
Interaction of Garcinia cambogia (Gaertn.) Desr. and Drugs as a Possible Mechanism of Liver Injury: The Case of Montelukast
 , , , ,
, , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Phytovigilance Methodology
2.2. In Vitro Toxicological Study
2.2.1. Chemicals
2.2.2. Garcinia Cambogia Extract
2.2.3. Cell Culture
2.2.4. Cytotoxicity Assay
2.2.5. Combination Assay
2.2.6. Analysis of G.-cambogia–Drug Interaction
2.2.7. Determination of Intracellular Levels of Reactive Oxygen Species (ROS)
2.2.8. Immunofluorescence Analysis of Nrf2
2.3. Statistical Analysis
3. Results
3.1. Analysis of Spontaneous Reports
3.2. In Vitro Analysis of G. cambogia Hepatotoxicity
3.2.1. Cytotoxicity of G. cambogia and Montelukast in Human Intrahepatic Cholangiocytes
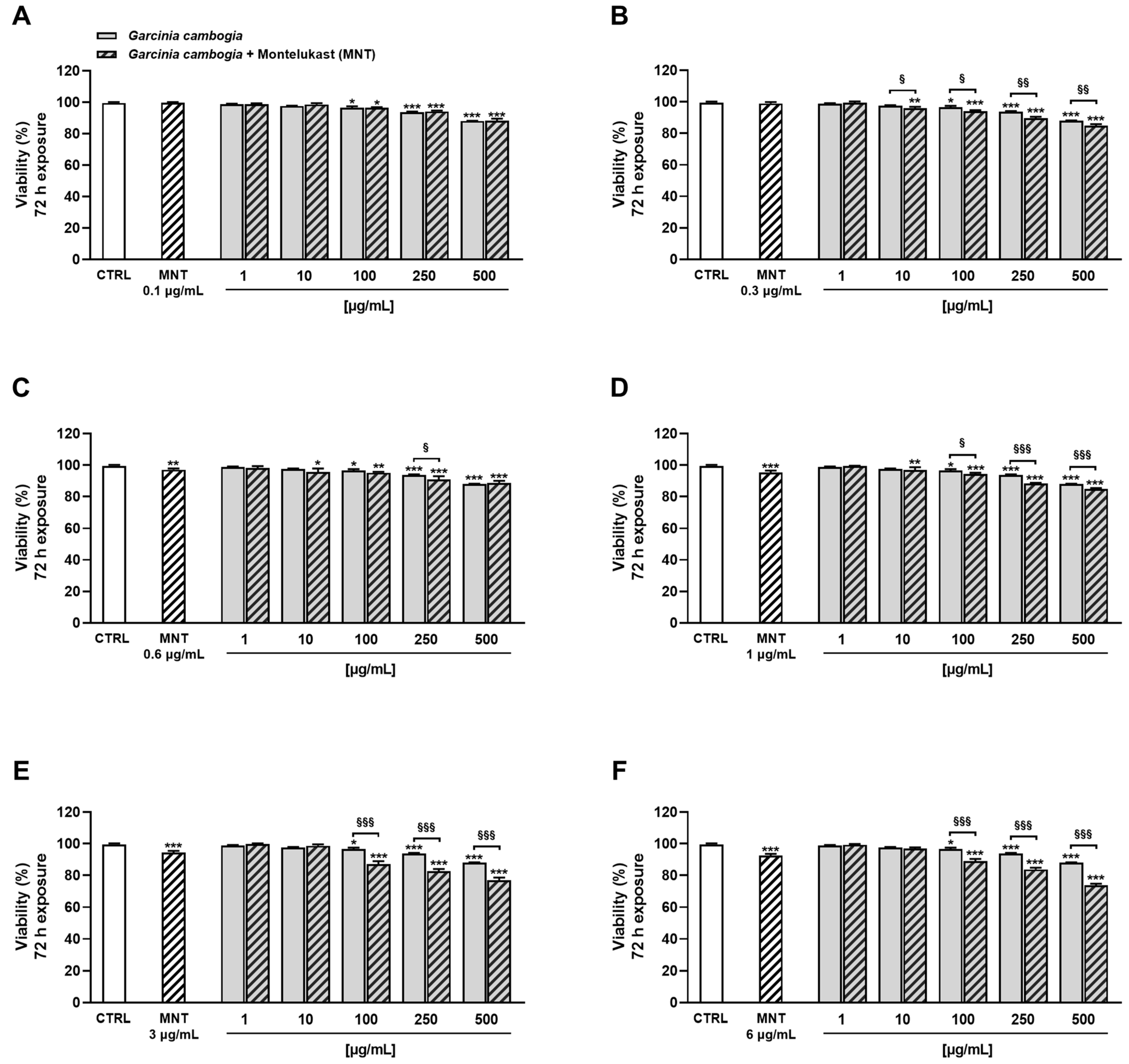
3.2.2. Montelukast Increases G. cambogia Cytotoxicity on Human Intrahepatic Cholangiocytes
3.2.3. Montelukast Increases G. cambogia Cytotoxicity by Enhancing Its Oxidative Properties
3.2.4. G. cambogia and Montelukast Affect Nrf2 Cytoplasmic Expression
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Di Giacomo, S.; Briz, O.; Vitalone, A.; Di Sotto, A. Editorial: Natural Products and Hepatic Health: Light and Shadows. Front. Pharmacol. 2022, 13, 868207. [Google Scholar] [CrossRef]
- Marin, J.J.G.; Serrano, M.A.; Monte, M.J.; Sanchez-Martin, A.; Temprano, A.G.; Briz, O.; Romero, M.R. Role of Genetic Variations in the Hepatic Handling of Drugs. Int. J. Mol. Sci. 2020, 21, 2884. [Google Scholar] [CrossRef]
- Reyes-Gordillo, K.; Shah, R.; Muriel, P. Oxidative Stress and Inflammation in Hepatic Diseases: Current and Future Therapy. Oxid. Med. Cell Longev. 2017, 2017, 3140673. [Google Scholar] [CrossRef] [PubMed]
- Esrefoglu, M. Oxidative stress and benefits of antioxidant agents in acute and chronic hepatitis. Hepat. Mon. 2012, 12, 160–167. [Google Scholar] [CrossRef]
- Kasai, S.; Shimizu, S.; Tatara, Y.; Mimura, J.; Itoh, K. Regulation of Nrf2 by Mitochondrial Reactive Oxygen Species in Physiology and Pathology. Biomolecules 2020, 10, 320. [Google Scholar] [CrossRef]
- Shekhova, E. Mitochondrial reactive oxygen species as major effectors of antimicrobial immunity. PLoS Pathog. 2020, 16, e1008470. [Google Scholar] [CrossRef] [PubMed]
- Li, S.; Hong, M.; Tan, H.Y.; Wang, N.; Feng, Y. Insights into the Role and Interdependence of Oxidative Stress and Inflammation in Liver Diseases. Oxid. Med. Cell Longev. 2016, 2016, 4234061. [Google Scholar] [CrossRef] [PubMed]
- Blas-García, A.; Apostolova, N. Novel Therapeutic Approaches to Liver Fibrosis Based on Targeting Oxidative Stress. Antioxidants 2023, 12, 1567. [Google Scholar] [CrossRef]
- Sato, K.; Kennedy, L.; Liangpunsakul, S.; Kusumanchi, P.; Yang, Z.; Meng, F.; Glaser, S.; Francis, H.; Alpini, G. Intercellular Communication between Hepatic Cells in Liver Diseases. Int. J. Mol. Sci. 2019, 20, 2180. [Google Scholar] [CrossRef]
- Li, Y.; Li, S.; Xue, X.; Wang, T.; Li, X. Integrating systematic pharmacology-based strategy and experimental validation to explore mechanism of Tripterygium glycoside on cholangiocyte-related liver injury. Chin. Herb. Med. 2022, 14, 563–575. [Google Scholar] [CrossRef]
- Yang, Y.; Ge, F.L.; Tang, J.F.; Qin, S.L.; Zeng, R.; Yao, M.L.; Xiao, X.H.; Bai, Z.F.; Tang, C.L. A review of herb-induced liver injury in mainland china. Front. Pharmacol. 2022, 13, 813073. [Google Scholar] [CrossRef]
- Ma, Z.T.; Shi, Z.; Xiao, X.H.; Wang, J.B. New Insights into Herb-Induced Liver Injury. Antioxid. Redox Signal 2023, 38, 1138–1149. [Google Scholar] [CrossRef] [PubMed]
- Byeon, J.-H.; Kil, J.-H.; Ahn, Y.-C.; Son, C.-G. Systematic review of published data on herb induced liver injury. J. Ethnopharmacol. 2019, 233, 190–196. [Google Scholar] [CrossRef]
- Teka, T.; Wang, L.; Gao, J.; Mou, J.; Pan, G.; Yu, H.; Gao, X.; Han, L. Polygonum multiflorum: Recent updates on newly isolated compounds, potential hepatotoxic compounds and their mechanisms. J. Ethnopharmacol. 2021, 271, 113864. [Google Scholar] [CrossRef] [PubMed]
- Mazzanti, G.; Di Sotto, A.; Vitalone, A. Hepatotoxicity of green tea: An update. Arch. Toxicol. 2015, 89, 1175–1191. [Google Scholar] [CrossRef] [PubMed]
- Menniti-Ippolito, F.; Ippoliti, I.; Pastorelli, A.A.; Altieri, I.; Scalise, F.; De Santis, B.; Debegnach, F.; Brera, C.; Pacifici, R.; Pichini, S.; et al. Turmeric (Curcuma longa L.) food supplements and hepatotoxicity: An integrated evaluation approach. Ann. Ist. Super. Sanita 2020, 56, 462–469. [Google Scholar] [CrossRef]
- Andueza, N.; Giner, R.M.; Portillo, M.P. Risks Associated with the Use of Garcinia as a Nutritional Complement to Lose Weight. Nutrients 2021, 13, 450. [Google Scholar] [CrossRef]
- Yousaf, M.N.; Chaudhary, F.S.; Hodanazari, S.M.; Sittambalam, C.D. Hepatotoxicity associated with Garcinia cambogia: A case report. World J. Hepatol. 2019, 11, 735–742. [Google Scholar] [CrossRef]
- Mas Ordeig, A.; Bordón García, N. Hepatotoxicity caused by Garcinia cambogia. Gastroenterol. Hepatol. 2020, 43, 134–135. [Google Scholar] [CrossRef]
- Lunsford, K.E.; Bodzin, A.S.; Reino, D.C.; Wang, H.L.; Busuttil, R.W. Dangerous dietary supplements: Garcinia cambogia-associated hepatic failure requiring transplantation. World J. Gastroenterol. 2016, 22, 10071–10076. [Google Scholar] [CrossRef] [PubMed]
- Kothadia, J.P.; Kaminski, M.; Samant, H.; Olivera-Martinez, M. Hepatotoxicity Associated with Use of the Weight Loss Supplement Garcinia cambogia: A Case Report and Review of the Literature. Case Rep. Hepatol. 2018, 2018, 6483605. [Google Scholar] [CrossRef] [PubMed]
- Crescioli, G.; Lombardi, N.; Bettiol, A.; Marconi, E.; Risaliti, F.; Bertoni, M.; Menniti Ippolito, F.; Maggini, V.; Gallo, E.; Firenzuoli, F.; et al. Acute liver injury following Garcinia cambogia weight-loss supplementation: Case series and literature review. Intern. Emerg. Med. 2018, 13, 857–872. [Google Scholar] [CrossRef] [PubMed]
- Corey, R.; Werner, K.T.; Singer, A.; Moss, A.; Smith, M.; Noelting, J.; Rakela, J. Acute liver failure associated with Garcinia cambogia use. Ann. Hepatol. 2016, 15, 123–126. [Google Scholar] [CrossRef]
- Anilkumar, A.T.; Manoharan, S.; Balasubramanian, S.; Perumal, E. Garcinia gummi-gutta: Phytochemicals and pharmacological applications. Biofactors 2023, 49, 584–599. [Google Scholar] [CrossRef]
- Semwal, R.B.; Semwal, D.K.; Vermaak, I.; Viljoen, A. A comprehensive scientific overview of Garcinia cambogia. Fitoterapia 2015, 102, 134–148. [Google Scholar] [CrossRef]
- Ferreira, V.; Mathieu, A.; Soucy, G.; Giard, J.M.; Erard-Poinsot, D. Acute Severe Liver Injury Related to Long-Term Garcinia cambogia Intake. ACG Case Rep. J. 2020, 7, e00429. [Google Scholar] [CrossRef]
- Flerova, E.; Ambilil, M.; Civan, J.M.; Sass, D.A.; Maley, W.R.; Pulinthanathu, R.; Huang, J. Striking Cholestatic Giant Cell Hepatitis Resulting in Fulminant Liver Failure After Garcinia Cambogia Use. Int. J. Surg. Pathol. 2023, 10668969231186926. [Google Scholar] [CrossRef]
- WHO-UMC. The Use of the WHO-UMC System for Standardised Case Causality Assessment. Available online: https://who-umc.org/media/164200/who-umc-causality-assessment_new-logo.pdf (accessed on 20 July 2023).
- Nguyen, T.; Nioi, P.; Pickett, C.B. The Nrf2-antioxidant response element signaling pathway and its activation by oxidative stress. J. Biol. Chem. 2009, 284, 13291–13295. [Google Scholar] [CrossRef]
- Banales, J.M.; Sáez, E.; Uriz, M.; Sarvide, S.; Urribarri, A.D.; Splinter, P.; Tietz Bogert, P.S.; Bujanda, L.; Prieto, J.; Medina, J.F.; et al. Up-regulation of microRNA 506 leads to decreased Cl−/HCO3− anion exchanger 2 expression in biliary epithelium of patients with primary biliary cirrhosis. Hepatology 2012, 56, 687–697. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Z.; Zhong, X.; Shen, H.; Sheng, L.; Liangpunsakul, S.; Lok, A.S.; Omary, M.B.; Wang, S.; Rui, L. Biliary NIK promotes ductular reaction and liver injury and fibrosis in mice. Nat. Commun. 2022, 13, 5111. [Google Scholar] [CrossRef]
- Kim, Y.J.; Choi, M.S.; Park, Y.B.; Kim, S.R.; Lee, M.K.; Jung, U.J. Garcinia Cambogia attenuates diet-induced adiposity but exacerbates hepatic collagen accumulation and inflammation. World J. Gastroenterol. 2013, 19, 4689–4701. [Google Scholar] [CrossRef]
- Altaş, U.; Altaş, Z.M.; Öz, F.; Özkars, M.Y. Evaluation of Neuropsychiatric Effects of Montelukast–Levocetirizine Combination Therapy in Children with Asthma and Allergic Rhinitis. Children 2023, 10, 1301. [Google Scholar] [CrossRef]
- Ranbaxy, U.-L. Montelukast Leaflet. Available online: https://www.medicines.org.uk/emc/files/pil.2622.pdf (accessed on 10 August 2023).
- Actis, G.C.; Bugianesi, E.; Ottobrelli, A.; Rizzetto, M. Fatal liver failure following food supplements during chronic treatment with montelukast. Dig. Liver Dis. 2007, 39, 953–955. [Google Scholar] [CrossRef] [PubMed]
- Ippoliti, I.; Menniti-Ippolito, F.; Mazzanti, G.; Di Giacomo, S. Suspected adverse reactions to performance enhancing dietary supplements: Spontaneous reports from the Italian phytovigilance system. Phytother. Res. 2021, 35, 3246–3261. [Google Scholar] [CrossRef]
- Italian-Ministerial-Decree. Regulation of the Use of Vegetable Substances and Preparations in Food Supplements (18A06095). Annex 2 “Documentation Supporting the Use of Substances and Herbal Preparations in Food Supplements”. 2018. Available online: https://www.gazzettaufficiale.it/eli/id/2018/09/26/18A06095/sg (accessed on 10 August 2023).
- Di Giacomo, S.; Di Sotto, A.; Angelis, A.; Percaccio, E.; Vitalone, A.; Gullì, M.; Macone, A.; Axiotis, E.; Skaltsounis, A.L. Phytochemical Composition and Cytoprotective Properties of the Endemic Sideritis sipylea Boiss Greek Species: A Valorization Study. Pharmaceuticals 2022, 15, 987. [Google Scholar] [CrossRef] [PubMed]
- Di Giacomo, S.; Gullì, M.; Facchinetti, R.; Minacori, M.; Mancinelli, R.; Percaccio, E.; Scuderi, C.; Eufemi, M.; Di Sotto, A. Sorafenib Chemosensitization by Caryophyllane Sesquiterpenes in Liver, Biliary, and Pancreatic Cancer Cells: The Role of STAT3/ABC Transporter Axis. Pharmaceutics 2022, 14, 1264. [Google Scholar] [CrossRef] [PubMed]
- Zheng, S.; Wang, W.; Aldahdooh, J.; Malyutina, A.; Shadbahr, T.; Tanoli, Z.; Pessia, A.; Tang, J. SynergyFinder Plus: Toward Better Interpretation and Annotation of Drug Combination Screening Datasets. Genom. Proteom. Bioinform. 2022, 20, 587–596. [Google Scholar] [CrossRef]
- Taiti, C.; Stefano, G.; Percaccio, E.; Di Giacomo, S.; Iannone, M.; Marianelli, A.; Di Sotto, A.; Garzoli, S. Addition of Spirulina to Craft Beer: Evaluation of the Effects on Volatile Flavor Profile and Cytoprotective Properties. Antioxidants 2023, 12, 1021. [Google Scholar] [CrossRef]
- El-Ashmawy, N.E.; Khedr, E.G.; Khedr, N.F.; El-Adawy, S.A. Suppression of epithelial-mesenchymal transition and SIRT1/AKT signaling pathway in breast cancer by montelukast. Int. Immunopharmacol. 2023, 119, 110148. [Google Scholar] [CrossRef]
- Kang, L.; Xiang, Q.; Zhan, S.; Song, Y.; Wang, K.; Zhao, K.; Li, S.; Shao, Z.; Yang, C.; Zhang, Y. Restoration of Autophagic Flux Rescues Oxidative Damage and Mitochondrial Dysfunction to Protect against Intervertebral Disc Degeneration. Oxid. Med. Cell Longev. 2019, 2019, 7810320. [Google Scholar] [CrossRef]
- Awortwe, C.; Makiwane, M.; Reuter, H.; Muller, C.; Louw, J.; Rosenkranz, B. Critical evaluation of causality assessment of herb-drug interactions in patients. Br. J. Clin. Pharmacol. 2018, 84, 679–693. [Google Scholar] [CrossRef] [PubMed]
- Foucquier, J.; Guedj, M. Analysis of drug combinations: Current methodological landscape. Pharmacol. Res. Perspect. 2015, 3, e00149. [Google Scholar] [CrossRef] [PubMed]
- Wen, Z.G.; Zhang, Q.Q.; Zhang, L.L.; Shen, M.F.; Huang, Y.S.; Zhao, L.H. Efficacy and safety of traditional chinese medicine treatment for overweight and obese individuals: A systematic review and meta-analysis. Front. Pharmacol. 2022, 13, 964495. [Google Scholar] [CrossRef]
- Allkanjari, O.; Annetta, A.; Di Sotto, A.; Vitalone, A. Safety of herbal dietary supplements used for weight loss: Sales data and phytovigilance awareness. Nutrire 2023, 48, 37. [Google Scholar] [CrossRef]
- Mazzanti, G.; Vitalone, A.; Da Cas, R.; Menniti-Ippolito, F. Suspected adverse reactions associated with herbal products used for weight loss: Spontaneous reports from the Italian Phytovigilance System. Eur. J. Clin. Pharmacol. 2019, 75, 1599–1615. [Google Scholar] [CrossRef]
- Idrees, Z.; Cancarevic, I.; Huang, L. FDA-Approved Pharmacotherapy for Weight Loss Over the Last Decade. Cureus 2022, 14, e29262. [Google Scholar] [CrossRef]
- Dickinson, A.; MacKay, D. Health habits and other characteristics of dietary supplement users: A review. Nutr. J. 2014, 13, 14. [Google Scholar] [CrossRef]
- Sile, I.; Teterovska, R.; Onzevs, O.; Ardava, E. Safety Concerns Related to the Simultaneous Use of Prescription or Over-the-Counter Medications and Herbal Medicinal Products: Survey Results among Latvian Citizens. Int. J. Environ. Res. Public. Health 2023, 20, 6551. [Google Scholar] [CrossRef]
- Dilber, M.; Bayar Muluk, N.; Vejselova Sezer, C.; Mehtap Kutlu, H.; Cingi, C. Is G. cambogia a promising treatment? Effects on cultured nasal epithelial cells. Eur. Rev. Med. Pharmacol. Sci. 2022, 26, 15–24. [Google Scholar] [CrossRef]
- Kim, I.H.; Nam, T.J. Enzyme-treated Ecklonia cava extract inhibits adipogenesis through the downregulation of C/EBPα in 3T3-L1 adipocytes. Int. J. Mol. Med. 2017, 39, 636–644. [Google Scholar] [CrossRef]
- Cao, H.; Al Mamun Bhuyan, A.; Umbach, A.T.; Ma, K.; Borst, O.; Gawaz, M.; Zhang, S.; Nürnberg, B.; Lang, F. Garcinol A Novel Inhibitor of Platelet Activation and Apoptosis. Toxins 2019, 11, 382. [Google Scholar] [CrossRef] [PubMed]
- Di Giacomo, S.; Di Sotto, A.; Mazzanti, G.; Wink, M. Chemosensitizing Properties of β-Caryophyllene and β-Caryophyllene Oxide in Combination with Doxorubicin in Human Cancer Cells. Anticancer. Res. 2017, 37, 1191–1196. [Google Scholar] [CrossRef]
- Harasym, T.O.; Liboiron, B.D.; Mayer, L.D. Drug Ratio-Dependent Antagonism: A New Category of Multidrug Resistance and Strategies for Its Circumvention. In Multi-Drug Resistance in Cancer; Zhou, J., Ed.; Humana Press: Totowa, NJ, USA, 2010; pp. 291–323. [Google Scholar]
- Calapai, G.; Casciaro, M.; Miroddi, M.; Calapai, F.; Navarra, M.; Gangemi, S. Montelukast-induced adverse drug reactions: A review of case reports in the literature. Pharmacology 2014, 94, 60–70. [Google Scholar] [CrossRef] [PubMed]
- Lassila, T.; Hokkanen, J.; Aatsinki, S.M.; Mattila, S.; Turpeinen, M.; Tolonen, A. Toxicity of Carboxylic Acid-Containing Drugs: The Role of Acyl Migration and CoA Conjugation Investigated. Chem. Res. Toxicol. 2015, 28, 2292–2303. [Google Scholar] [CrossRef] [PubMed]
- Fei, Z.; Zhang, L.; Wang, L.; Jiang, H.; Peng, A. Montelukast ameliorated pemetrexed-induced cytotoxicity in hepatocytes by mitigating endoplasmic reticulum (ER) stress and nucleotide oligomerization domain-like receptor protein 3 (NLRP3) activation. Bioengineered 2022, 13, 7894–7903. [Google Scholar] [CrossRef]
- Pu, S.; Liu, Q.; Li, Y.; Li, R.; Wu, T.; Zhang, Z.; Huang, C.; Yang, X.; He, J. Montelukast Prevents Mice Against Acetaminophen-Induced Liver Injury. Front. Pharmacol. 2019, 10, 1070. [Google Scholar] [CrossRef]
- El-Kashef, D.H.; Zaghloul, R.A. Ameliorative effect of montelukast against carbon tetrachloride-induced hepatotoxicity: Targeting NLRP3 inflammasome pathway. Life Sci. 2022, 304, 120707. [Google Scholar] [CrossRef] [PubMed]
- El-Baz, A.M.; Shata, A.; Hassan, H.M.; El-Sokkary, M.M.A.; Khodir, A.E. The therapeutic role of lactobacillus and montelukast in combination with metformin in diabetes mellitus complications through modulation of gut microbiota and suppression of oxidative stress. Int. Immunopharmacol. 2021, 96, 107757. [Google Scholar] [CrossRef]
- Sripradha, R.; Sridhar, M.G.; Maithilikarpagaselvi, N. Antihyperlipidemic and antioxidant activities of the ethanolic extract of Garcinia cambogia on high fat diet-fed rats. J. Complement. Integr. Med. 2016, 13, 9–16. [Google Scholar] [CrossRef]
- Attia, R.T.; Abdel-Mottaleb, Y.; Abdallah, D.M.; El-Abhar, H.S.; El-Maraghy, N.N. Raspberry ketone and Garcinia Cambogia rebalanced disrupted insulin resistance and leptin signaling in rats fed high fat fructose diet. Biomed. Pharmacother. 2019, 110, 500–509. [Google Scholar] [CrossRef]
- Han, J.H.; Park, M.H.; Myung, C.S. Garcinia cambogia Ameliorates Non-Alcoholic Fatty Liver Disease by Inhibiting Oxidative Stress-Mediated Steatosis and Apoptosis through NRF2-ARE Activation. Antioxidants 2021, 10, 1226. [Google Scholar] [CrossRef] [PubMed]
- Asghar, M.; Monjok, E.; Kouamou, G.; Ohia, S.E.; Bagchi, D.; Lokhandwala, M.F. Super CitriMax (HCA-SX) attenuates increases in oxidative stress, inflammation, insulin resistance, and body weight in developing obese Zucker rats. Mol. Cell Biochem. 2007, 304, 93–99. [Google Scholar] [CrossRef]
- Sripradha, R.; Sridhar, M.G.; Maithilikarpagaselvi, N. Hydroxycitric acid ameliorates high-fructose-induced redox imbalance and activation of stress sensitive kinases in male Wistar rats. J. Basic. Clin. Physiol. Pharmacol. 2016, 27, 349–356. [Google Scholar] [CrossRef]
- Jung, T.Y.; Lee, A.Y.; Song, J.H.; Lee, M.Y.; Lim, J.O.; Lee, S.J.; Ko, J.W.; Shin, N.R.; Kim, J.C.; Shin, I.S.; et al. Scrophularia koraiensis Nakai Attenuates Allergic Airway Inflammation via Suppression of NF-κB and Enhancement of Nrf2/HO-1 Signaling. Antioxidants 2020, 9, 99. [Google Scholar] [CrossRef] [PubMed]
- Weerachayaphorn, J.; Amaya, M.J.; Spirli, C.; Chansela, P.; Mitchell-Richards, K.A.; Ananthanarayanan, M.; Nathanson, M.H. Nuclear Factor, Erythroid 2-Like 2 Regulates Expression of Type 3 Inositol 1,4,5-Trisphosphate Receptor and Calcium Signaling in Cholangiocytes. Gastroenterology 2015, 149, 211–222.e210. [Google Scholar] [CrossRef] [PubMed]
- Vuppalanchi, R.; Bonkovsky, H.L.; Ahmad, J.; Barnhart, H.; Durazo, F.; Fontana, R.J.; Gu, J.; Khan, I.; Kleiner, D.E.; Koh, C.; et al. Garcinia cambogia, Either Alone or in Combination With Green Tea, Causes Moderate to Severe Liver Injury. Clin. Gastroenterol. Hepatol. 2022, 20, e1416–e1425. [Google Scholar] [CrossRef]
- Anaya-Morua, W.; Villafan-Bernal, J.R.; Ramírez-Moreno, E.; García-Ortiz, H.; Martínez-Portilla, R.J.; Contreras-Cubas, C.; Martínez-Hernández, A.; Centeno-Cruz, F.; Pedroza-Montoya, F.E.; Orozco, L.; et al. Total Antioxidant Capacity in Obese and Non-Obese Subjects and Its Association with Anthropo-Metabolic Markers: Systematic Review and Meta-Analysis. Antioxidants 2023, 12, 1512. [Google Scholar] [CrossRef]
- García-Sánchez, A.; Miranda-Díaz, A.G.; Cardona-Muñoz, E.G. The Role of Oxidative Stress in Physiopathology and Pharmacological Treatment with Pro- and Antioxidant Properties in Chronic Diseases. Oxidative Med. Cell. Longev. 2020, 2020, 2082145. [Google Scholar] [CrossRef]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Gender/ Age n/ID References | Adverse Reaction | Product | Reason for Use | Latency/Treatment Duration (Days) | Laboratory Data a | Seriousness | Other Medications/ Other Diseases | Outcome | Dechallenge/Rechallenge |
|---|---|---|---|---|---|---|---|---|---|
| F/45 1/275 [35] | Massive hepatic necrosis, acute hepatic failure | 1. Top line advantra Z 2. Kalo rapido | Weight loss | 1. 15/8 2. NR/NR | AST > 1000 ALT 2512 TB 5.7 GGT 31 | H | Montelukast/Hepatic steatosis | D | 1. NR/NR 2. NR/NR |
| F/39 2/309 | Acute hepatitis | 1. Peso stop 2. Magrixs | Weight loss | 1. 55/54 2. 213/522 | AST-ALT > 3000, Bilirubin 30 Virus markers: negative | H | NR/NR | CR | 1. +/NR 2. +/NR |
| F/39 3/1080 [22] | Cholestatic hepatitis | 1. Obless 2. Citrus aurantium 6%, Rhodiola, Orthosiphon | Weight loss | 1. 40/30 2. 40/30 | AST 1682 ALT 1868 TB 14.79 DB 13.17 | H | Metildopa/Metabolic syndrome | P | 1. NR/NR 2. NR/NR |
| F/61 4/1382 [22] | Cholestatic hepatitis | Super ananas slim | Weight loss | NR/NR | AST 1071 ALT 1625 | H | NR/NR | CR | +/NR |
| F/52 5/1389 [22] | Acute hepatitis | 1. G. cambogia 2. Green coffee | Weight loss | 1. NR/NR 2. NR/NR | AST 1442 ALT 1819 TB 14.7 GGT 223 Virus markers: negative | NR | NO/NR | CR | 1. +/NR 2. +/NR |
| F/47 6/1415 [22] | Abdominal pain, hepatomegaly, acute hepatitis | Herbalife, thermo giallo | Weight loss | NR/NR | AST 67 ALT 266 TB 0.7 | H | Levothyroxine/Hypertension, hypothyroidism, obesity | CR | +/NR |
| F/57 7/1853 | Acute hepatitis | 1. CRCMN-P 2. Garcinia 1000 3. Piperina and Curcuma | Weight loss | 1. 30/NR 2. 30/NR 3. 15/15 | ALT 2291 TB 7.5 | H | Eliquis, Almarytm, Eutirox, Lasix /Hypothyroidism, atrial fibrillation | R | 1. +/NR 2. +/NR 3. +/NR |
| F/42 8/1988 | Jaundice, asthenia, nausea anorexia | Garcinia body slim | NR | NR/NR | ALT 2388 TB 3.5 GGT 341 | H | NR/Papillary thyroid carcinoma with hypothyroidism; bronchial asthma | R | NR/NR |
| n/ID | Product Name | Composition |
|---|---|---|
| 1/275 | 1. Top line advantra Z | 1. Advantra ZTM Citrus aurantium fruit peel d.e. (dry extract) 6% synephrine; Garcinia cambogia fruit peel d.e. 60% hydroxycitric acid; L-phenylalanine; Gymnema silvestris leaves d.e. 25% gymnemic acid; L-carnitine hydrochloride; Phaseolus vulgaris bean pod d.e. |
| 2. Kalo rapido | 2. Hydrolyzed collagen; sodium hyaluronate; Betula alba leaf extract; Citrus aurantium leaf extract; Magnolia officinalis bark extract; Bambusa vulgaris leaf extract; glutamine; L-orthine; magnesium pyruvate. | |
| 2/309 | 1. Peso stop | 1. Green tea leaves d.e. 5% caffeine; Gymnema silvestre leaves d.e. 26% gymnemic acids; bean protein concentrate (phaseolamine); pineapple fruit d.e. enzymatic activity 250 GDU/g; Clarinol natural concentrate of omega 6 fatty acids; conjugated linoleic acid (CLA) from vegetable oils; choline bitartrate; inositol; L-carnitine; cinnamon bark d.e. 1.6% MHCP (methylhydroxycalcalone polymer); green coffee seed d.e. 50% chlorogenic acid; bioperine (Piper nigrum) fruit d.e. 95% in piperine. |
| 2. Magrixs | 2. Thermal water from the Montegrimano spa; green tea (Camellia sinensis) leaves; Garcinia (Garcinia cambogia) fruit; pineapple (Ananas sativa) stem; fennel (Foeniculum vulgare) seeds; orthosiphon (Ortosiphon stamineus) leaves; burdock (Arctium lappa) root; Cassia nomame (Cassia mimosoides) plant d.e. 8% (2s)-3,4,7-trihydroxyflavan-(4 beta − 8) catechin; banaba (Lagerstroemia speciosa) leaves d.e. 1% corosolic acid. | |
| 3/1080 | 1. Obless | 1. Citrus (Citrus aurantium var. amara L., fruit) d.e. 10% synephrine (equal to a content of 14 mg) 140 mg; Garcinia (Garcinia cambogia Desr., fruit) d.e. 60% hydroxycitric acid (equal to a content of 72 mg) 120 mg; Ortosifon (Orthosiphon stamineus Benth, leaves) d.e. 0.2% sinensetin (equal to a content of 0.2 mg.) 100 mg; Griffonia simplicifolia Baill., seeds d.e. 99% 5-hydroxy-L-tryptophan (equal to a content of 75 mg) 75 mg. |
| 2. Citrus aurantium 6%, rhodiola, orthosiphon | 2. Citrus aurantium 6%; rhodiola; orthosiphon. | |
| 4/1382 | Super ananas slim | Pineapple concentrated juice (Ananas comosus (L.) Merr.) fruit; pineapple (Ananas comosus (L.) Merr.) stem d.e. 250 GDU/g bromelain; mate (Ilex paraguariensis A. St. Hill.) leaf d.e. 2% caffeine; garcinia cambogia (Garcinia cambogia (gaernt) Desr.) fruit d.e. 60% hydroxycitric acid; pineapple (Ananas comosus (L.) Merr.) stem d.e. 2500 GDU/g bromelain. |
| 5/1389 | 1. Garcinia cambogia 2. Green coffee | 1. Garcinia cambogia extract 400 mg 60% hydroxycitric acid (240 mg). 2. Green Coffee extract 400 mg 50% chlorogenic acid (200 mg). |
| 6/1415 | Herbalife, thermo giallo | Garcinia cambogia extract; chromium chloride. |
| 7/1853 | 1. CRCMN-P 2. Garcinia 1000 3. Piperina and Curcuma | 1. Unknown composition 2. Garcinia not otherwise specified 3. Turmeric (Curcuma longa root, 360 mg) d.e. 95% curcuminoids; turmeric (Curcuma longa root powder, 360 mg); black pepper (Piper nigrum fruit, 80 mg) d.e. 95% piperine. |
| 8/1988 | Garcinia body slim | Inulin 500 mg; garcinia fruit d.e. 300 mg of which 180 mg hydroxycitric acid; green tea 20 mg; coleus d.e. 20 mg; gymnema d.e. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Di Giacomo, S.; Di Sotto, A.; Percaccio, E.; Scuotto, E.; Battistelli, C.; Mazzanti, G.; Menniti-Ippolito, F.; Ippoliti, I. Interaction of Garcinia cambogia (Gaertn.) Desr. and Drugs as a Possible Mechanism of Liver Injury: The Case of Montelukast. Antioxidants 2023, 12, 1771. https://doi.org/10.3390/antiox12091771
Di Giacomo S, Di Sotto A, Percaccio E, Scuotto E, Battistelli C, Mazzanti G, Menniti-Ippolito F, Ippoliti I. Interaction of Garcinia cambogia (Gaertn.) Desr. and Drugs as a Possible Mechanism of Liver Injury: The Case of Montelukast. Antioxidants. 2023; 12(9):1771. https://doi.org/10.3390/antiox12091771
Chicago/Turabian StyleDi Giacomo, Silvia, Antonella Di Sotto, Ester Percaccio, Erica Scuotto, Cecilia Battistelli, Gabriela Mazzanti, Francesca Menniti-Ippolito, and Ilaria Ippoliti. 2023. "Interaction of Garcinia cambogia (Gaertn.) Desr. and Drugs as a Possible Mechanism of Liver Injury: The Case of Montelukast" Antioxidants 12, no. 9: 1771. https://doi.org/10.3390/antiox12091771