
Long-Term Immunomodulatory Impact of VNS on Peripheral Cytokine Profiles and Its Relationship with Clinical Response in Difficult-to-Treat Depression (DTD)
 , , and
, , and
Abstract
:1. Introduction
2. Results
2.1. Sample Description
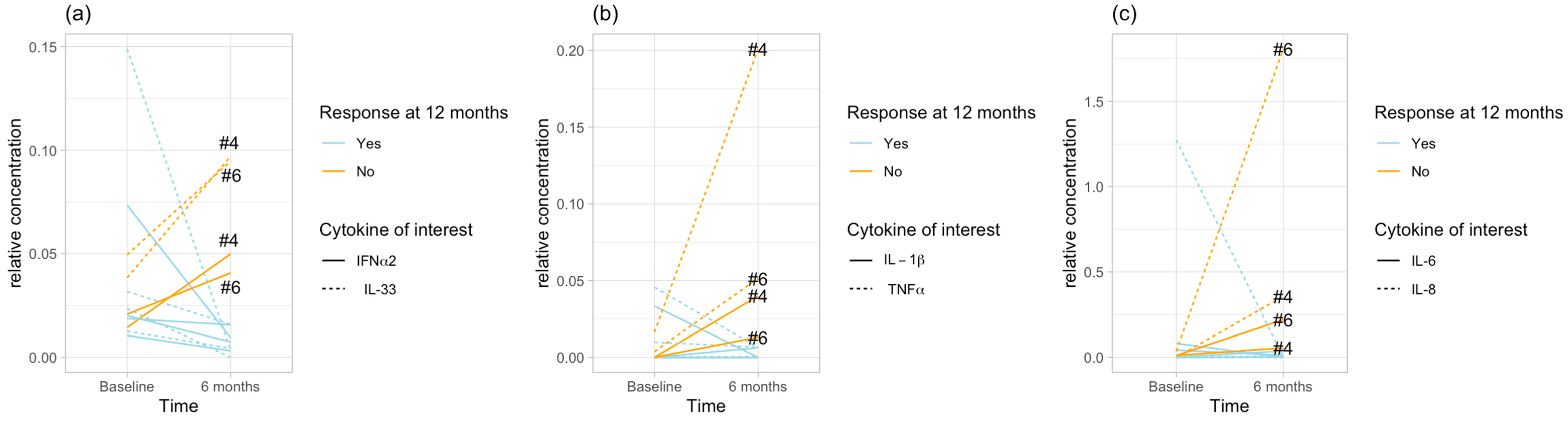
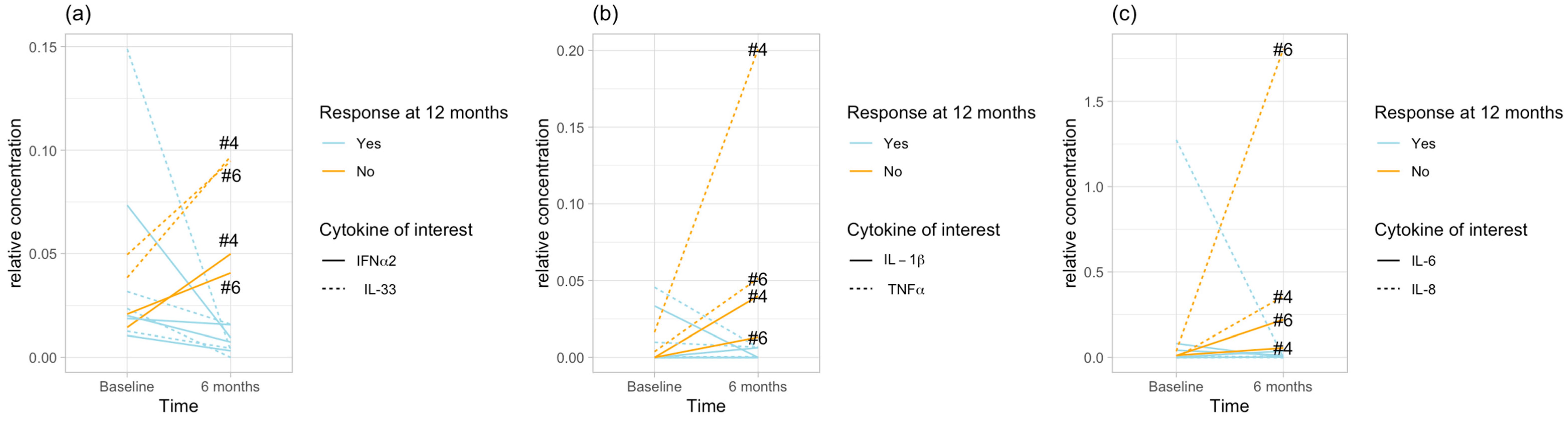
2.2. Cytokine Clusters
- 0.336 between IL-1β and TNF-α, indicating the closest relationship;
- 0.344 between IL-6 and IL-8;
- 0.599 between IFN-α2 and IL-33.
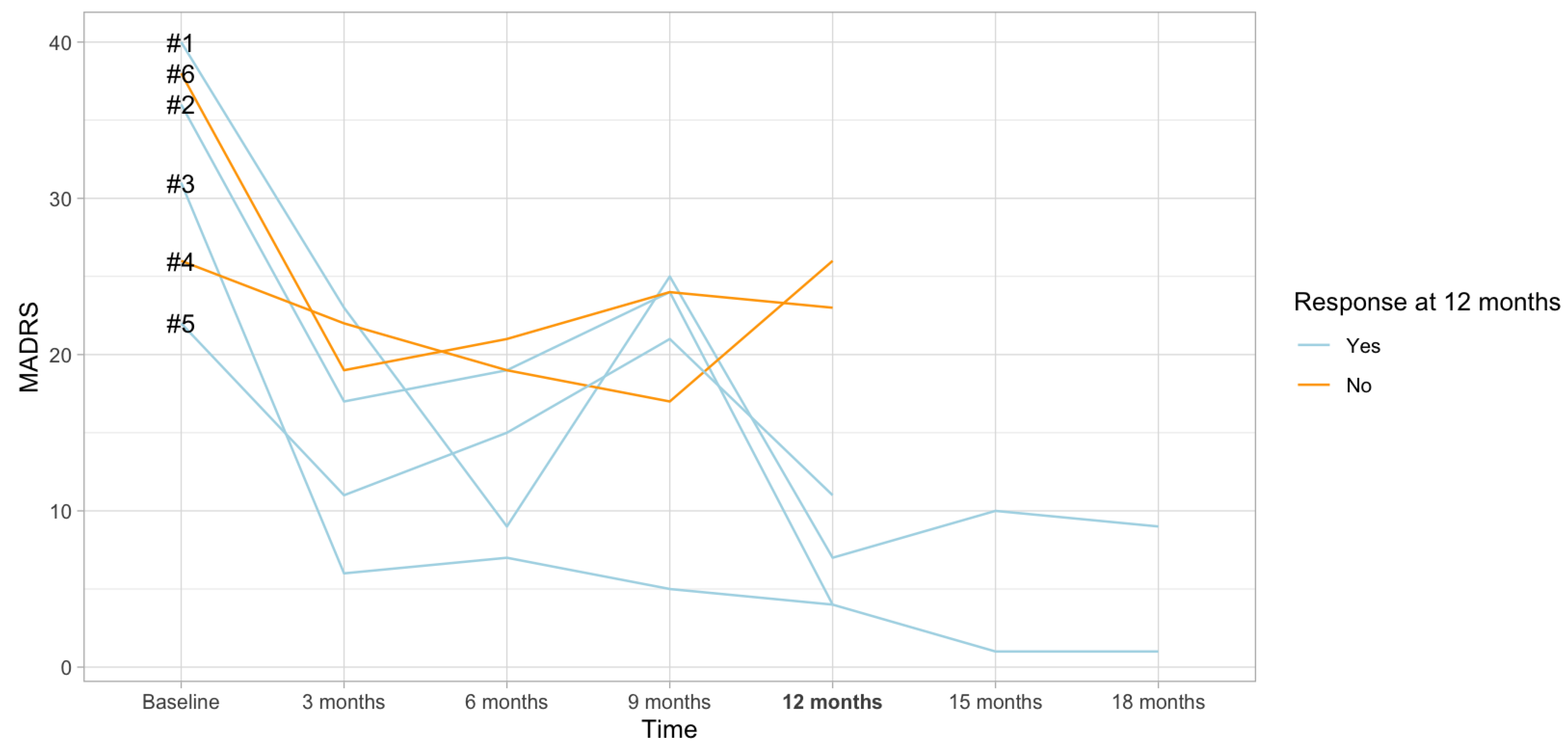
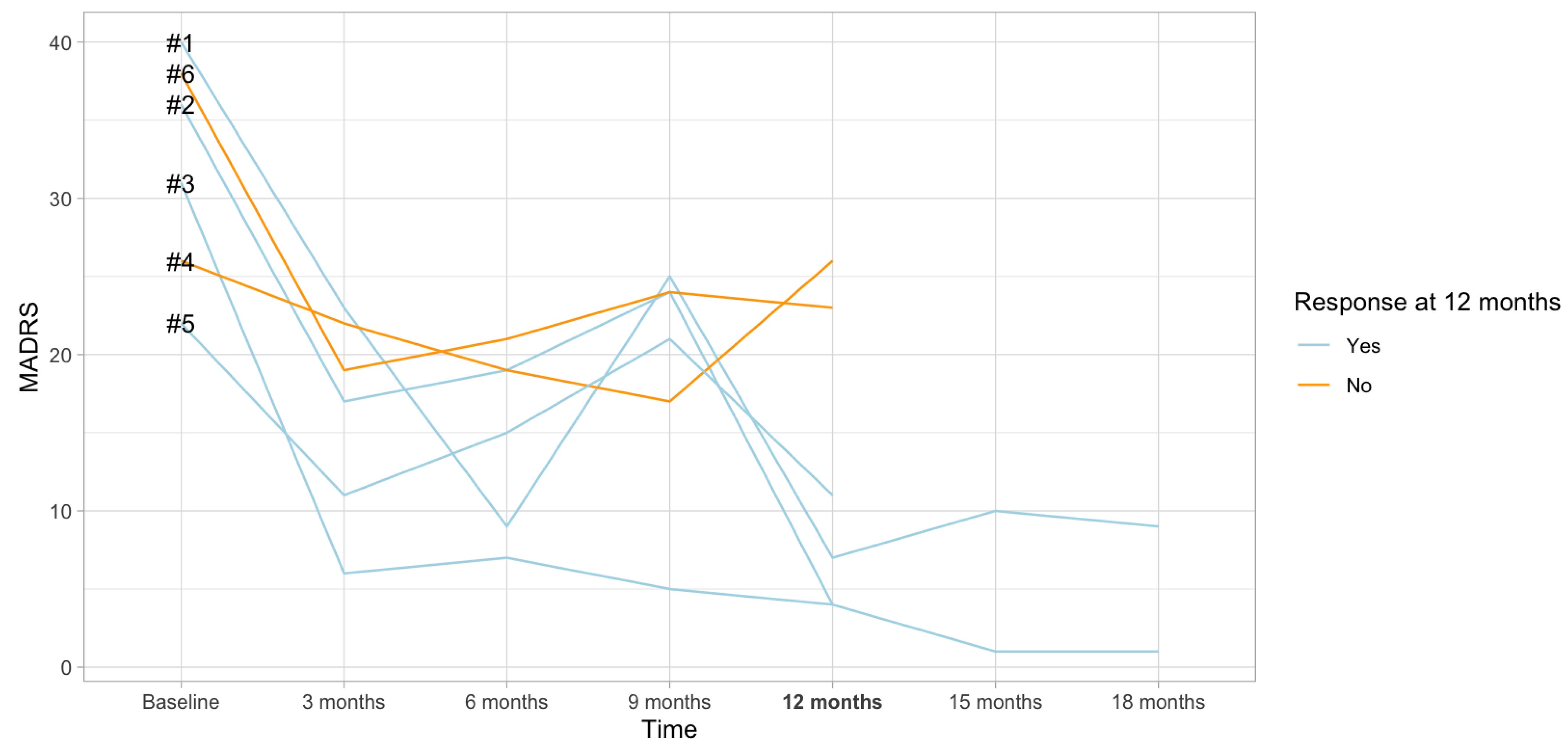
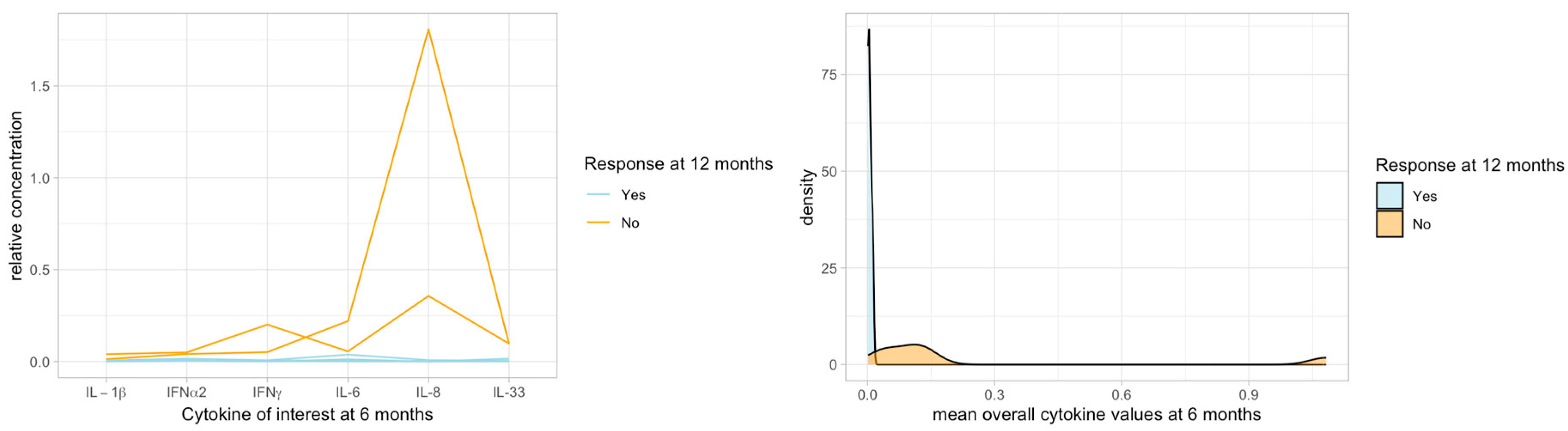
2.3. Cytokines and Clinical Response
3. Discussion
4. Strengths and Limitations
5. Material and Methods
5.1. Study Design
5.2. Inflammatory Protein Measurements
5.3. Statistical Analyses
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Beurel, E.; Toups, M.; Nemeroff, C.B. The Bidirectional Relationship of Depression and Inflammation: Double Trouble. Neuron 2020, 107, 234–256. [Google Scholar] [CrossRef] [PubMed]
- Malhi, G.S.; Mann, J.J. Depression. Lancet 2018, 392, 2299–2312. [Google Scholar] [CrossRef] [PubMed]
- Kverno, K.S.; Mangano, E. Treatment-Resistant Depression: Approaches to Treatment. J. Psychosoc. Nurs. Ment. Health Serv. 2021, 59, 7–11. [Google Scholar] [CrossRef] [PubMed]
- McAllister-Williams, R.H.; Bulmer, S.; Newton, K.; Heath, K.; Cousins, D.A.; Currie, A. Assessment for Vagus Nerve Stimulation in Patients with Difficult-to-Treat Depression: A Model from the Newcastle Regional Affective Disorders Service (RADS). J. Affect. Disord. 2021, 280, 315–318. [Google Scholar] [CrossRef]
- Rush, A.J.; Aaronson, S.T.; Demyttenaere, K. Difficult-to-Treat Depression: A Clinical and Research Roadmap for When Remission Is Elusive. Aust. N. Z. J. Psychiatry 2019, 53, 109–118. [Google Scholar] [CrossRef] [PubMed]
- Kraus, C.; Quach, D.; Sholtes, D.M.; Kavakbasi, E.; De Zwaef, R.; Dibué, M.; Zajecka, J.; Baune, B.T. Setting Up a Successful Vagus Nerve Stimulation Service for Patients with Difficult-to-Treat Depression. Neuromodul. J. Int. Neuromodul. Soc. 2022, 25, 316–326. [Google Scholar] [CrossRef]
- Milev, R.V.; Giacobbe, P.; Kennedy, S.H.; Blumberger, D.M.; Daskalakis, Z.J.; Downar, J.; Modirrousta, M.; Patry, S.; Vila-Rodriguez, F.; Lam, R.W.; et al. Canadian Network for Mood and Anxiety Treatments (CANMAT) 2016 Clinical Guidelines for the Management of Adults with Major Depressive Disorder: Section 4. Neurostimulation Treatments. Can. J. Psychiatry Rev. Can. Psychiatr. 2016, 61, 561–575. [Google Scholar] [CrossRef] [PubMed]
- Zunszain, P.A.; Hepgul, N.; Pariante, C.M. Inflammation and Depression. Curr. Top. Behav. Neurosci. 2013, 14, 135–151. [Google Scholar] [CrossRef] [PubMed]
- Baune, B.T. Are Non-Steroidal Anti-Inflammatory Drugs Clinically Suitable for the Treatment of Symptoms in Depression-Associated Inflammation? Curr. Top. Behav. Neurosci. 2017, 31, 303–319. [Google Scholar] [CrossRef]
- Kavakbasi, E.; Sampson, E.; Mills, N.T.; Hori, H.; Schwarte, K.; Hohoff, C.; Schubert, K.O.; Clark, S.R.; Fourrier, C.; Baune, B.T. Inflammation-Stratified Augmentation of Vortioxetine with Celecoxib: Results from a Double-Blind, Randomized, Placebo-Controlled Trial in Major Depressive Disorder. J. Neurochem. 2023. online ahead of print. [Google Scholar] [CrossRef]
- Lichtblau, N.; Schmidt, F.M.; Schumann, R.; Kirkby, K.C.; Himmerich, H. Cytokines as Biomarkers in Depressive Disorder: Current Standing and Prospects. Int. Rev. Psychiatry Abingdon Engl. 2013, 25, 592–603. [Google Scholar] [CrossRef]
- Breit, S.; Kupferberg, A.; Rogler, G.; Hasler, G. Vagus Nerve as Modulator of the Brain-Gut Axis in Psychiatric and Inflammatory Disorders. Front. Psychiatry 2018, 9, 44. [Google Scholar] [CrossRef] [PubMed]
- Bonaz, B.; Sinniger, V.; Pellissier, S. Anti-Inflammatory Properties of the Vagus Nerve: Potential Therapeutic Implications of Vagus Nerve Stimulation. J. Physiol. 2016, 594, 5781–5790. [Google Scholar] [CrossRef] [PubMed]
- Borovikova, L.V.; Ivanova, S.; Zhang, M.; Yang, H.; Botchkina, G.I.; Watkins, L.R.; Wang, H.; Abumrad, N.; Eaton, J.W.; Tracey, K.J. Vagus Nerve Stimulation Attenuates the Systemic Inflammatory Response to Endotoxin. Nature 2000, 405, 458–462. [Google Scholar] [CrossRef] [PubMed]
- Kalkman, H.O.; Feuerbach, D. Modulatory Effects of A7 nAChRs on the Immune System and Its Relevance for CNS Disorders. Cell. Mol. Life Sci. CMLS 2016, 73, 2511–2530. [Google Scholar] [CrossRef] [PubMed]
- Bonaz, B. Non-Invasive Vagus Nerve Stimulation: The Future of Inflammatory Bowel Disease Treatment? Bioelectron. Med. 2023, 9, 26. [Google Scholar] [CrossRef] [PubMed]
- Liu, J.J.; Wei, Y.B.; Strawbridge, R.; Bao, Y.; Chang, S.; Shi, L.; Que, J.; Gadad, B.S.; Trivedi, M.H.; Kelsoe, J.R.; et al. Peripheral Cytokine Levels and Response to Antidepressant Treatment in Depression: A Systematic Review and Meta-Analysis. Mol. Psychiatry 2020, 25, 339–350. [Google Scholar] [CrossRef]
- O’Brien, S.M.; Scott, L.V.; Dinan, T.G. Cytokines: Abnormalities in Major Depression and Implications for Pharmacological Treatment. Hum. Psychopharmacol. 2004, 19, 397–403. [Google Scholar] [CrossRef] [PubMed]
- Osimo, E.F.; Pillinger, T.; Rodriguez, I.M.; Khandaker, G.M.; Pariante, C.M.; Howes, O.D. Inflammatory Markers in Depression: A Meta-Analysis of Mean Differences and Variability in 5,166 Patients and 5,083 Controls. Brain Behav. Immun. 2020, 87, 901–909. [Google Scholar] [CrossRef] [PubMed]
- Drevets, W.C.; Wittenberg, G.M.; Bullmore, E.T.; Manji, H.K. Immune Targets for Therapeutic Development in Depression: Towards Precision Medicine. Nat. Rev. Drug Discov. 2022, 21, 224–244. [Google Scholar] [CrossRef]
- Cahill, C.M.; Rogers, J.T. Interleukin (IL) 1beta Induction of IL-6 Is Mediated by a Novel Phosphatidylinositol 3-Kinase-Dependent AKT/IkappaB Kinase Alpha Pathway Targeting Activator Protein-1. J. Biol. Chem. 2008, 283, 25900–25912. [Google Scholar] [CrossRef]
- Ridker, P.M. From C-Reactive Protein to Interleukin-6 to Interleukin-1: Moving Upstream To Identify Novel Targets for Atheroprotection. Circ. Res. 2016, 118, 145–156. [Google Scholar] [CrossRef] [PubMed]
- Shin, H.C.; Jo, B.G.; Lee, C.-Y.; Lee, K.-W.; Namgung, U. Hippocampal Activation of 5-HT1B Receptors and BDNF Production by Vagus Nerve Stimulation in Rats under Chronic Restraint Stress. Eur. J. Neurosci. 2019, 50, 1820–1830. [Google Scholar] [CrossRef]
- Parente, J.; Gianlorenco, A.C.; Rebello-Sanchez, I.; Kim, M.; Prati, J.M.; Kim, C.K.; Choi, H.; Song, J.-J.; Fregni, F. Neural, Anti-Inflammatory, and Clinical Effects of Transauricular Vagus Nerve Stimulation in Major Depressive Disorder: A Systematic Review. Int. J. Neuropsychopharmacol. 2023, 27, pyad058. [Google Scholar] [CrossRef] [PubMed]
- Lespérance, P.; Desbeaumes Jodoin, V.; Drouin, D.; Racicot, F.; Miron, J.-P.; Longpré-Poirier, C.; Fournier-Gosselin, M.-P.; Thebault, P.; Lapointe, R.; Arbour, N.; et al. Vagus Nerve Stimulation Modulates Inflammation in Treatment-Resistant Depression Patients: A Pilot Study. Int. J. Mol. Sci. 2024, 25, 2679. [Google Scholar] [CrossRef]
- Aaronson, S.T.; Sears, P.; Ruvuna, F.; Bunker, M.; Conway, C.R.; Dougherty, D.D.; Reimherr, F.W.; Schwartz, T.L.; Zajecka, J.M. A 5-Year Observational Study of Patients With Treatment-Resistant Depression Treated With Vagus Nerve Stimulation or Treatment as Usual: Comparison of Response, Remission, and Suicidality. Am. J. Psychiatry 2017, 174, 640–648. [Google Scholar] [CrossRef]
- Strawbridge, R.; Hodsoll, J.; Powell, T.R.; Hotopf, M.; Hatch, S.L.; Breen, G.; Cleare, A.J. Inflammatory Profiles of Severe Treatment-Resistant Depression. J. Affect. Disord. 2019, 246, 42–51. [Google Scholar] [CrossRef] [PubMed]
- Köhler, C.A.; Freitas, T.H.; Maes, M.; de Andrade, N.Q.; Liu, C.S.; Fernandes, B.S.; Stubbs, B.; Solmi, M.; Veronese, N.; Herrmann, N.; et al. Peripheral Cytokine and Chemokine Alterations in Depression: A Meta-Analysis of 82 Studies. Acta Psychiatr. Scand. 2017, 135, 373–387. [Google Scholar] [CrossRef]
- Rajasundaram, S.; Rahman, R.P.; Woolf, B.; Zhao, S.S.; Gill, D. Morning Cortisol and Circulating Inflammatory Cytokine Levels: A Mendelian Randomisation Study. Genes 2022, 13, 116. [Google Scholar] [CrossRef] [PubMed]
- Herriot, H.; Wrosch, C.; Gouin, J.-P.; Miller, G.E. Intra-Individual Cortisol Variability and Low-Grade Inflammation over 10 Years in Older Adults. Psychoneuroendocrinology 2017, 77, 141–149. [Google Scholar] [CrossRef]
- Knight, E.L.; Jiang, Y.; Rodriguez-Stanley, J.; Almeida, D.M.; Engeland, C.G.; Zilioli, S. Perceived Stress Is Linked to Heightened Biomarkers of Inflammation via Diurnal Cortisol in a National Sample of Adults. Brain Behav. Immun. 2021, 93, 206–213. [Google Scholar] [CrossRef]
- Bonaz, B.; Sinniger, V.; Pellissier, S. The Vagus Nerve in the Neuro-Immune Axis: Implications in the Pathology of the Gastrointestinal Tract. Front. Immunol. 2017, 8, 1452. [Google Scholar] [CrossRef] [PubMed]
- Lin, Y.-C.; Lin, Y.-C.; Huang, M.-Y.; Kuo, P.-L.; Wu, C.-C.; Lee, M.-S.; Hsieh, C.-C.; Kuo, H.-F.; Kuo, C.-H.; Tsai, W.-C.; et al. Tumor Necrosis Factor-Alpha Inhibitors Suppress CCL2 Chemokine in Monocytes via Epigenetic Modification. Mol. Immunol. 2017, 83, 82–91. [Google Scholar] [CrossRef] [PubMed]
- do Prado-Lima, P.A.S.; Costa-Ferro, Z.S.M.; de Freitas Souza, B.S.; da Cruz, I.B.M.; Lab, B. Is There a Place for Cellular Therapy in Depression? World J. Psychiatry 2021, 11, 553–567. [Google Scholar] [CrossRef] [PubMed]
- Nagappan, P.G.; Chen, H.; Wang, D.-Y. Neuroregeneration and Plasticity: A Review of the Physiological Mechanisms for Achieving Functional Recovery Postinjury. Mil. Med. Res. 2020, 7, 30. [Google Scholar] [CrossRef] [PubMed]
- Dellarole, A.; Morton, P.; Brambilla, R.; Walters, W.; Summers, S.; Bernardes, D.; Grilli, M.; Bethea, J.R. Neuropathic pain-induced depressive-like behavior and hippocampal neurogenesis and plasticity are dependent on TNFR1 signaling. Brain Behav. Immun. 2014, 41, 65–81. [Google Scholar] [CrossRef] [PubMed]
- Chen, M.-H.; Li, C.-T.; Lin, W.-C.; Hong, C.-J.; Tu, P.-C.; Bai, Y.-M.; Cheng, C.-M.; Su, T.-P. Rapid Inflammation Modulation and Antidepressant Efficacy of a Low-Dose Ketamine Infusion in Treatment-Resistant Depression: A Randomized, Double-Blind Control Study. Psychiatry Res. 2018, 269, 207–211. [Google Scholar] [CrossRef] [PubMed]
- Guloksuz, S.; Rutten, B.P.F.; Arts, B.; van Os, J.; Kenis, G. The Immune System and Electroconvulsive Therapy for Depression. J. ECT 2014, 30, 132–137. [Google Scholar] [CrossRef] [PubMed]
- Gay, F.; Romeo, B.; Martelli, C.; Benyamina, A.; Hamdani, N. Cytokines Changes Associated with Electroconvulsive Therapy in Patients with Treatment-Resistant Depression: A Meta-Analysis. Psychiatry Res. 2021, 297, 113735. [Google Scholar] [CrossRef] [PubMed]
- Zhao, X.; Li, Y.; Tian, Q.; Zhu, B.; Zhao, Z. Repetitive Transcranial Magnetic Stimulation Increases Serum Brain-Derived Neurotrophic Factor and Decreases Interleukin-1β and Tumor Necrosis Factor-α in Elderly Patients with Refractory Depression. J. Int. Med. Res. 2019, 47, 1848–1855. [Google Scholar] [CrossRef]
- Sramek, J.J.; Murphy, M.F.; Cutler, N.R. Sex Differences in the Psychopharmacological Treatment of Depression. Dialogues Clin. Neurosci. 2016, 18, 447–457. [Google Scholar] [CrossRef]
- Fang, Y.-T.; Lin, Y.-T.; Tseng, W.-L.; Tseng, P.; Hua, G.-L.; Chao, Y.-J.; Wu, Y.-J. Neuroimmunomodulation of Vagus Nerve Stimulation and the Therapeutic Implications. Front. Aging Neurosci. 2023, 15, 1173987. [Google Scholar] [CrossRef] [PubMed]
- Young, A.H.; Juruena, M.F.; De Zwaef, R.; Demyttenaere, K. Vagus Nerve Stimulation as Adjunctive Therapy in Patients with Difficult-to-Treat Depression (RESTORE-LIFE): Study Protocol Design and Rationale of a Real-World Post-Market Study. BMC Psychiatry 2020, 20, 471. [Google Scholar] [CrossRef] [PubMed]
- R Core Team. A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2008; Available online: https://www.R-project.org/ (accessed on 9 April 2024).


{kind=link}
{kind=link}
{kind=link}
| Mean age at time of implantation (years) | 47.8 |
| Gender, Women | 83.3%, n = 5 |
| Psychiatric comorbidities | n = 2, Post-traumatic stress disorder |
| Mean age at first onset of depression (years) | 21.2 |
| Mean duration of current episode (months) | 28.7 |
Treatment history prior to VNS
| 100% (n = 6) 66.6% (n = 4) 33.3% (n = 2) 33.3% (n = 2) |
| Baseline MADRS (mean) | 32.2 |
| 12 months MADRS (mean) | 12.5 |
| 12 months response rate (%) | 66.6 (4 out of 6) |
| Cluster-Based * Cytokine Pairs | Cluster Tree Height ** | V0 Correlation *** Coefficient; p-Value | V6 Correlation *** Coefficient; p-Value (p(Corrected)-Value) |
|---|---|---|---|
| TNFa–IL-1β | extra low | 0.655; p = 0.158 | 0.941; p = 0.005, (p(corr) = 0.015) |
| IL-6–IL-8 | extra low | 0.213; p = 0.686 | 0.941; p = 0.005, (p(corr) = 0.015) |
| IFNα2–IL-33 | low | 0.714; p = 0.111 | 0.829; p = 0.042 |
| Cytokine | Concentration Baseline (Mean) | Concentation at 6 Months (Mean) | Change | Test Statistics (Wilcoxon Test) | p-Value | |
|---|---|---|---|---|---|---|
| Responder to VNS at 12 months | IL-1β | 0.00843 | 0.00165 | Decrease | −0.447 | 0.655 |
| TNF-α | 0.01398 | 0.00343 | Decrease | −1.069 | 0.285 | |
| IL-6 | 0.03175 | 0.01308 | Decrease | −0.365 | 0.715 | |
| IL-8 | 0.32100 | 0.00203 | Decrease | −1.069 | 0.285 | |
| IFN-α2 | 0.03068 | 0.00893 | Decrease | −1.826 | 0.068 | |
| IL-33 | 0.05418 | 0.00595 | Decrease | −1.826 | 0.068 | |
| Non-responder to VNS at 12 months | IL-1β | 0.00010 | 0.02650 | Increase | 1.342 | 0.180 |
| TNF-α | 0.01005 | 0.12595 | Increase | 1.342 | 0.180 | |
| IL-6 | 0.01125 | 0.13780 | Increase | 1.342 | 0.180 | |
| IL-8 | 0.01805 | 1.08195 | Increase | 1.342 | 0.180 | |
| IFN-α2 | 0.01760 | 0.04530 | Increase | 1.342 | 0.180 | |
| IL-33 | 0.04395 | 0.09585 | Increase | 1.342 | 0.180 |
| Cytokine | Mean Concentration of the Cytokine at 6 Months | Mann–Whitney U Test | Ratio of Cytokine Concetration in Non-responders/Responders | |
|---|---|---|---|---|
| Responder | Non-responder | p-Value (Exact; Asymptotic) | ||
| IL-1β | 0.001650 | 0.026500 | 0.049; 0.133 | 16.1 |
| TNF-α | 0.003425 | 0.125950 | 0.064; 0.133 | 36.8 |
| IL-6 | 0.013075 | 0.137800 | 0.064; 0.133 | 10.5 |
| IL-8 | 0.002025 | 1.081950 | 0.049; 0.133 | 534.3 |
| IFN-α2 | 0.008925 | 0.045300 | 0.064; 0.133 | 5.1 |
| IL-33 | 0.005950 | 0.095850 | 0.064; 0.133 | 16.1 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kavakbasi, E.; Van Assche, E.; Schwarte, K.; Hohoff, C.; Baune, B.T. Long-Term Immunomodulatory Impact of VNS on Peripheral Cytokine Profiles and Its Relationship with Clinical Response in Difficult-to-Treat Depression (DTD). Int. J. Mol. Sci. 2024, 25, 4196. https://doi.org/10.3390/ijms25084196
Kavakbasi E, Van Assche E, Schwarte K, Hohoff C, Baune BT. Long-Term Immunomodulatory Impact of VNS on Peripheral Cytokine Profiles and Its Relationship with Clinical Response in Difficult-to-Treat Depression (DTD). International Journal of Molecular Sciences. 2024; 25(8):4196. https://doi.org/10.3390/ijms25084196
Chicago/Turabian StyleKavakbasi, Erhan, Evelien Van Assche, Kathrin Schwarte, Christa Hohoff, and Bernhard T. Baune. 2024. "Long-Term Immunomodulatory Impact of VNS on Peripheral Cytokine Profiles and Its Relationship with Clinical Response in Difficult-to-Treat Depression (DTD)" International Journal of Molecular Sciences 25, no. 8: 4196. https://doi.org/10.3390/ijms25084196