
Association between Platelet-Derived Growth Factor Receptor Alpha Gene Polymorphisms and Platelet-Rich Plasma’s Efficiency in Treating Lateral Elbow Tendinopathy—A Prospective Cohort Study
 , , , , ,
, , , , ,  ,
,  ,
,
Abstract
1. Introduction
2. Results
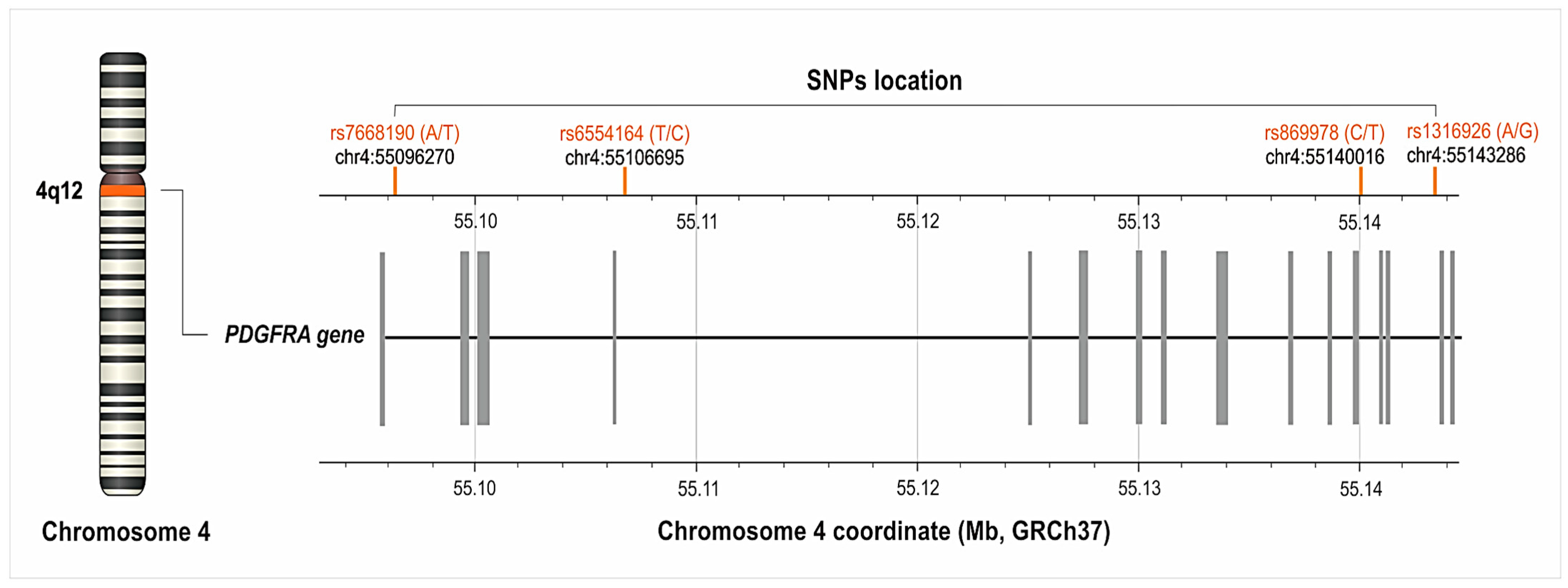
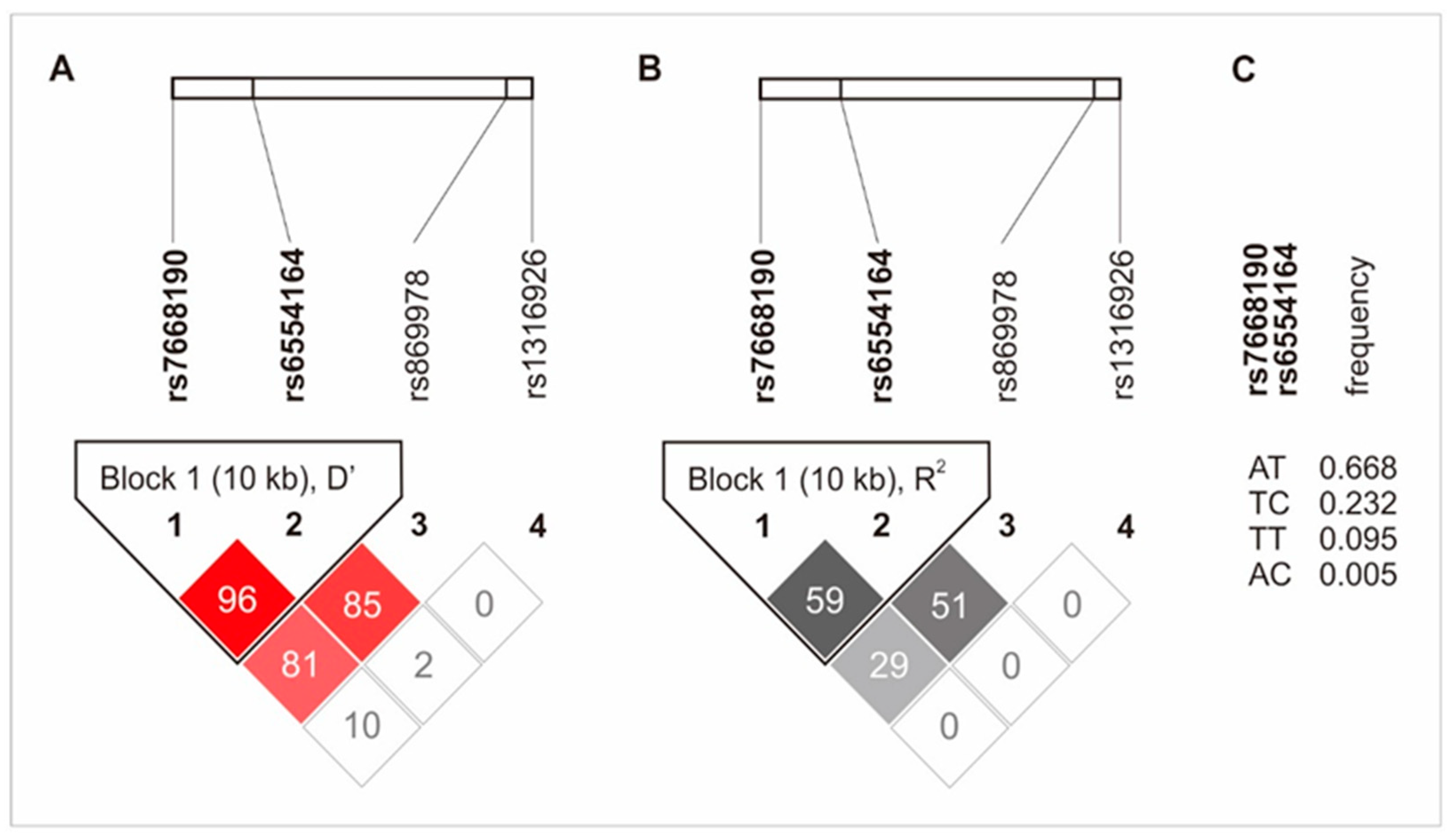
2.1. Characteristic of the PDGFRA Gene’s Polymorphisms

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| SNP | Chromosome 4 Coordinate * | PDGFRA Gene Coordinate | Minor Allele | Minor Allele Frequency (%) ** | Alleles | n | (%) | Genotype | n | (%) |
|---|---|---|---|---|---|---|---|---|---|---|
| rs7668190 | 55096270 | 6007 | T | 27.63 | A | 118 | (62.43) | AA | 61 | (46.21) |
| T | 71 | (37.57) | AT | 57 | (43.18) | |||||
| TT | 14 | (10.61) | ||||||||
| AA + AT | 118 | (89.39) | ||||||||
| TT + AT | 71 | (53.79) | ||||||||
| rs6554164 | 55106695 | 16432 | C | 22.96 | T | 124 | (69.27) | TT | 76 | (58.02) |
| C | 55 | (30.73) | CT | 48 | (36.64) | |||||
| CC | 7 | (5.34) | ||||||||
| TT + CT | 124 | (94.67) | ||||||||
| CC + TT | 55 | (41.98) | ||||||||
| rs869978 | 55140016 | 49753 | T | 22.17 | C | 127 | (74.71) | CC | 89 | (67.42) |
| T | 43 | (25.29) | CT | 38 | (28.79) | |||||
| TT | 5 | (3.79) | ||||||||
| CC + CT | 127 | (96.21) | ||||||||
| TT + CT | 43 | (32.58) | ||||||||
| rs1316926 | 55143286 | 53023 | G | 48.61 | A | 108 | (55.10) | AA | 44 | (33.33) |
| G | 88 | (44.90) | AG | 64 | (48.48) | |||||
| GG | 24 | (18.18) | ||||||||
| AA + AG | 108 | (96.97) | ||||||||
| GG + AG | 88 | (66.67) |

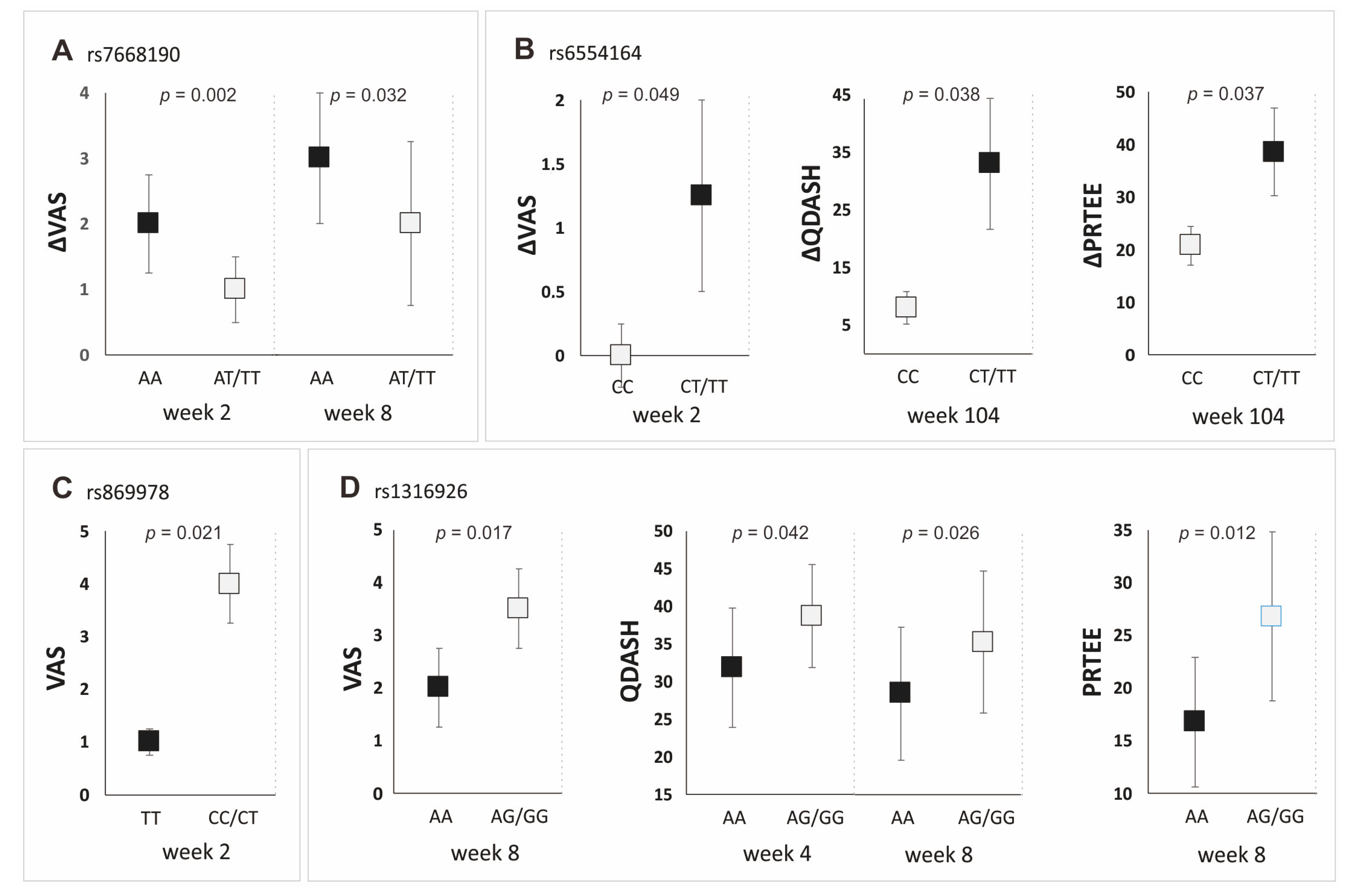
2.2. The Influence of the Studied Polymorphisms on PROM Values, Achievement of MCID and Platelet Parameters
3. Discussion
4. Materials and Methods
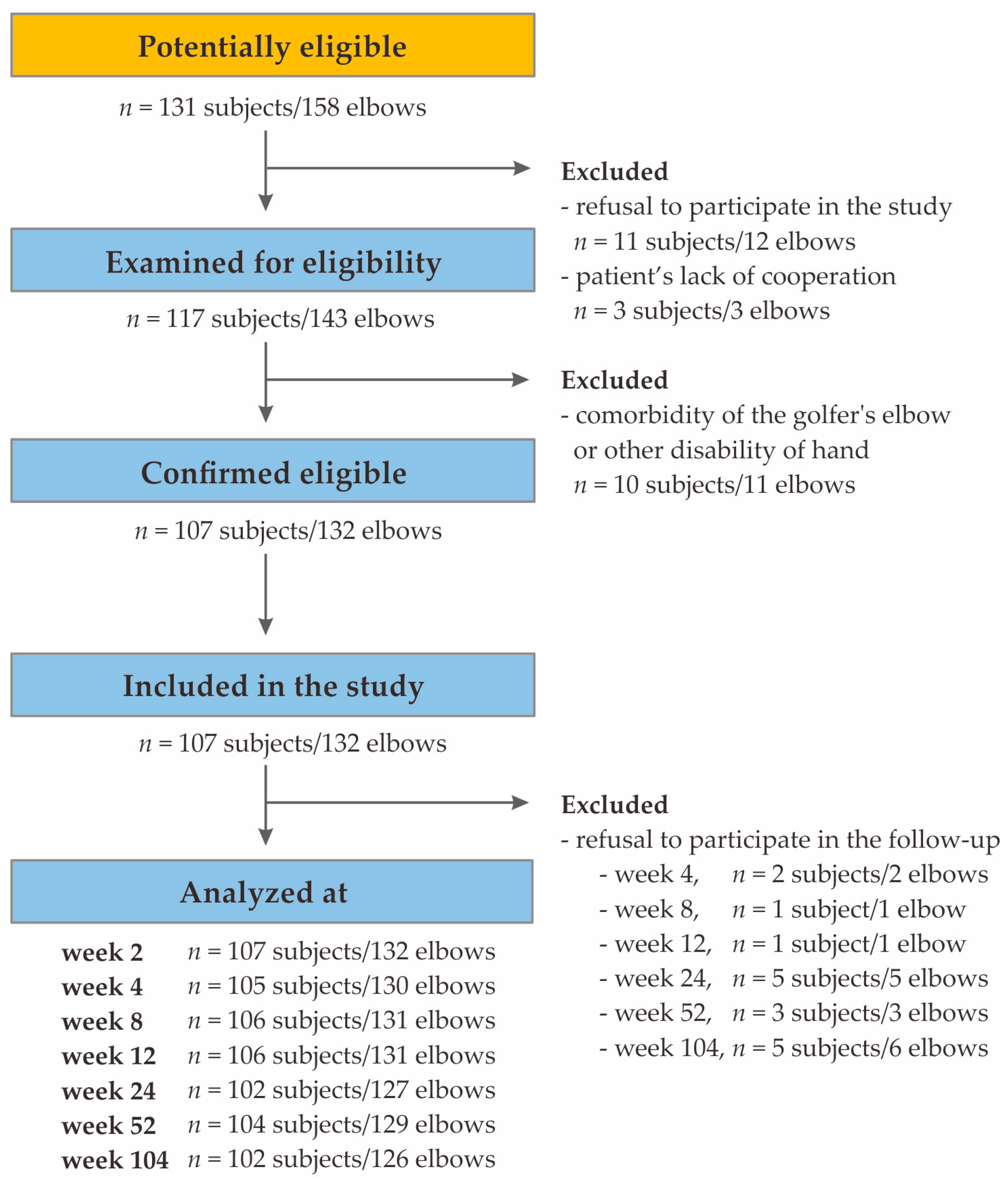
4.1. Patient Selection
4.2. Characteristics of the Study Group
4.3. PRP Separation, Injection Procedure, Whole Blood and PRP Parameters
4.4. Genetic Analyses
4.5. Statistical Analysis
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Rogers, M.A.; Fantauzzo, K.A. The emerging complexity of PDGFRs: Activation, internalization and signal attenuation. Biochem. Soc. Trans. 2020, 48, 1167–1176. [Google Scholar] [CrossRef] [PubMed]
- Heldin, C.H.; Westermark, B. Mechanism of Action and In Vivo Role of Platelet-Derived Growth Factor. Physiol. Rev. 1999, 79, 1283–1316. [Google Scholar] [CrossRef] [PubMed]
- Heldin, C.H.; Lennartsson, J. Structural and Functional Properties of Platelet-Derived Growth Factor and Stem Cell Factor Receptors. Cold Spring Harb. Perspect. Biol. 2013, 5, a009100. [Google Scholar] [CrossRef]
- Wu, E.; Palmer, N.; Tian, Z.; Moseman, A.P.; Galdzicki, M.; Wang, X.; Berger, B.; Zhang, H.; Kohane, I.S. Comprehensive Dissection of PDGF-PDGFR Signaling Pathways in PDGFR Genetically Defined Cells. PLoS ONE 2008, 3, e3794. [Google Scholar] [CrossRef]
- Andrae, J.; Gallini, R.; Betsholtz, C. Role of platelet-derived growth factors in physiology and medicine. Genes Dev. 2008, 22, 1276–1312. [Google Scholar] [CrossRef] [PubMed]
- Millar, N.L.; Silbernagel, K.G.; Thorborg, K.; Kirwan, P.D.; Galatz, L.M.; Abrams, G.D.; Murrell, G.A.C.; McInnes, I.B.; Rodeo, S.A. Tendinopathy. Nat. Rev. Dis. Prim. 2021, 7, 1. [Google Scholar] [CrossRef] [PubMed]
- Kheiran, A.; Pandey, A.; Pandey, R. Common tendinopathies around the elbow; what does current evidence say? J. Clin. Orthop. Trauma 2021, 19, 216–223. [Google Scholar] [CrossRef] [PubMed]
- Karaduman, M.; Okkaoglu, M.C.; Sesen, H.; Taskesen, A.; Ozdemir, M.; Altay, M. Platelet-rich plasma versus open surgical release in chronic tennis elbow: A retrospective comparative study. J. Orthop. 2016, 13, 10–14. [Google Scholar] [CrossRef][Green Version]
- Boswell, S.G.; Cole, B.J.; Sundman, E.A.; Karas, V.; Fortier, L.A. Platelet-Rich Plasma: A Milieu of Bioactive Factors. Arthrosc. J. Arthrosc. Relat. Surg. 2012, 28, 429–439. [Google Scholar] [CrossRef]
- Zhou, Y.; Wang, J.H.C. PRP Treatment Efficacy for Tendinopathy: A Review of Basic Science Studies. BioMed Res. Int. 2016, 2016, 9103792. [Google Scholar] [CrossRef]
- Jarosz, A.; Szyluk, K.; Iwanicka, J.; Balcerzyk, A.; Nowak, T.; Iwanicki, T.; Negru, M.; Kalita, M.; Francuz, T.; Garczorz, W.; et al. What Role Does PDGFA Gene Polymorphisms Play in Treating Tennis Elbow with PRP? A Prospective Cohort Study. J. Clin. Med. 2022, 11, 3504. [Google Scholar] [CrossRef] [PubMed]
- Niemiec, P.; Szyluk, K.; Balcerzyk, A.; Kalita, M.; Jarosz, A.; Iwanicka, J.; Iwanicki, T.; Nowak, T.; Negru, M.; Francuz, T.; et al. Why PRP works only on certain patients with tennis elbow? Is PDGFB gene a key for PRP therapy effectiveness? A prospective cohort study. BMC Musculoskelet. Disord. 2021, 22, 710. [Google Scholar] [CrossRef] [PubMed]
- Szyluk, K.; Jarosz, A.; Balcerzyk-Matić, A.; Iwanicka, J.; Iwanicki, T.; Nowak, T.; Gierek, M.; Negru, M.; Kalita, M.; Górczyńska-Kosiorz, S.; et al. Polymorphic Variants of the PDGFRB Gene Influence Efficacy of PRP Therapy in Treating Tennis Elbow: A Prospective Cohort Study. J. Clin. Med. 2022, 11, 6362. [Google Scholar] [CrossRef] [PubMed]
- Niemiec, P.; Jarosz, A.; Balcerzyk-Matić, A.; Iwanicka, J.; Nowak, T.; Iwanicki, T.; Gierek, M.; Kalita, M.; Garczorz, W.; Francuz, T.; et al. Genetic Variability in VEGFA Gene Influences the Effectiveness of Tennis Elbow Therapy with PRP: A Two-Year Prospective Cohort Study. Int. J. Mol. Sci. 2023, 24, 17292. [Google Scholar] [CrossRef]
- National Library of Medicine (US): National Center for Biotechnology Information. Available online: https://www.ncbi.nlm.nih.gov/snp/ (accessed on 15 February 2023).
- National Institutes of Health. LDlink (US): LDmatrix Tool. Available online: https://ldlink.nih.gov/?tab=ldmatrix (accessed on 5 February 2024).
- Sedaghat, A.R. Understanding the Minimal Clinically Important Difference (MCID) of Patient-Reported Outcome Measures. Otolaryngol. Neck Surg. 2019, 161, 551–560. [Google Scholar] [CrossRef]
- Sugg, K.B.; Markworth, J.F.; Disser, N.P.; Rizzi, A.M.; Talarek, J.R.; Sarver, D.C.; Brooks, S.V.; Mendias, C.L. Postnatal tendon growth and remodeling require platelet-derived growth factor receptor signaling. Am. J. Physiol. Physiol. 2018, 314, C389–C403. [Google Scholar] [CrossRef] [PubMed]
- Kendal, A.R.; Layton, T.; Al-Mossawi, H.; Appleton, L.; Dakin, S.; Brown, R.; Loizou, C.; Rogers, M.; Sharp, R.; Carr, A. Multi-omic single cell analysis resolves novel stromal cell populations in healthy and diseased human tendon. Sci. Rep. 2020, 10, 13939. [Google Scholar] [CrossRef]
- Harvey, T.; Flamenco, S.; Fan, C.M. A Tppp3+Pdgfra+ tendon stem cell population contributes to regeneration and reveals a shared role for PDGF signalling in regeneration and fibrosis. Nat. Cell Biol. 2019, 21, 1490–1503. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.; Xu, Y.; Dai, G.; Shi, Q.; Duan, C. Enhanced Repaired Enthesis Using Tenogenically Differentiated Adipose-Derived Stem Cells in a Murine Rotator Cuff Injury Model. Stem Cells Int. 2022, 2022, 1309684. [Google Scholar] [CrossRef]
- Zou, X.; Tang, X.Y.; Qu, Z.Y.; Sun, Z.W.; Ji, C.F.; Li, Y.J.; Guo, S.D. Targeting the PDGF/PDGFR signaling pathway for cancer therapy: A review. Int. J. Biol. Macromol. 2022, 202, 539–557. [Google Scholar] [CrossRef]
- Pandey, P.; Khan, F.; Upadhyay, T.K.; Seungjoon, M.; Park, M.N.; Kim, B. New insights about the PDGF/PDGFR signaling pathway as a promising target to develop cancer therapeutic strategies. Biomed. Pharmacother. 2023, 161, 114491. [Google Scholar] [CrossRef] [PubMed]
- Schatteman, G.C.; Motley, S.T.; Effmann, E.L.; Bowen-Pope, D.F. Platelet-derived growth factor receptor alpha subunit deleted Patch mouse exhibits severe cardiovascular dysmorphogenesis. Teratology 1995, 51, 351–366. [Google Scholar] [CrossRef] [PubMed]
- Szubert, S.; Moszynski, R.; Szpurek, D.; Romaniuk, B.; Sajdak, S.; Nowicki, M.; Michalak, S. The expression of Platelet-derived Growth factor receptors (PDGFRs) and their correlation with overall survival of patients with ovarian cancer. Ginekol. Pol. 2019, 90, 242–249. [Google Scholar] [CrossRef]
- Lu, J.; Li, H.; Zhang, Z.; Xu, R.; Wang, J.; Jin, H. Platelet-rich plasma in the pathologic processes of tendinopathy: A review of basic science studies. Front. Bioeng. Biotechnol. 2023, 11, 1187974. [Google Scholar] [CrossRef] [PubMed]
- Hayashi, T.; Yamamoto, S.; Hamashima, T.; Mori, H.; Sasahara, M.; Kuroda, S. Critical role of platelet-derived growth factor–α in angiogenesis after indirect bypass in a murine moyamoya disease model. J. Neurosurg. 2021, 134, 1535–1543. [Google Scholar] [CrossRef] [PubMed]
- Vassbotn, F.S.; Havnen, O.K.; Heldin, C.H.; Holmsen, H. Negative feedback regulation of human platelets via autocrine activation of the platelet-derived growth factor alpha-receptor. J. Biol. Chem. 1994, 269, 13874–13879. [Google Scholar] [CrossRef] [PubMed]
- The Human Protein Atlas. Available online: https://www.proteinatlas.org/ENSG00000134853-PDGFRA/single+cell+type (accessed on 31 January 2024).
- The Human Protein Atlas. Available online: https://www.proteinatlas.org/ENSG00000113721-PDGFRB/single+cell+type (accessed on 31 January 2024).
- Gasparyan, A.Y.; Sandoo, A.; Stavropoulos-Kalinoglou, A.; Kitas, G.D. Mean platelet volume in patients with rheumatoid arthritis: The effect of anti-TNF-alpha therapy. Rheumatol. Int. 2010, 30, 1125–1129. [Google Scholar] [CrossRef] [PubMed]
- Korniluk, A.; Koper-Lenkiewicz, O.M.; Kamińska, J.; Kemona, H.; Dymicka-Piekarska, V. Mean Platelet Volume (MPV): New Perspectives for an Old Marker in the Course and Prognosis of Inflammatory Conditions. Mediat. Inflamm. 2019, 2019, 9213074. [Google Scholar] [CrossRef] [PubMed]
- Braekkan, S.K.; Mathiesen, E.B.; Njølstad, I.; Wilsgaard, T.; Størmer, J.; Hansen, J.B. Mean platelet volume is a risk factor for venous thromboembolism: The Tromsø study. J. Thromb. Haemost. 2010, 8, 157–162. [Google Scholar] [CrossRef]
- Handtke, S.; Thiele, T. Large and small platelets—(When) do they differ? J. Thromb. Haemost. 2020, 18, 1256–1267. [Google Scholar] [CrossRef]
- Handtke, S.; Steil, L.; Palankar, R.; Conrad, J.; Cauhan, S.; Kraus, L.; Ferrara, M.; Dhople, V.; Wesche, J.; Völker, U.; et al. Role of Platelet Size Revisited—Function and Protein Composition of Large and Small Platelets. Thromb. Haemost. 2019, 119, 407–420. [Google Scholar] [CrossRef] [PubMed]
- Pokrovskaya, I.D.; Yadav, S.; Rao, A.; McBride, E.; Kamykowski, J.A.; Zhang, G.; Aronova, M.A.; Leapman, R.D.; Storrie, B. 3D ultrastructural analysis of α-granule, dense granule, mitochondria, and canalicular system arrangement in resting human platelets. Res. Pract. Thromb. Haemost. 2020, 4, 72–85. [Google Scholar] [CrossRef] [PubMed]
- Ozer, K.; Kankaya, Y.; Çolak, Ö. An important and overlooked parameter in platelet rich plasma preparation: The mean platelet volume. J. Cosmet. Dermatol. 2019, 18, 474–482. [Google Scholar] [CrossRef] [PubMed]
- Bessman, D.J.; Williams, L.J.; Gilmer, R.P. Mean Platelet Volume. The Inverse Relation of Platelet Size and Count in Normal Subjects, and an Artifact of Other Particles. Am. J. Clin. Pathol. 1981, 76, 289–293. [Google Scholar] [CrossRef] [PubMed]
- Verdoia, M.; Barbieri, L.; Schaffer, A.; Bellomo, G.; Marino, P.; De Luca, G. Impact of renal function on mean platelet volume and its relationship with coronary artery disease: A single-centre cohort study. Thromb. Res. 2016, 141, 139–144. [Google Scholar] [CrossRef] [PubMed]
- Ittermann, T.; Feig, M.A.; Petersmann, A.; Radke, D.; Greinacher, A.; Völzke, H.; Thiele, T. Mean platelet volume is more important than age for defining reference intervals of platelet counts. PLoS ONE 2019, 14, e0213658. [Google Scholar] [CrossRef] [PubMed]
- Kuter, D.J. The Physiology of Platelet Production. Stem Cells 1996, 14, 88–101. [Google Scholar] [CrossRef]
- Del Buono, A.; Oliva, F.; Osti, L.; Maffulli, N. Metalloproteases and tendinopathy. Muscles Ligaments Tendons J. 2013, 3, 51–57. [Google Scholar] [CrossRef] [PubMed]
- Steinmann, S.; Pfeifer, C.G.; Brochhausen, C.; Docheva, D. Spectrum of Tendon Pathologies: Triggers, Trails and End-State. Int. J. Mol. Sci. 2020, 21, 844. [Google Scholar] [CrossRef]
- Cook, J.L.; Purdam, C.R. Is tendon pathology a continuum? A pathology model to explain the clinical presentation of load-induced tendinopathy. Br. J. Sports Med. 2009, 43, 409–416. [Google Scholar] [CrossRef]
- GWAS Central. Available online: https://www.gwascentral.org/ (accessed on 5 February 2024).
- Golicki, D.; Krzysiak, M.; Strzelczyk, P. Translation and Cultural Adaptation of the Polish Version of the Disabilities of the Arm, Shoulder and Hand (DASH) and QuickDASH Questionnaires. Ortop. Traumatol. Rehabil. 2014, 16, 387–395. [Google Scholar] [CrossRef]
- Goguł, P.; Latosiewicz, R.; Goguł, M.; Majewska, D.; Gawęda, K. Quality of polish translation and cultural adaptation of PRTEE (Patient–RatedTennis Elbow Evaluation). Health Sport 2016, 6, 2391–8306. [Google Scholar] [CrossRef]
- Hao, Q.; Devji, T.; Zeraatkar, D.; Wang, Y.; Qasim, A.; Siemieniuk, R.A.C.; Vandvik, P.O.; Lähdeoja, T.; Carrasco-Labra, A.; Agoritsas, T.; et al. Minimal important differences for improvement in shoulder condition patient-reported outcomes: A systematic review to inform a BMJ Rapid Recommendation. BMJ Open 2019, 9, e028777. [Google Scholar] [CrossRef]
- Smith-Forbes, E.V.; Howell, D.M.; Willoughby, J.; Pitts, D.G.; Uhl, T.L. Specificity of the minimal clinically important difference of the quick Disabilities of the Arm Shoulder and Hand (QDASH) for distal upper extremity conditions. J. Hand Ther. 2016, 29, 81–88. [Google Scholar] [CrossRef]
- Poltawski, L.; Watson, T. Measuring clinically important change with the Patient-rated Tennis Elbow Evaluation. J. Hand Ther. 2011, 16, 52–57. [Google Scholar] [CrossRef]
- Barrett, J.C.; Fry, B.; Maller, J.; Daly, M.J. Haploview: Analysis and visualization of LD and haplotype maps. Bioinformatics 2005, 21, 263–265. [Google Scholar] [CrossRef]
- Gabriel, S.B.; Schaffner, S.F.; Nguyen, H.; Moore, J.M.; Roy, J.; Blumenstiel, B.; Higgins, J.; DeFelice, M.; Lochner, A.; Faggart, M.; et al. The Structure of Haplotype Blocks in the Human Genome. Science 2002, 296, 2225–2229. [Google Scholar] [CrossRef]



| Model of Heredity | SNP | Genotype | PROM | Week of Follow-Up | MCID+ Patients | MCID– Patients | p | ||
|---|---|---|---|---|---|---|---|---|---|
| n | % | n | % | ||||||
| Additive | rs6554164 | CC | VAS | 2 | 0 | 0.00 | 7 | 10.29 | 0.004 |
| CT | 18 | 29.51 | 29 | 42.65 | |||||
| TT | 43 | 70.49 | 32 | 47.06 | |||||
| CC | QDASH | 104 | 0 | 0.00 | 5 | 13.89 | 0.011 | ||
| CT | 36 | 41.86 | 11 | 30.56 | |||||
| TT | 50 | 58.14 | 20 | 55.56 | |||||
| rs1316926 | AA | VAS | 12 | 33 | 38.37 | 11 | 23.91 | 0.015 | |
| AG | 33 | 38.37 | 30 | 65.22 | |||||
| GG | 20 | 23.26 | 5 | 10.87 | |||||
| Dominant/recessive | rs7668190 | AA | VAS | 2 | 34 | 55,74 | 26 | 38.24 | 0.039 |
| AT/TT | 27 | 44.26 | 42 | 61.76 | |||||
| AA | VAS | 8 | 43 | 53.75 | 18 | 35.29 | 0.039 | ||
| AT/TT | 37 | 46.26 | 33 | 64.71 | |||||
| rs6554164 | CC | VAS | 2 | 0 | 0.00 | 7 | 10.29 | 0.010 | |
| CT/TT | 61 | 100.00 | 61 | 89.71 | |||||
| CC | QDASH | 2 | 0 | 0.00 | 7 | 8.43 | 0.042 | ||
| CT/TT | 46 | 100.00 | 76 | 91.57 | |||||
| CC | QDASH | 104 | 1 | 1.16 | 5 | 13.89 | 0.009 | ||
| CT/TT | 85 | 98.84 | 31 | 86.11 | |||||
| SNP | Platelet Parameter | Median | QD | Median | QD | p Mann– Whitney U-test |
|---|---|---|---|---|---|---|
| rs7668190 | AA | AT + TT | ||||
| PLT PRP | 349.00 | 90.50 | 327.00 | 52.00 | 0.035 | |
| PCT PRP | 0.32 | 0.08 | 0.28 | 0.05 | 0.042 | |
| rs869978 | TT | CT + CC | ||||
| PLT | 170.50 | 19.25 | 246.00 | 35.00 | 0.005 | |
| PCT | 1.75 | 0.18 | 2.32 | 0.36 | 0.015 | |
| MPV | 10.15 | 0.10 | 9.10 | 0.70 | 0.043 | |
| PDW | 16.30 | 0.03 | 16.00 | 0.15 | 0.016 | |
| rs1316926 | AA | AG + GG | ||||
| PLT PRP | 307.00 | 70.75 | 353.50 | 58.00 | 0.032 | |
| Characteristics | |||
|---|---|---|---|
| General | Number of subjects, N | 107 | - |
| Number of elbows, n (%) | 132 | (100.0) | |
| Tennis elbow in the dominant limb, n (%) | 86 | (65.2) | |
| Age, median ± QD | 46.00 | 5.50 | |
| BMI, median ± QD | 25.65 | 2.00 | |
| Current smokers, n (%) | 22 | (16.6) | |
| Comorbidities | Diabetes mellitus, n (%) | 4 | (3.0) |
| Gout, n (%) | 8 | (6.1) | |
| Thyroid diseases, n (%) | 15 | (11.4) | |
| Hypertension, n (%) | 18 | (13.6) | |
| Whole Blood parameters | PLT 109/L, median ± QD | 240.00 | 40.50 |
| PCT mL/L, median ± QD | 2.31 | 0.36 | |
| MPV fl, median ± QD | 9.10 | 0.73 | |
| PDW fl, median ± QD | 16.10 | 0.15 | |
| PRP parameters | PLT 109/L, median ± QD | 343.00 | 65.00 |
| PCT mL/L, median ± QD | 0.30 | 0.06 | |
| MPV fl, median ± QD | 8.60 | 0.40 | |
| PDW fl, median ± QD | 14.60 | 0.25 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jarosz, A.; Balcerzyk-Matić, A.; Iwanicka, J.; Iwanicki, T.; Nowak, T.; Szyluk, K.; Kalita, M.; Górczyńska-Kosiorz, S.; Kania, W.; Niemiec, P. Association between Platelet-Derived Growth Factor Receptor Alpha Gene Polymorphisms and Platelet-Rich Plasma’s Efficiency in Treating Lateral Elbow Tendinopathy—A Prospective Cohort Study. Int. J. Mol. Sci. 2024, 25, 4266. https://doi.org/10.3390/ijms25084266
Jarosz A, Balcerzyk-Matić A, Iwanicka J, Iwanicki T, Nowak T, Szyluk K, Kalita M, Górczyńska-Kosiorz S, Kania W, Niemiec P. Association between Platelet-Derived Growth Factor Receptor Alpha Gene Polymorphisms and Platelet-Rich Plasma’s Efficiency in Treating Lateral Elbow Tendinopathy—A Prospective Cohort Study. International Journal of Molecular Sciences. 2024; 25(8):4266. https://doi.org/10.3390/ijms25084266
Chicago/Turabian StyleJarosz, Alicja, Anna Balcerzyk-Matić, Joanna Iwanicka, Tomasz Iwanicki, Tomasz Nowak, Karol Szyluk, Marcin Kalita, Sylwia Górczyńska-Kosiorz, Wojciech Kania, and Paweł Niemiec. 2024. "Association between Platelet-Derived Growth Factor Receptor Alpha Gene Polymorphisms and Platelet-Rich Plasma’s Efficiency in Treating Lateral Elbow Tendinopathy—A Prospective Cohort Study" International Journal of Molecular Sciences 25, no. 8: 4266. https://doi.org/10.3390/ijms25084266
APA StyleJarosz, A., Balcerzyk-Matić, A., Iwanicka, J., Iwanicki, T., Nowak, T., Szyluk, K., Kalita, M., Górczyńska-Kosiorz, S., Kania, W., & Niemiec, P. (2024). Association between Platelet-Derived Growth Factor Receptor Alpha Gene Polymorphisms and Platelet-Rich Plasma’s Efficiency in Treating Lateral Elbow Tendinopathy—A Prospective Cohort Study. International Journal of Molecular Sciences, 25(8), 4266. https://doi.org/10.3390/ijms25084266