1. Introduction
The lung epithelium forms the first line of defence against inhaled pathogens and, through regulation of epithelial barrier functions, it is a key player in maintaining tissue homeostasis [
1]. Key components in anti-microbial defence are secreted by bronchial epithelial cells (BECs) into the mucus layer and include defensins, nitric oxide (NO), and reactive oxygen species (ROS) [
2]. The mucus layer itself is mainly composed of hydrated mucins that provide viscosity and enables entrapment of bacteria, which are transported out of the lungs to the hypopharynx via the action of ciliated epithelial cells within the mucociliary escalator. In the healthy lung, commensal bacteria are adapted to these epithelial defence mechanisms and a stable microflora can develop without causing any inflammation. However, some pathogenic bacteria can overcome the anti-microbial defence mechanisms of the epithelium and cause symptomatic infections [
3].
Francisella tularensis is a Gram-negative, pleomorphic, aerobic coccobacillus and is the causative agent of the disease tularaemia. Tularaemia is endemic in Scandinavia and North America with 30%–60% mortality following exposure to the most pathogenic strains, if left untreated [
4]. Symptoms of pneumonic tularaemia include coughing, chest pains, and difficulty breathing. Aerosolised
F. tularensis is the most likely candidate for use as a bioweapon [
5]. With as few as 10 colony-forming units able to cause serious disease [
4] this bacterium is placed on the Center for Disease Control and Prevention (CDC) Category A list of agents that pose a risk to national security and, as such, is handled at Advisory Committee on Dangerous Pathogens (ACDP) Level 3 [
6]. An attenuated subspecies known as
F. tularensis subsp.
holarctica Live Vaccine Strain (LVS) is often used to enable higher throughput studies at ACDP Level 2 and shares many characteristics with more virulent strains [
7].
Burkholderia pseudomallei is endemic in Thailand and Australia and causes melioidosis with non-specific symptoms leading to septic shock and high mortality rates if left untreated [
8,
9]. Meliodosis results from an acute or latent infection with the longest recorded period of latency some 62 years [
10]. Therapeutic options for melioidosis are limited with no licensed vaccine and antibiotics being required for many months. For
Burkholderia pseudomallei the ACDP2 model organism
Burkholderia thailandensis has a reduced virulence (~10
5 fold) [
11] but is genetically similar to
B. pseudomallei sharing 95% 16S rRNA similarity and virulence factor homologues [
12]. By using these less virulent strains and by understanding their limitations it is possible to conduct mechanistic studies without the restrictions of working to ACDP3. Both tularaemia and melioidosis are most severe after exposure by the inhalation route and as such their interaction with the lung epithelium remains an important area of study.
The majority of experimental studies investigating respiratory infections are performed in animals, mainly mice. Animal models have several shortfalls and the translation of findings into the human situation can be difficult. As an alternative to animal models in respiratory research, human cell-based ex vivo and in vitro models have been developed [
13]. However, there are only a limited number of studies published that use human in vitro models to investigate epithelial-bacterial interactions. A variety of human lung epithelial cell lines are used in respiratory research, but only a few are able to express tight junction complexes under certain culture conditions which are an essential part of the physical barrier of the epithelial sheet. Tight junctions also maintain the polarity of the epithelium and distinguish between the lumen-facing apical, and the ‘tissue-facing’ basolateral compartment.
Despite their advantages, cell line models of the polarised airway epithelium have some limitations as they do not express all components of the epithelial barrier functions observed in vivo, such as ciliated cells and mucus-producing goblet cells. An in vitro model that recapitulates the in vivo situation more closely utilises human primary bronchial epithelial cells (PBECs) which can be differentiated to form a pseudostratified mucociliary epithelium when grown at the air-liquid interface on semi-permeable membrane supports. While these in vitro cultures are expensive to maintain, and results can be variable due to the phenotypic differences of the donors, they are invaluable for determination of the response of the human airway epithelial barrier to infection. Furthermore, such in vitro models allow higher throughput preliminary evaluation of therapeutics, making them ideal for early drug discovery.
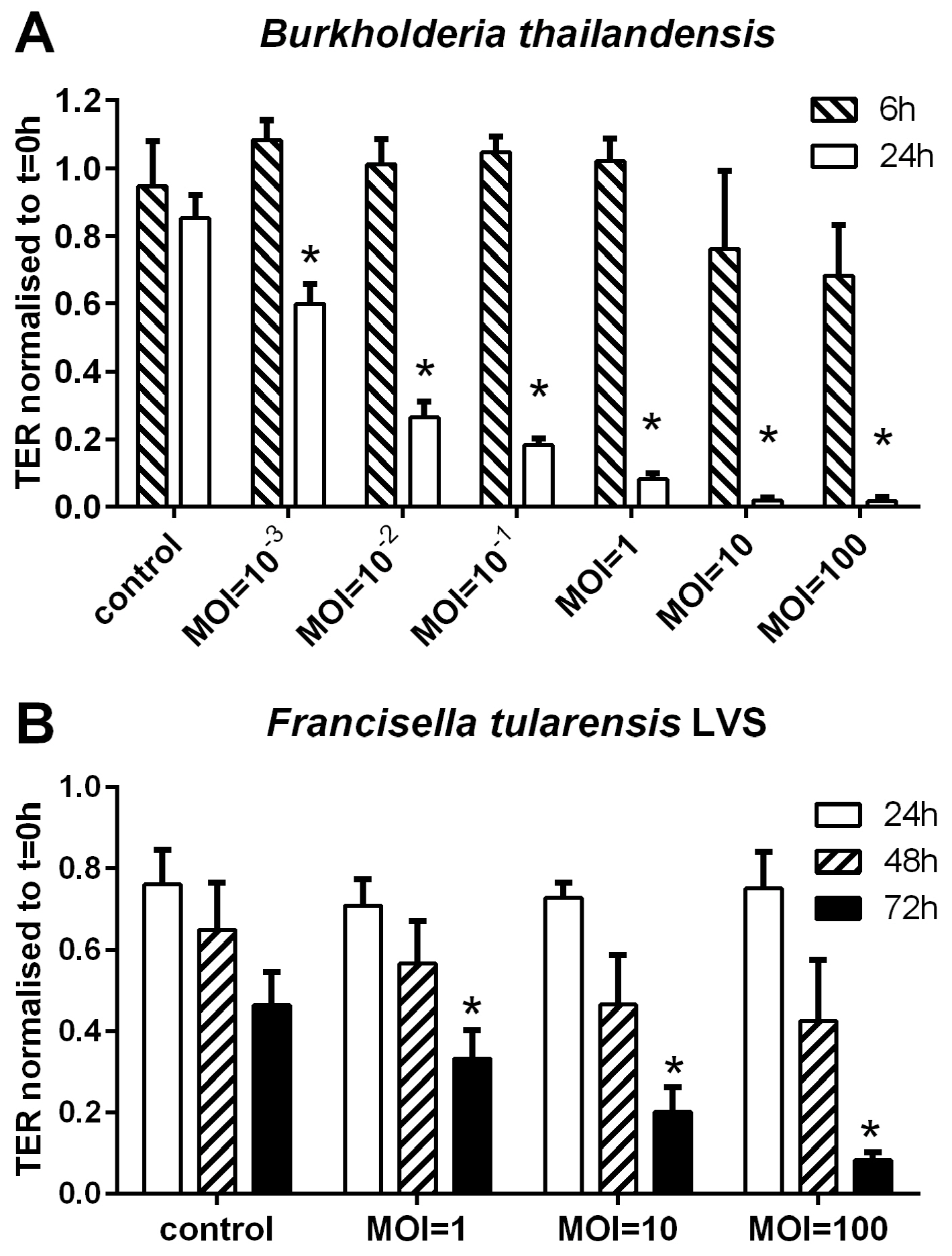
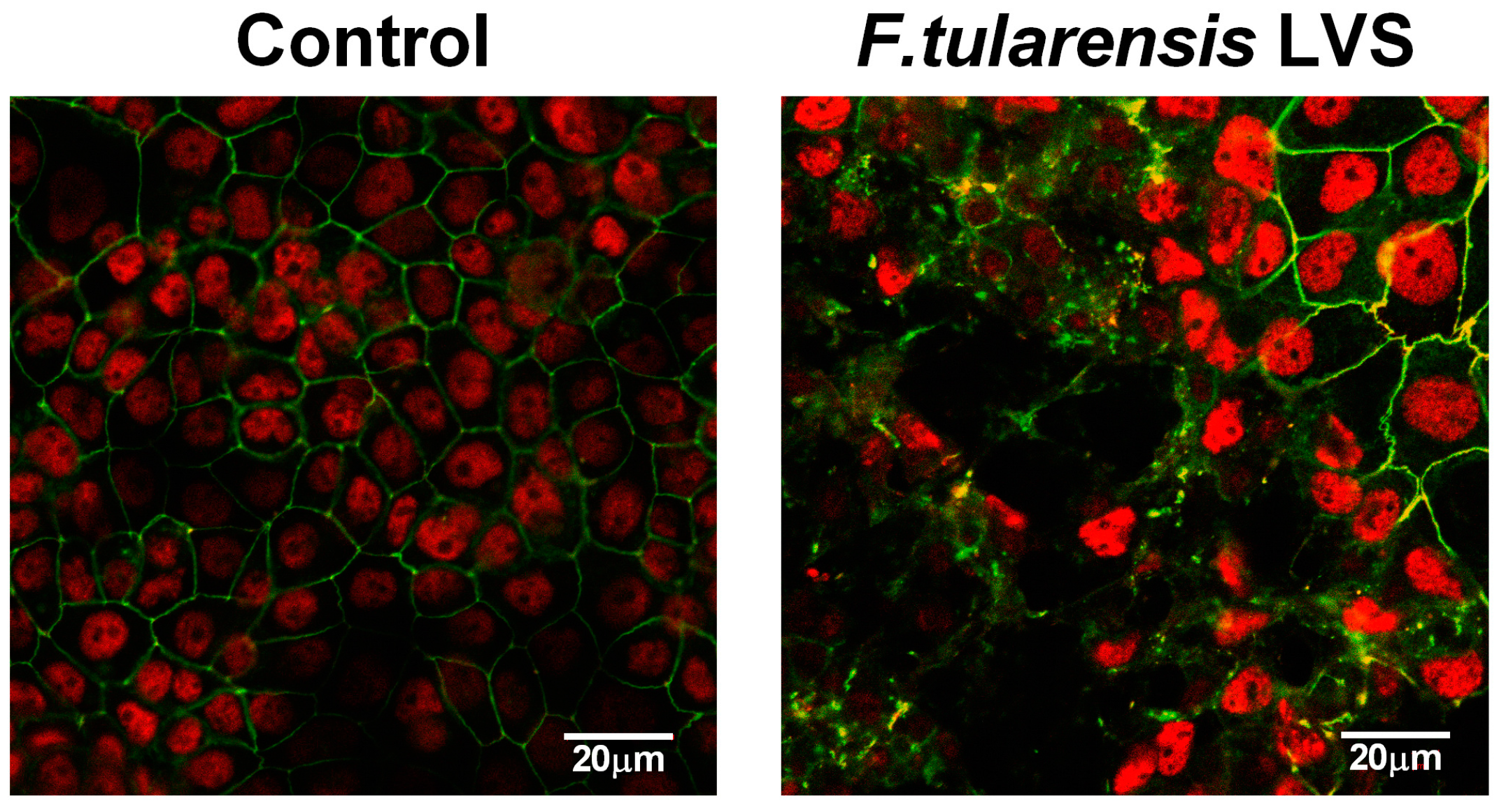
The aim of this study was to analyse the effect of B. thailandensis and F. tularensis LVS infection on airway epithelial barrier properties. We show that B. thailandensis and F. tularensis both disrupt the physical barrier resulting in their passage from the apical to the basolateral epithelial surface and activation of the immunological barrier with induction of TNF-α release. We confirm these findings utilising fully-differentiated primary epithelial cells exposed to B. thailandensis. Additionally, we demonstrate the use of this model to identify novel therapeutic candidates for the treatment of respiratory pathogens.
3. Discussion
In this study we demonstrate that the polarised cell line 16HBE14o- is a useful in vitro model of the airway epithelium for studying the effect of B. thailandensis and the slower growing F. tularensis on epithelial barrier functions. Both bacteria are able to diminish the physical barrier properties, although in these models the airway epithelium is more susceptible to B. thailandensis than to F. tularensis LVS. The passage of bacteria across the epithelial barrier is linked to the breakdown of the physical barrier. Both bacterial strains induce a proinflammatory response with the induction of TNF-α release in a MOI-dependent manner. Furthermore, the activation of the airway epithelial barrier functions induced by B. thailandensis infection are reduced by the corticosteroid fluticasone propionate resulting in improved physical barrier properties, reduced bacterial passage, and decreased release of TNF-α.
The interaction of different genera of bacteria with the airway epithelium has been analysed previously using in vitro cell culture or animal models [
17]. In the lung, epithelial cells are the first line of defence and express a variety of pathogen recognition receptors (PRRs) including toll-like receptors (TLRs) [
18,
19]. Important PRRs for bacterial cell wall components, like lipopeptides or lipopolysaccharides (LPS), are TLR2 and 4. Binding of bacterial products to TLR2 or 4 results in downstream activation of NF-κB and p38 mitogen-activated protein kinase (MAPK) signalling pathways [
18,
20], which are involved in the regulation of the physical but also the immunological barrier functions of airway epithelial cells. Interestingly, it has been shown that
Burkholderia cenocepacia activates an inflammatory response in airway epithelial cells via TLR5 independent of TLR2/4 signalling [
21]. Additionally, a breakdown of the physical barrier can be mediated independently of PPR signalling by the release of bacterial virulence factors; for example, type III toxins of
Pseudomonas aeruginosa interfering with cytoskeletal organisation [
22] or hemolysin A, a pore-forming protein, released by
Staphylococcus aureus [
23].
Frequently, a breakdown of the epithelial physical barrier is correlated with an increase in paracellular permeability of macromolecules, as well as particles, including the transmigration of bacteria into the interstitium. An increased passage of bacteria across the airway epithelial sheet has been shown previously using in vitro models with various bacterial strains. For example, infection of polarised 16HBE cells with
Staphylococcus aureus increased the passage across the epithelial layer, a process that is thought to be mediated by the bacterial surface protein A [
24]. The type III toxins of
Pseudomonas aeruginosa are also associated with increase bacterial passage across the epithelium [
22]. Other bacterial virulence factors like rhamnolipids released by
P. aeruginosa interfere with the physical barrier properties of the airway epithelium and enhance the invasion of bacteria across the epithelial barrier [
25]. Furthermore, bacterial activation of TLR2, p38 MAPK, and TGF-β signalling pathways are involved in the bacteria-induced barrier disruption and increased passage of bacteria across the epithelial layer [
20]. In contrast, studies using gut epithelial models, suggest that commensal and probiotic bacteria have protective effects on epithelial barrier function [
26] indicating that comparative work on airway commensals would be of interest.
An important role of the airway epithelium in response to bacterial infections is the induction of inflammation, which is mediated by the release of inflammatory mediators. Airway epithelial cells are able to release a variety of pro- and anti-inflammatory mediators [
1] orchestrating the infiltration and activation of immune cells in the airway mucosa. Important immune cells required for bacterial clearance are macrophages and neutrophils, which are attracted and activated to sites of infection by IL-8, IL-6, and TNF-α [
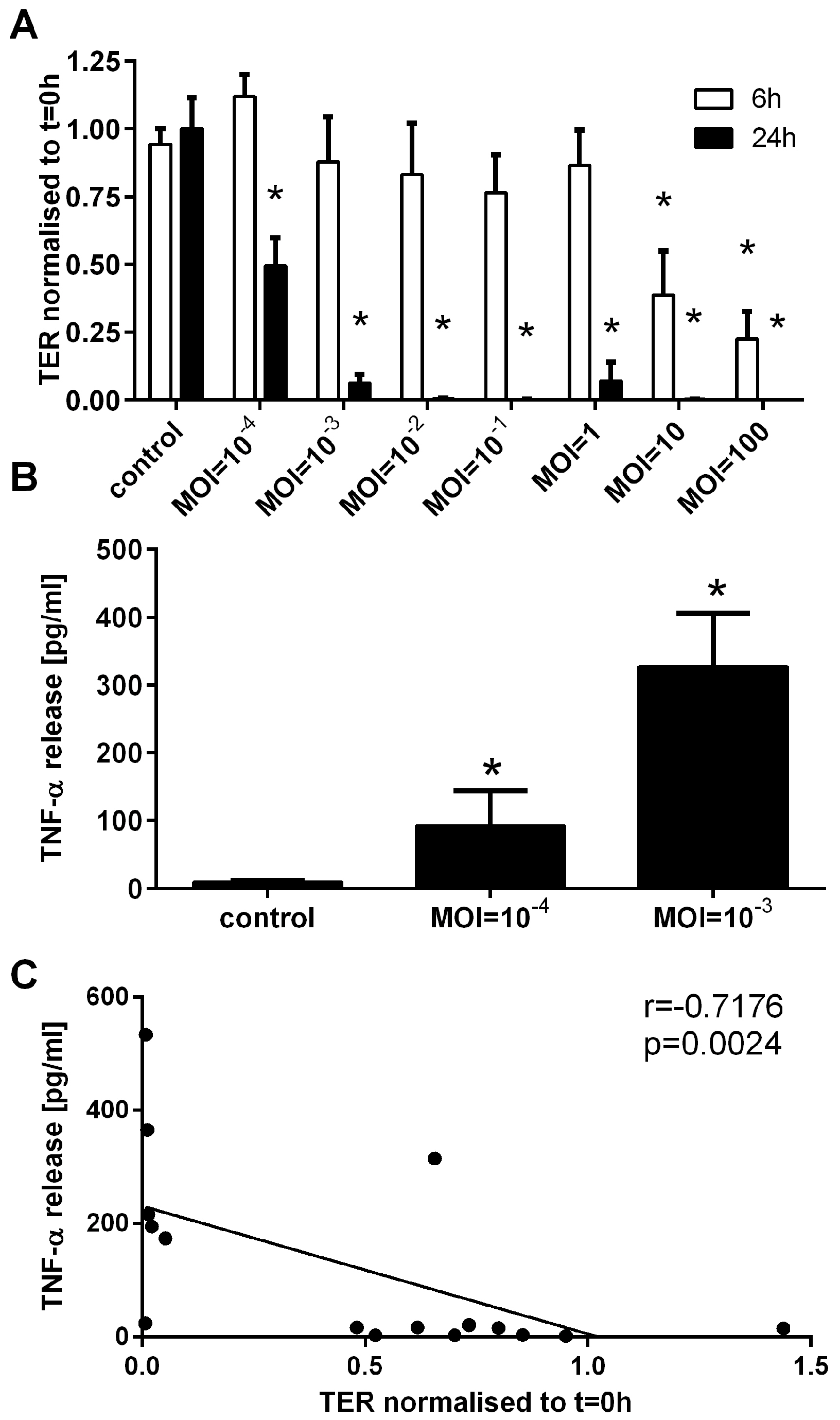
27]. Here we show that
B. thailandensis and
F. tularensis both induce the release of TNF-α by airway epithelial cells, which can activate an inflammatory response.
In the airway mucosa at sites of bacterial infection, infiltrating activated immune cells release a variety of anti-microbial molecules, including ROS and NO. However, excessive inflammation can result in tissue damage and facilitate systemic infection. Therefore, regulating excessive airway inflammation and a breakdown of the physical barrier properties during bacterial infections is one of the most promising therapeutic strategies despite the use of antibiotics. In this study we investigated the effect of corticosteroids and anti-TNF-α therapy on the physical and immunological barrier properties of airway epithelial cells. TNF-α has been shown to mediate a disruption of the physical barrier of airway epithelial cells [
14], which might increase the passage of bacteria across the epithelial barrier and contribute to systemic infection. The breakdown of the physical barrier properties of the airway epithelium during bacterial infection was reduced by administrating a TNF-α binding drug leading to a decrease in bacterial passage across the epithelium. Administration of anti-TNF-α drugs during bacterial airway infections might help reduce the risk of systemic infections.
The corticosteroid fluticasone propionate improved the physical barrier properties, decreased the passage of bacteria across the epithelium, and reduced the release of inflammatory mediator by the airway epithelium during bacterial infection. Corticosteroids have previously been shown to improve the physical barrier properties of airway epithelial cells [
15]; however, their effect on bacterial passage across the airway epithelium during bacterial infections has not been analysed. Additionally, the effects of corticosteroids on airway epithelial functions involved in innate and adaptive immunity are well known [
28]. Our data showing reduced release of TNF-α during
B. thailandensis infection by corticosteroid treatments are in line with previously published data for other respiratory pathogens. In these prior studies using an airway epithelial cell line in monolayer culture, it has been shown that fluticasone propionate inhibits
S. aureus-induced IL-8, IL-6, and TNF-α expression in airway epithelial cells by reducing AP-1 and NF-κB signalling [
29].
Reduction of the inflammatory response of airway epithelial cells during bacterial infections has the potential to prevent excessive inflammation in the airways that can ultimately cause severe tissue damage, septicaemia, and lung failure. Here we demonstrate the use of human epithelial cell models in order to evaluate putative therapeutics that aid in the maintenance of lung barrier function during the course of an infection. The administration of corticosteroids or anti-TNF-α drugs represent potential therapeutic strategies that maintain the physical barrier functions of the lung and reduce the risk of excessive inflammation during lung infections with pathogenic bacteria, such as B. thailandensis.
4. Experimental Section
4.1. Cell Culture
The human bronchial epithelial cell line 16HBE14o- (16HBE; a gift from Prof. D.C. Gruenert, San Francisco, CA, USA) and differentiated primary human bronchial epithelial cells (PBECs) were used in this study. 16HBE cells were maintained in minimum essential medium (MEM) with Glutamax and supplemented with 10% foetal bovine serum and penicillin/streptomycin (Life technologies, Paisley, UK) on PureCol collagen I (Advanced BioMatrix, San Diego, CA, USA) coated culture flasks. Experiments were carried out using collagen-coated Transwell® permeable supports (diameter 6.5 mm, polyester membrane with 3 µm pores, Corning Life Sciences, Amsterdam, The Netherlands). Cells were seeded at a density of 1.5 × 105 cells in 200 µL growth medium; the basolateral compartment contained 500 µL of the same medium. Medium exchange was carried out every 2–3 days. 16HBE cells formed a polarised epithelial sheet within seven days of culture, as monitored by measuring the transepithelial resistance (TER) using an EVOM voltohmmeter (World Precision Instruments, Hitchin, UK). Cells with a TER <330 Ω·cm2 on day 7 were used for experiments.
Differentiation of human PBECs at the air-liquid interface (ALI) was performed as previously described [
30]. Briefly, PBECs were obtained by epithelial brushings using fiber optic bronchoscopy from healthy subjects selected from a volunteer database. All procedures were approved by the Southampton and South West Hampshire Research Ethics Committee and were undertaken following informed consent. PBECs were cultured in bronchial epithelial growth medium (BEGM; Lonza, Basel, Switzerland). At passage 2, cells were cultured on collagen coated Transwell
® permeable supports (diameter 6.5 mm, polyester membrane with 0.4 µm pores, Corning Life Sciences, Amsterdam, The Netherlands) and differentiation was induced by ALI culture for 21 days. TER was monitored weekly and cells with a TER <330 Ω·cm
2 on day 21 were used for experiments.
4.2. Bacterial Culture
B. thailandensis strain E264 [
31] was grown in liquid LB medium at 37 °C, 5% CO
2 under agitation. Bacterial growth was assessed by measuring the optical density at OD
600nm. For determination of live bacteria counts, serial dilutions of the bacterial suspension culture were plated on LB agar plates, incubated for 24 h and the colony-forming unit (CFU) per mL liquid medium calculated.
The live attenuated strain of F. tularensis (LVS) was reconstituted from Pasteurella tularensis Vaccine Batch Lot 4 (National Drug Co., Swiftwater, PA, USA). All stocks and working cultures were handled in accordance with ACDP containment level 2 requirements. Bacteria were resuscitated from frozen stock cultures by overnight growth at 37 °C on BCGA plates. For infection assays spectrophotometric measurements were taken of bacteria resuspended in PBS where an absorbance of 0.2 at 590 nm equated to 1 × 109 cfu/mL. Enumeration of bacteria from all infection experiments were carried out using a logarithmic serial dilution of samples in PBS cultured on BCGA plates in triplicate at 37 °C for 48 h.
4.3. Infection of Airway Epithelial Cells
Cells were cultured in antibiotic free medium 24 h before and throughout the experiments. After measuring the TER (t = 0 h), the apical medium of airway epithelial cells was removed and replaced with 100 µL of bacterial suspension at indicated multiplicity of infection (MOI). Cells were incubated for 60 min at 37 °C and, subsequently, the apical bacterial solution was removed. In experiments performed with polarised 16HBE cells, 200 µL of fresh medium was added to the apical compartment while differentiated PBECs were cultured at the air-liquid interface for the duration of the experiment. The TER was measured after indicated time points. The background TER of an empty transwell (170 Ω) was subtracted and TER data were normalised to the measurements before infection at t = 0 h. After taking apical and basolateral supernatants, bacterial live counts were determined, and the supernatants stored at −20 °C until further analysis.
The effect of the glucocorticoid fluticasone propionate (Sigma Aldrich, Gillingham, UK) and the TNF-α binding drug Enbrel (Wyeth Europa Ltd., Maidenhead, UK) was analysed on airway epithelial barrier functions during bacterial infection. Polarised 16HBE cells were pre-incubated with 10 nM FP or 10 μg/mL Enbrel in the apical and basolateral medium for 60 min prior infection. Apical supernatants were removed and replaced by the B. thailandensis suspension at indicated MOIs without inhibitors. After incubation for 60 min at 37 °C the apical bacterial solution was removed and 200 µL of fresh medium containing inhibitors was added to the apical compartment.
4.4. Confocal Laser Scanning Microscopy
Visualisation of cellular junctions was performed using confocal microscopy. Cells were seeded onto 10 mm diameter glass coverslips (VWR International Ltd., Lutterworth, UK) in 24-well plates. At experimental time-points cells were fixed with 1 mL of 4% w/v paraformaldehyde (Pioneer Research Chemicals, Colchester, UK) before being permeabilised with 0.2% saponin). Cells were quenched with 50 mM ammonium chloride in PBS for ten minutes before being blocked in 0.2% w/v gelatine), 0.02% saponin, 0.02% w/v sodium azide (all Sigma) in PBS (defined as PGAS) overnight at 4 °C. Coverslips were then incubated with 50 μL (10 μg/mL) IgG polyclonal antibodies to the tight junction protein occludin (Life Technologies, Paisley, UK) for 1 h at room temperature, washed three times with 1 mL PGAS and incubated with 50 μL (5 μg/mL) AlexaFluor®488 goat-anti-rabbit polyclonal antibodies (Life Technologies) for a further one hour in the dark at room temperature. After washing three times with 1 mL PGAS coverslips were mounted in UltraCruz mounting media containing DAPI (Santa Cruz Biotechnology Inc., Dallas, TX, USA). Fluorescence was assessed using an Olympus IX70 confocal microscope (Olympus, Hamburg, Germany) fitted with an Olympus Fluoview filter unit and Omnichrome ion laser power pack. All images were observed at 600× magnification and image capture was carried out using FluoView software (Olympus). Occludin stain is shown in green, whereas nuclei are shown in red.
4.5. Release of Inflammatory Mediators
In experiments with B. thailandensis-infected airway epithelial cells the basolateral release of TNF-α was determined by ELISA using a human TNF-α DuoSet ELISA kit (R&D Systems, Abingdon, UK). The release of basolateral TNF-α of airway epithelial cells infected with F. tularensis LVS was analysed using a Cytometric Bead Array (BD Biosciences, Oxford, UK) following the manufacturer’s instructions.
4.6. Statistical Analysis
Statistical evaluation was performed using the software SigmaPlot 12.5. After testing for normality using the Kolmogorov-Smirnov test, related samples were analysed for statistical significance using the paired Student’s t-test or the non-parametric Wilcoxon test. Differences were regarded as significant when p ≤ 0.05.


 ,
, {kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}





