
Unveiling Gender-Based Musculoskeletal Disorders in the Construction Industry: A Comprehensive Analysis

1
Department of Civil Engineering, University College of Engineering, Panruti 607106, India
2
Department of Civil Engineering, M. Kumarasamy College of Engineering, Karur 639113, India
3
Center of Excellence in Interdisciplinary Research for Sustainable Development, Faculty of Engineering, Chulalongkorn University, Bangkok 10330, Thailand
*
Authors to whom correspondence should be addressed.
Buildings 2024, 14(4), 1169; https://doi.org/10.3390/buildings14041169
Submission received: 24 February 2024
/
Revised: 2 April 2024
/
Accepted: 14 April 2024
/
Published: 21 April 2024
(This article belongs to the Section Construction Management, and Computers & Digitization)
Abstract
:Without physically intensive building, modern infrastructure development would be impossible. Musculoskeletal diseases (MSDs) and other occupational health issues may arise in such a demanding environment. Construction workers often develop MSDs from repeated actions, uncomfortable postures, and heavy lifting. Musculoskeletal disorders may damage muscles, bones, tendons, ligaments, etc. The effect of MSDs is well known; occupational health studies increasingly include gender-specific aspects. Despite being in the minority, the number of female construction employees is growing. However, physiological variations and occupational activities and environments may provide distinct obstacles. Thus, identifying gender-specific MSDs in construction is essential for worker safety. This research proposes a gender-specific machine learning (ML)-based musculoskeletal disorder detection framework (GS-ML-MSD2F) in the construction industry. A simple random selection procedure chose 250 female and 250 male rebar workers with at least six months of experience for the dataset. In January and June 2023, face-to-face interviews and ergonomic evaluations were undertaken. The data were analyzed using different machine learning methods, and the effectiveness of the methods was studied. The data showed that 60% of female rebar workers had MSD symptoms. The lower back and shoulders accounted for 40% of cases. Multiple machine learning methods revealed two significant factors related to musculoskeletal disorders: lengthy working hours and uncomfortable postures, and long working hours had an adjusted odds ratio of 8.5%, whereas awkward posture had an adjusted odds ratio of 42.5%. These results emphasize the relevance of working hours and posture in MSD prevention for female rebar workers in the construction sector.
1. Introduction
It is estimated that 73 million people across the world are subjected to physical stress on the job. Careers in farming, mining, building, and cleaning are just a few examples; all fall under the category of “hazardous labor” [1]. Women and girls are more likely to start working before they are mature enough to handle the responsibilities of an adult, take on additional home responsibilities, work longer hours, and receive less nutritious food, based on data by the WHO [2,3]. Increases in both the prevalence of diseases and the number of people needing medical attention coincide with India’s rapidly changing demographic profile [4]. Due to a lack of comprehensive social security institutions, however, the healthcare system is woefully inadequate to deal with the health problems associated with an increasingly elderly population [5]. Additionally, India confronts vast disparity in social and economic factors that have led to a “triple burden of diseases” or the simultaneous emergence of communicable diseases, non-communicable illnesses, and new infectious illnesses [6]. Barriers exist in the form of uncontrolled systems, a lack of resources, an inefficient public health system, a predominately privatized health sector, and large out-of-pocket expenditure (OOPE) when it comes to providing healthcare for people [7].
An “adverse response individuals have to too much pressure or different kinds of demand placed upon them” is how stress at work is defined [8]. Stress in the workplace is a leading contributor to occupational illness, which includes a wide range of conditions, from musculoskeletal diseases and depression to injuries and heart disease [9]. When an organization has an issue with worker safety or productivity, they may often request an ergonomics job-related analysis and intervention, often known as francophone ergonomics [10]. Ergonomists spend a lot of time observing workers to get a thorough grasp of their work and the physical, mental, social, and organizational factors that contribute to the issue. The challenging components are targeted for intervention if the research’s participants confirm the ergonomist’s judgment [11]. Partnerships with stakeholders like employers and unions in the workplace facilitate learning about critical health and productivity concerns and developing strategies to address them [12]. Such investigations rely heavily on long-term observations of work occurring at deliberately chosen locations and times, with verification from employees and other relevant informants [13]. Workers are monitored to determine what factors affect their performance, such as hazards in the workplace that make it difficult for them to work safely [14]. Work has varied effects on men and women because of persistent discrimination in the workplace. Women and men are commonly segregated into various fields, complete distinct activities even within the same field (horizontal segregation), and have unequal power structures within their respective companies (vertical segregation) [15].
Therefore, occupational health studies must account for differences in risks and outcomes based on sex and gender [16]. Studies of the physical or physiological aspects of work may benefit from the consideration of sex (biological differences). In contrast, studies of the social, identity, or power aspects of work may benefit from consideration of gender (social roles) [17]. Because of the interconnected nature of the physical and social dimensions of exposure, it can be challenging to draw clear distinctions between sex and gender in practice [18]. Workplace environments are fraught with underlying tensions, including competing social, political, and economic interests, which must be carefully considered when attempting to integrate a sex- or gender-sensitive strategy into occupational health research involving ergonomic solutions. The importance of scientific understanding regarding working conditions and occupational health is heightened when contrasting work-related ideals are considered, such as workplace freedom and development versus productivity in the face of competitive pressures and the need to decrease costs. This information can be fabricated and put to use in ways that are not necessarily conducive to health maintenance, such as for the sake of financial gain. One example of clashing interests is the widespread use of standardized tests in the recruitment process, even when they have little bearing on the position being filled. This can lead to systemic discrimination against women.
Stress in the workplace is linked to decreased output and higher expenses. When it comes to stress at work, the construction industry ranks near the top. In the construction industry, professionals frequently face limited resources and severe deadlines, with costly consequences for any slips. Long hours are typical in the construction sector. The high levels of change and uncertainty inherent in construction projects increase the difficulty of the work involved. Construction workers face additional pressure from factors like poor communication, unpleasant environments at work, and job confusion and conflict. Insufficient feedback, inadequate interaction, insufficient personnel, overly ambitious deadlines, work pressure, and contradictory demands have been recognized as the most common causes of stress in the workplace. Strain effects, or unfavorable reactions to stress in the workplace, are common among construction workers. Physical symptoms (such as skeletal-muscular discomfort, lack of appetite, sweating, palpitations, and trembling) and adverse feelings (such as worrying, weariness, and anxiety) are just some of the strain symptoms that are observed among construction professionals due to work stress [19].
There is no doubt that construction sector workers experience high levels of stress, which calls for more research into the problem’s sources, impacts, and potential solutions. Professionals’ reactions to stress and their methods for dealing with it in the construction business have received less attention than they deserve [20]. Women are more likely to sustain injuries on the job in settings that were created with men in mind, according to these studies. The mental health of women is negatively impacted by macho culture and other factors (such as a lack of education and tools designed specifically for women’s bodies, forms, and physical aptitudes).
The most important contributions of this research are as follows:
The present research puts forth a framework for the detection of musculoskeletal disorders in the building trade that is informed by gender-specific machine learning (ML). Consequently, it is essential for construction worker safety to identify MSDs that affect one gender. In-person interviews and assessments of working conditions were conducted. Various machine learning techniques are applied to the data, and their efficacy is evaluated. Approximately 60% of the women who worked with rebar reported experiencing symptoms consistent with MSD. Pain in the lower back and shoulders accounts for 40% of all cases.
Long work hours and awkward postures are highlighted by several machine-learning approaches as major contributors to musculoskeletal problems. These findings highlight the importance of working hours and posture in preventing MSDs for female rebar workers in the construction industry. This outline serves as the foundation for the rest of the paper. In Section 1, we provide a thorough overview, and in Section 2, we analyze the relevant literature. In Section 3, we will discuss the purpose and operation of the gender-specific machine learning (ML) based musculoskeletal disorder detection framework (GS-ML-MSD2F). The experimental setup is presented in Section 4. Section 5 wraps up the research by speculating on what comes next.
2. Literature Review
In this section, we will consider the most recent achievements of scientists around the globe.
Habib, R. R. et al. [21] investigated differences in ergonomic risks and musculoskeletal illnesses [DER-MI] in their study, with a focus on the effects of sex and gender. Musculoskeletal problems, as well as data on demographics, occupations, and socioeconomic status, were compiled. The findings suggested that children participated in vigorous activity. Girls were more likely to perform repeated motions, whereas boys were more likely to lift large objects. Girls completed more work at home and in the community, making them more susceptible to wrist and hand pain. While more boys said their pay was contingent on reaching a daily production quota, more women said they were under pressure to complete their tasks on time. Refugee children from Syria who are working require emergency health protection. Younger children may be discouraged from working by these interventions, while those aimed at youngsters of working age may make them able to work in safer conditions.
Messing, K. et al. [22] incorporated the ergonomics of workplace tasks [EWT] into their study. It relies primarily on observation to help businesses revamp their operations for better health without sacrificing efficiency. Attempts by ergonomists to incorporate gender into their interventions have gained momentum in recent years. Similarly, ergonomists have been noting and recording how crucial it is to take into account the social aspects of work, such as the formation of relationships between employees. There are many ways in which gender and biological sex can have an impact on the workplace, including (1) gendered employment and task allocations; (2) genetic differences between genders impact how individuals respond to their surroundings on the job; and (3) ties between workers and upper management or clients that are based on gender rather than merit or competence. Considering actions indicative of a healthy work–life balance, an ergonomist has a number of challenges when trying to observe these events.
Laberge, M. et al. [23] delivered a study focusing on the fields of ergonomics and occupational health; the results of incorporating sex and gender (s/g) analysis into knowledge-based translation (iKT) are the focus of this article, with Projects [S/G-iKT]. The results of the thematic analysis of 15 in-depth interviews with researchers involved in these IRs are reported below. The findings paint a comprehensive picture of the ripple impacts in several domains, such as partners’ perceptions, organizational contexts, policies and procedures, and financial outcomes. The assessment of direct health outcomes is challenging in this category of IR when measuring health consequences is not the primary goal. In contrast to treatments in which the issues of gender and sex were not explicitly addressed, those in which they were led to changes at the systemic rather than the organizational level.
Important strain effects (ISEs) encountered by construction workers have been substantiated, and the importance and effectiveness of countermeasures are emphasized in a paper by Bowen P. et al. [24]. The work involved in the construction industry is really strenuous. Many workers in the construction industry face stress at work, which can have negative impacts on their bodies, minds, and communities. To offset these consequences, they employ a wide range of coping strategies. In Cape Town, South Africa, experts in the building trade (architects, project managers, construction managers, civil engineers, and quantity surveyors) were polled to ascertain their take on workplace stress and how to alleviate it. The results suggest that dissatisfaction, exhaustion, interpersonal stress, occupational stress, and emotional distress were the top five most impactful strain effects. Male professionals reported more exhaustion and dissatisfaction than their female counterparts, whereas women reported more low self-esteem. With respect to effectiveness, “travel”, “non-competitive sporting activity”, “music”, “increased caffeine intake”, and “walking” ranked as the top coping techniques. Men were found to prefer more strenuous physical activities than women.
Sahoo, H. et al. [25] introduced assessing the current state of health concerns (ACHCs), which is crucial for achieving the goals related to healthy ageing and reflecting the momentum produced surrounding the issue of an ageing population in India. The research synthesizes empirical research papers to talk about the healthcare requirements of the elderly, how often they use medical services, and how much they end up spending on medical care. The review used a systematic search strategy to find all applicable studies that met the inclusion and exclusion criteria. Over seventy studies were included after applying the inclusion criteria for the analysis and systematic review. Existing gender and erotological research in India pays scant attention to the health of older women or the health effects of widowhood, despite the fact that India’s ageing population is becoming increasingly female, characterized by a high rate of widowhood among elderly ladies. Inadequate insurance protection and high out-of-pocket medical costs represent a serious threat to the financial security of the elderly, especially those from lower socioeconomic backgrounds. Micro-level interventions, in which families play a central role in improving caring, are needed to address health inequalities among the elderly in India effectively. Reduced medical costs for low-income seniors can be achieved by expanded health insurance and the building of supported high-quality public health facilities.
DER-MI, EWT, S/G- iKT, ISE, and ACHC are all popular models that could benefit from refinements to increase their utility. The following have been highlighted as areas where more information is needed. However, research investigating the efficacy of combining treatment modalities for musculoskeletal disorders is sparse. The present research puts forth a framework for the detection of musculoskeletal disorders in the building trade that is informed by gender-specific machine learning (ML).
Gender-specific machine learning-based musculoskeletal disorder detection framework (GS-ML-MSD2F): The age at which participants began working, the nature of their employment (seasonal, year-round, or both), the participants’ occupations, the number of hours they worked per day, whether or not they took a week off each year, the number of years they worked, and whether or not they took a weekly vacation were examined. In total, 96% of women and 91% of men said they repeatedly extended and flexed their elbows for more than 1 h every day. Females were more likely than males to report daily wrist and finger movements of more than 4 h. Six factors were used to determine a person’s ergonomic risk: the number of times they had to bend and straighten their elbows, the number of times they had to move their wrists and fingers, the number of times they had to squat or kneel, the number of times they had to work with their hands higher than their shoulders, the number of times they had to lift more than 30 pounds, and the number of times they had to climb stairs. The research analyzed the effects of work stress on working women.
The survey asked respondents whether or not they had ever experienced any of the following forms of work pressure: their employer paying them based on the number of tasks they complete each day, being required to complete a certain number of tasks every day, and being paid more as a result; laboring under duress to complete the task on time; and laboring through severe pain for fear of job loss. Several inquiries concerned domestic chores: whether or not they have been completed (yes/no), how often (hours per week), and what kind of work is carried out. Core housework duties such as cleaning, laundry, ironing, and cooking were performed, and people (childcare and eldercare) and the home itself (groceries, water, and gas for heating), maintaining the home (cleaning, repairs, washing vehicles, garbage collection), transporting heavy items (water, mattresses), and escorting family members were also included. Self-reports of discomfort in the following musculoskeletal areas were used to diagnose musculoskeletal disorders: the wrist or hand, the foot, the back, the neck, the shoulders, the elbow, the joints, and the knee.
More men than women said they spent more than an hour a day working with their hands above their shoulders. The percentage of men who said they regularly lifted 35 kg loads throughout the workday was 40.1%, whereas the percentage of women was 23.2%. Males were more likely to report using staircases more than 25 times per day (16.3% vs. 10.1%). Many young people, especially young women and young men have experienced work pressure to complete tasks on time. Similarly, women were more likely than men to women report receiving a bonus for meeting daily productivity targets. However, more men than women claimed that their pay was contingent upon the quantity of goods sold each day.
Issues related to the musculoskeletal system:
Multiple sclerosis was reported by about 4% of working women. Back discomfort, foot pain, joint pain, and knee pain are the most often reported MS conditions. The prevalence of wrist or hand pain is much lower among men than among women. Male and female street service workers reported significantly different rates of MS problems. Women were more likely than men to complain of wrist or hand pain if they repeatedly bent and straightened their elbows for more than an hour a day. In addition, women were more likely than men to complain of wrist or hand pain if they spent more than an hour a day working with their hands higher than their shoulders.
3. Materials and Methods
Figure 1 shows the coding structure and related concepts given for a clear idea about the proposed methodology. Intervention research (IR) fact sheets were created first. These documents detailed the IR’s setting, including the proposal’s initiator, the intervention’s design, the involved parties, and the intended recipients of the s/g transformative approach. With an inductive method (interviewers did not indicate an impact category), a hierarchical classification analysis was conducted. Two research assistants and the lead investigator independently completed vertical coding on the entire interview content (less than 10% disagreement) to provide an initial analysis framework. A final set of codes and their meaning was agreed upon after a detailed discussion of the data content and coding following this initial data entry. Hence, to develop the analytical methodology further, the project committee was provided with textual excerpts and IR briefs on three separate occasions. Through this iterative process, we were able to refine our coding categories and levels. The first-level themes of these numerous case studies describe the various methodological components of the IR, which can be used to identify the various logic models now in use for interventions of this type. This kind of analysis is fundamental in learning about the positive and negative effects of IR elements. We can already assert that there are many moving parts and that they are intricate. Interventions are more likely to be effective if researchers are able to tailor their strategies to the unique needs and priorities of their community partners. The methodological aspects that lead to success in various contexts could be investigated in future studies. As it stands, we can confidently assert that studying gender in the workplace requires a socio-constructivist worldview and would suffer from the use of methods developed with positivist epistemology.
where
From the above Equation (1), is the vector solution where denotes the position and is the real numbers randomly chosen between (0 and 1). is a constant, and is a random integer within a given range (0, 1) in Equation (2).
In the above Equation (3), is the probability vector of node and is the feasible solution vector.
Figure 1.
Coding structure and related concepts.

Consequences of Workplace Stress:
In accordance with the widely accepted interactional approach to stress, we use the term “stress” to refer to a holistic concept that incorporates stimuli from the environment and demands (i.e., stressors), stress responses (i.e., strains), and additional factors (e.g., personality, coping strategies, and environmental support) that all influence the relationship between stressors and strains. Figure 2 shows the interplay between stressors, strain effects, and moderating variables. Conversely, stress is a mental condition caused by a mismatch between what must be done and what a person has available to help them complete the task at hand, such as in the case of a busy workplace. Strains are reactions to stress with harmful consequences. Previous studies have found a number of distinct strains, each of which manifests uniquely. Headaches, gastrointestinal problems, heart disease, depression, anxiety, poor decision-making, memory loss, and impulsive behavior are just some of the physical, mental, cognitive, and behavioral strains that have been identified. Interpersonal stresses caused by stressors can cause rifts in personal relationships, while occupational stresses have a negative effect on productivity and well-being in the office. Stress can have unintended consequences for a person’s relationships with friends and family.
A b-strategy is any conceivable tactic; is the number of mutants that have reached a crucial level in Equation (4).
Equation (5) indicates that is the b strategy for q parts of stress, is the mutual function for a random integer, is the constant used for conversion, is the stress factor, is the coefficient of the mutual index between the related factors, is the part of related factors, and is the stress for the bilingual m kind of people.
Equation (6) indicates the intervening variables and is the coefficient for the same, is the stress related to the workload and poor working conditions, is the strain effects, and is the work pressure that presents consequences.
Figure 2.
Correlations among stresses, buffering factors, and tension outcomes.

Previous studies have shown a wide range of deleterious consequences of job stress in the construction sector, many of which are analogous to the aforementioned strain effects. When construction project managers are under excessive pressure at work (such as from meeting project deadlines and completing their workload), they may experience burnout, a psychological response that manifests physically in the form of a wide range of symptoms, including fatigue, dizziness, nausea, and vomiting. Research shows that construction project managers’ stress levels have a negative effect on their productivity and relationships with co-workers.
Some of the characteristics in the research were linked to MSD reports using Chi-square tests and logistic regression analyses. The MSDs were taken as the experimental units of analysis. Figure 3 depicts the independent variables that were defined, which included demographic traits and certain workplace conditions. In this, the psychological and physical factors that contribute to the socio-demographic factors that relate to the work related to musculoskeletal disorders are taken into consideration. Work-related stress, job satisfaction, social support, a steady work tempo, and general good health are examples of psychological aspects; physical factors include things like working posture, workload, repetitive moments, and vibration. The goal of this cross-sectional study is to look at how certain characteristics are associated with an increased incidence of musculoskeletal condition pain and discomfort among female construction workers. This cross-sectional study set out to look at how the likelihood of developing a musculoskeletal disorder is associated with certain demographic and lifestyle characteristics among female construction workers.
Equation (7) represents the musculoskeletal disorder, and is the work-related musculoskeletal disorder and is the socio-demographic factor.
Equation (8) represents the socio-demographic factor, where represents the psychological factors and and are the physical factors.
is the psychological factors, where is work stress, is work satisfaction, is social support, is the workplace, and is the good health in Equation (9)
is the physical factors, where is working posture, is workload, is repetitive movement, and is body vibration in Equation (10).
By substituting (9) and (10) into Equation (8), we obtain
The term “psychosocial factors at work” is used to describe the ways in which a person’s physical and mental well-being, as well as their productivity and contentment in their job, are affected by their exposure to and management of various aspects of the workplace and the organization in which they work. They may be exposed to stress and other work-related musculoskeletal disorder (WRMSD) triggers. Somatic stress symptoms, such as abdominal pain, head pain, and heart palpitations, appear to be linked to one another. Participants with at least one WRMSD in any body segment who took part in research relating to psychosocial factors reported lower job satisfaction, less teamwork and interaction among co-workers and less support from superiors.
WRMSDs can be caused by stresses, repetition, vibrations, and awkward positions. Female workers’ WRMSDs were shown to be significantly associated with patient-handling jobs. When it comes to being healthy on the job, there are a number of physical elements to consider. Carrying heavy goods, dragging or pushing machines, lifting patients, performing repeated actions, extreme flexion, bending, twisting, and sudden motions are some of the physical challenges that workers experience. More and more parts of the body start to have issues as a result of the elevated levels of physical activity. Other causes of MSDs include prolonged periods of standing and uncomfortable body positions.
Figure 3.
In-depth conceptualization framework.

There are two main types of musculoskeletal disorders (MSDs): specific and non-specific. Pain in the musculoskeletal system without convincing evidence of a specific condition characterizes non-specific musculoskeletal disorders. Overuse syndrome, repetitive motion injuries, cumulative trauma disorders, RSIs, CTDs, overuse injuries, regional musculoskeletal diseases, and soft tissue disorders are all kinds of issues related to musculoskeletal disorders. Although the lower extremities have gained more attention as of late, the lower back, neck, shoulders, knees, forearms, hands, and ankles/feet are the parts of the body with the highest prevalence of WRMSDs. The extremities, trunk, or both can be affected by MSDs.
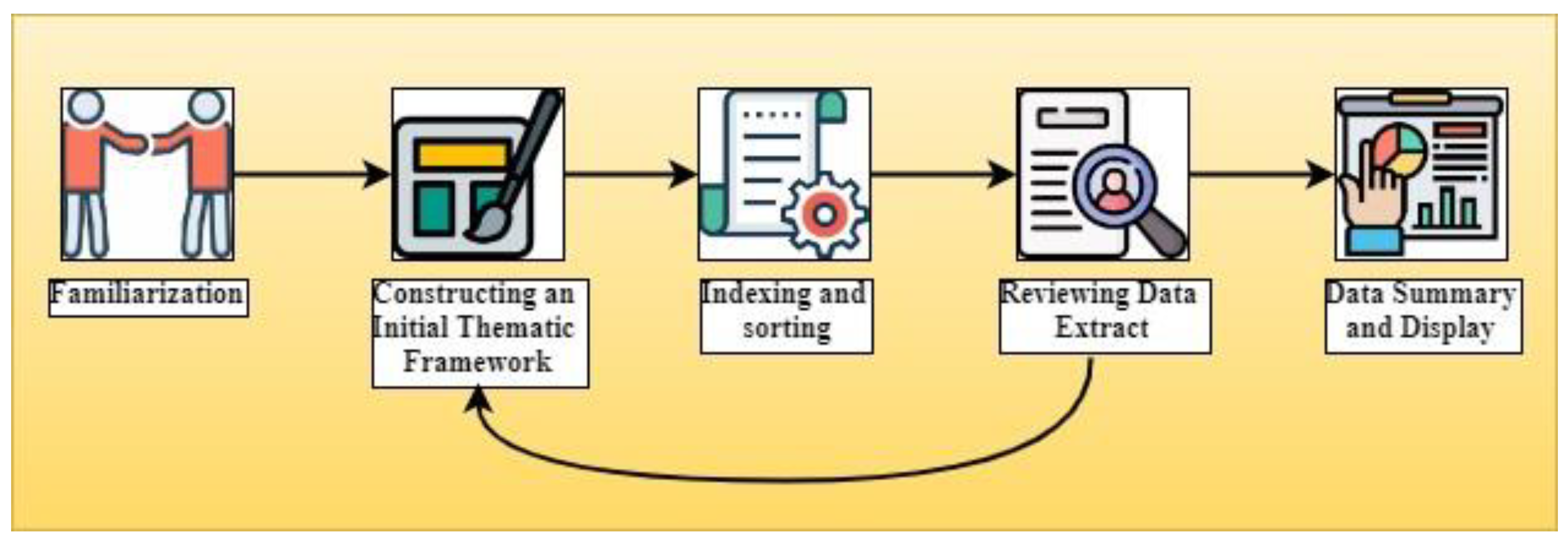
Common in mixed-method studies is the use of a “generic” qualitative analysis strategy. A “framework approach” is adopted, which consists of five interconnected steps to provide shape to the analysis. The first author began the analytical process by reading and rereading the transcripts to become familiar with the data and then coded the data. Another author, who is a specialist in qualitative research, reviewed the coding procedure. The coding and categorizing activities benefited from “mapping” techniques (Figure 4). Each category is described, and those with similar meanings were reclassified under overarching “thematic” headings. We went back and looked at the labels and descriptions we used for the raw data to make sure they represented the interview data and to see if any information we had coded should have been moved to new categories. In total, 19 categories and four overarching themes emerged from this procedure. The survey research phase began with a questionnaire based on the results of the qualitative research phase.
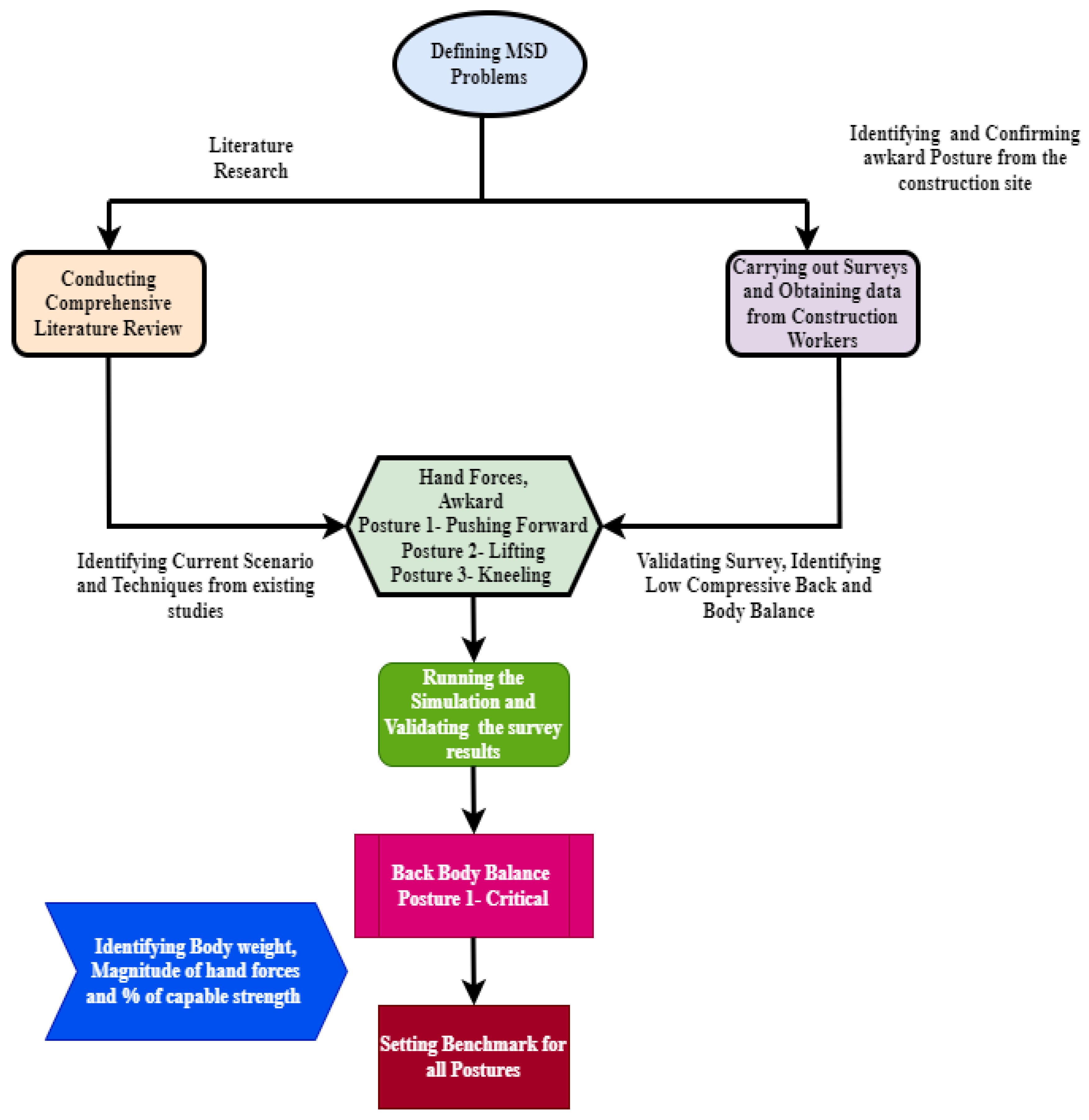
Figure 5 depicts the research methodology map. Four “processes” and two “outputs”, denoted by numbers (1) through (5), were involved in each phase of this study. Therefore, to choose the variables and construct the simulation model for each “process”, we applied a set of criteria (or standard mean). The first step was to conduct extensive literature evaluations to determine the factors (such as anthropometry and hand forces) that contribute to workers’ MSDs. Second, research involving anthropometry and hand forces was reviewed extensively to determine their role in employees’ MSDs. Third, research on workers performing construction-related tasks verified the variables that influenced workers’ MSD symptoms. The research yielded anthropometric and hand-force information on uncomfortable stances. According to the results, there are a few difficult postures that stand out when performing a certain task: advancing, lifting, and kneeling. This model predicts the changes in physical demands as workers move from one awkward posture to another, takes pictures of each awkward posture, creates a digital twin of virtual workers based on the pictures, duplicates the postures, and calculates the lower back compression and body balance of the virtual workers.
The GS-ML-MSD2F methodology is a research-based strategy for building data and preparing management capabilities. As a result, this research examines the most productive frameworks for the building sector and features numerous innovative system studies in the field of machine learning. In light of these challenges, the suggested model GS-ML-MSD2F emerged as the most advantageous alternative to the pre-existing DER-MI, EWT, S/G- iKT, ISE, and ACHC models.
4. Results and Discussion
The sample population consists of 250 female and 250 male rebar workers with a minimum of six months of experience, selected using a simple random selection process. Face-to-face questioning and ergonomic assessments were performed in January and June of 2023. Several machine learning techniques were applied to the data, and the results were compared and contrasted.
The vast majority of IR is interested in studies that compare the work of men and women or that detail the experiences of women and men in the workplace. A greater emphasis on women’s complex and often difficult work in jobs that seem easy (such as semiskilled trades, hairstyling, cleaning, wrapping, and production line work) and recognition that women are impacted at least as much as men by work-related injuries and illnesses were the two main changes found in this impact category.
Dataset Description: This study aims to assess the frequency of musculoskeletal diseases (MSDs) and the variables contributing to their development among office workers engaged in activity-based work (ABW). Methods: For the study [26], 42 ABW and 68 control office workers participated. When comparing the ABW group to the control group, we did not find statistically significant changes in the incidence of MSDs across major body parts. When comparing the two groups during the previous six months, the ABW group reported considerably higher pain in the right wrist, hand, and finger (p < 0.05) than the control group. The ABW group showed a considerable increase in work-related physical activity and time spent standing each day (p < 0.05). All other pain-related variables showed no statistically significant differences.
Table 1 above provides a comparison and contrast of dataset approaches from a number of disciplines, focusing on performance. All the current approaches, including DER-MI, EWT, S/G-iKT, ISE, ACHC, and the projected GS-ML-MSD2F, are given, along with the total number of workers. The overall percentage is greater for the proposed model, at 99.34%.
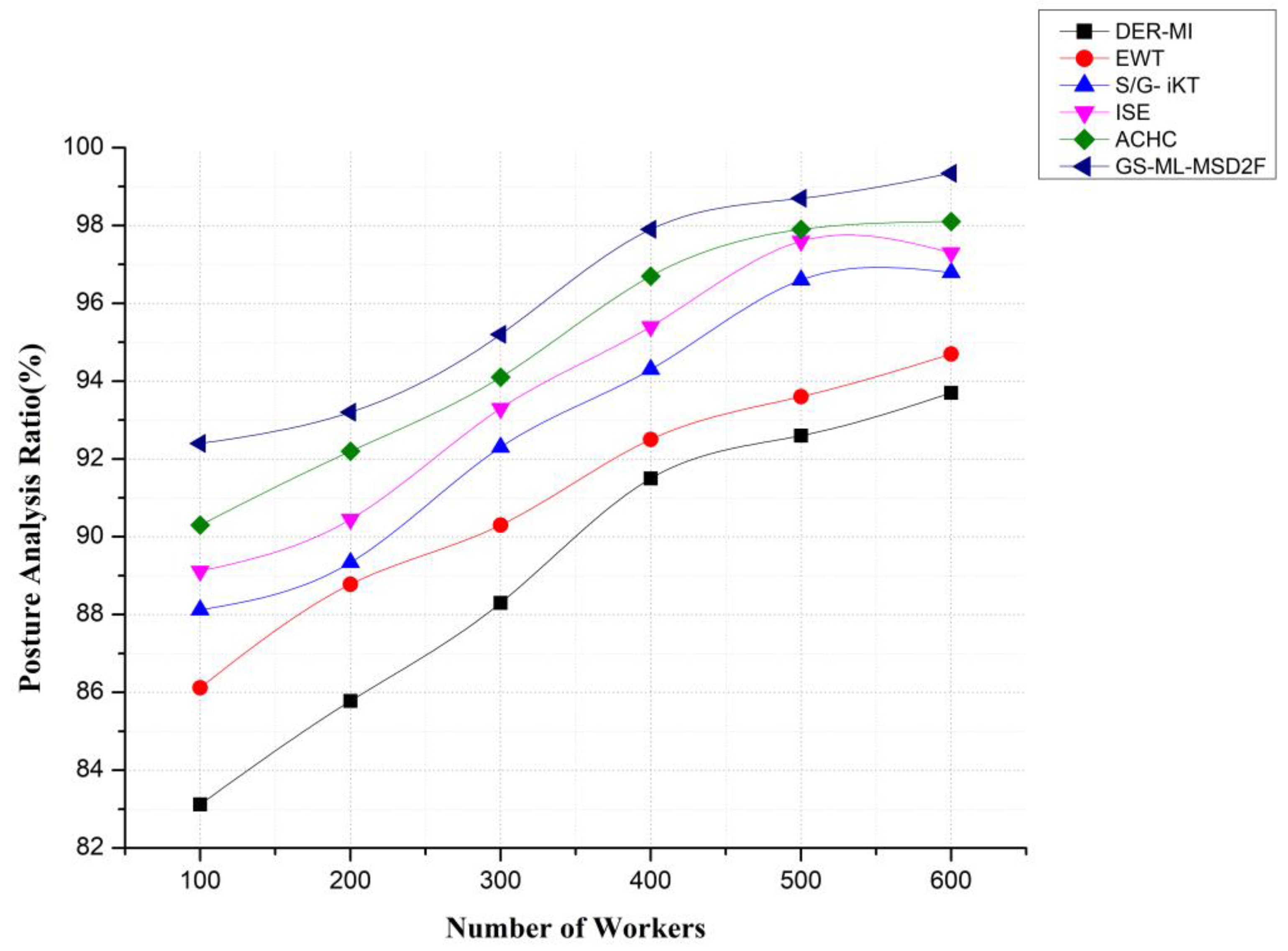
4.1. Posture Analysis
Figure 6 depicts the steps involved in the posture detection process. The number of workers (represented by the X axis) is shown against the posture detection factor (represented by the Y axis). Postural evaluation involves visual and tactile identification of paired anatomic landmarks for symmetry and static postural alignment. The patient must remain steady, with their face to the front, feet shoulder-width apart, and arms relaxed to the sides. Weak back and abdominal muscles, extended sitting, or poor workplace ergonomics may cause this posture. Slouching may cause neck, back, and shoulder pain by compressing spinal discs. These data are useful for enhancing posture detection. GS-ML-MSD2F is the best model for assessing and forecasting tracking. As a result, posture detection outperforms alternative models.
4.2. Musculoskeletal Disorder Analysis
Figure 7 depicts the process of detecting musculoskeletal abnormalities. The number of workers is plotted along the X axis, while musculoskeletal detection is shown along the Y axis. It is reasonable to treat men and women equally when they have equivalent orthopedic injuries. However, some musculoskeletal ailments disproportionately affect women or are otherwise exclusive to women. As part of a comprehensive musculoskeletal evaluation, measuring the patient’s strength, range of motion (both active and passive), and any signs of inflammation, pain, or edema in the joints is important. One of the initial signs of osteomyelitis might be pseudoparalysis, irritability, or discomfort while palpating a bone. This information can be used to improve musculoskeletal disorder detection. When evaluating and making predictions about tracking, GS-ML-MSD2F is the most effective model. This means that musculoskeletal detection is superior to the other methods.
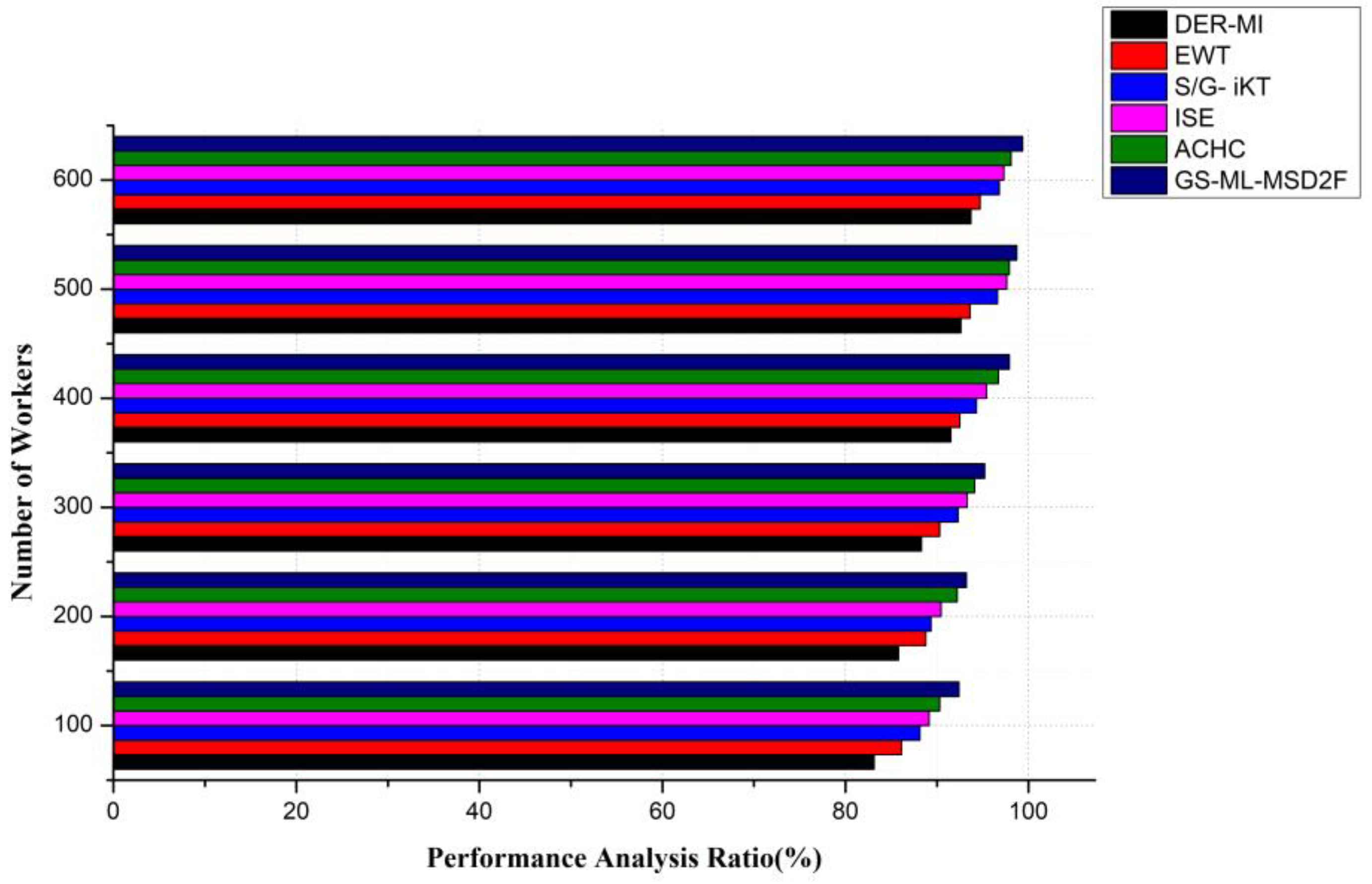
4.3. Performance Analysis
The performance analysis procedure is shown in Figure 8. Employee count (Y-axis) and productivity (X-axis) are displayed against one another. Range of motion (looking at the joint on its own, its limitations, and any hypo- or hypermobility it may have), reflex and sensory function (examining dermatomes, reflexes, and sensory function to find potential issues), and strength testing are the main components of a proper evaluation. When evaluating the musculoskeletal system, it is necessary to gather information on the patient’s mobility and their body’s structure and motion. A registered nurse will perform a musculoskeletal system physical exam regularly to check for anomalies and evaluate the patient’s function. We can utilize these data to boost performance. GS-ML-MSD2F is the best model for assessing data and producing predictions. Therefore, GS-ML-MSD2F is preferable to other approaches.
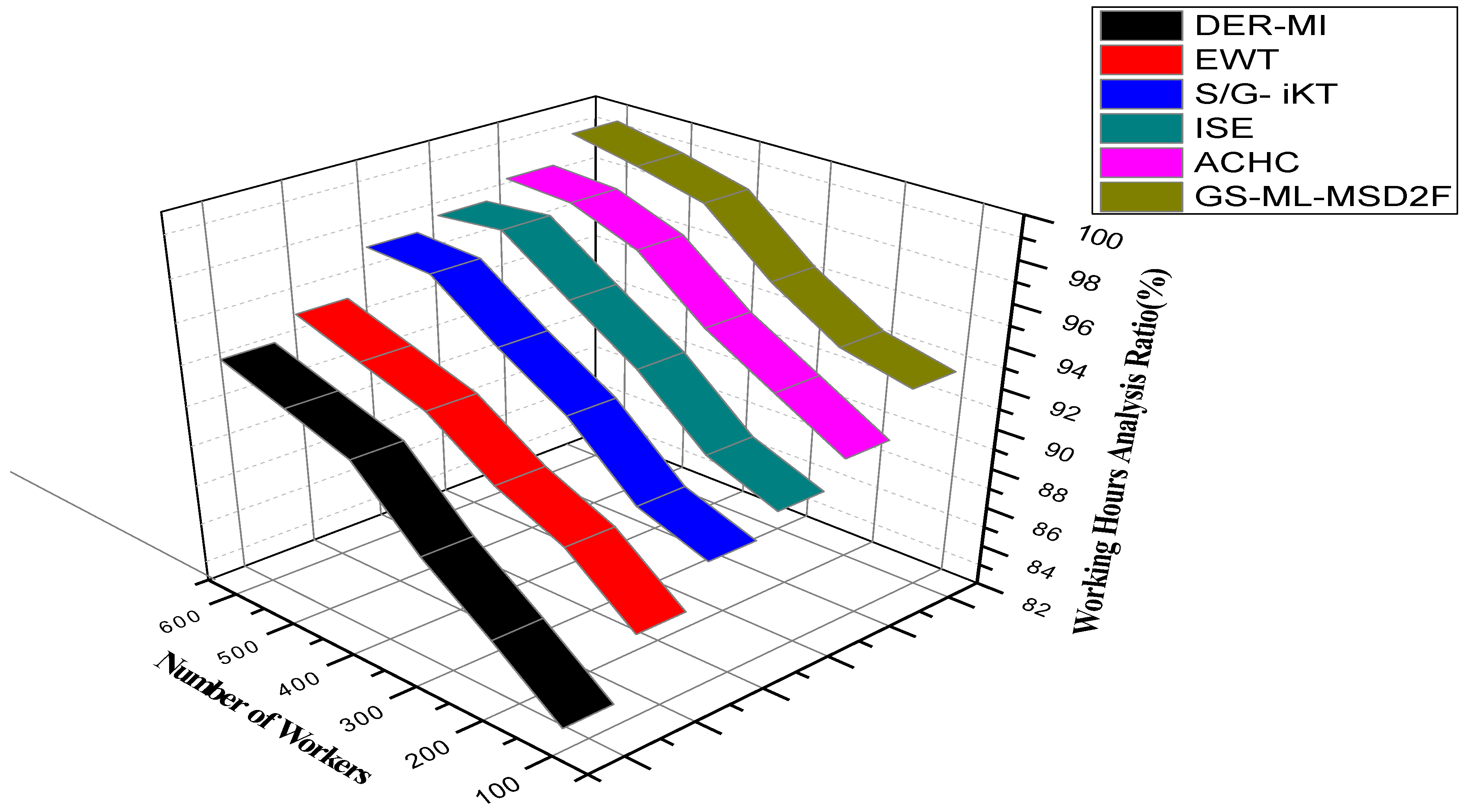
4.4. Working Hours Analysis
Figure 9 depicts the steps of the working hours analysis. The number of employees (X-axis) and the number of hours they put in every week (Y-axis) are plotted side by side. This information will help us improve our efficiency. The most effective model for evaluating data and making predictions is GS-ML-MSD2F. This is why GS-ML-MSD2F is superior to alternative methods. Despite the IR’s best intentions, female workers were unwilling to engage in studies conducted in mixed settings where men made up the majority. The researchers attributed this pushback to women’s concerns that their performance in the workplace would be unfairly judged based on the study’s findings.
4.5. Stress Analysis
Figure 10 depicts the steps of the stress-testing technique. The number of employees is shown along the X axis and the types of stress are shown along the Y axis. Muscles constrict in stress response, which in turn reduces blood flow. The musculoskeletal system becomes more permanently contracted when you experience persistent stress. Chronic pain, such as back and neck pain, and ancillary conditions like migraine may develop through repeated tensing of the same muscles over an extended period. Muscles contract in response to emotional or physical strain. Muscle tension is the body’s defense mechanism against pain and damage, and it happens almost automatically in response to stress. A person’s muscles tighten up all at once in response to stress that comes on suddenly, and then they relax after the stress goes away. The information gathered could be valuable in the long run. When comparing the regulated stress analysis projections to other models, GS-ML-MSD2F fares exceptionally well.
Detection of stress and other parameters, technical performance, etc., are all measured against competing models. The GS-ML-MSD2F model is proposed, and all current models are compared to it. High detection, high performance, and high-stress analysis and posture analysis were all obtained using GS-ML-MSD2F, as suggested by the findings.
5. Conclusions
Construction workers make up a disproportionate share of the illness burden due to MSDs, which restrict everyday activities, negatively impact mental and physical health, and decrease overall well-being. This investigation established several important things: (1) workers’ lower backs were the most often afflicted area, and WMSDs were widespread among workers within a year. Afterward, the regions of the shoulder, neck, upper back, hand/wrist, knee, ankle/foot, elbow, and hip/thigh were examined. The results showed that (1) the WMSDs were associated with the participants’ demographics, job locations, and length of employment. Additionally, MSDs had an impact on both work responsibilities and normal activities. These results highlight the need for WMSD preventive and education initiatives in India. Reducing the incidence of these injuries may be possible with the help of treatment and preventative programs that are both readily available and provide early access. Finding, ranking, and weighing solutions that may assist female construction workers in overcoming gender-specific difficulties was the primary goal of this research. The researchers hope that by shedding light on the unique experiences of women in the construction industry, policymakers and managers will be better able to create welcoming workplaces where all employees, including women, can thrive and advance in their careers. The significant incidence of WMSDs among office workers has to be addressed via appropriate screening and interventions, as our data demonstrate. Workers of a certain age, gender, and level of experience and with certain shift lengths should be given extra care since they are more likely to suffer from these conditions. To manage WMSDs, it is crucial to observe each worker regularly. This is not dependent on their knowledge of these illnesses or any potential contemporary office settings; rather, it allows for detecting and reducing risk factors. Since office workers’ ergonomics training may not be enough to prevent WMSDs, we propose instituting policies to enhance workers’ health and provide them with optimum workstation components that should be customized for each individual and maintained regularly. To effectively prevent WMSDs, workers should take an active role in implementing and maintaining these safeguards. Most people who experience stress report feeling more frustrated, exhausted, stressed in their relationships (both personal and professional), and angry or irritable. All of these problems may be traced back to the stressful conditions inherent in building projects, such as tight deadlines, high levels of complexity, rivalry among workers, the necessity of working together, and an unbalanced work–life schedule.
Author Contributions
Conceptualization, S.K.P. and K.M.; methodology, S.K.P. and K.M.; software, validation, formal analysis, investigation, and resources, S.K.P. and K.M; data curation, writing—original draft preparation, and writing—review and editing, B.P.; visualization, supervision, project and administration, S.K.P., K.M. and B.P.; funding acquisition, B.P. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Data Availability Statement
The raw data supporting the conclusions of this article will be made available by the authors on request.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Hasan, A.; Kamardeen, I. Occupational health and safety barriers for gender diversity in the Australian construction industry. J. Constr. Eng. Manag. 2022, 148, 04022100. [Google Scholar] [CrossRef]
- Karthick, S.; Kermanshachi, S.; Pamidimukkala, A.; Namian, M. A review of construction workforce health challenges and strategies in extreme weather conditions. Int. J. Occup. Saf. Ergon. 2023, 29, 773–784. [Google Scholar] [CrossRef] [PubMed]
- Sang, K.; Calvard, T.; Remnant, J. Disability and academic careers: Using the social relational model to reveal the role of human resource management practices in creating disability. Work Employ. Soc. 2022, 36, 722–740. [Google Scholar] [CrossRef]
- Sarac, B.N. Exploring the Representation of Gender-Based Violence Against Yazidi Women. Ph.D. Thesis, University of Portsmouth, Portsmouth, UK, 2022. [Google Scholar]
- Marcos-Marcos, J.; Mateos, J.T.; Gasch-Gallén, À.; Álvarez-Dardet, C. Men’s health across the life course: A gender relational (critical) overview. J. Gend. Stud. 2021, 30, 772–785. [Google Scholar] [CrossRef]
- Cameron, A.; Tedds, L.M. Gender-Based Violence, Economic Security, and the Potential of Basic Income: A Discussion Paper. Available online: https://mpra.ub.uni-muenchen.de/107478/1/MPRA_paper_107478.pdf (accessed on 30 April 2021).
- Forssberg, K.S.; Vänje, A.; Parding, K. Bringing in gender perspectives on systematic occupational safety and health management. Saf. Sci. 2022, 152, 105776. [Google Scholar] [CrossRef]
- Eichler, M. Making military and Veteran women (in)visible: The continuity of gendered experiences in military-to-civilian transition. J. Mil. Veteran Fam. Health 2022, 8, 36–45. [Google Scholar] [CrossRef]
- Thiojaya, J.; Qomariyah, N.N. Classification of Human Gender through Machine Learning Analysis of Gait. In Proceedings of the 2023 International Seminar on Intelligent Technology and Its Applications (ISITIA), Surabaya, Indonesia, 26–27 July 2023; IEEE: Washington, DC, USA, 2023; pp. 382–387. [Google Scholar]
- Hiramatsu, A. Female taxi drivers in Mexico City: Facing patriarchal structures as a force of oppression. Gend. Work. Organ. 2022, 29, 1638–1657. [Google Scholar]
- Lilja, I. Unseen Victims: Why Refugee Women Victims of Gender-Based Violence Do Not Receive Assistance in the EU; European Institute for Crime Prevention and Control: Helsinki, Finland, 2020. [Google Scholar]
- Aparicio Martín, E. Proposal of intervention promoted by the government delegation of spain for gender based violence. Analysis of a referent document for professionals. Revista de Comunicación de la SEECI 2020, 51, 63–82. [Google Scholar] [CrossRef]
- Laberge, M.; Chadoin, M.; Inigo, M.; Messing, K.; Lefrançois, M.; Sultan-Taïeb, H.; Chatigny, C.; Riel, J.; Webb, J.; Fillion, M.; et al. Integration of sex and gender in interventions by students in ergonomics. Ergonomics 2022, 65, 1578–1591. [Google Scholar] [CrossRef] [PubMed]
- Bosomworth, J.; Khan, Z. Analysis of Gender-Based Inequality in Cardiovascular Health: An Umbrella Review. Cureus 2023, 15, e43482. [Google Scholar] [CrossRef] [PubMed]
- Carè, A. Gender imbalance in medical imaging datasets for Artificial Intelligence. In Proceedings of the Igmcongress 2022 10th Congress of the International Society of Gender Medicine, Padua, Italy, 16–17 September 2022. [Google Scholar]
- Muruzi, Y.L.; Gutura, P. Gender-Based Violence and Women with Physical Disabilities in South Africa: A Forgotten Cohort at Risk. Gend. Behav. 2022, 20, 19367–19375. [Google Scholar]
- van den Hurk, L.; Hiltner, S.; Oertelt-Prigione, S. Operationalization and Reporting Practices in Manuscripts Addressing Gender Differences in Biomedical Research: A Cross-Sectional Bibliographical Study. Int. J. Environ. Res. Public Health 2022, 19, 14299. [Google Scholar] [CrossRef] [PubMed]
- Gaudet, S.; Marchand, I.; Bujaki, M.; Bourgeault, I.L. Women and gender equity in academia through the conceptual lens of care. J. Gend. Stud. 2022, 31, 74–86. [Google Scholar] [CrossRef]
- Slade, T.; Gross, D.P.; Niwa, L.; McKillop, A.B.; Guptill, C. Sex and gender demographic questions: Improving methodological quality, inclusivity, and ethical administration. Int. J. Soc. Res. Methodol. 2021, 24, 727–738. [Google Scholar] [CrossRef]
- RamPrakash, R.; Lingam, L. Why is women’s utilization of a publicly funded health insurance low?: A qualitative study in Tamil Nadu, India. BMC Public Health 2021, 21, 350. [Google Scholar] [CrossRef] [PubMed]
- Habib, R.R.; Ziadee, M.; Abi Younes, E.; Harastani, H. Syrian refugee child workers: Gender differences in ergonomic exposures and musculoskeletal health. Appl. Ergon. 2020, 83, 102983. [Google Scholar] [CrossRef] [PubMed]
- Messing, K.; Lefrançois, M.; Saint-Charles, J. Observing Inequality: Can Ergonomic Observations Help Interventions Transform the Role of Gender in Work Activity? Comput. Support. Coop. Work (CSCW) 2021, 30, 215–249. [Google Scholar] [CrossRef]
- Laberge, M.; Blanchette-Luong, V.; Blanchard, A.; Sultan-Taïeb, H.; Riel, J.; Lederer, V.; Saint-Charles, J.; Chatigny, C.; Lefrançois, M.; Webb, J.; et al. Impacts of considering sex and gender during intervention studies in occupational health: Researchers’ perspectives. Appl. Ergon. 2020, 82, 102960. [Google Scholar] [CrossRef] [PubMed]
- Bowen, P.; Peihua Zhang, R.; Edwards, P. An investigation of work-related strain effects and coping mechanisms among South African construction professionals. Constr. Manag. Econ. 2021, 39, 298–322. [Google Scholar] [CrossRef]
- Sahoo, H.; Govil, D.; James, K.S.; Prasad, R.D. Health issues, health care utilization and health care expenditure among elderly in India: Thematic review of literature. Aging Health Res. 2021, 1, 100012. [Google Scholar] [CrossRef]
- Musculoskeletal Disorders and Associated Factors among Office Workers in an Activity-Based Work Environment. Available online: https://datasetsearch.research.google.com/search?src=0&query=Musculoskeletal%20Disorders%20in%20%20workers&docid=L2cvMTFsY193a3FxZg%3D%3D (accessed on 3 April 2024).
Figure 4.
Methodology for analysis frameworks.

Figure 5.
Research approach.

Figure 6.
Posture analysis.

Figure 7.
Musculoskeletal analysis.

Figure 8.
Performance analysis.

Figure 9.
Working hours analysis.

Figure 10.
Stress analysis.


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Table 1.
Performance comparison of different methods.
| No. of Workers | DER-MI | EWT | S/G- iKT | ISE | ACHC | GS-ML-MSD2F |
|---|---|---|---|---|---|---|
| 100 | 83.12 | 86.12 | 88.12 | 89.12 | 90.3 | 92.4 |
| 200 | 85.78 | 88.78 | 89.34 | 90.45 | 92.2 | 93.2 |
| 300 | 88.3 | 90.3 | 92.3 | 93.3 | 94.1 | 95.2 |
| 400 | 91.5 | 92.5 | 94.3 | 95.4 | 96.7 | 97.9 |
| 500 | 92.6 | 93.6 | 96.6 | 97.6 | 97.9 | 98.7 |
| 600 | 93.7 | 94.7 | 96.79 | 97.3 | 98.1 | 99.34 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Paramasivam, S.K.; Mani, K.; Paneerselvam, B. Unveiling Gender-Based Musculoskeletal Disorders in the Construction Industry: A Comprehensive Analysis. Buildings 2024, 14, 1169. https://doi.org/10.3390/buildings14041169
AMA Style
Paramasivam SK, Mani K, Paneerselvam B. Unveiling Gender-Based Musculoskeletal Disorders in the Construction Industry: A Comprehensive Analysis. Buildings. 2024; 14(4):1169. https://doi.org/10.3390/buildings14041169
Chicago/Turabian StyleParamasivam, Suresh Kumar, Kanitha Mani, and Balamurugan Paneerselvam. 2024. "Unveiling Gender-Based Musculoskeletal Disorders in the Construction Industry: A Comprehensive Analysis" Buildings 14, no. 4: 1169. https://doi.org/10.3390/buildings14041169
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.