
Enhancing the Differentiation between Intestinal Behçet’s Disease and Crohn’s Disease through Quantitative Computed Tomography Analysis

Abstract
:
1. Introduction
2. Materials and Methods
2.1. Patients
2.2. Assessment Items
2.3. Quantification of Body Composition Parameters Based on CTE
2.4. Imaging Technique
2.5. Statistical Analysis
3. Results
3.1. Clinical Date
3.2. Laboratory Results
3.3. Endoscopic Characteristics
3.4. Image Features
3.5. Body Composition Analysis
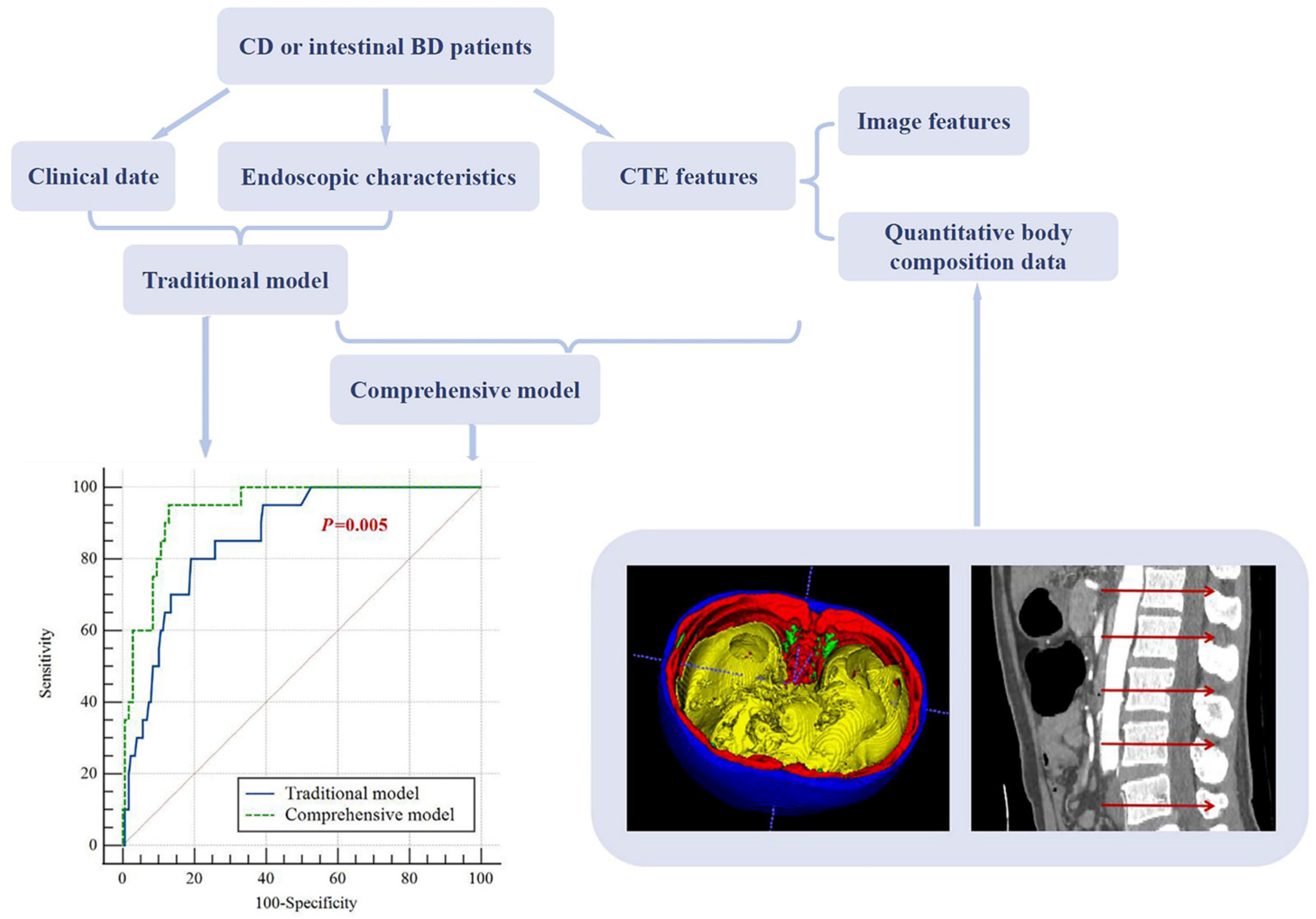
3.6. Identification Models
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Hatemi, G.; Yazici, Y.; Yazici, H. Behçet’s syndrome. Rheum. Dis. Clin. N. Am. 2013, 39, 245–261. [Google Scholar] [CrossRef]
- Mahr, A.; Maldini, C. Epidemiology of Behçet’s disease. Rev. Med. Interne 2014, 35, 81–89. [Google Scholar] [CrossRef] [PubMed]
- Peker, E.; Erden, A.; Erden, İ.; Düzgün, N. Intestinal Behçet Disease: Evaluation with MR Enterography—A Case-Control Study. AJR Am. J. Roentgenol. 2018, 211, 767–775. [Google Scholar] [CrossRef]
- Kim, D.H.; Cheon, J.H. Intestinal Behçet’s Disease: A True Inflammatory Bowel Disease or Merely an Intestinal Complication of Systemic Vasculitis? Yonsei Med. J. 2016, 57, 22–32. [Google Scholar] [CrossRef] [PubMed]
- International Study Group for Behçet’s Disease. Criteria for diagnosis of Behçet’s disease. Lancet 1990, 335, 1078–1080. [Google Scholar]
- Cheon, J.H.; Kim, E.S.; Shin, S.J.; Kim, T.I.; Lee, K.M.; Kim, S.W.; Kim, J.S.; Kim, Y.S.; Choi, C.H.; Ye, B.D.; et al. Development and validation of novel diagnostic criteria for intestinal Behçet’s disease in Korean patients with ileocolonic ulcers. Am. J. Gastroenterol. 2009, 104, 2492–2499. [Google Scholar] [CrossRef]
- Valenti, S.; Gallizzi, R.; De Vivo, D.; Romano, C. Intestinal Behçet and Crohn’s disease: Two sides of the same coin. Pediatr. Rheumatol. Online J. 2017, 15, 33. [Google Scholar] [CrossRef]
- Ebert, E.C. Gastrointestinal manifestations of Behçet’s disease. Dig. Dis. Sci. 2009, 54, 201–207. [Google Scholar] [CrossRef]
- Jung, Y.S.; Cheon, J.H.; Park, S.J.; Hong, S.P.; Kim, T.I.; Kim, W.H. Long-term clinical outcomes of Crohn’s disease and intestinal Behcet’s disease. Inflamm. Bowel Dis. 2013, 19, 99–105. [Google Scholar] [CrossRef]
- Zhang, T.; Hong, L.; Wang, Z.; Fan, R.; Zhang, M.; Lin, Y.; Cheng, M.; Zhou, X.; Sun, P.; Lin, X.; et al. Comparison between Intestinal Behçet’s Disease and Crohn’s Disease in Characteristics of Symptom, Endoscopy, and Radiology. Gastroenterol. Res. Pract. 2017, 2017, 3918746. [Google Scholar] [CrossRef]
- Rocha, R.; Santana, G.O.; Almeida, N.; Lyra, A.C. Analysis of fat and muscle mass in patients with inflammatory bowel disease during remission and active phase. Br. J. Nutr. 2009, 101, 676–679. [Google Scholar] [CrossRef]
- Yuan, G.; He, Y.; Cao, Q.-H.; Tang, M.-M.; Xie, Z.-L.; Qiu, Y.; Zeng, Z.-R.; Peng, S.; Chen, M.-H. Visceral adipose volume is correlated with surgical tissue fibrosis in Crohn’s disease of the small bowel. Gastroenterol. Rep. 2022, 10, goac044. [Google Scholar] [CrossRef] [PubMed]
- Holt, D.Q.; Moore, G.T.; Strauss, B.J.G.; Hamilton, A.L.; De Cruz, P.; Kamm, M.A. Visceral adiposity predicts post-operative Crohn’s disease recurrence. Aliment. Pharmacol. Ther. 2017, 45, 1255–1264. [Google Scholar] [CrossRef]
- Büning, C.; von Kraft, C.; Hermsdorf, M.; Gentz, E.; Wirth, E.K.; Valentini, L.; Haas, V. Visceral Adipose Tissue in Patients with Crohn’s Disease Correlates with Disease Activity, Inflammatory Markers, and Outcome. Inflamm. Bowel Dis. 2015, 21, 2590–2597. [Google Scholar] [CrossRef] [PubMed]
- Yang, H.; Zhang, H.; Liu, W.; Han, W.; Guo, T.; Lai, Y.; Tan, B.; Wang, C.; Chen, M.; Gao, X.; et al. Computed tomography enterography increases the ability of endoscopy to differentiate Crohn’s disease from intestinal Behçet’s disease. Front. Med. 2022, 9, 900458. [Google Scholar] [CrossRef]
- Bernstein, C.N.; Eliakim, A.; Fedail, S.; Fried, M.; Gearry, R.; Goh, K.-L.; Hamid, S.; Khan, A.G.; Khalif, I.; Ng, S.C.; et al. World Gastroenterology Organisation Global Guidelines Inflammatory Bowel Disease: Update August 2015. J. Clin. Gastroenterol. 2016, 50, 803–818. [Google Scholar] [CrossRef]
- Li, J.; Li, P.; Bai, J.; Lyu, H.; Li, Y.; Yang, H.; Shen, B.; Qian, J.-M. Discriminating potential of extraintestinal systemic manifestations and colonoscopic features in Chinese patients with intestinal Behçet’s disease and Crohn’s disease. Chin. Med. J. 2015, 128, 233–238. [Google Scholar] [CrossRef] [PubMed]
- Bruining, D.H.; Zimmermann, E.M.; Loftus, E.V.; Sandborn, W.J.; Sauer, C.G.; Strong, S.A. Consensus Recommendations for Evaluation, Interpretation, and Utilization of Computed Tomography and Magnetic Resonance Enterography in Patients with Small Bowel Crohn’s Disease. Radiology 2018, 286, 776–799. [Google Scholar] [CrossRef]
- Shi, L.; Wang, Y.-d.; Shen, X.-d.; Mao, R.; Meng, J.-X.; Huang, S.-Y.; Song, T.; Li, Z.-P.; Feng, S.-T.; Lin, S.-C.; et al. Clinical outcome is distinct between radiological stricture and endoscopic stricture in ileal Crohn’s disease. Eur. Radiol. 2023. online ahead of print. [Google Scholar] [CrossRef]
- Xiong, Z.; Zhou, Z.; Hao, L.; Li, Y.; Hu, X.; Hu, D.; Luo, Y.; Wang, Y.; Shen, Y.; Li, Z. The relationship between perianal fistula activity and abdominal adipose tissue in Crohn’s disease: An observational study. Insights Imaging 2022, 13, 156. [Google Scholar] [CrossRef]
- Taylor, S.A.; Avni, F.; Cronin, C.G.; Hoeffel, C.; Kim, S.H.; Laghi, A.; Napolitano, M.; Petit, P.; Rimola, J.; Tolan, D.J.; et al. The first joint ESGAR/ESPR consensus statement on the technical performance of cross-sectional small bowel and colonic imaging. Eur. Radiol. 2017, 27, 2570–2582. [Google Scholar] [CrossRef]
- Feng, R.; Chao, K.; Chen, S.L.; Sun, C.H.; Qiu, Y.; Chen, B.L.; Mao, R.; He, Y.; Cao, Q.H.; Xue, L.; et al. Heat shock protein family A member 6 combined with clinical characteristics for the differential diagnosis of intestinal Behçet’s disease. J. Dig. Dis. 2018, 19, 350–358. [Google Scholar] [CrossRef] [PubMed]
- Ye, J.-F.; Guan, J.-L. Differentiation between intestinal Behçet’s disease and Crohn’s disease based on endoscopy. Turk. J. Med. Sci. 2019, 49, 42–49. [Google Scholar] [CrossRef]
- Ma, L.; Wang, M.; Li, W.; Liu, W.; Yang, H.; Jiang, Y.; Zhu, Q. Pilot case-control study to explore the value of intestinal ultrasound in the differentiation of two common diseases involving the ileocecal region: Intestinal Behçet’s disease and Crohn’s disease. Quant. Imaging Med. Surg. 2021, 11, 3200–3208. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.K.; Kim, B.K.; Kim, T.I.; Kim, W.H. Differential diagnosis of intestinal Behçet’s disease and Crohn’s disease by colonoscopic findings. Endoscopy 2009, 41, 9–16. [Google Scholar] [CrossRef] [PubMed]
- Fernandes, T.; Oliveira, M.I.; Castro, R.; Araújo, B.; Viamonte, B.; Cunha, R. Bowel wall thickening at CT: Simplifying the diagnosis. Insights Imaging 2014, 5, 195–208. [Google Scholar] [CrossRef] [PubMed]
- Bettenworth, D.; Bokemeyer, A.; Baker, M.; Mao, R.; Parker, C.E.; Nguyen, T.; Ma, C.; Panés, J.; Rimola, J.; Fletcher, J.G.; et al. Assessment of Crohn’s disease-associated small bowel strictures and fibrosis on cross-sectional imaging: A systematic review. Gut 2019, 68, 1115–1126. [Google Scholar] [CrossRef]
- Kedia, S.; Madhusudhan, K.S.; Sharma, R.; Bopanna, S.; Yadav, D.P.; Goyal, S.; Jain, S.; Das, P.; Dattagupta, S.; Makharia, G.; et al. Combination of increased visceral fat and long segment involvement: Development and validation of an updated imaging marker for differentiating Crohn’s disease from intestinal tuberculosis. J. Gastroenterol. Hepatol. 2018, 33, 1234–1241. [Google Scholar] [CrossRef]
- Seetharaman, J.; Srivastava, A.; Yadav, R.R.; Singh, S.K.; Mishra, P.; Sen Sarma, M.; Poddar, U. Visceral fat indices: Do they help differentiate Crohn’s disease and Intestinal tuberculosis in children? J. Crohns Colitis 2023. online ahead of print. [Google Scholar] [CrossRef]
- Zhou, Z.L.; Xiong, Z.M.; Xie, Q.G.; Xiao, P.; Zhang, Q.P.; Gu, J.; Li, J.; Hu, D.Y.; Hu, X.M.; Shen, Y.Q.; et al. Computed tomography-based multiple body composition parameters predict outcomes in Crohn’s disease. Insights Imaging 2021, 12, 135. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Item | Intestinal BD (n = 20) | CD (n = 179) | p Value |
|---|---|---|---|
| Sex (male/female) | 11/9 | 143/36 | 0.025 |
| Age (year) | 38.00 (33.25, 47.75) | 27.00 (23.00, 34.00) | <0.001 |
| Disease course (month) | 3.00 (1.00, 12.00) | 10.00 (2.00, 24.00) | 0.059 |
| Abdominal pain | 16 (80.0%) | 143 (79.9%) | >0.99 |
| Diarrhea | 7 (35.0%) | 137 (76.5%) | <0.001 |
| Fever | 3 (15.0%) | 36 (20.2%) | 0.794 |
| Weight loss | 8 (40.0%) | 83 (46.4%) | 0.588 |
| Gastrointestinal bleeding | 11 (55.0%) | 108 (60.3%) | 0.644 |
| Oral ulcer | 16 (80.0%) | 10 (5.6%) | <0.001 |
| Genital ulcer | 8 (40.0%) | 0 | <0.001 |
| Intestinal symptoms as primary manifestation | 6 (30.0%) | 166 (93.3%) | <0.001 |
| Perianal lesion | 0 | 109 (60.9%) | <0.001 |
| CRP (mg/L) | 11.50 (2.48, 34.93) | 25.00 (10.50, 48.00) | 0.014 |
| ESR (mm/h) | 16.00 (10.00, 28.75) | 23.00 (13.00, 40.00) | 0.149 |
| Albumin (g/L) | 39.33 ± 6.41 | 37.20 ± 6.54 | 0.168 |
| Range of albumin | 22.5–50.6 | 21.2–67.9 | |
| Hemoglobin (g/L) | 113.80 ± 22.00 | 115.58 ± 22.66 | 0.739 |
| Endoscope type | |||
| Small intestine endoscopy | 3 | 40 | |
| Colonoscopy | 18 | 145 | |
| Longitudinal ulcer | 1 (5.0%) | 78 (43.6%) | <0.001 |
| Ulcer distribution | 0.001 | ||
| Focal | 15 (75.0%) | 51 (28.5%) | |
| Segmental | 5 (25.0%) | 128 (71.5%) | |
| Ileocecal valve deformity | 9 (45.0%) | 56 (31.3%) | 0.215 |
| Noncaseating granuloma | 2 (10.0%) | 100 (56.2%) | <0.001 |
| Item | Intestinal BD (n = 20) | CD (n = 179) | p Value | Kappa Value |
|---|---|---|---|---|
| Pattern of bowel wall thickening | <0.001 | 0.755 | ||
| Polypoid | 10 (50.0%) | 19(10.6%) | ||
| Homogeneous | 10 (50.0%) | 160 (89.4%) | ||
| Enhancement pattern | 0.314 | 0.824 | ||
| Layered | 11 (55.0%) | 123 (68.7%) | ||
| Homogeneous | 9 (45.0%) | 56 (31.3%) | ||
| Intestinal segment involvement | ||||
| Jejunum | 1 (5.0%) | 17 (9.5%) | 0.799 | 0.939 |
| Proximal ileum | 1 (5.0%) | 82 (45.8%) | <0.001 | 0.878 |
| Terminal ileum | 12 (60.0%) | 135 (75.4%) | 0.137 | 0.884 |
| Cecum | 16 (80.0%) | 119 (66.5%) | 0.220 | 0.884 |
| Colorectum | 9 (45.0%) | 118 (65.9%) | 0.065 | 0.934 |
| Ascending colon | 9 (45.0%) | 81 (45.3%) | 0.983 | 0.980 |
| Transverse colon | 0 | 77 (43.0%) | <0.001 | 0.958 |
| Descending colon | 0 | 67 (37.4%) | 0.001 | 0.966 |
| Sigmoid colon | 0 | 72 (40.2%) | <0.001 | 0.968 |
| Rectum | 0 | 55 (30.7%) | 0.004 | 0.889 |
| Asymmetrical thickening of bowel wall | 3(15.0%) | 74 (41.3%) | 0.022 | 0.836 |
| Comb sign | 6 (30.0%) | 134 (74.9%) | <0.001 | 0.803 |
| Intestinal stenosis | 3 (15.0%) | 80 (44.7%) | 0.011 | 0.813 |
| Penetration (sinus, fistula, abscess) | 3 (15.0%) | 11 (6.1%) | 0.314 | 0.802 |
| Item | Intestinal BD (n = 20) | CD (n = 179) | p Value |
|---|---|---|---|
| VSRL1 | 0.86 (0.43, 1.78) | 1.26 (0.59, 3.51) | 0.086 |
| VSRL2 | 0.91 (0.37, 1.47) | 1.11 (0.64, 2.00) | 0.063 |
| VSRL3 | 0.75 (0.35, 1.17) | 0.91 (0.37, 1.47) | 0.088 |
| VSRL4 | 0.68 (0.37, 0.96) | 0.81 (0.54, 1.40) | 0.046 |
| VSRL5 | 0.59 (0.36, 0.95) | 0.85 (0.54, 1.40) | 0.013 |
| VSRvolume | 0.77 (0.36, 1.11) | 0.97 (0.63, 1.35) | 0.072 |
| CV | 0.23 (0.19, 0.44) | 0.35 (0.25, 0.51) | 0.039 |
| L1 VAT attenuation (HU) | |||
| 25% quartile | −101.65 ± 14.84 | −90.18 ± 16.41 | 0.003 |
| Median | −80.50 (−100.75, −70.00) | −68 (−82.00, −54.00) | 0.003 |
| 75% quartile | −57.00 (−78.25, −41.50) | −41.00 (−54.00, −28.00) | 0.001 |
| L2 VAT attenuation (HU) | |||
| 25% quartile | −100.70 ± 12.77 | −90.69 ± 17.49 | 0.014 |
| Median | −82.15 ± 15.18 | −69.91 ± 18.98 | 0.006 |
| 75% quartile | −56.50 (−75.75, −43.19) | −41.00 (−54.00, −29.00) | 0.001 |
| L3 VAT attenuation (HU) | |||
| 25% quartile | −103.55 ± 12.89 | −93.38 ± 16.86 | 0.010 |
| Median | −84.13 ± 15.71 | −71.84 ± 19.28 | 0.003 |
| 75% quartile | −60.50 (−77.25, −44.75) | −43.00 (−57.00, −30.00) | 0.002 |
| L4 VAT attenuation (HU) | |||
| 25% quartile | −106.90 ± 9.71 | −93.48 ± 17.70 | 0.001 |
| Median | −88.75 ± 12.69 | −71.80 ± 20.10 | <0.001 |
| 75% quartile | −68.00 (−77.50, −53.00) | −42.00 (−58.00, −29.00) | <0.001 |
| L5 VAT attenuation (HU) | |||
| 25% quartile | −101.70 ± 13.29 | −90.13 ± 18.11 | 0.006 |
| Median | −83.15 ± 16.15 | −69.19 ± 20.39 | 0.003 |
| 75% quartile | −59.50 (−79.75, −45.50) | −42.00 (−58.00, −28.00) | 0.001 |
| Item | Traditional Model | Comprehensive Model | ||||
|---|---|---|---|---|---|---|
| p Value | OR | 95% CI | p Value | OR | 95% CI | |
| Age | 0.002 | 1.069 | 1.025–1.116 | 0.016 | 1.060 | 1.011–1.112 |
| Sex (male) | 0.253 | 0.523 | 0.172–1.589 | 0.887 | 0.908 | 0.239–3.456 |
| Ulcer distribution (focal) | 0.001 | 7.020 | 2.290–21.524 | 0.001 | 10.772 | 2.738–42.383 |
| Proximal ileum involvement | 0.007 | 0.045 | 0.005–0.435 | |||
| Asymmetrical thickening of bowel wall | 0.167 | 0.308 | 0.058–1.637 | |||
| Intestinal stenosis | 0.017 | 0.147 | 0.030–0.710 | |||
| Area ratio of L4 VAT/SAT | 0.118 | 0.271 | 0.053–1.391 | |||
| CV | 0.038 | 0.026 | 0.001-0.822 | |||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Li, Y.; Xiong, Z.; Jiang, Y.; Shen, Y.; Hu, X.; Hu, D.; Li, Z. Enhancing the Differentiation between Intestinal Behçet’s Disease and Crohn’s Disease through Quantitative Computed Tomography Analysis. Bioengineering 2023, 10, 1211. https://doi.org/10.3390/bioengineering10101211
Li Y, Xiong Z, Jiang Y, Shen Y, Hu X, Hu D, Li Z. Enhancing the Differentiation between Intestinal Behçet’s Disease and Crohn’s Disease through Quantitative Computed Tomography Analysis. Bioengineering. 2023; 10(10):1211. https://doi.org/10.3390/bioengineering10101211
Chicago/Turabian StyleLi, Yuanqiu, Ziman Xiong, Yuchen Jiang, Yaqi Shen, Xuemei Hu, Daoyu Hu, and Zhen Li. 2023. "Enhancing the Differentiation between Intestinal Behçet’s Disease and Crohn’s Disease through Quantitative Computed Tomography Analysis" Bioengineering 10, no. 10: 1211. https://doi.org/10.3390/bioengineering10101211