. 2008, 46, 2074–2077. [Google Scholar]
- Caliendo, A.M. Multiplex PCR and Emerging Technologies for the Detection of Respiratory Pathogens. Clin. Infect. Dis. 2011, 52 (suppl. 4), S326–S330. [Google Scholar]
- Endimiani, A.; Hujer, K.M.; Hujer, A.M.; Kurz, S.; Jacobs, M.R.; Perlin, D.S.; Bonomo, R.A. Are We Ready for Novel Detection Methods to Treat Respiratory Pathogens in Hospital-Acquired Pneumonia? Clin. Infect. Dis. 2011, 52 (suppl. 4), S373–S383. [Google Scholar]
- Russek-Cohen, E.; Feldblyum, T.; Whitaker, K.B.; Hojvat, S. FDA Perspectives on Diagnostic Device Clinical Studies for Respiratory Infections. Clin. Infect. Dis. 2011, 52 (suppl. 4), S305–S311. [Google Scholar]
- Ecker, D.J.; Sampath, R.; Li, H.; Massire, C.; Matthews, H.E.; Toleno, D.; Hall, T.A.; Blyn, L.B.; Eshoo, M.W.; Ranken, R.; Hofstadler, S.A.; Tang, Y.-W. New Technology for Rapid Molecular Diagnosis of Bloodstream Infections. Expert Rev. Mol. Diagn. 2010, 10, 399–415. [Google Scholar] [CrossRef]
- Seng, P.; Rolain, J.-M.; Fournier, P.E.; La Scola, B.; Drancourt, M.; Raoult, D. MALDI-TOF-Mass Spectrometry Applications in Clinical Microbiology. Future Microbiol. 2010, 5, 1733–1754. [Google Scholar]
- Dekker, J.P.; Branda, J.A. MALDI-TOF Mass Spectrometry in the Clinical Microbiology Laboratory. Clin. Microbiol. Newslett. 2011, 33, 87–93. [Google Scholar]
- La Scola, B. Intact Cell MALDI-TOF Mass Spectrometry-Based Approaches for the Diagnosis of Bloodstream Infections. Expert Rev. Mol. Diagn. 2011, 11, 287–298. [Google Scholar]
- Brzuszkiewicz, E.; Thürmer, A.; Schuldes, J.; Leimbach, A.; Liesegang, H.; Meyer, F.D.; Boelter, J.; Petersen, H.; Gottschalk, G.; Daniel, R. Genome Sequence Analyses of Two Isolates from the Recent Escherichia coli Outbreak in Germany Reveal the Emergence of a New Pathotype: Entero-Aggregative-Haemorrhagic Escherichia coli (EAHEC). Arch. Microbiol. 2011, 193, 883–891. [Google Scholar] [CrossRef]
- Emonet, S.; Shah, H.N.; Cherkaoui, A.; Schrenzel, J. Application and Use of Various Mass Spectrometry Methods in Clinical Microbiology. Clin. Microbiol. Infect. 2010, 16, 1604–1613. [Google Scholar]
- Mitka, M. Hospitalizations for Extreme Conditions Mean Extreme Expenses, Study Verifies. JAMA 2010, 304, 2579–2580. [Google Scholar]
- Ehrmeyer, S.S.; Laessig, R.H. Point-of-Care Testing, Medical Error, and Patient Safety: a 2007 Assessment. Clin. Chem. Lab. Med. 2007, 45, 766–773. [Google Scholar] [CrossRef]
- Nichols, J.H. Point of Care Testing. Clin. Lab. Med. 2007, 27, 893–908. [Google Scholar]
- Nichols, J.H. The Future of Point-of-Care Testing. Point Care 2008, 7, 271–273. [Google Scholar]
- Trevino, E.A.; Weissfeld, A.S. The Case for Point-of-Care Testing in Infectious-Disease Diagnosis. Clin. Microbiol. Newslett. 2007, 29, 177–179. [Google Scholar]
- Overturf, G.D. CLIA Waived Testing in Infectious Diseases. Pediatr. Infect. Dis. J. 2008, 27, 1009–1012. [Google Scholar]
- Rajan, A.; Glorikian, H. Point-of-Care Diagnostics: Market Trends and Growth Drivers. Expert Opin. Med. Diagn. 2009, 3, 1–4. [Google Scholar]
- Clerc, O.; Greub, G. Routine Use of Point-of-Care Tests: Usefulness and Application in Clinical Microbiology. Clin. Microbiol. Infect. 2010, 16, 1054–1061. [Google Scholar]
- Niemz, A.; Ferguson, T.M.; Boyle, D.S. Point-of-Care Nucleic Acid Testing for Infectious Diseases. Trends Biotechnol. 2011, 29, 240–250. [Google Scholar]
- Centers for Medicare and Medicaid Services (U.S. Department of Health and Human Services). Tests Granted Waived Status Under CLIA (database). Available online: http://www.cms.hhs.gov/CLIA/downloads/waivetbl.pdf (accessed in November 2011).
- Kibe, S.; Adams, K.; Barlow, G. Diagnostic and Prognostic Biomarkers of Sepsis in Critical Care. J. Antimicrob. Chemother. 2011, 66 (suppl. 2), ii33–ii40. [Google Scholar]
- Schuetz, P.; Albrich, W.; Mueller, B. Procalcitonin for Diagnosis of Infection and Guide to Antibiotic Decisions: Past, Present and Future. BMC Med. 2011, 9, 107. [Google Scholar]
- Luppa, P.B.; Müller, C.; Schlichtiger, A.; Schlebusch, H. Point-of-Care Testing (POCT): Current Techniques and Future Perspectives. Trends Anal. Chem. 2011, 30, 887–898. [Google Scholar]
- Jahn, U.R.; Van Aken, H. Near-Patient Testing—Point-of-Care or Point of Costs and Convenience? Br. J. Anesthesia 2003, 90, 425–427. [Google Scholar] [CrossRef]
- Huckle, D. Point-of-Care Diagnostics: an Advancing Sector with Nontechnical Issues. Expert Rev. Mol. Diagn. 2008, 8, 679–688. [Google Scholar]
- GenMark Diagnostics Home Page. Available online: http://www.genmarkdx.com (accessed in May 2012).
- Miller, M.B.; Tang, Y.-W. Basic Concepts of Microarrays and Potential Applications in Clinical Microbiology. Clin. Microbiol. Rev. 2009, 22, 611–633. [Google Scholar] [CrossRef]
- Weile, J; Knabbe, C. Current Applications and Future Trends of Molecular Diagnostics in Clinical Bacteriology. Anal. Bioanal. Chem. 2009, 394, 731–742. [Google Scholar] [CrossRef]
- Jordan, B.R. Is There a Niche for DNA Microarrays in Molecular Diagnostics? Expert Rev. Mol. Diagn. 2010, 10, 875–882. [Google Scholar] [CrossRef]
- Bauer, M.; Reinhart, K. Molecular Diagnostics of Sepsis—Where are We Today? Int J Med Microbiol 2010, 300, 411–413. [Google Scholar] [CrossRef]
- Cenciarini-Borde, C.; Courtois, S.; La Scola, B. Nucleic Acids as Viability Markers for Bacteria Detection Using Molecular Tools. Future Microbiol. 2009, 4, 45–64. [Google Scholar]
- Jofre, J. AR Blanch. Feasibility of Methods Based on Nucleic Acid Amplification Techniques to Fulfil the Requirements for Microbiological Analysis of Water Quality. J. Appl. Microbiol. 2010, 109, 1853–1867. [Google Scholar] [CrossRef]
- Ince, J.; McNally, A. Development of Rapid Automated Diagnostics for Infectious Diseases: Advances and Challenges. Expert Rev. Med. Devices 2009, 6, 641–651. [Google Scholar]
- Kiechle, F.L.; Holland, C.A. Point-of-Care Testing and Molecular Diagnostics: Miniaturization Required. Clin. Lab. Med. 2009, 29, 555–560. [Google Scholar]
- Bissonnette, L.; Bergeron, M.G. Diagnosing Infections - Current and Anticipated Technologies for Point-of-Care Diagnostics and Home-Based Testing. Clin. Microbiol. Infect. 2010, 16, 1044–1053. [Google Scholar]
- Eicher, D.; Merten, C.A. Microfluidic Devices for Diagnostic Applications. Expert Rev. Mol. Diagn. 2011, 11, 505–519. [Google Scholar]
- Haeberle, S.; Zengerle, R. Microfluidic Platforms for Lab-on-a-Chip Applications. Lab Chip 2007, 7, 1094–1110. [Google Scholar]
- Siegrist, J.; Peytavi, R.; Bergeron, M.G.; Madou, M. Microfluidics for IVD Analysis: Triumphs and Hurdles of Centrifugal Platforms - Part 1: Molecular Fundamentals. IVD Technol. 2009, 15 (9), 27–33. [Google Scholar]
- Gorkin, R.; Park, J.; Siegrist, J.; Amasia, M.; Lee, B.S.; Park, J.-M.; Kim, J.; Kim, H.; Madou, M.; Cho, Y.-K. Centrifugal Microfluidics for Biomedical Applications. Lab Chip 2010, 10, 1758–1773. [Google Scholar]
- Lien, K.-Y.; Lee, G.-B. Miniaturization of Molecular Biological Techniques for Gene Assay. Analyst 2010, 135, 1499–1518. [Google Scholar]
- Siegrist, J.; Peytavi, R.; Bergeron, M.G.; Madou, M. Microfluidics for IVD Analysis: Triumphs and Hurdles of Centrifugal Platforms - Part 2: Centrifugal Microfluidics. IVD Technol. 2010, 16(1), 41–47, 2010a. [Google Scholar]
- Ferguson, R.S.; Buchsbaum, S.F.; Wu, T.-T.; Hsieh, K.; Xiao, Y.; Sun, R.; Soh, H.T. Genetic Analysis of H1N1 Influenza Virus from Throat Swab Samples in a Microfluidic System for Point-of-Care Diagnostics. J. Am. Chem. Soc. 2011, 133, 9129–9135. [Google Scholar]
- Schumacher, S.; Nestler, J.; Otto, T.; Wegener, M.; Ehrentreich-Förster, E.; Michel, D.; Wunderlich, K.; Palzer, S.; Sohn, K.; Weber, A.; Burgard, M.; Grzesiak, A.; Teichert, A.; Brandenburg, A.; Koger, B.; Albers, J.; Nebling, E.; Bier, F.F. Highly-Integrated Lab-on-a-Chip System for Point-of-Care Multiparameter Analysis. Lab Chip 2011. DOI:10.1039/C1LC20693A.. [Google Scholar]
- Becker, H.; Gärtner, C. Polymer Microfabrication Technologies for Microfluidic Systems. Anal. Bioanal. Chem. 2008, 390, 89–111. [Google Scholar]
- Sollier, E.; Murray, C.; Maoddi, P.; Di Carlo, D. Rapid Prototyping Polymers for Microfluidic Devices and High Pressure Injections. Lab Chip 2011, 11, 3752–3765. [Google Scholar]
- Madou, M.; Zoval, J.; Jia, G.; Kido, H.; Kim, J.; Kim, N. Lab on a CD. Annu. Rev. Biomed. Eng. 2006, 8, 601–628. [Google Scholar]
- Oh, K.W.; Ahn, C.H. A Review of Microvalves. J. Micromech. Microeng. 2006, 16, R13–R39. [Google Scholar]
- Nolte, D.D. Invited Review Article: Review of Centrifugal Microfluidic and Bio-Optical Disks. Rev. Sci. Instrum. 2009, 80, 101101. [Google Scholar]
- Mosadegh, B.; Bersano-Begey, T.; Park, J.Y.; Burns, M.A.; Takayama, S. Next-Generation Integrated Microfluidic Circuits. Lab Chip 2011, 11, 2813–2818. [Google Scholar]
- Cho, Y.-K.; Lee, J.-G.; Park, J.-M.; Lee, B.-S.; Lee, Y.; Ko, C. One-Step Pathogen Specific DNA Extraction from Whole Blood on a Centrifugal Microfluidic Device. Lab Chip 2007, 7, 565–573. [Google Scholar]
- Wen, J.; Legendre, L.A.; Bienvenue, J.M.; Landers, J.P. Purification of Nucleic Acids in Microfluidic Devices. Anal. Chem. 2008, 80, 6472–6479. [Google Scholar]
- Kim, J.; Johnson, M.; Hill, P.; Gale, B.K. Microfluidic Sample Preparation: Cell Lysis and Nucleic Acid Purification. Integr. Biol. 2009, 1, 574–586. [Google Scholar]
- Baek, S.-K.; Min, J.; Park, J.-H. Wireless Induction Heating in a Microfluidic Device for Cell Lysis. Lab Chip 2010, 10, 909–917. [Google Scholar]
- Siegrist, J.; Gorkin, R.; Bastien, M.; Stewart, G.; Peytavi, R.; Kido, H.; Bergeron, M.G.; Madou, M. Validation of a Centrifugal Microfluidic Sample Lysis and Homogenization Platform for Nucleic Acid Extraction with Clinical Samples. Lab Chip 2010, 10, 363–371, 2010b. [Google Scholar]
- Root, B.E.; Agarwal, A.K.; Kelso, D.M.; Barron, A.E. Purification of HIV RNA from Serum Using a Polymer Capture Matrix. Anal. Chem. 2011, 83, 982–988. [Google Scholar]
- Zhang, C.; Xu, J.; Ma, W.; Zheng, W. PCR Microfluidic Devices for DNA Amplification. Biotechnol. Adv. 2006, 24, 243–284. [Google Scholar]
- Zhang, Y.; Ozdemir, P. Microfluidic DNA Amplification - A Review. Anal. Chim. Acta 2009, 638, 115–125. [Google Scholar]
- Cooney, C.G.; Sipes, D.; Thakore, N.; Holmberg, R.; Belgrader, P. A Plastic, Disposable Microfluidic Flow Cell for Coupled On-Chip PCR and Microarray Detection of Infectious Agents. Biomed. Microdevices 2011. DOI 10.1007/s10544-011-9584-9.. [Google Scholar]
- Marasso, S.L.; Giuri, E.; Canavese, G.; Castagna, G.; Quaglio, M.; Ferrante, I.; Perrone, D.; Cocuzza, M. A Multilevel Lab on Chip Platform for DNA Analysis. Biomed. Microdevices 2011, 13, 19–27. [Google Scholar] [CrossRef]
- Sun, Y.; Perch-Nielsen, I.; Dufva, M.; Sabourin, D.; Bang, D.D.; Hogberg, J.; Wolff, A. Direct Immobilization of DNA Probes on Non-Modified Plastics by UV Irradiation and Integration in Microfluidic Devices for Rapid Bioassay. Anal. Bioanal. Chem. 2011. DOI 10.1007/s00216-011-5459-4.. [Google Scholar]
- Wang, L.; Li, P.C.H. Microfluidic DNA Microarray Analysis: a Review. Anal. Chim. Acta 2011, 687, 12–27. [Google Scholar]
- Goff, D.A. Antimicrobial Stewardship: Bridging the Gap between Quality Care and Cost. Curr. Opin. Infect. Dis. 2011, 24 (suppl. 1), S11–S20. [Google Scholar]
- Micek, S.T.; Reichley, R.M.; Kollef, M.H. Health Care-Associated Pneumonia (HCAP) - Empiric Antibiotics Targeting Methicillin-Resistant Staphylococcus aureus (MRSA) and Pseudomonas aeruginosa Predict Optimal Outcome. Medicine 2011, 90, 390–395. [Google Scholar] [CrossRef]
- Dellinger, R.P.; Levy, M.M.; Carlet, J.M.; Bion, J.; Parker, M.M.; Jaeschke, R.; Reinhart, K.; Angus, D.C.; Brun-Buisson, C.; Beale, R.; Calandra, T.; Dhainaut, J.-F.; Gerlach, H.; Harvey, M.; Marini, J.J.; Marshall, J.; Ranieri, M.; Ramsay, G.; Sevransky, J.; Thompson, B.T.; Townsend, S.; Vender, J.S.; Zimmerman, J.L.; Vincent, J.-L. for the International Surviving Sepsis Campaign Guidelines Committee. Surviving Sepsis Campaign: International Guidelines for Management of Severe Sepsis and Septic Shock: 2008. Crit. Care Med. 2008, 36, 296–327. [Google Scholar]
- Brown, J.; Paladino, J.A. Impact of Rapid Methicillin-Resistant Staphylococcus aureus Polymerase Chain Reaction Testing on Mortality and Cost Effectiveness in Hospitalized Patients with Bacteraemia. Pharmacoeconomics 2010, 28, 567–575. [Google Scholar]
- Bauer, K.A.; West, J.E.; Balada-Llasat, J.-M.; Pancholi, P.; Stevenson, K.B.; Goff, D.A. An Antimicrobial Stewardship Program's Impact with Rapid Polymerase Chain Reaction Methicillin Staphylococcus aureus/S. aureus Blood Culture Test in Patients with S. aureus Bacteremia. Clin. Infect. Dis. 2010, 51, 1074–1080. [Google Scholar] [CrossRef]
- Paolucci, M.; Landini, M.P.; Sambri, V. Conventional and Molecular Techniques for the Early Diagnosis of Bacteraemia. Int. J. Antimicrob. Agents 2010, 36S, S6–S16. [Google Scholar]
- McGeer, A.J. Diagnostic Testing or Empirical Therapy for Patients Hospitalized with Suspected Influenza: What to Do? Clin. Infect. Dis. 2009, 48, S14–S19. [Google Scholar] [CrossRef]
- Infectious Diseases Society of America. An Unmet Medical Need: Rapid Molecular Diagnostics Tests for Respiratory Tract Infections. Clin. Infect. Dis. 2011, 52 (S4), S384–S395. [Google Scholar]
- Shen, B.; Hwang, J. The Clinical Utility of Precision Medicine: Properly Assessing the Value of Emerging Diagnostic Tests. Clin. Pharmacol. Ther. 2010, 88, 754–756. [Google Scholar]
- Mirnezami, R.; Nicholson, J.; Darzi, A. Preparing for Precision Medicine. N. Engl. J. Med. 2012, 366, 489–491. [Google Scholar]
- Richmond, T.D. The Current Status and Future Potential of Personalized Diagnostics: Streamlining a Customized Process. Biotechnol. Annu. Rev. 2008, 14, 411–422. [Google Scholar]
- Ehrmeyer, S.S.; Laessig, R.H. Regulatory Compliance for Point-of-Care Testing: 2009 United States Perspective. Clin. Lab. Med. 2009, 29, 463–478. [Google Scholar]
- Gibbs, J.N. Regulating Molecular Diagnostic Assays: Developing a New Regulatory Structure for a New Technology. Expert Rev. Mol. Diagn. 2011, 11, 367–381. [Google Scholar]
- Genetic Information Nondiscrimination Act (GINA) of 2008. Available online: http://www.genome.gov/24519851 (accessed in May 2012).
- Glinskii, V.G.; Glinsky, G.V. Emerging Genomic Technologies and the Concept of Personalized Medicine. Cell Cycle 2008, 7, 2278–2285. [Google Scholar]
- Hudson, K.L. Genomics, Health Care, and Society. N. Engl. J. Med. 2011, 365, 1033–1041. [Google Scholar] [CrossRef]
- Rogowski, W. Current Impact of Gene Technology on Healthcare—A Map of Economic Assessments. Health Policy 2007, 80, 340–357. [Google Scholar]
© 2012 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/3.0/).
Share and Cite
Bissonnette, L.; Bergeron, M.G. Infectious Disease Management through Point-of-Care Personalized Medicine Molecular Diagnostic Technologies. J. Pers. Med. 2012, 2, 50-70. https://doi.org/10.3390/jpm2020050
Bissonnette L, Bergeron MG. Infectious Disease Management through Point-of-Care Personalized Medicine Molecular Diagnostic Technologies. Journal of Personalized Medicine. 2012; 2(2):50-70. https://doi.org/10.3390/jpm2020050
Chicago/Turabian StyleBissonnette, Luc, and Michel G. Bergeron. 2012. "Infectious Disease Management through Point-of-Care Personalized Medicine Molecular Diagnostic Technologies" Journal of Personalized Medicine 2, no. 2: 50-70. https://doi.org/10.3390/jpm2020050
APA StyleBissonnette, L., & Bergeron, M. G. (2012). Infectious Disease Management through Point-of-Care Personalized Medicine Molecular Diagnostic Technologies. Journal of Personalized Medicine, 2(2), 50-70. https://doi.org/10.3390/jpm2020050