Use of 3D Printing in Model Manufacturing for Minor Surgery Training of General Practitioners in Primary Care


1
Department of Mechanical Engineering, University of Cordoba, Medina Azahara Avenue, Cordoba 14071, Spain. [email protected] (M.C.L.)
2
Primary Care Center of La Carlota, La Paz Avenue, La Carlota, Cordoba 14100, Spain
*
Author to whom correspondence should be addressed.
Appl. Sci. 2019, 9(23), 5212; https://doi.org/10.3390/app9235212
Submission received: 1 November 2019
/
Revised: 28 November 2019
/
Accepted: 28 November 2019
/
Published: 30 November 2019
(This article belongs to the Special Issue Special Issue of the Manufacturing Engineering Society 2019 (SIMES-2019))
Abstract
:Featured Application
The proposed models can be used to train general practitioners in minor surgery courses in primary care centers.
Abstract
In order to increase the efficiency of the Spanish health system, minor surgery programs are currently carried out in primary care centers. This organizational change has led to the need to train many general practitioners (GPs) in this discipline on a practical level. Due to the cost of the existing minor surgery training models in the market, pig’s feet or chicken thighs are used to practice the removal of figured lesions and the suture of wounds. In the present work, the use of 3D printing is proposed, to manufacture models that reproduce in a realistic way the most common lesions in minor surgery practice, and that allow doctors to be trained in an adequate way. Four models with the most common dermal lesions have been designed and manufactured, and then evaluated by a panel of experts. Face validity was demonstrated with four items on a five-point Likert scale that was completed anonymously. The models have obtained the following results: aesthetic recreation, 4.6 ± 0.5; realism during anesthesia infiltration, 4.8 ± 0.4; realism during lesion removal, 2.8 ± 0.4; realism during surgical wound closure, 1.2 ± 0.4. The score in this last section could be improved if a more elastic skin-colored filament were found on the market.
1. Introduction
Additive manufacturing is a manufacturing process by which parts are generated directly from a three-dimensional (3D) model, usually using a single machine (3D printer). These 3D printers manufacture the part layer by layer, using a raw material (resin, powder, filament) and an energy source [1]. The fused deposition modeling (FDM) 3D printing technique is used in different sectors [2]: automotive, aeronautics, medicine, architecture, or art.
There are several 3D printing techniques [3]: stereolithography (SLA), polyjet (PJ), selective laser sintering (SLS), and binder jetting (BJ). However, the most commonly used technique today is the fused deposition modeling (FDM) technique [4,5,6,7]. This technique has several advantages [8]: machines and filaments have low costs; it is easy to find information on the internet about this technique; the learning curve is short; and there is a large catalog of filaments available on the market, with multiple qualities and applications [9].
This paper focuses on the use of 3D printing in primary care centers. For years, the FDM technique has been used at the hospital level in different services and areas, with different objectives [10,11]: (i) to train students and residents during their training period [12,13,14]; (ii) to explain the interventions to patients before the operation [15,16]; (iii) to prepare the intervention, when it is complex [17,18]; (iv) to manufacture custom prostheses [6], among other uses. Despite the increasing use of 3D printing in hospitals [19], the authors have not found any work related to the use of 3D printing in primary care. In the present work, we propose the use of 3D printing to train general practitioners in minor surgery.
In Spain, with the development of primary care, the competencies of general practitioners (GPs) have been expanded with the aim of increasing the efficiency of the health system [20]. As in other European countries, the development of one of these competencies led to the creation of minor surgery programs in health centers [21]. In them, interventions for common lesions (dermal nevus, seborrheic keratosis, or epidermal cyst) are carried out [22].
GPs should learn these skills during their resident internal doctor-training period. However, due to the shortage of skilled adjunct professionals, practical training in this field is not adequate [23]. To make up for this lack, GPs interested in developing these aspects of their professional competence have to be trained through specific courses [24].
In minor surgery courses, the different phases of an intervention are taught [25]: (i) infiltration of anesthesia at the local level, (ii) removal of the lesion, and (iii) closure of the surgical wound. There are training models on the market that allow some of these phases to be practiced; however, these models have several handicaps: they do not have all the typical lesions in minor surgery, they do not faithfully reproduce the lesions of minor surgery, and they have a high cost. For these reasons, courses traditionally use pig’s feet, chicken thighs or bacon to practice the removal of figured lesions and suturing of wounds.
The purpose of this project is to design, manufacture (via the FDM 3D printing technique), and evaluate models for minor surgery courses in primary care centers. For this purpose, the most common lesions in minor surgery have been selected and modeled in 3D. These models have been manufactured using a double extruder printer, equipped with flexible filament. The models thus manufactured have been evaluated by a panel of experts in minor surgery. In addition, the models have been uploaded to an open standard tessellation (STL) file-exchange platform so that they can be used or improved by any interested person.
2. Materials and Methods
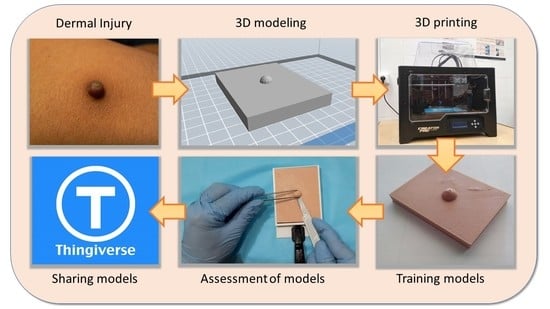
The methodology followed during this work has been the following (Figure 1): (i) in a first phase, it was decided which lesions were going to be modeled, the photographs to be taken as reference were selected, and some preliminary sketches were elaborated; (ii) then, the different lesions were modeled, using a parametric software of 3D design; (iii) the third phase consisted of importing the STL file from the slicing software, and selecting the print parameters necessary to generate the corresponding numerical control program; (iv) the different lesions were then printed; (v) once manufactured, the models were evaluated by a panel of experts; (vi) finally, the models were uploaded to an STL file-exchange platform.
2.1. Initial Stage
The first stage of the work corresponds to a series of meetings of the research team. The first decision made during this stage was which lesions were to be modeled (Figure 2): seborrheic keratosis, epidermal cyst, dermal nevus, and ingrown toenail. These lesions were chosen because they are the most frequently occurring in minor surgery patients.
During this stage, sketches of the lesions were drawn. In addition, important decisions were reached about the size of the models, the most suitable position for printing, the entities that make up the model, and use of the different materials or densities needed. These decisions are important as they have a direct impact on the manufacturing process (Table 1) [26]. At this stage, it was also agreed to fix the models to the table, so that they are firmly tied to the table during the intervention simulations.
2.2. 3D Modeling
From photographs (Figure 2), and from the sketches created in the previous stage (Figure 3a), 3D models of the lesions were made. The parametric software SolidWorks [27] was used for this purpose (Figure 3b). Once the lesion was modeled, the file was exported in STL standard, which is the format accepted by the slicing software.
The models corresponding to the dermal nevus, seborrheic keratosis and epidermal cyst were modeled with dimensions of 80 × 60 × 6 mm3. The model to reproduce the ingrown toenail was modeled to a realistic size.
2.3. Slicing
A numerical control (NC) code, which tells 3D printers what to do at any given moment, was needed. These NC codes are generated by slicing software from the STL files (Figure 3c). The 3D printer used in this work has been manufactured by FlashForge [28]. This company has developed its own slicing software for its 3D printers called FlashPrint [29]. In this software, it is necessary to indicate which material is going to be used, and which values for printing parameters are going to be selected [8]: extrusion temperature, layer height, print speed, among others. The values used in the present work are shown in Table 2.
2.4. 3D Printing
A FlashForge Creator Pro printer was used for the printing process. This machine has a hot bed (dimensions 225 x 125 mm2) and is equipped with two extruders (Figure 4). Several filaments have been used to print the models: a skin-resembling thermoplastic elastomer (TPE), Recreus brand (for the skin); a skin-resembling TPE, Tianse brand (for the inner sphere of the epidermal cyst and the nail); and a black TPE, Smart Materials 3D (for the seborrheic keratosis, Figure 3d).
2.5. Assessment
Once the models were printed, they underwent evaluation by a panel made up of five experts in minor surgery. The members of the evaluation panel are general practitioners, who work in rural primary care centers belonging to the Andalusian Health Service, and who each have more than 15 years of experience. These general practitioners perform interventions at least once a week.
It is difficult to find general practitioners who are experts in minor surgery. Although the number of experts may seem insufficient, according to [30] the results obtained with the use of a panel of five experts are adequate.
Each expert performed an operation simulation using each of the models. Subsequently, the experts filled out a survey, wherein they were asked their opinion on four main aspects of realism in the training models: aesthetics, infiltration of the anesthesia, removal of the lesion, and closure of the surgical wound. In this survey, the Likert 5-point scale was used (1—very disagreeable; 5—very agreeable). For additional information, the experts wrote a paragraph in relation to each of the aspects evaluated.
2.6. Sharing the Models
After the evaluation, the STL models were uploaded to Thingiverse [31]. Thingiverse is a repository for sharing 3D pieces. The idea is to share the designs developed during this project through creative commons license, so that anyone interested in performing practice in minor surgery can print them at home or at a primary care center.
3. Results
In the present work, models that reproduce lesions typical of minor surgery were designed and manufactured using 3D printing in order to train GPs in practical courses in this discipline. Once printed, the models were evaluated by a panel of experts. The aspects evaluated were: the aesthetic recreation of the models, realism during the infiltration of the anesthesia, realism in the removal of the lesion, and realism during the closure of the surgical wound. After the evaluation, the models were uploaded to Thingiverse [31] so that they can be used by any interested user (Figure 5).
3.1. Aesthetic Recreation Level
The score obtained by the models in this aspect was 4.6 ± 0.5. The panel of experts agreed that the models realistically recreate the most common injuries in minor surgery (Figure 6). One of the experts especially valued the effort made, as he said that the work is not easy. Another expert confessed that this work opens a very hopeful door to the teaching of minor surgery, which is as important as it is unknown to most GPs working in the field of primary care.
3.2. Realism During Anesthesia Infiltration
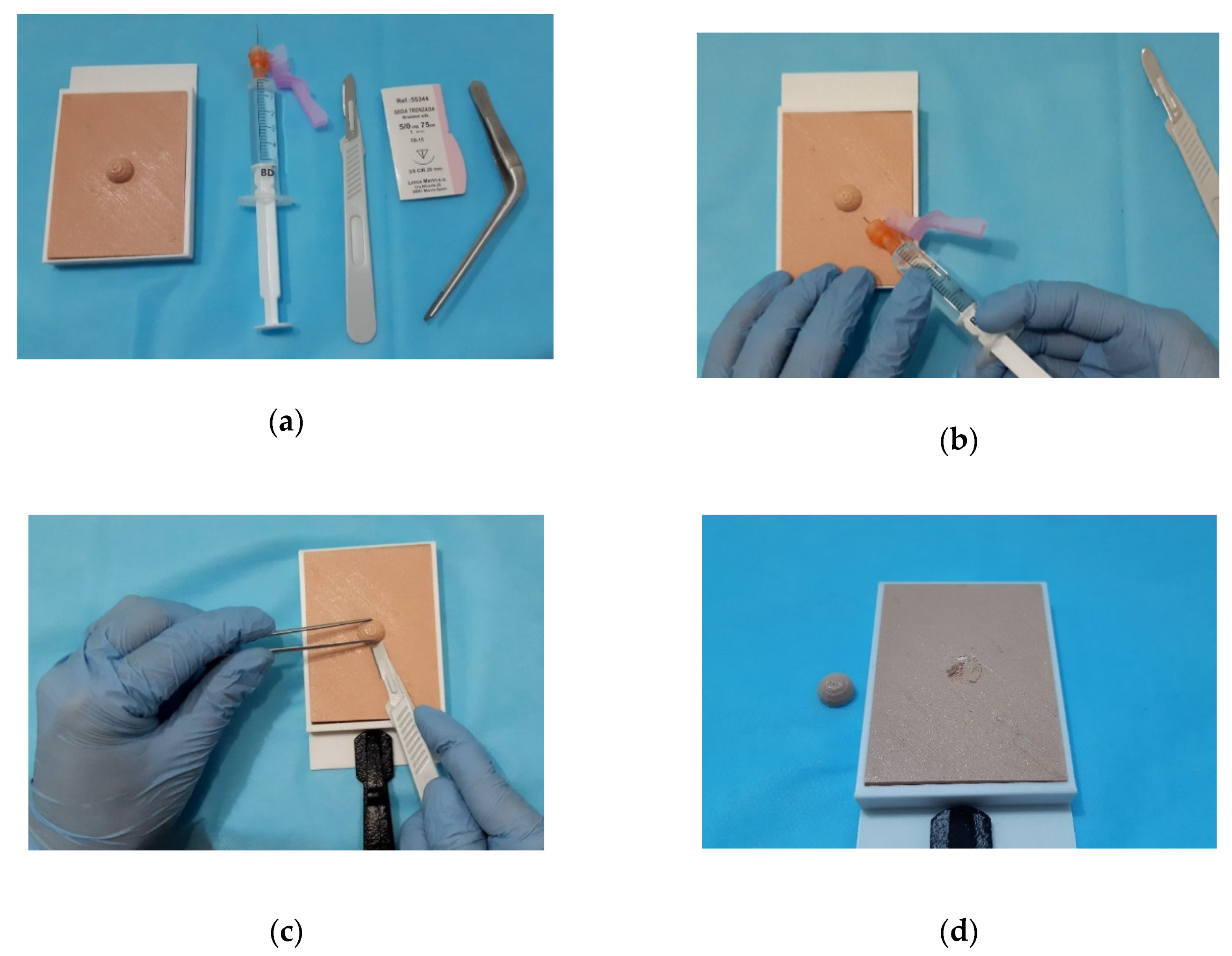
The score obtained by the models in this aspect was 4.8 ± 0.4. On this issue, the panel of experts agreed that the feel of the infiltration realistic (Figure 7a,b); it is especially realistic in the lesion of seborrheic keratosis and in the toe. One of the experts indicated that an improvement of the models would involve the possibility of injecting water with red dye to simulate blood, if not in the entire model, then at least around the lesion. In the case of the toe, a rigid tube could be added in the center to simulate the bone and a small ‘pipe’ on both sides to simulate the blood vessels.
3.3. Realism During Removal of the Lesion
The score obtained by the models in this aspect was 2.8 ± 0.4. In this third question, the panel of experts agreed again: in general, the sense of touch is not very similar to reality (Figure 7c). The material used is harder than human skin. There is even the risk of cutting yourself with the scalpel. One of the experts recommended using a material like silicone.
On the other hand, in the lesion of the cyst, the ‘skin’ should completely cover the cyst capsule. It is necessary to paint it to delimit the lesion and it is also necessary to have superficial material so that once the capsule has been removed, the skin can be sutured (bringing the edges of the wound closer together).
3.4. Realism During Surgical Wound Closure
The score obtained by the models in this aspect was 1.2 ± 0.4. In the case of seborrheic keratosis and fibroepithelioma, the wound would not be sutured but cauterized with the electric scalpel (Figure 7d). In the case of the cyst and toe, the silk suture would be used. However, the material is too hard, and the suture is very difficult to perform. The toe and nail do not reproduce the lesion well, so their intervention is not viable. The nail should be a thinner sheet and in the proximal part should be included ‘inside the skin’.
3.5. Cost of Models
The technology of fused filament deposition modeling has a low cost: printers are becoming cheaper and have a low electrical consumption; on the other hand, filaments cost between 25 and 60 euros/kilo, depending on the type of material.
From the data shown in Table 3, the cost of the different models manufactured has been calculated (Table 4). The price of labor has not been included in this calculation, as it is understood that the supervision of a printer could be carried out by resident internal doctors as part of their training. The price of each model is around 6 Euros (the ingrown toenail is cheaper because it has less material). The cost of a commercial training model is 38 Euros.
4. Discussion
In this work, 3D models that reproduce the most frequent lesions in minor surgery have been modeled, manufactured and evaluated. These models are representative of realistic lesions, since they are intended to be used to train GPs in primary care centers.
Manufactured training models cost less than commercial ones and faithfully reproduce injuries and lesions. In addition, they have been developed under an open-source license, so that anyone interested can download and print them from their home or primary care center.
The models have been evaluated by a panel of experts in minor surgery. Four aspects were assessed: the level of aesthetic recreation, realism during infiltration of the anesthesia, realism during removal of the lesion, and realism during closure of the surgical wound.
The panel of experts valued the level of recreation of the lesions positively, as well as the realism during the infiltration of the anesthesia. The removal of the lesion is more laborious than in real interventions, due to the density selected as the printing parameter and the qualities of the material used. It is not possible to close the surgical wound because the material is not elastic enough.
From the results obtained, the following statements can be made:
- Primary care centers can now access 3D printing. In hospitals, 3D-printed models have been used for several years to train surgeons [11,19]. Waran et al. [17] have found that the use of training models manufactured using 3D printing increases the success rate in major surgery operations and reduces the time spent on each intervention. Driven by this reality, the authors propose the use of this methodology in primary care centers, to carry out practical courses that serve to initiate GPs in minor surgery.
- The cost of the proposed models is low. FDM 3D printing allows healthcare resources to be manufactured at a low cost [32]. The training models proposed in this work have a cost of 6 Euros, compared to 38 Euros for commercial training models. This detail is important in a public health system such as the Spanish one, or in developing countries [33]. In addition, the proposed process allows a user to customize the models, and to manufacture those that have interest in each geographic point [34].
- The proposed models have a high level of aesthetic recreation. In major surgery, when lesions have some complexity, images taken by computed tomography (CT) and magnetic resonance imaging (MRI) are used to model the lesion in 3D [35]. In this case, the models have been performed in parametric design software from photographs and drawings made by one of the authors, an expert in minor surgery. However, the panel of experts have positively assessed the level of aesthetic recreation in the models.
- The models have been shared on Thingiverse. In the ‘maker’ world it is common to share designed models. This is one of the main attractions of 3D printing. Thingiverse is a widely used platform for sharing general models, although there are specific platforms for biomedical models, such as one developed by the National Institutes of Health of United States (NIH 3D) [36].
- FDM 3D printing technology is suitable for this purpose. There are 3D printing technologies that can print models of great complexity [37], although their cost cannot be borne by a primary care center. In the present work, the use of FDM technology has been proposed, which is the cheapest technology, and which provides a surface finish suitable for the intended use.
- The filament used is not elastic enough and it is not possible to close the surgical wound. It is necessary to look in the market for more elastic filaments that are available in skin color to overcome this handicap.
5. Conclusions
The present work proposes the use of the FDM technique of 3D printing to manufacture models of typical lesions in minor surgery. It is intended to use these models to train general practitioners in primary care centers. The models have been manufactured and evaluated by a panel of experts. The models have been approved in three of the four categories evaluated. In addition, the models have been uploaded to Thingiverse for anyone to download and use.
Author Contributions
Conceptualization, M.C.L. and P.E.R.; methodology, M.C.L. and A.C.-H.; software, A.C.-H.; validation, M.C.L., A.C.-H. and P.E.R.; formal analysis, M.C.L.; investigation, M.C.L.; resources, P.E.R.; data curation, A.C.-H.; writing—original draft preparation, M.C.L.; writing—review and editing, P.E.R.; visualization, M.C.L. and A.C.-H.; supervision, P.E.R.; project administration, P.E.R.; funding acquisition, P.E.R.
Funding
The authors would like to thank the funding received by the University of Cordoba’s Own Research Plan (2019).
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Lipson, H.; Kurman, M. Fabricated: The New World of 3D Printing; John Wiley & Sons Inc.: Indianapolis, IN, USA, 2013. [Google Scholar]
- Wong, K.V.; Hernandez, A. A Review of Additive Manufacturing. ISRN Mech. Eng. 2012, 2012, 1–10. [Google Scholar] [CrossRef]
- Sun, Z.; Lau, I.; Wong, Y.H.; Yeong, C.H. Personalized Three-Dimensional Printed Models in Congenital Heart Disease. J. Clin. Med. 2019, 8, 522. [Google Scholar] [CrossRef] [PubMed]
- Ahn, S.; Montero, M.; Odel, D.; Roundy, S.; Wright, P.K. Anisotropic material properties of fused deposition modeling ABS. Rapid Prototyp. J. 2002, 8, 248–257. [Google Scholar] [CrossRef]
- Ngo, T.D.; Kashani, A.; Imbalzano, G.; Nguyen, K.T.Q.; Hui, D. Additive manufacturing (3D printing): A review of materials, methods, applications and challenges. Compos. Part B Eng. 2018, 143, 172–196. [Google Scholar] [CrossRef]
- Ten Kate, J.; Smit, G.; Breedveld, P. 3D-printed upper limb prostheses: A review. Disabil. Rehabil. Assist. Technol. 2017, 12, 300–314. [Google Scholar] [CrossRef]
- Turner, B.N.; Strong, R.; Gold, S.A. A review of melt extrusion additive manufacturing processes: I. Process design and modeling. Rapid Prototyp. J. 2014, 20, 192–204. [Google Scholar] [CrossRef]
- Barrios, J.M.; Romero, P.E. Improvement of surface roughness and hydrophobicity in PETG parts manufactured via fused deposition modeling (FDM): An application in 3D printed self—Cleaning parts. Materials 2019, 12, 2499. [Google Scholar] [CrossRef]
- Smart Materials 3D. Available online: https://www.smartmaterials3d.com/en/ (accessed on 17 January 2019).
- Lee Ventola, C. Medical applications for 3D printing: Current and projected uses. Pharm. Ther. 2014, 39, 704–711. [Google Scholar]
- Tack, P.; Victor, J.; Gemmel, P.; Annemans, L. 3D-printing techniques in a medical setting: A systematic literature review. Biomed. Eng. Online 2016, 15, 115. [Google Scholar] [CrossRef]
- Mcmenamin, P.G.; Quayle, M.R.; Mchenry, C.R.; Adams, J.W. The production of anatomical teaching resources using three-dimensional (3D) printing technology. Anat. Sci. Educ. 2014, 7, 479–486. [Google Scholar] [CrossRef]
- Barber, S.R.; Kozin, E.D.; Dedmon, M.; Lin, B.M.; Lee, K.; Sinha, S.; Black, N.; Remenschneider, A.K.; Lee, D.J. 3D-printed pediatric endoscopic ear surgery simulator for surgical training. Int. J. Pediatr. Otorhinolaryngol. 2016, 90, 113–118. [Google Scholar] [CrossRef] [PubMed]
- Ho, D.; Squelch, A.; Sun, Z. Modelling of aortic aneurysm and aortic dissection through 3D printing. J. Med. Radiat. Sci. 2017, 64, 10–17. [Google Scholar] [CrossRef] [PubMed]
- Pérez-Mañanes, R.; Calvo-Haro, J.; Arnal-Burró, J.; Chana-Rodríguez, F.; Sanz-Ruiz, P.; Vaquero-Martín, J. Our experience with domestic 3D printing in Orthopedic Surgery and Traumatology. Do it yourself. Rev. Latinoam. Cirugía Ortopédica 2016, 1, 47–53. [Google Scholar] [CrossRef]
- Allan, A.; Kealley, C.; Squelch, A.; Wong, Y.H.; Yeong, C.H.; Sun, Z. Patient-specific 3D printed model of biliary ducts with congenital cyst. Quant. Imaging Med. Surg. 2019, 9, 86–93. [Google Scholar] [CrossRef]
- Waran, V.; Narayanan, V.; Karuppiah, R.; Pancharatnam, D.; Chandran, H.; Raman, R.; Rahman, Z.A.A.; Owen, S.L.F.; Aziz, T.Z. Injecting realism in surgical training—Initial simulation experience with custom 3D models. J. Surg. Educ. 2014, 71, 193–197. [Google Scholar] [CrossRef]
- Michalski, M.H.; Ross, J.S. The shape of things to come: 3D printing in medicine. JAMA 2014, 312, 2213–2214. [Google Scholar] [CrossRef]
- Martelli, N.; Serrano, C.; Van Den Brink, H.; Pineau, J.; Prognon, P.; Borget, I.; El Batti, S. Advantages and disadvantages of 3-dimensional printing in surgery: A systematic review. Surgery 2016, 159, 1485–1500. [Google Scholar] [CrossRef]
- Tárraga López, P.J.; Marín Nieto, E.; García Olmo, D.; Celada Rodríguez, A.; Solera Albero, J. Economic impact of the introduction of a minor surgery program in primary care. Aten. Primaria 2001, 27, 335–338. [Google Scholar] [CrossRef]
- Gokani, V.J.; Ferguson, H.J.M.; Fitzgerald, J.E.F.; Beamish, A.J. Surgical training in primary care: Consensus recommendations by the Association of Surgeons in Training. Int. J. Surg. 2014, 12, S1–S4. [Google Scholar] [CrossRef]
- Serra, M.; Arevalo, A.; Ortega, C.; Ripoll, A.; Giménez, N. Minor surgery activity in primary care. J. R. Soc. Med. Short Rep. 2010, 1, 1–8. [Google Scholar] [CrossRef]
- Puche, J.M.; Muñoz, P.A. Program to introduce and develop minor surgery at a primary-care center in Spain. Arch. Med. Fam. 2009, 11, 39–49. [Google Scholar]
- Garrido, S.E.; García, R.V.; Nogales, P.A. Continuing education in primary care: The educational needs of its professionals. Aten. Primaria 2002, 30, 368–373. [Google Scholar]
- Brown, J. Minor Surgery, a Text and Atlas, 4th ed.; CRC Press: London, UK, 2001; ISBN 978-0340761137. [Google Scholar]
- Thompson, M.K.; Moroni, G.; Vaneker, T.; Fadel, G.; Campbell, R.I.; Gibson, I.; Bernard, A.; Schulz, J.; Graf, P.; Ahuja, B.; et al. Design for additive manufacturing: Trends, opportunities, considerations, and constraints. CIRP Ann. Manuf. Technol. 2016, 65, 737–760. [Google Scholar] [CrossRef]
- SolidWorks. Available online: https://www.solidworks.com/ (accessed on 1 November 2019).
- FlashForge. Available online: https://www.flashforge.com/ (accessed on 1 November 2019).
- FlashPrint. Available online: https://www.flashforge.com/download-center (accessed on 1 November 2019).
- Hyrkäs, K.; Appelqvist-Schmidlechner, K.; Oksa, L. Validating an instrument for clinical supervision using an expert panel. Int. J. Nurs. Stud. 2003, 40, 619–625. [Google Scholar] [CrossRef]
- Thingiverse. Available online: https://www.thingiverse.com/ (accessed on 1 November 2019).
- Rismani, S.; Van der Loos, H.F.M. The Competitive Advantage of Using 3D-Printing in Low-Resource Healthcare Settings. In Proceedings of the 20th International Conference on Engineering Design, Milan, Italy, 27–30 July 2015; pp. 1–10. [Google Scholar]
- Corsini, L.; Aranda-Jan, C.B.; Moultrie, J. Using digital fabrication tools to provide humanitarian and development aid in low-resource settings. Technol. Soc. 2019, 58, 101117. [Google Scholar] [CrossRef]
- Petrick, I.J.; Simpson, T.W. 3D printing disrupts manufacturing. Res. Technol. Manag. 2013, 56, 12–16. [Google Scholar] [CrossRef]
- Rengier, F.; Mehndiratta, A.; Von Tengg-Kobligk, H.; Zechmann, C.M.; Unterhinninghofen, R.; Kauczor, H.U.; Giesel, F.L. 3D printing based on imaging data: Review of medical applications. Int. J. Comput. Assist. Radiol. Surg. 2010, 5, 335–341. [Google Scholar] [CrossRef]
- Coakley, M.F.; Hurt, D.E.; Weber, N.; Mtingwa, M.; Fincher, E.C.; Alekseyev, V.; Chen, D.T.; Yun, A.; Gizaw, M.; Swan, J.; et al. The NIH 3D print exchange: A public resource for bioscientific and biomedical 3D prints. 3D Print. Addit. Manuf. 2014, 1, 137–140. [Google Scholar] [CrossRef]
- Jacobs, S.; Grunert, R.; Mohr, F.W.; Falk, V. 3D-Imaging of cardiac structures using 3D heart models for planning in heart surgery: A preliminary study. Interact. Cardiovasc. Thorac. Surg. 2008, 7, 6–9. [Google Scholar] [CrossRef] [Green Version]
Figure 1.
Diagram summarizing graphically the stages followed during the execution of the work: initial phase, where the sketches of the models were generated; the 3D modeling of the different models; slicing of the models and configuration of the 3D printer; the 3D printing of the models and post-processing tasks; evaluation of the models; uploading of the standard tessellation (STL) files to Thingiverse.
Figure 1.
Diagram summarizing graphically the stages followed during the execution of the work: initial phase, where the sketches of the models were generated; the 3D modeling of the different models; slicing of the models and configuration of the 3D printer; the 3D printing of the models and post-processing tasks; evaluation of the models; uploading of the standard tessellation (STL) files to Thingiverse.

Figure 2.
Images of the most common lesions in the minor surgery practice: dermal nevus (a); seborrheic keratosis (b); epidermal cyst (c); ingrown toenail (d).
Figure 2.
Images of the most common lesions in the minor surgery practice: dermal nevus (a); seborrheic keratosis (b); epidermal cyst (c); ingrown toenail (d).

Figure 3.
Modeling and manufacturing of the seborrheic keratosis training model: draft developed in initial stage (a); the 3D model generated by SolidWorks software (b); the imported model in FlashPrint slicing software (c); the 3D printed lesion (d).
Figure 3.
Modeling and manufacturing of the seborrheic keratosis training model: draft developed in initial stage (a); the 3D model generated by SolidWorks software (b); the imported model in FlashPrint slicing software (c); the 3D printed lesion (d).

Figure 4.
FlashForge Creator Pro 3D printer used in the project (left); rear of the printer, with two bobbins of skin-resembling thermoplastic elastomer (TPE) filament (right).
Figure 4.
FlashForge Creator Pro 3D printer used in the project (left); rear of the printer, with two bobbins of skin-resembling thermoplastic elastomer (TPE) filament (right).

Figure 5.
User web page created in Thingiverse to upload the models of minor surgery injuries. Any interested user can download these standard tessellation (STL) models for free and print them in their home or primary care center.
Figure 5.
User web page created in Thingiverse to upload the models of minor surgery injuries. Any interested user can download these standard tessellation (STL) models for free and print them in their home or primary care center.

Figure 6.
Models of minor surgical lesions: dermal nevus (a); seborrheic keratosis (b); epidermal cyst (c); ingrown toenail (d).
Figure 6.
Models of minor surgical lesions: dermal nevus (a); seborrheic keratosis (b); epidermal cyst (c); ingrown toenail (d).

Figure 7.
Stages of the intervention performed on the dermal nevus model: preparation of the necessary material (a); infiltration of the anesthesia (b); removal of the lesion (c); outcome (d).
Figure 7.
Stages of the intervention performed on the dermal nevus model: preparation of the necessary material (a); infiltration of the anesthesia (b); removal of the lesion (c); outcome (d).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Table 1.
Relationship between initial decisions and the designing and manufacturing process.
| Initial Decisions | Have Influence on |
|---|---|
| Size | Print time |
| Print position | Possibility of printing Surface roughness |
| Entities that make up the model | Procedure to model the lesion in 3D |
| Combination of materials | Using the two 3D printer extruders |
| Print density | Flexibility of the model Print time |
| Pattern | Flexibility of the model |
Table 2.
Parameter values used during printing.
| Print Parameter | Value |
|---|---|
| Extrusion Temperature | 225 °C |
| Bed Temperature | 50 °C |
| Layer Height | 0.18 mm |
| First-Level Layer Height | 0.27 mm |
| Retraction Length | 3.7 mm |
| Fill Density | 90% |
| Fill Pattern | Hexagon |
Table 3.
Parameter values used during costing.
| Parameter | Value |
|---|---|
| Cost of plastic (€/kg) | 60 |
| Cost of electrical energy (€/kWh) | 0.15 |
| 3D Printer power (kW) | 0.500 |
| Cost of the 3D printer (€) | 599 |
| Amortization period (years) | 1 |
| Days active per year | 250 |
| Hours per day (h) | 8 |
| Failure rate (%) | 5 |
Table 4.
Cost of printing the training models manufactured (not including the cost of labor, as the printing could be supervised by internal doctors’ residents as part of their training process).
Table 4.
Cost of printing the training models manufactured (not including the cost of labor, as the printing could be supervised by internal doctors’ residents as part of their training process).
| Parameter | Dermal Nevus | Seborrheic Keratosis | Epidermal Cyst | Ingrown Nail |
|---|---|---|---|---|
| Workpiece mass (kg) | 0.06 | 0.05 | 0.06 | 0.01 |
| Printing time (h) | 5.9 | 5.80 | 6.00 | 2.01 |
| Cost of plastic material (€) | 3.61 | 3.10 | 3.61 | 0.98 |
| Cost of electricity (€) | 0.44 | 0.44 | 0.45 | 0.15 |
| Equipment amortization cost (€) | 1.77 | 1.74 | 1.80 | 0.60 |
| Cost of failures (€) | 0.29 | 0.26 | 0.29 | 0.09 |
| Total (€) | 6.11 | 5.53 | 6.15 | 1.81 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Luque, M.C.; Calleja-Hortelano, A.; Romero, P.E. Use of 3D Printing in Model Manufacturing for Minor Surgery Training of General Practitioners in Primary Care. Appl. Sci. 2019, 9, 5212. https://doi.org/10.3390/app9235212
AMA Style
Luque MC, Calleja-Hortelano A, Romero PE. Use of 3D Printing in Model Manufacturing for Minor Surgery Training of General Practitioners in Primary Care. Applied Sciences. 2019; 9(23):5212. https://doi.org/10.3390/app9235212
Chicago/Turabian StyleLuque, M.C., A. Calleja-Hortelano, and P.E. Romero. 2019. "Use of 3D Printing in Model Manufacturing for Minor Surgery Training of General Practitioners in Primary Care" Applied Sciences 9, no. 23: 5212. https://doi.org/10.3390/app9235212
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.