
Carbonic Anhydrase IX Expression and Treatment Response Measured in Rectal Adenocarcinoma Following Neoadjuvant Chemo-Radiotherapy


Abstract
1. Introduction
2. Results
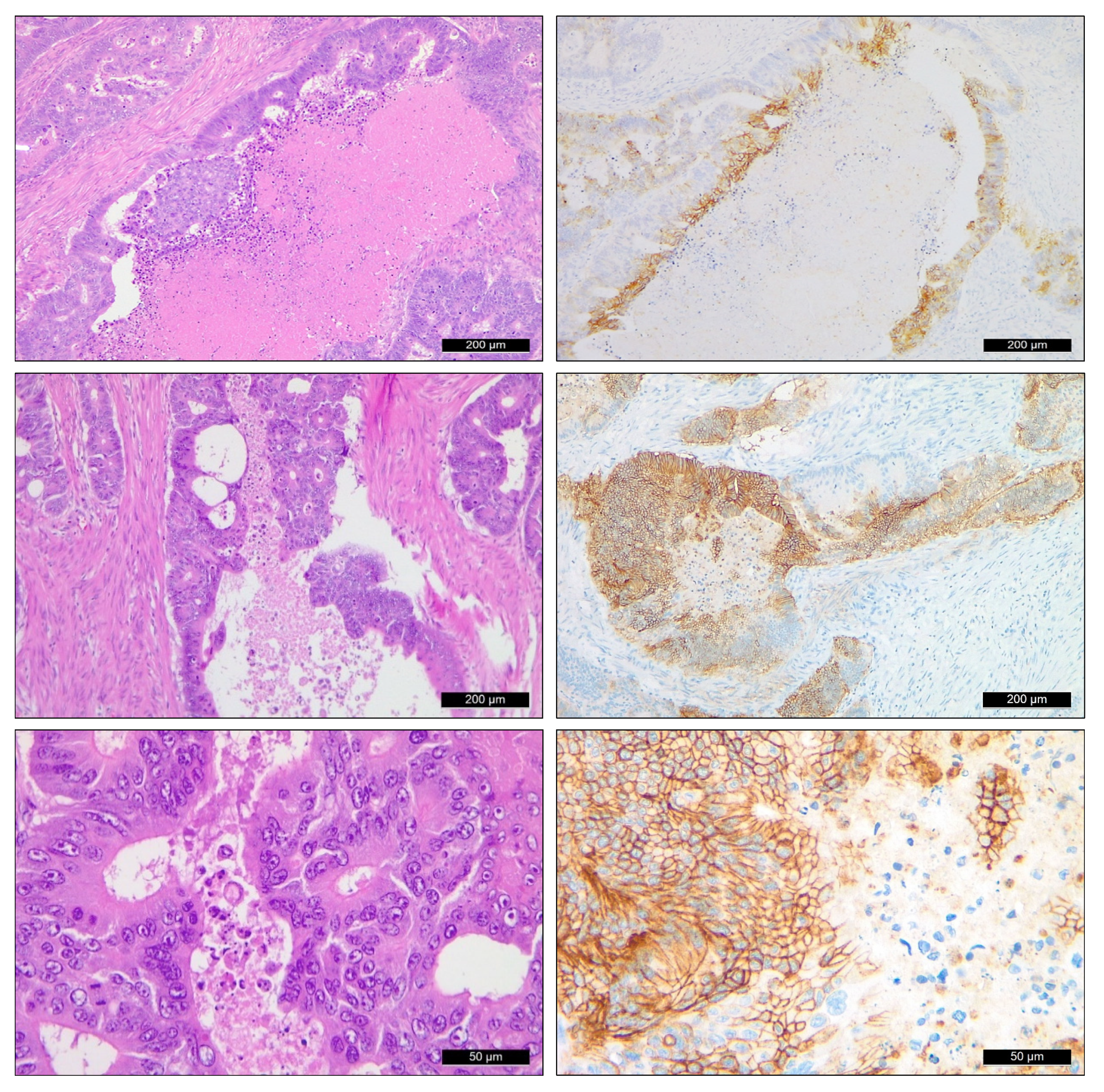
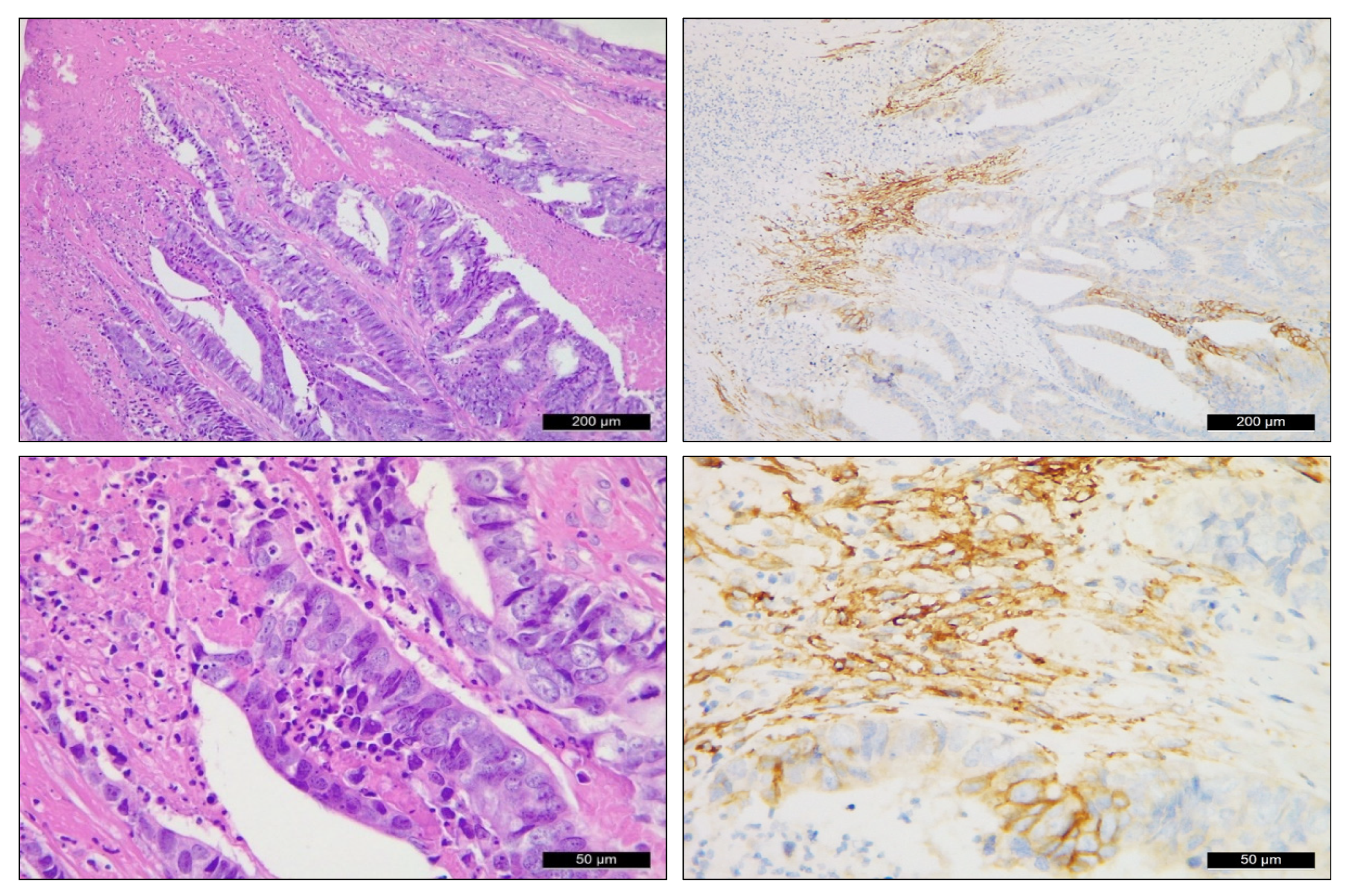
2.1. CAIX Expression Pattern in Rectal Adenocarcinoma Samples
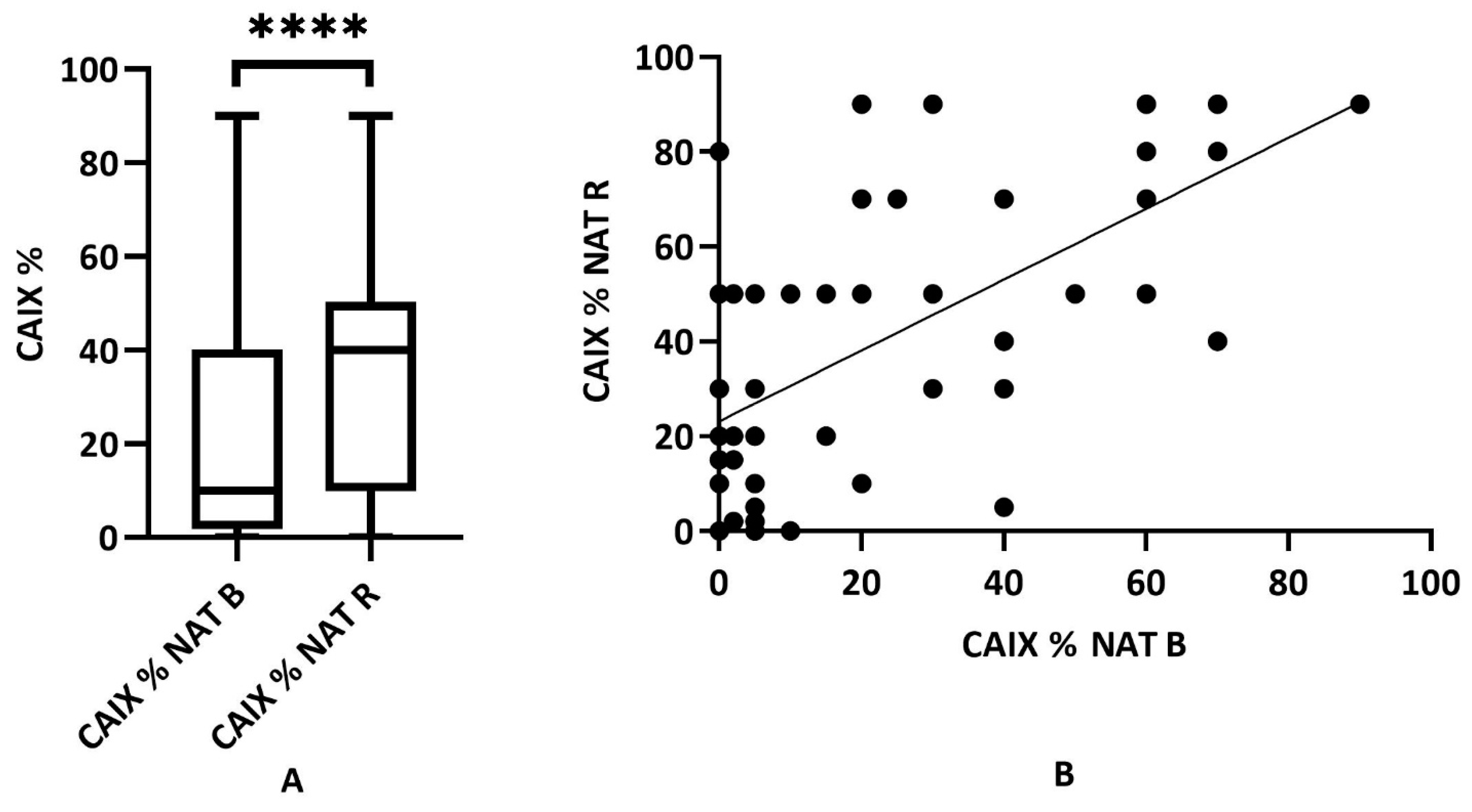
2.2. Expression Dynamics of CAIX in Neoadjuvant-Treated Rectal (NAT) Adenocarcinomas (n = 55)
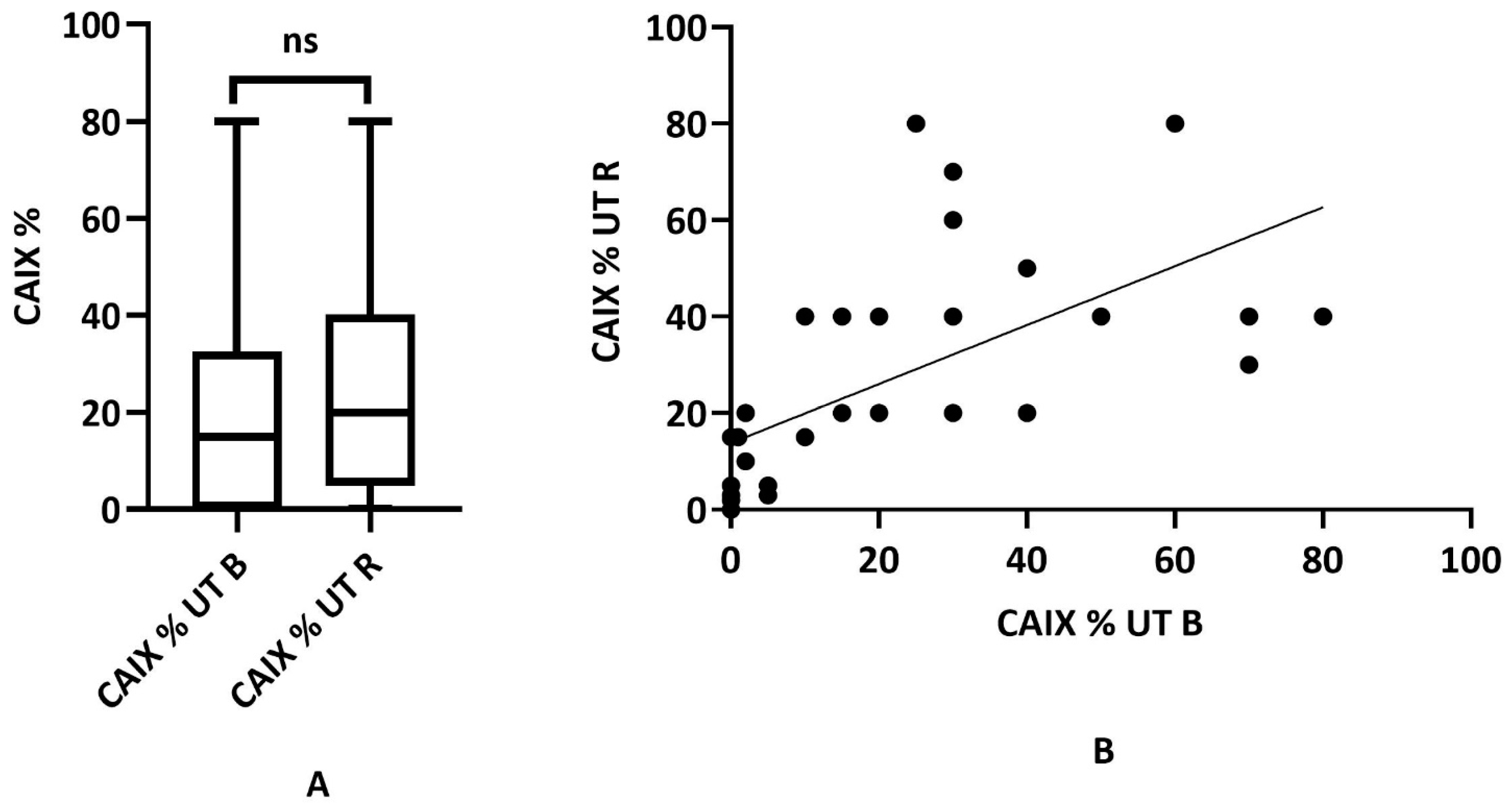
2.3. Immunohistochemical CAIX Expression of Untreated (UT) Rectal Adenocarcinoma (n = 34)
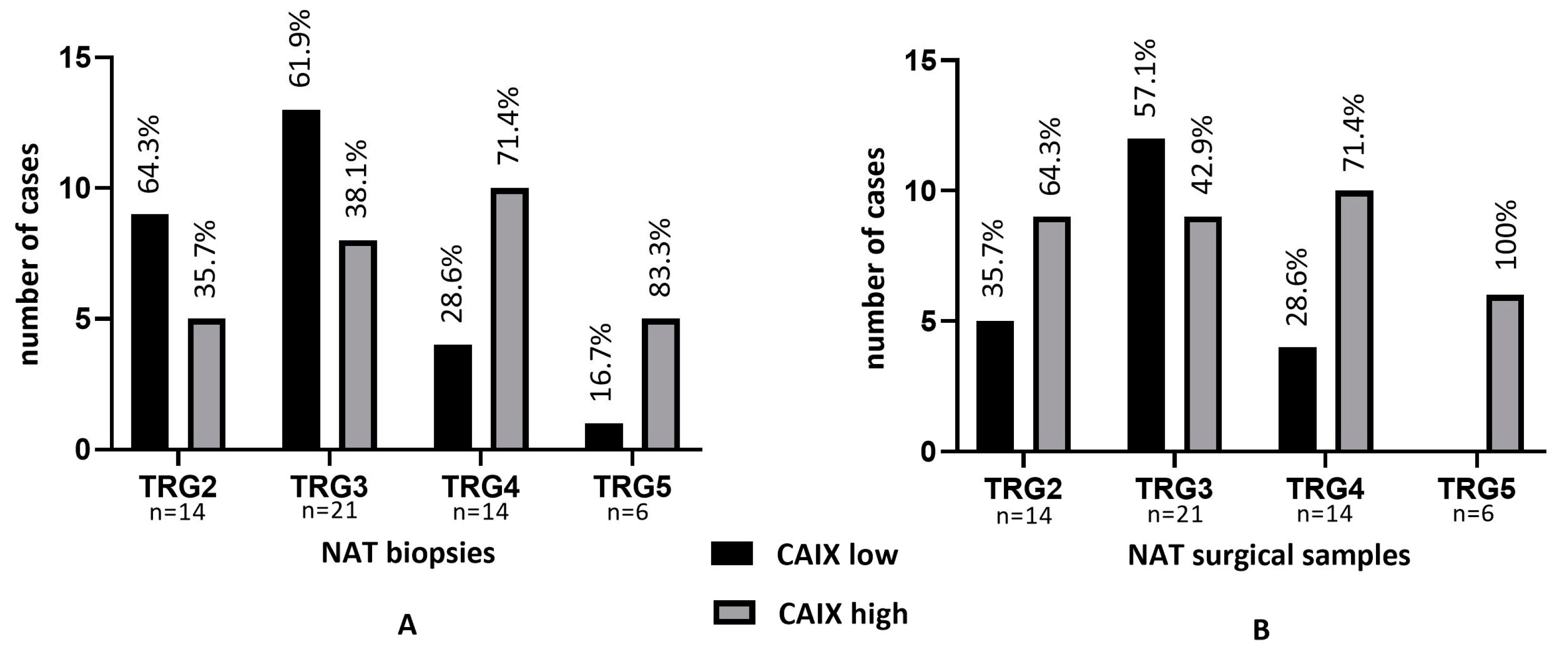
2.4. Tumor Regression Grade and CAIX in NAT Biopsy and NAT Surgical Specimens (n = 55)
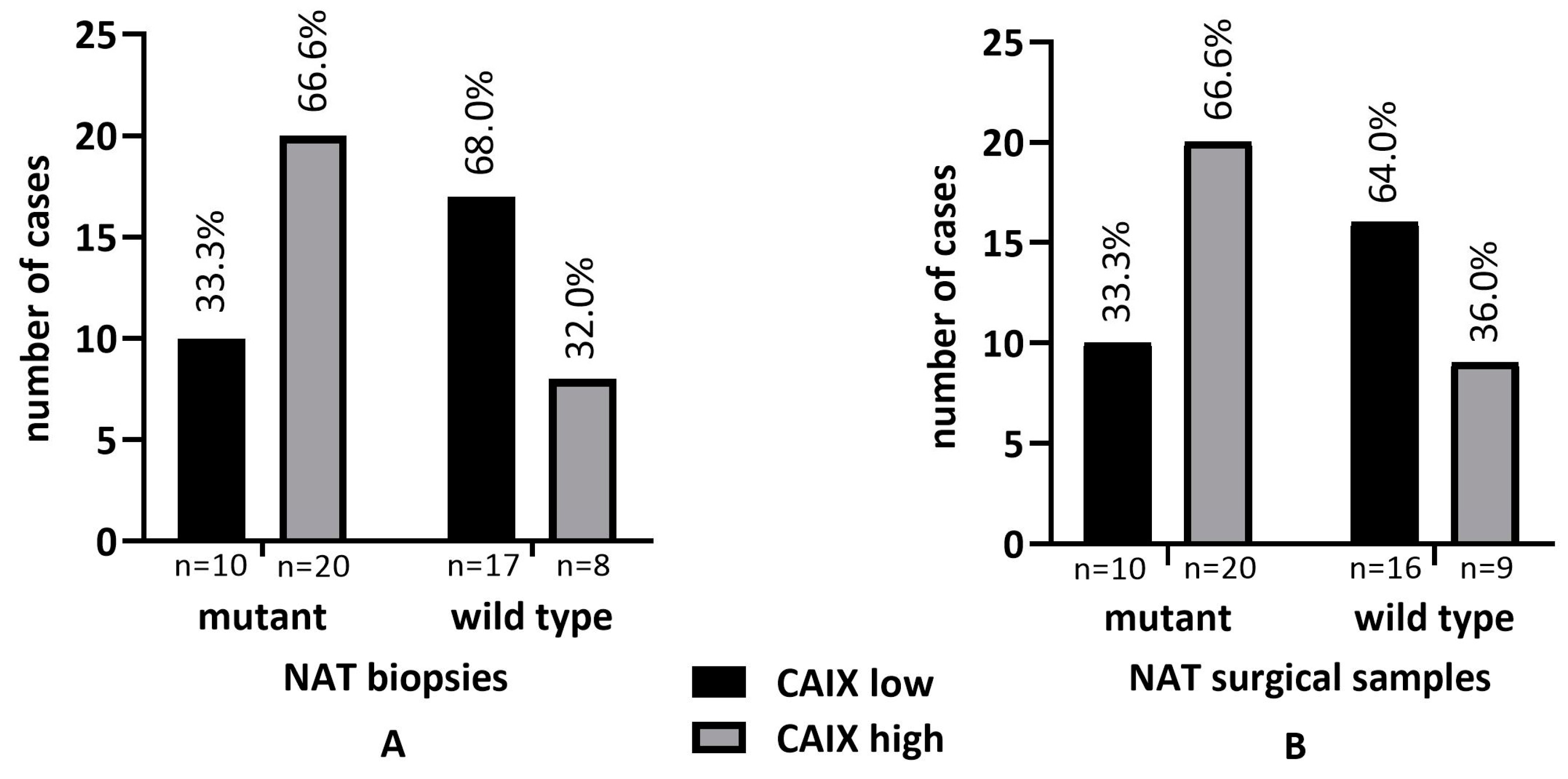
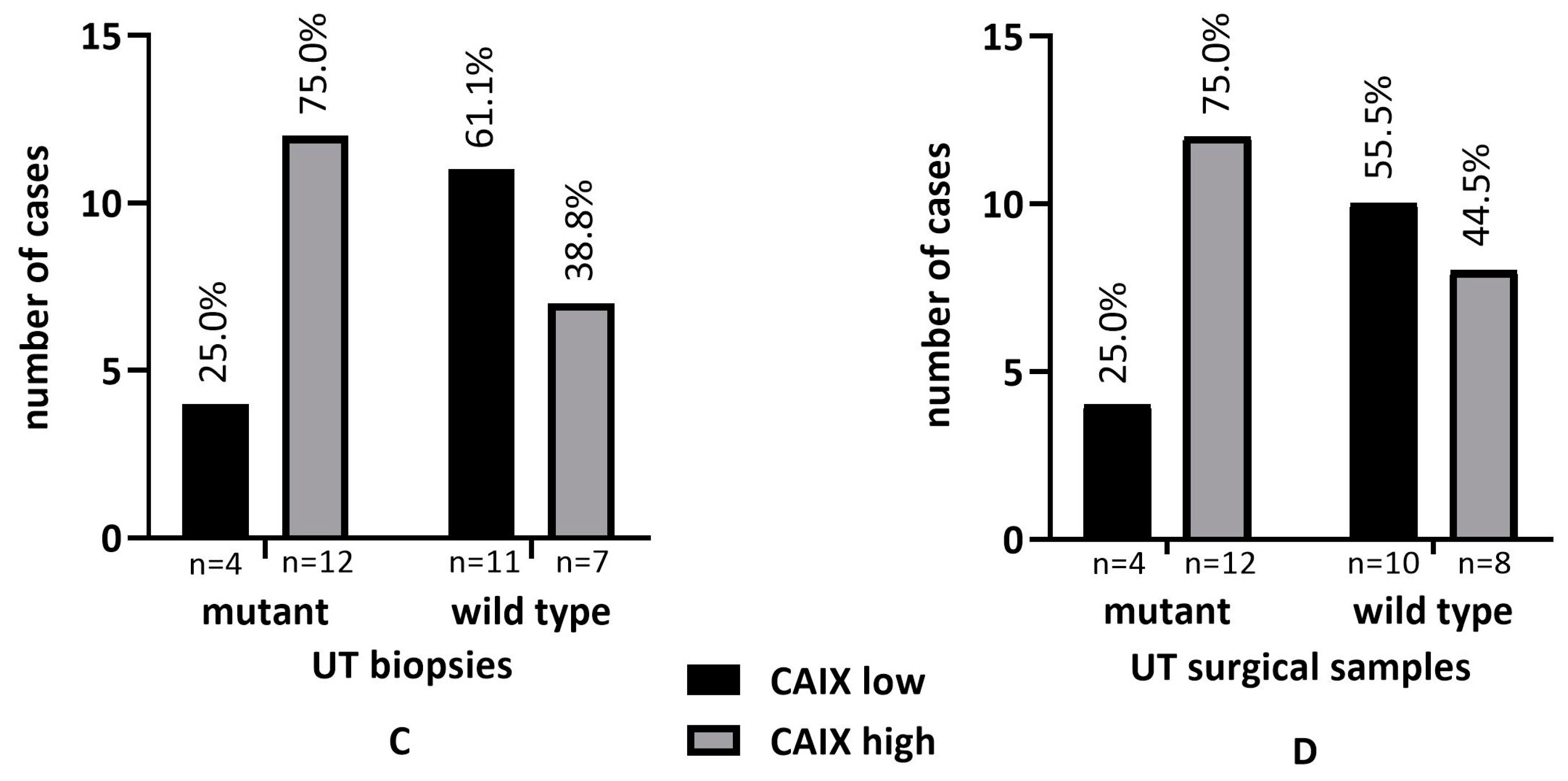
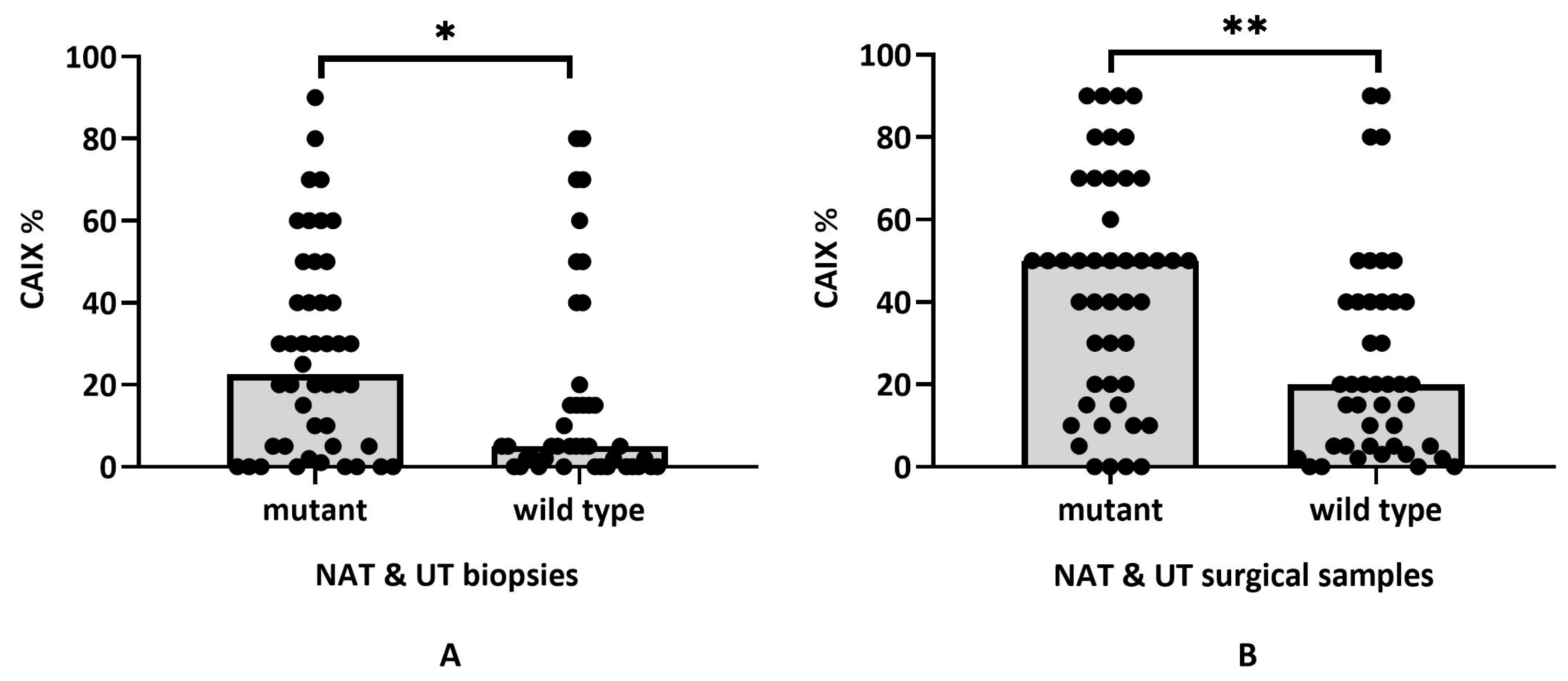
2.5. KRAS Status and CAIX Expression in NAT and UT
2.6. Patient Survival and CAIX Expression in NAT and UT Samples
3. Materials and Methods
3.1. Patients and Study Design
3.2. Immunohistochemical Detection of CAIX
3.3. Tumor DNA Extraction from FFPE Tissue Samples
3.4. Mutation Testing Using StripAssay
3.5. Statistical Analysis
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Dayde, D.; Tanaka, I.; Jain, R.; Tai, M.C.; Taguchi, A. Predictive and Prognostic Molecular Biomarkers for Response to Neoadjuvant Chemoradiation in Rectal Cancer. Int. J. Mol. Sci. 2017, 18, 573. [Google Scholar] [CrossRef] [PubMed]
- Korkeila, E.A.; Sundström, J.; Pyrhönen, S.; Syrjänen, K. Carbonic Anhydrase IX, Hypoxia-Inducible Factor-1α, Ezrin and Glucose Transporter-1 as Predictors of Disease Outcome in Rectal Cancer: Multivariate Cox Survival Models Following Data Reduction by Principal Component Analysis of the Clinicopathological Predictors. Anticancer Res. 2011, 31, 4529–4535. [Google Scholar] [PubMed]
- Vitoratou, D.-I.; Tolia, M.; Liakos, P.; Tsoukalas, N.; Giaginis, C.; Nikolaou, M.; Nikolaou, G.; Rigas, G.; Psarianos, K.; Lioupis, A.; et al. Clinical Value of Significance of Hypoxia Inducible Factor-1α, Glucose Transporter-1 and Carbonic Anhydrase IX in Rectal Cancer after Preoperative Chemoradiotherapy. J. BUON 2019, 24, 456–463. [Google Scholar] [PubMed]
- Span, P.N.; Bussink, J. Biology of Hypoxia. Semin. Nucl. Med. 2015, 45, 101–109. [Google Scholar] [CrossRef] [PubMed]
- Gillies, R.J.; Gatenby, R.A. Hypoxia and Adaptive Landscapes in the Evolution of Carcinogenesis. Cancer Metastasis Rev. 2007, 26, 311–317. [Google Scholar] [CrossRef] [PubMed]
- Saka, B.; Ekinci, O.; Dursun, A.; Akyurek, N. Clinicopathologic and Prognostic Significance of Immunohistochemical Expression of HIF-1α, CXCR4 and CA9 in Colorectal Carcinoma. Pathol. Res. Pract. 2017, 213, 783–792. [Google Scholar] [CrossRef]
- Aldera, A.P.; Govender, D. Carbonic Anhydrase IX: A Regulator of PH and Participant in Carcinogenesis. J. Clin. Pathol. 2021, 74, 350–354. [Google Scholar] [CrossRef]
- Becker, H.M. Carbonic Anhydrase IX and Acid Transport in Cancer. Br. J. Cancer 2020, 122, 157–167. [Google Scholar] [CrossRef]
- Matolay, O.; Beke, L.; Gyurkovics, A.; Francz, M.; Varjasi, G.; Rejtő, L.; Illés, Á.; Bedekovics, J.; Méhes, G. Quantitative Analysis of Carbonic Anhydrase IX Uncovers Hypoxia-Related Functional Differences in Classical Hodgkin Lymphoma Subtypes. Int. J. Mol. Sci. 2019, 20, 3463. [Google Scholar] [CrossRef]
- Lin, C.; Ng, H.L.H.; Pan, W.; Chen, H.; Zhang, G.; Bian, Z.; Lu, A.; Yang, Z. Exploring Different Strategies for Efficient Delivery of Colorectal Cancer Therapy. Int. J. Mol. Sci. 2015, 16, 26936–26952. [Google Scholar] [CrossRef]
- Shin, H.-J.; Rho, S.B.; Jung, D.C.; Han, I.-O.; Oh, E.-S.; Kim, J.-Y. Carbonic Anhydrase IX (CA9) Modulates Tumor-Associated Cell Migration and Invasion. J. Cell Sci. 2011, 124, 1077–1087. [Google Scholar] [CrossRef]
- Huang, B.-R.; Liu, Y.-S.; Lai, S.-W.; Lin, H.-J.; Shen, C.-K.; Yang, L.-Y.; Lu, D.-Y. CAIX Regulates GBM Motility and TAM Adhesion and Polarization through EGFR/STAT3 under Hypoxic Conditions. Int. J. Mol. Sci. 2020, 21, 5838. [Google Scholar] [CrossRef] [PubMed]
- Stewart, D.J.; Nunez, M.I.; Behrens, C.; Liu, D.; Lin, Y.H.; Lee, J.J.; Roth, J.; Heymach, J.; Swisher, S.G.; Hong, W.K.; et al. Membrane Carbonic Anhydrase IX Expression and Relapse Risk in Resected Stage I-II Non-Small-Cell Lung Cancer. J. Thorac. Oncol. 2014, 9, 675–684. [Google Scholar] [CrossRef] [PubMed]
- McDonald, P.C.; Swayampakula, M.; Dedhar, S. Coordinated Regulation of Metabolic Transporters and Migration/Invasion by Carbonic Anhydrase IX. Metabolites 2018, 8, 20. [Google Scholar] [CrossRef] [PubMed]
- McDonald, P.C.; Chafe, S.C.; Brown, W.S.; Saberi, S.; Swayampakula, M.; Venkateswaran, G.; Nemirovsky, O.; Gillespie, J.A.; Karasinska, J.M.; Kalloger, S.E.; et al. Regulation of PH by Carbonic Anhydrase 9 Mediates Survival of Pancreatic Cancer Cells With Activated KRAS in Response to Hypoxia. Gastroenterology 2019, 157, 823–837. [Google Scholar] [CrossRef]
- Andreucci, E.; Peppicelli, S.; Carta, F.; Brisotto, G.; Biscontin, E.; Ruzzolini, J.; Bianchini, F.; Biagioni, A.; Supuran, C.T.; Calorini, L. Carbonic Anhydrase IX Inhibition Affects Viability of Cancer Cells Adapted to Extracellular Acidosis. J. Mol. Med. 2017, 95, 1341–1353. [Google Scholar] [CrossRef]
- van Kuijk, S.J.A.; Yaromina, A.; Houben, R.; Niemans, R.; Lambin, P.; Dubois, L.J. Prognostic Significance of Carbonic Anhydrase IX Expression in Cancer Patients: A Meta-Analysis. Front. Oncol. 2016, 6, 69. [Google Scholar] [CrossRef]
- Juhász, P.; Hasulyó, D.; Bedekovics, J.; Beke, L.; Kacsala, N.; Török, M.; Méhes, G. Carbonic Anhydrase IX (CAIX) Expressing Hypoxic Micro-Environment Hampers CD8+ Immune Cell Infiltrate in Breast Carcinoma. Appl. Immunohistochem. Mol. Morphol. 2023, 31, 26–32. [Google Scholar] [CrossRef]
- Méhes, G.; Matolay, O.; Beke, L.; Czenke, M.; Jóna, Á.; Miltényi, Z.; Illés, Á.; Bedekovics, J. Hypoxia-Related Carbonic Anhydrase IX Expression Is Associated with Unfavourable Response to First-Line Therapy in Classical Hodgkin’s Lymphoma. Histopathology 2019, 74, 699–708. [Google Scholar] [CrossRef]
- Neri, D.; Supuran, C.T. Interfering with PH Regulation in Tumours as a Therapeutic Strategy. Nat. Rev. Drug Discov. 2011, 10, 767–777. [Google Scholar] [CrossRef] [PubMed]
- Ward, C.; Meehan, J.; Gray, M.; Kunkler, I.H.; Langdon, S.P.; Argyle, D.J. Carbonic Anhydrase IX (CAIX), Cancer, and Radiation Responsiveness. Metabolites 2018, 8, 13. [Google Scholar] [CrossRef] [PubMed]
- Korkeila, E.; Talvinen, K.; Jaakkola, P.M.; Minn, H.; Syrjänen, K.; Sundström, J.; Pyrhönen, S. Expression of Carbonic Anhydrase IX Suggests Poor Outcome in Rectal Cancer. Br. J. Cancer 2009, 100, 874–880. [Google Scholar] [CrossRef] [PubMed]
- Kováčová, Z.; Hodorová, I. Carbonic Anhydrase IX and Survivin in Colorectal Adenocarcinoma Cells: Slovakian Population Study. Biology 2021, 10, 872. [Google Scholar] [CrossRef] [PubMed]
- Tupá, V.; Drahošová, S.; Grendár, M.; Adamkov, M. Expression and Association of Carbonic Anhydrase IX and Cyclooxygenase-2 in Colorectal Cancer. Pathol. Res. Pract. 2019, 215, 705–711. [Google Scholar] [CrossRef] [PubMed]
- Guedj, N.; Bretagnol, F.; Rautou, P.-E.; Deschamps, L.; Cazals-Hatem, D.; Bedossa, P.; Panis, Y.; Couvelard, A. Predictors of Tumor Response after Preoperative Chemoradiotherapy for Rectal Adenocarcinomas. Hum. Pathol. 2011, 42, 1702–1709. [Google Scholar] [CrossRef]
- Thies, S.; Langer, R. Tumor Regression Grading of Gastrointestinal Carcinomas after Neoadjuvant Treatment. Front. Oncol. 2013, 3, 262. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.H.; Chang, H.J.; Kim, D.Y.; Park, J.W.; Baek, J.Y.; Kim, S.Y.; Park, S.C.; Oh, J.H.; Yu, A.; Nam, B.-H. What Is the Ideal Tumor Regression Grading System in Rectal Cancer Patients after Preoperative Chemoradiotherapy? Cancer Res. Treat. 2016, 48, 998–1009. [Google Scholar] [CrossRef] [PubMed]
- Debucquoy, A.; Goethals, L.; Libbrecht, L.; Perneel, C.; Geboes, K.; Ectors, N.; McBride, W.H.; Haustermans, K. Molecular and Clinico-Pathological Markers in Rectal Cancer: A Tissue Micro-Array Study. Int. J. Color. Dis. 2009, 24, 129–138. [Google Scholar] [CrossRef] [PubMed]
- Nakada, N.; Mikami, T.; Horie, K.; Nagashio, R.; Sakurai, Y.; Sanoyama, I.; Yoshida, T.; Sada, M.; Kobayashi, K.; Sato, Y.; et al. Expression of CA2 and CA9 Carbonic Anhydrases in Ulcerative Colitis and Ulcerative Colitis-Associated Colorectal Cancer. Pathol. Int. 2020, 70, 523–532. [Google Scholar] [CrossRef]
- Fokas, E.; Ströbel, P.; Fietkau, R.; Ghadimi, M.; Liersch, T.; Grabenbauer, G.G.; Hartmann, A.; Kaufmann, M.; Sauer, R.; Graeven, U.; et al. Tumor Regression Grading After Preoperative Chemoradiotherapy as a Prognostic Factor and Individual-Level Surrogate for Disease-Free Survival in Rectal Cancer. JNCI J. Natl. Cancer Inst. 2017, 109, djx095. [Google Scholar] [CrossRef] [PubMed]
- Viikilä, P.; Kivelä, A.J.; Mustonen, H.; Koskensalo, S.; Waheed, A.; Sly, W.S.; Pastorek, J.; Pastorekova, S.; Parkkila, S.; Haglund, C. Carbonic Anhydrase Enzymes II, VII, IX and XII in Colorectal Carcinomas. World J. Gastroenterol. 2016, 22, 8168–8177. [Google Scholar] [CrossRef] [PubMed]










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Clinicopathological Parameters in Treated Patients | Quantity of CAIX Expression in Biopsy | Quantity of CAIX Expression in Resection | Fisher’s Exact Test in Biopsy | Fisher’s Exact Test in Resection | ||
|---|---|---|---|---|---|---|
| CAIXlow | CAIXhigh | CAIXlow | CAIXhigh | |||
| Total (n = 55) | 27 | 28 | 26 | 29 | p > 0.9999 | |
| Sex | p > 0.7807 | |||||
| Male (n = 35) | 19 | 16 | 18 | 17 | p > 0.4032 | |
| Female (n = 20) | 8 | 12 | 9 | 11 | ||
| Grade of tumor | ||||||
| G2 (n = 36) | 20 | 16 | 19 | 17 | ||
| G3 (n = 17) | 6 | 11 | 6 | 11 | p > 0.4466 | p > 0.5609 |
| G4 (n = 2) | 1 | 1 | 1 | 1 | ||
| Lymph nodes | ||||||
| positive (n = 16) | - | - | 9 | 7 | - | p > 0.5532 |
| negative (n = 39) | - | - | 17 | 22 | ||
| Metastasis | ||||||
| present (n = 11) | - | - | 6 | 5 | - | p > 0.9999 |
| absent (n = 44) | - | - | 24 | 20 | ||
| Necrosis | ||||||
| present (n(B) = 2; n(R) = 24) | 8 | 7 | 9 | 15 | p > 0.4706 | p > 0.1965 |
| absent (n(B) = 15; n(R) = 16) | 0 | 2 | 10 | 6 | ||
| Stroma | ||||||
| present (n(B) = 4; n(R) = 24) | 2 | 2 | 13 | 11 | p > 0.9999 | p > 0.4183 |
| absent (n(B) = 51; n(R) = 31) | 25 | 26 | 13 | 19 | ||
| Tumor-infiltrating lymphocytes | ||||||
| present (n(R) = 24) | - | - | 13 | 11 | - | p > 0.7910 |
| absent (n(R) = 31) | - | - | 18 | 13 | ||
| Mucinous phenotype | ||||||
| present (n = 11) | 3 | 8 | 4 | 7 | p > 0.1771 | p > 0.5104 |
| absent (n = 44) | 24 | 20 | 22 | 22 | ||
| Tumor regression grade | ||||||
| TRG2 (n = 14) | 9 | 5 | 5 | 9 | p > 0.0660 | p > 0.0590 |
| TRG3 (n = 21) | 13 | 8 | 12 | 9 | ||
| TRG4 (n = 14) | 4 | 10 | 4 | 10 | ||
| TRG5 (n = 6) | 1 | 5 | 0 | 6 | ||
| KRAS status | ||||||
| wild-type (n = 25) | 17 | 8 | 16 | 9 | p < 0.0151 | p < 0.0316 |
| mutant (n = 30) | 10 | 20 | 10 | 20 | ||
| Clinicopathological Parameters in Untreated Patients | Quantity of CAIX Expression in Biopsy | Quantity of CAIX Expression in Resection | Fisher’s Exact Test in Biopsy | Fisher’s Exact Test in Resection | ||
|---|---|---|---|---|---|---|
| CAIXlow | CAIXhigh | CAIXlow | CAIXhigh | |||
| Total (n = 34) | 15 | 19 | 14 | 20 | p > 0.9999 | |
| Sex | p > 0.2714 | |||||
| Male (n = 23) | 12 | 11 | 12 | 11 | p > 0.4768 | |
| Female (n = 11) | 4 | 7 | 3 | 8 | ||
| Grade of tumor | ||||||
| G1 (n(B) = 1, n(R) = 1) | 0 | 1 | 0 | 1 | p > 0.3547 | p > 0.9068 |
| G2 (n(B) = 28, n(R) = 19) | 14 | 14 | 9 | 10 | ||
| G3 (n(B) = 5, n(R) = 13) | 1 | 4 | 5 | 8 | ||
| G4 (n = 1 R) | - | - | 0 | 1 | ||
| Lymph nodes | ||||||
| positive (n = 17) | - | - | 6 | 11 | - | p > 0.7283 |
| negative (n = 17) | - | - | 8 | 9 | ||
| Metastasis | ||||||
| present (n = 5) | - | - | 1 | 4 | - | p > 0.3786 |
| absent (n = 29) | - | - | 13 | 16 | ||
| Necrosis | ||||||
| present (n(B) = 2; n(R) = 26) | 0 | 2 | 9 | 17 | p > 0.4667 | p > 0.5320 |
| absent (n(B) = 4; n(R) = 3) | 2 | 2 | 0 | 3 | ||
| Stroma | ||||||
| present (n(B) = 0; n(R) = 9) | - | - | 3 | 6 | - | p > 0.9999 |
| absent (n(B) = 34; n(R) = 25) | 14 | 20 | 8 | 17 | ||
| Tumor-infiltrating lymphocytes | ||||||
| present (n(R) = 19) | - | - | 5 | 9 | - | p > 0.4953 |
| absent (n(R) = 15) | - | - | 10 | 10 | ||
| Mucinous phenotype | ||||||
| present (n = 6) | 2 | 4 | 1 | 5 | p > 0.6722 | p > 0.3636 |
| absent (n = 28) | 13 | 15 | 13 | 15 | ||
| KRAS status | ||||||
| Wild-type (n = 18) | 11 | 7 | 10 | 8 | p < 0.0454 | p > 0.0921 |
| mutant (n = 16) | 4 | 12 | 4 | 12 | ||
| NAT Treated Patients | UT (Control) Patients | |||
|---|---|---|---|---|
| Characteristics | Classification | % (N = 55) | Classification | % (N = 34) |
| Sex | Male | 35 | Male | 23 |
| Female | 20 | Female | 11 | |
| Age | Male (range) | 68.6 (41–85) | Male | 68.43 (51–84) |
| Female (range) | 66.2 (52–84) | Female | 69 (52–83) | |
| Histological grade | G1 | 0 | G1 | 1 |
| G2 | 36 | G2 | 19 | |
| G3 | 17 | G3 | 13 | |
| G4 | 2 | G4 | 1 | |
| Tumor depth | T1 | 0 | T1 | 3 |
| T2 | 29 | T2 | 9 | |
| T3 | 25 | T3 | 19 | |
| T4 | 1 | T4 | 3 | |
| Nx | 0 | Nx | 2 | |
| N0 | 33 | N0 | 10 | |
| N1 | 15 | N1 | 14 | |
| N2 | 7 | N2 | 8 | |
| Mx | 51 | Mx | 0 | |
| M0 | 0 | M0 | 0 | |
| M1 (liver) | 4 | M1 (liver) | 1 | |
| Mucinous phenotype | Present | 11 | Present | 6 |
| Absent | 44 | Absent | 28 | |
| KRAS status | Wild-type | 25 | Wild-type | 18 |
| Mutant | 30 | Mutant | 16 | |
| Type of neoadjuvant treatment | Capecitabine & RT | 32 | ||
| 5FU & FOL & RT | 16 | |||
| 5FU &RT | 5 | |||
| RT | 2 | |||
| Tumor regresssion grade | R1 | 0 | ||
| R2 | 14 | |||
| R3 | 21 | |||
| R4 | 14 | |||
| R5 | 6 | |||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bádon, E.S.; Beke, L.; Mokánszki, A.; András, C.; Méhes, G. Carbonic Anhydrase IX Expression and Treatment Response Measured in Rectal Adenocarcinoma Following Neoadjuvant Chemo-Radiotherapy. Int. J. Mol. Sci. 2023, 24, 2581. https://doi.org/10.3390/ijms24032581
Bádon ES, Beke L, Mokánszki A, András C, Méhes G. Carbonic Anhydrase IX Expression and Treatment Response Measured in Rectal Adenocarcinoma Following Neoadjuvant Chemo-Radiotherapy. International Journal of Molecular Sciences. 2023; 24(3):2581. https://doi.org/10.3390/ijms24032581
Chicago/Turabian StyleBádon, Emese Sarolta, Lívia Beke, Attila Mokánszki, Csilla András, and Gábor Méhes. 2023. "Carbonic Anhydrase IX Expression and Treatment Response Measured in Rectal Adenocarcinoma Following Neoadjuvant Chemo-Radiotherapy" International Journal of Molecular Sciences 24, no. 3: 2581. https://doi.org/10.3390/ijms24032581
APA StyleBádon, E. S., Beke, L., Mokánszki, A., András, C., & Méhes, G. (2023). Carbonic Anhydrase IX Expression and Treatment Response Measured in Rectal Adenocarcinoma Following Neoadjuvant Chemo-Radiotherapy. International Journal of Molecular Sciences, 24(3), 2581. https://doi.org/10.3390/ijms24032581