
Eosinophils in Oral Disease: A Narrative Review

 ,
,  , ,
, ,  , and
, and 
Abstract
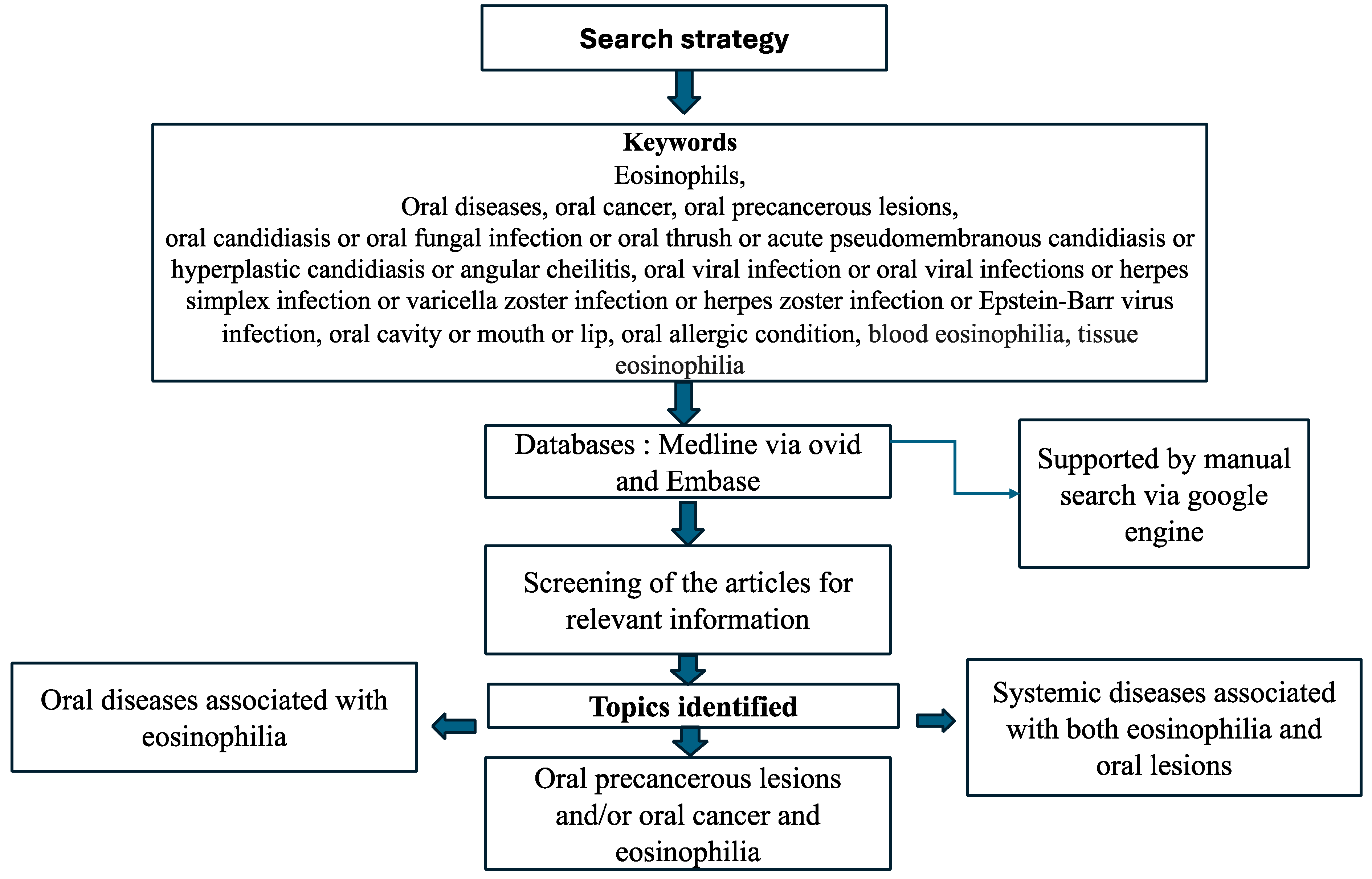
1. Introduction

- Oral diseases—associated with TE and/or blood eosinophilia (BE).
- Systemic diseases—associated with both eosinophilia and oral lesions.
2. Eosinophils and Oral Diseases
2.1. Oral Diseases Associated with Tissue Eosinophilia and/or Blood Eosinophilia
2.1.1. Reactive Lesions
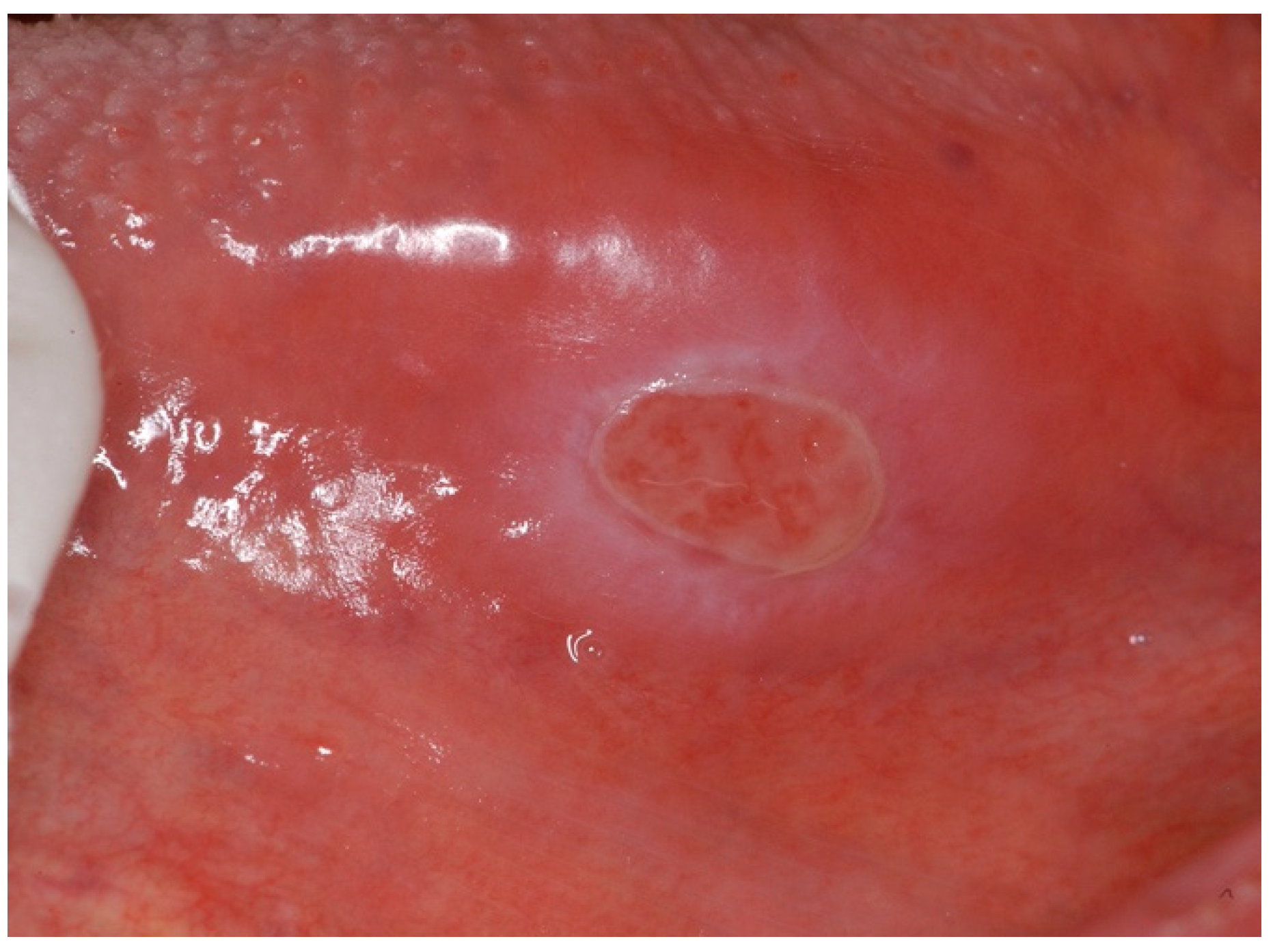
- An oral eosinophilic ulcer is an inflammatory reactive lesion of unknown aetiology, with trauma implicated as causative; hence, it is not commonly observed clinically. Various terminologies have been used to describe this lesion, including “eosinophilic ulcer”, “eosinophilic granuloma of soft tissue”, and “traumatic ulcerative granuloma with stromal eosinophilia (TUGSE)” [22]. It was first described by Popoff in 1956 and later by Shapiro and Juhlin [23]. Clinically, TUGSE manifests as a painful single ulcer with indurated borders, mostly on the surface of the tongue, but can involve any oral mucosal site and is a self-limiting lesion that tends to heal spontaneously (Figure 3) [23,24].
- Riga–Fede disease: this eponym is used to describe an infantile benign condition characterised by the presence of ulcers on the dorsal surface of the tongue (60% of lesions), the lips, palate, mucous membrane of the vestibule and the floor of the mouth. The disease is closely related to TUGSE but is predominantly observed in infants, typically caused by repetitive trauma to the oral mucosa from natal or neonatal teeth [28]. This traumatic and often lingual ulceration is accompanied by eosinophilic granuloma and the eosinophilic ulceration of the tongue and oral mucosa [29]. Ulcerations may be painful, and extraction or odontoplasty are the most effective treatments [28]. Due to the distinctive clinical features, diagnostic assessment and specific treatment, it is useful to classify Riga–Fede disease and eosinophilic ulcers separately from a clinical standpoint [30].
- Eosinophilic granuloma is a rare benign bone lesion, accounting for less than 1% of bone tumours. It mostly affects children under 10 years of age, with the mandible being the most frequently affected site. It represents a mild localised type of oral Langerhans cell histiocytosis (LCH) without malignant transformation. Radiologically, it manifests as teeth resorption, with the teeth appearing to be floating in the air. A histopathological examination reveals the scattered sheets of eosinophilic infiltrates [31,32].
2.1.2. Oral Lichenoid Lesions (OLLs)
2.1.3. Oral Vesicular and Bullous Lesions
- Pemphigus vegetans: this is the rarest clinical variant of pemphigus, comprising 1–2% of all pemphigus cases. It differentiates from pemphigus vulgaris through the development of vegetative plaques in intertriginous regions and oral mucosa and by the presence of autoantibodies against desmoglein 3. Two clinical subtypes exist characterised by flaccid bullae and erosions (Neumann subtype) or pustules (Hallopeau subtype). Both subtypes progress to the development of hyperpigmented vegetative plaques accompanied by pustules. A histopathological examination reveals intraepithelial abscesses with the significant presence of eosinophils [36].
- Bullous pemphigoid (BP) is a chronic autoimmune blistering disease which mainly involves the skin but, on rare occasions, can affect the oral mucous membrane (Figure 6), usually associated with an older age demographic [37]. It is a subtype of the autoimmune blistering disease (AIBD), in contrast to the mucous membrane pemphigoid (MMP), which is also a subtype of AIBD but with a predominantly oral mucous presentation. Mucosal lesions of BP are mild, affecting only about 10–20% of patients, and exhibit less aggressive mucosal erosion and blistering lesions [38,39]. A histopathological examination is characterised by submucosal blister formation with a mixed inflammatory cell infiltrate, particularly eosinophils. BE has also been distinguished as a characteristic of bullous pemphigoid [40,41]. Peripheral eosinophilia is associated with increased levels of IL-5, the key mediator of eosinophil activation produced by T helper cells and mast cells [42]. Elevated levels of IL-5 in serum and blister fluids have been reported in 50–60% of bullous pemphigoid (BP) cases [43]. Moreover, eotaxin-1/CCL11, a chemokine also known as eosinophil chemotactic protein, is overexpressed by keratinocytes within the BP blisters, which may instigate the recruitment of eosinophils into the blister site [44,45,46].
2.2. Systemic Diseases Associated with Oral Lesions and Eosinophilia
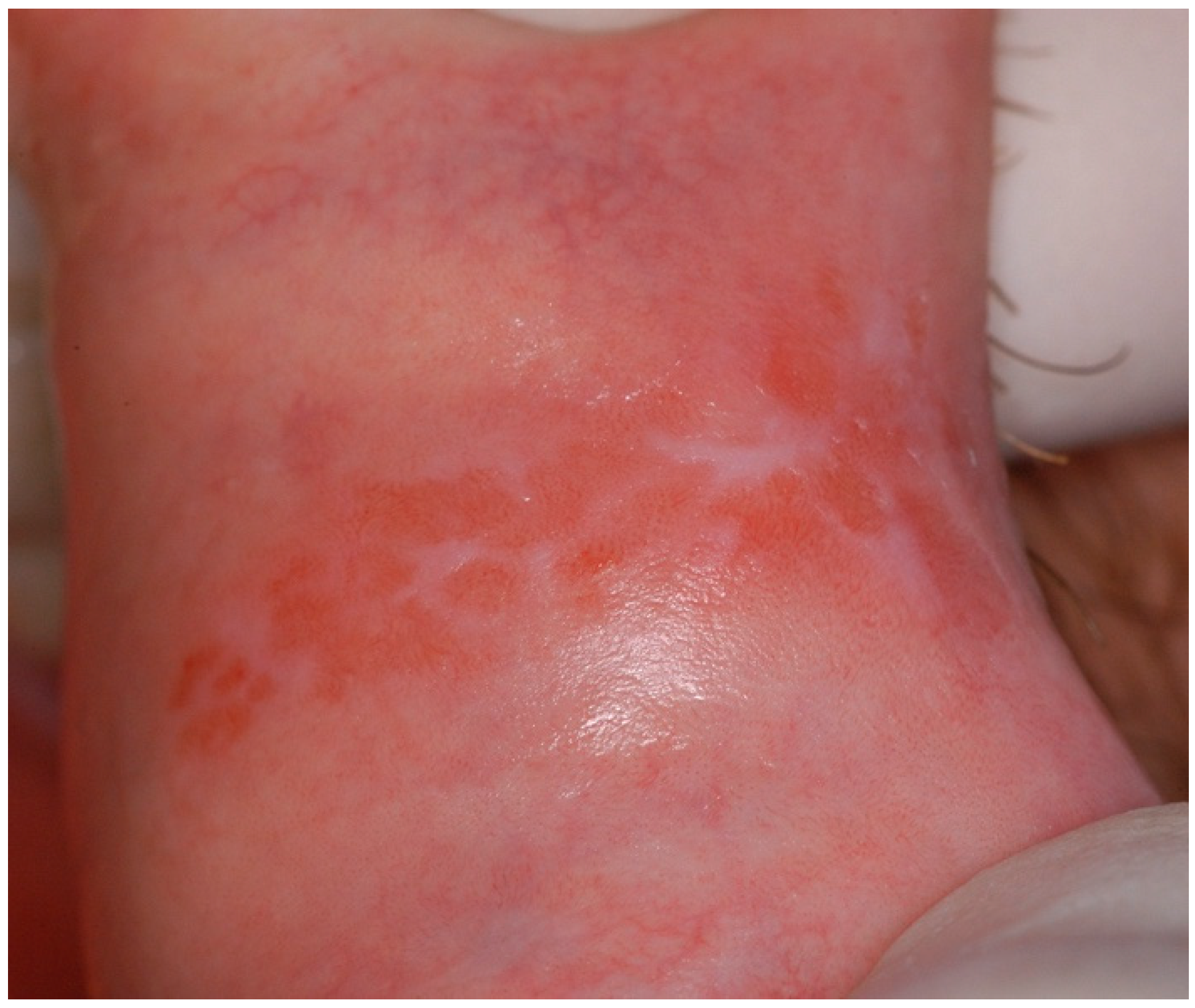
- Crohn’s disease (CD) is a chronic inflammatory bowel disease that affects the GI tract. Oral manifestations of CD (oral Crohn’s) are common and include ulcers, the fissuring of the lip, cobblestoning of the buccal mucosa, angular cheilitis, mucosal polyps and perioral erythema (Figure 7). A blood investigation into CD patients revealed leucocytosis and eosinophilia, with eosinophils identified as important contributing cells to tissue immune cell infiltration [47,48].
- Kimura’s disease is a rare chronic inflammatory disease associated with the systematic elevation of eosinophils levels. First described by Kimura et al. [49], it presents as a non-tender subcutaneous lesion in the head and neck region, with only a few reports in the oral cavity [50]. Histopathological examination indicates a nodular architecture and follicular hyperplasia with intense eosinophilic infiltration [51,52,53].
- Hypereosinophilic syndrome (HES) is a rare disorder characterised by a persistent absolute eosinophil count ≥ 1.5 × 109/L, whereby “persistent” denotes the detection of HE on at least two measurements with a minimum of a 2-week interval between them, together with the documentation of eosinophilic infiltrates or the presence of their products, eosinophil-associated organ damage, and the exclusion of another underlying disorder as the primary driver of organ damage [11] The oral presentation of HES manifests as painful mucosal lesions presenting as ulcerations and erosions localized to the lips, gingiva, tongue, and palatal mucosa, all associated with intense eosinophilic infiltration [54].
- IgG4-related disease is a systemic immune-mediated condition characterised by an elevation in serum IgG4 and IgE levels and eosinophilia [55,56]. It can affect any part of the body and is characterised by pancreatitis, retroperitoneal fibrosis, mucosal and glandular infiltration, as well as cutaneous manifestations [36]. The salivary glands are the third most affected tissues after the pancreas and biliary tract [57], mainly resulting in IgG4-related Mikulicz Diseases (IgG4-MD) and IgG4-related Chronic Sclerosing Sialadentis (IgG4-CSS) [58]. In addition, the tongue and the palate can be involved, resulting in tumefactive or erosive lesions [59]. Although the involvement of the oral cavity is an infrequent manifestation of IgG4-related disease, it should be taken into consideration as a possible differential diagnosis once neoplastic conditions are excluded. The histological examination represents the mainstay for the diagnosis of this condition [60].
- Eosinophilic granulomatosis with polyangiitis (EGPA), formerly known as Churg-Strauss syndrome, is a rare condition, immune-mediated, and multisystemic disease characterised by BE and TE, late-onset asthma, and small-to-medium vessel vasculitis [61]. Oral lesions represent an uncommon presentation; however, ulcers involve the palate, tongue, and floor of the mouth [62,63]. Gingival bleeding and painful blisters on the tongue have been reported by some research groups. In all these cases, the unresponsiveness to local measures and the detection of granular or necrotic lesions exhibiting an eosinophilic inflammatory infiltrate on biopsy may guide the tentative diagnosis. Also, the salivary glands may be involved in granulomatous inflammation, resulting in a marked swelling [64]. Finally, another recent case report by Suzuki et al. [65] described swelling of the floor of the mouth and cervical soft tissue-mimicking IgG4-related disease as an initial manifestation of EGPA.
3. Role of Eosinophils in Oral Precancerous Lesions
4. Role of Eosinophils in Oral Cancer
5. Discussion
6. Limitations and Future Implications
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
Abbreviations
References
- Ehrlich, P. Uber die Specifischen Granulation des Blutes. Archiv fur Anatomie und Physiologie; Physiologische Abteilung; Leipzig, Veit & Company: Leipzig, Germany, 1879. [Google Scholar]
- Saraswathi, T.; Nalinkumar, S.; Ranganathan, K.; Umadevi, R.; Elizabeth, J. Eosinophils in health and disease: An overview. J. Oral Maxillofac. Pathol. 2003, 7, 31–33. [Google Scholar]
- Kovalszki, A.; Weller, P.F. Eosinophilia. Prim. Care 2016, 43, 607–617. [Google Scholar] [CrossRef]
- Wardlaw, A.J.; Moqbel, R.; Kay, A.B. Eosinophils: Biology and role in disease. Adv. Immunol. 1995, 60, 151–266. [Google Scholar] [PubMed]
- Long, H.; Zhang, G.; Wang, L.; Lu, Q. Eosinophilic Skin Diseases: A Comprehensive Review. Clin. Rev. Allergy Immunol. 2016, 50, 189–213. [Google Scholar] [CrossRef] [PubMed]
- Varricchi, G.; Galdiero, M.R.; Loffredo, S.; Lucarini, V.; Marone, G.; Mattei, F.; Marone, G.; Schiavoni, G. Eosinophils: The unsung heroes in cancer? Oncoimmunology 2018, 7, e1393134. [Google Scholar] [CrossRef] [PubMed]
- Stone, K.D.; Prussin, C.; Metcalfe, D.D. IgE, mast cells, basophils, and eosinophils. J. Allergy Clin. Immunol. 2010, 125 (Suppl. S2), S73–S80. [Google Scholar] [CrossRef]
- Lombardi, C.; Berti, A.; Cottini, M. The emerging roles of eosinophils: Implications for the targeted treatment of eosinophilic-associated inflammatory conditions. Curr. Res. Immunol. 2022, 3, 42–53. [Google Scholar] [CrossRef] [PubMed]
- Blausen Medical. Medical gallery of Blausen Medical 2014. WikiJournal Med. 2014, 1, 1–79. [Google Scholar] [CrossRef]
- Valent, P.; Klion, A.D.; Horny, H.P.; Roufosse, F.; Gotlib, J.; Weller, P.F.; Hellmann, A.; Metzgeroth, G.; Leiferman, K.M.; Arock, M.; et al. Contemporary consensus proposal on criteria and classification of eosinophilic disorders and related syndromes. J. Allergy Clin. Immunol. 2012, 130, 607–612.e9. [Google Scholar] [CrossRef]
- Valent, P.; Klion, A.D.; Roufosse, F.; Simon, D.; Metzgeroth, G.; Leiferman, K.M.; Schwaab, J.; Butterfield, J.H.; Sperr, W.R.; Sotlar, K.; et al. Proposed refined diagnostic criteria and classification of eosinophil disorders and related syndromes. Allergy 2023, 78, 47–59. [Google Scholar] [CrossRef]
- Ponath, P.D.; Qin, S.; Ringler, D.J.; Clark-Lewis, I.; Wang, J.; Kassam, N.; Smith, H.; Shi, X.; Gonzalo, J.A.; Newman, W.; et al. Cloning of the human eosinophil chemoattractant, eotaxin. Expression, receptor binding, and functional properties suggest a mechanism for the selective recruitment of eosinophils. J. Clin. Investig. 1996, 97, 604–612. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.J.; Jacobsen, E.A.; McGarry, M.P.; Schleimer, R.P.; Lee, N.A. Eosinophils in health and disease: The LIAR hypothesis. Clin. Exp. Allergy 2010, 40, 563–575. [Google Scholar] [CrossRef] [PubMed]
- Davoine, F.; Lacy, P. Eosinophil cytokines, chemokines, and growth factors: Emerging roles in immunity. Front. Immunol. 2014, 5, 570. [Google Scholar] [CrossRef] [PubMed]
- Simon, H.U.; Yousefi, S.; Germic, N.; Arnold, I.C.; Haczku, A.; Karaulov, A.V.; Simon, D.; Rosenberg, H.F. The Cellular Functions of Eosinophils: Collegium Internationale Allergologicum (CIA) Update 2020. Int. Arch. Allergy Immunol. 2020, 181, 11–23. [Google Scholar] [CrossRef] [PubMed]
- Wechsler, M.E.; Munitz, A.; Ackerman, S.J.; Drake, M.G.; Jackson, D.J.; Wardlaw, A.J.; Dougan, S.K.; Berdnikovs, S.; Schleich, F.; Matucci, A.; et al. Eosinophils in Health and Disease: A State-of-the-Art Review. Mayo Clin. Proc. 2021, 96, 2694–2707. [Google Scholar] [CrossRef] [PubMed]
- Redd, W.D.; Dellon, E.S. Eosinophilic Gastrointestinal Diseases Beyond the Esophagus: An Evolving Field and Nomenclature. Gastroenterol. Hepatol. 2022, 18, 522–528. [Google Scholar]
- von Arnim, U.; Malfertheiner, P. Eosinophilic esophagitis—Treatment of eosinophilic esophagitis with drugs: Corticosteroids. Dig. Dis. 2014, 32, 126–129. [Google Scholar] [CrossRef] [PubMed]
- Collins, M.H.; Capocelli, K.; Yang, G.-Y. Eosinophilic gastrointestinal disorders pathology. Front. Med. 2018, 4, 261. [Google Scholar] [CrossRef] [PubMed]
- Peurala, E.; Tuominen, M.; Löyttyniemi, E.; Syrjänen, S.; Rautava, J. Eosinophilia is a favorable prognostic marker for oral cavity and lip squamous cell carcinoma. Apmis 2018, 126, 201–207. [Google Scholar] [CrossRef]
- Cormier, S.A.; Taranova, A.G.; Bedient, C.; Nguyen, T.; Protheroe, C.; Pero, R.; Dimina, D.; Ochkur, S.I.; O’neill, K.; Colbert, D.; et al. Pivotal Advance: Eosinophil infiltration of solid tumors is an early and persistent inflammatory host response. J. Leukoc. Biol. 2006, 79, 1131–1139. [Google Scholar] [CrossRef]
- Ficarra, G.; Prignano, F.; Romagnoli, P. Traumatic eosinophilic granuloma of the oral mucosa: A CD30+(Ki-1) lymphoproliferative disorder? Oral Oncol. 1997, 33, 375–379. [Google Scholar] [CrossRef] [PubMed]
- Fonseca, F.P.; de Andrade, B.A.; Coletta, R.D.; Vargas, P.A.; Lopes, M.A.; de Almeida, O.P.; Santos-Silva, A.R. Clinicopathological and immunohistochemical analysis of 19 cases of oral eosinophilic ulcers. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2013, 115, 532–540. [Google Scholar] [CrossRef] [PubMed]
- Segura, S.; Pujol, R.M. Eosinophilic ulcer of the oral mucosa: A distinct entity or a non-specific reactive pattern? Oral Dis. 2008, 14, 287–295. [Google Scholar] [CrossRef] [PubMed]
- Chatzistamou, I.; Doussis-Anagnostopoulou, I.; Georgiou, G.; Gkilas, H.; Prodromidis, G.; Andrikopoulou, M.; Sklavounou, A. Traumatic ulcerative granuloma with stromal eosinophilia: Report of a case and literature review. J. Oral Maxillofac. Surg. 2012, 70, 349–353. [Google Scholar] [CrossRef]
- Sugaya, N.; Martignago, F.; Pinto, D.; Migliari, D. Recurrent Oral Eosinophilic Ulcers of the Oral Mucosa. A Case Report. Open Dent. J. 2018, 12, 19–23. [Google Scholar] [CrossRef] [PubMed]
- Chandra, S.; Raju, S.; Sah, K.; Anand, P. Traumatic ulcerative granuloma with stromal eosinophilia. Arch. Iran Med. 2014, 17, 91–94. [Google Scholar]
- Iandolo, A.; Amato, A.; Sangiovanni, G.; Argentino, S.; Pisano, M. Riga-Fede disease: A systematic review and report of two cases. Eur. J. Paediatr. Dent. 2021, 22, 323–331. [Google Scholar]
- Ceyhan, A.M.; Yildirim, M.; Basak, P.Y.; Akkaya, V.B.; Ayata, A. Traumatic lingual ulcer in a child: Riga-Fede disease. Clin. Exp. Dermatol. 2009, 34, 186–188. [Google Scholar] [CrossRef]
- Lakkam, B.D.; Astekar, M.; Alam, S.; Saleem, A. Traumatic ulcerative granuloma with stromal eosinophilia: A puzzle. J. Oral Maxillofac. Pathol. 2021, 25 (Suppl. S1), S42–S45. [Google Scholar]
- Prathap, A.; Areekkal, R.R.; Thomas, E.; Pratap, N.; Udayakumar, V. Eosinophilic Granuloma of the Mandible. Ann. Maxillofac. Surg. 2020, 10, 254–257. [Google Scholar] [CrossRef]
- Sai, S.; Fujii, K.; Masui, F.; Kida, Y. Solitary eosinophilic granuloma of the sternum. J. Orthop. Sci. 2005, 10, 108–111. [Google Scholar] [CrossRef] [PubMed]
- Kamath, V.V.; Setlur, K.; Yerlagudda, K. Oral lichenoid lesions—A review and update. Indian J. Dermatol. 2015, 60, 102. [Google Scholar] [CrossRef] [PubMed]
- Lodolo, M.; Gobbo, M.; Bussani, R.; Torelli, L.; Rupel, K.; Ottaviani, G.; Poropat, A.; Biasotto, M. Histopathology of oral lichen planus and oral lichenoid lesions: An exploratory cross-sectional study. Oral Dis. 2023, 29, 1259–1268. [Google Scholar] [CrossRef] [PubMed]
- Ismail, S.B.; Kumar, S.K.; Zain, R.B. Oral lichen planus and lichenoid reactions: Etiopathogenesis, diagnosis, management and malignant transformation. J. Oral Sci. 2007, 49, 89–106. [Google Scholar] [CrossRef] [PubMed]
- Farah, C.; Balasubramaniam, R.; McCullough, M.J. Contemporary Oral Medicine; Springer: Berlin/Heidelberg, Germany, 2019. [Google Scholar]
- Chen, X.; Zhao, W.; Jin, H.; Li, L. Risk Factors for Mucosal Involvement in Bullous Pemphigoid and the Possible Mechanism: A Review. Front. Med. 2021, 8, 680871. [Google Scholar] [CrossRef] [PubMed]
- Zuo, Y.; Evangelista, F.; Culton, D.; Guilabert, A.; Lin, L.; Li, N.; Diaz, L.; Liu, Z. IgG4 autoantibodies are inhibitory in the autoimmune disease bullous pemphigoid. J. Autoimmun. 2016, 73, 111–119. [Google Scholar] [CrossRef]
- Rashid, H.; Lamberts, A.; Diercks, G.F.H.; Pas, H.H.; Meijer, J.M.; Bolling, M.C.; Horváth, B. Oral Lesions in Autoimmune Bullous Diseases: An Overview of Clinical Characteristics and Diagnostic Algorithm. Am. J. Clin. Dermatol. 2019, 20, 847–861. [Google Scholar] [CrossRef] [PubMed]
- Bernard, P.; Venot, J.; Constant, F.; Bonnetblanc, J.M. Blood eosinophilia as a severity marker for bullous pemphigoid. J. Am. Acad. Dermatol. 1987, 16, 879–881. [Google Scholar] [CrossRef]
- Bushkell, L.L.; Jordon, R.E. Bullous pemphigoid: A cause of peripheral blood eosinophilia. J. Am. Acad. Dermatol. 1983, 8, 648–651. [Google Scholar] [CrossRef]
- Roufosse, F. Targeting the Interleukin-5 Pathway for Treatment of Eosinophilic Conditions Other than Asthma. Front. Med. 2018, 5, 49. [Google Scholar] [CrossRef]
- Kridin, K. Peripheral eosinophilia in bullous pemphigoid: Prevalence and influence on the clinical manifestation. Br. J. Dermatol. 2018, 179, 1141–1147. [Google Scholar] [CrossRef] [PubMed]
- D’Auria, L.; Pietravalle, M.; Mastroianni, A.; Ferraro, C.; Mussi, A.; Bonifati, C.; Giacalone, B.; Ameglio, F. IL-5 levels in the serum and blister fluid of patients with bullous pemphigoid: Correlations with eosinophil cationic protein, RANTES, IgE and disease severity. Arch. Dermatol. Res. 1998, 290, 25–27. [Google Scholar] [CrossRef] [PubMed]
- Frezzolini, A.; Teofoli, P.; Cianchini, G.; Barduagni, S.; Ruffelli, M.; Ferranti, G.; Puddu, P.; De Pita, O. Increased expression of eotaxin and its specific receptor CCR3 in bullous pemphigoid. Eur. J. Dermatol. 2002, 12, 27–31. [Google Scholar]
- Wakugawa, M.; Nakamura, K.; Hino, H.; Toyama, K.; Hattori, N.; Okochi, H.; Yamada, H.; Hirai, K.; Tamaki, K.; Furue, M. Elevated levels of eotaxin and interleukin-5 in blister fluid of bullous pemphigoid: Correlation with tissue eosinophilia. Br. J. Dermatol. 2000, 143, 112–116. [Google Scholar] [CrossRef] [PubMed]
- Jacobs, I.; Ceulemans, M.; Wauters, L.; Breynaert, C.; Vermeire, S.; Verstockt, B.; Vanuytsel, T. Role of Eosinophils in Intestinal Inflammation and Fibrosis in Inflammatory Bowel Disease: An Overlooked Villain? Front. Immunol. 2021, 12, 754413. [Google Scholar] [CrossRef] [PubMed]
- Pecci-Lloret, M.P.; Ramirez-Santisteban, E.; Hergueta-Castillo, A.; Guerrero-Gironés, J.; Oñate-Sánchez, R.E. Oral Manifestations of Crohn’s Disease: A Systematic Review. J. Clin. Med. 2023, 12, 6450. [Google Scholar] [CrossRef]
- Kimura, T.; Yoshimura, S.; Ishikawa, E. On the Unusual Granulation Combined with Hyperplastic Changes of Lymphatic Tissues. Trans. Soc. Pathol. Jpn. 1948, 37, 179–180. [Google Scholar]
- Lei, X.; Yu, D.; Feng, X.; Shen, Y.; Zhu, H. A Rare Kimura’s Disease in the Oral Cavity with Severe Sleep Apnea: Case Report and Literature Review. Medicina 2022, 58, 1810. [Google Scholar] [CrossRef]
- Iida, S.; Fukuda, Y.; Ueda, T.; Sakai, T.; Okura, M.; Kogo, M. Kimura’s disease: Report of a case with presentation in the cheek and upper eyelid. J. Oral Maxillofac. Surg. 2005, 63, 690–693. [Google Scholar] [CrossRef]
- Sato, R.; Bandoh, N.; Goto, T.; Ichikawa, H.; Uemura, A.; Suzuki, S.; Yamaguchi, T.; Aimono, E.; Nishihara, H.; Katada, A.; et al. Kimura Disease Presenting with Buccal Mass: A Case Report and Literature Review. Head Neck Pathol. 2021, 15, 657–662. [Google Scholar] [CrossRef]
- Yadav, V.; Bhagat, A.; Mohapatra, S.; Arora, K.S. Kimura’s disease: A diagnostic dilemma. BMJ Case Rep. 2019, 12, e228194. [Google Scholar] [CrossRef]
- Ionescu, M.A.; Murata, H.; Janin, A. Oral mucosa lesions in hypereosinophilic syndrome—An update. Oral Dis. 2008, 14, 115–122. [Google Scholar] [CrossRef] [PubMed]
- Umehara, H.; Okazaki, K.; Kawa, S.; Takahashi, H.; Goto, H.; Matsui, S.; Ishizaka, N.; Akamizu, T.; Sato, Y.; Kawano, M.; et al. The 2020 revised comprehensive diagnostic (RCD) criteria for IgG4-RD. Mod. Rheumatol. 2021, 31, 529–533. [Google Scholar] [CrossRef] [PubMed]
- Wallace, Z.S.; Naden, R.P.; Chari, S.; Choi, H.; Della-Torre, E.; Dicaire, J.F.; Hart, P.A.; Inoue, D.; Kawano, M.; Khosroshahi, A.; et al. The 2019 American College of Rheumatology/European League Against Rheumatism Classification Criteria for IgG4-Related Disease. Arthritis Rheumatol. 2020, 72, 7–19. [Google Scholar] [CrossRef]
- Geyer, J.T.; Deshpande, V. IgG4-associated sialadenitis. Curr. Opin. Rheumatol. 2011, 23, 95–101. [Google Scholar] [CrossRef] [PubMed]
- Wu, S.; Wang, H. IgG4-related digestive diseases: Diagnosis and treatment. Front. Immunol. 2023, 14, 1278332. [Google Scholar] [CrossRef] [PubMed]
- Pereira, G.G.; Pontes, F.S.C.; Soares, C.D.; de Carvalho, M.G.F.; da Silva, T.A.; Calderaro, D.C.; Ferreira, G.A.; Tanure, L.A.; de Souza, L.L.; Rodrigues-Fernandes, C.I.; et al. Oral and maxillofacial manifestations of IgG4-related disease: A clinicopathological study. J. Oral Pathol. Med. 2022, 51, 493–500. [Google Scholar] [CrossRef] [PubMed]
- Rampi, A.; Lanzillotta, M.; Mancuso, G.; Vinciguerra, A.; Dagna, L. IgG4-Related Disease of the Oral Cavity. Case Series from a Large Single-Center Cohort of Italian Patients. Int. J. Environ. Res. Public Health 2020, 17, 8179. [Google Scholar] [CrossRef]
- White, J.; Dubey, S. Eosinophilic granulomatosis with polyangiitis: A review. Autoimmun Rev. 2023, 22, 103219. [Google Scholar] [CrossRef]
- Noda, S.; Komiya, Y.; Soejima, M. A case of eosinophilic granulomatosis with polyangiitis presented with blisters on the tongue. Clin. Rheumatol. 2022, 41, 1925–1926. [Google Scholar] [CrossRef]
- Otsuka, T.; Iwata, H.; Kosumi, H.; Muramatsu, K.; Ito, T.; Tsujiwaki, M.; Fujita, Y.; Kamaguchi, M.; Kitagawa, Y.; Shimizu, H. Refractory oral ulcers in eosinophilic granulomatosis with polyangiitis. J. Dermatol. 2019, 46, e377–e378. [Google Scholar] [CrossRef] [PubMed]
- Vaglio, A.; Maritati, F.; Zwerina, J. Response to: Eosinophilic granulomatosis with polyangiitis can manifest lacrimal and salivary glands swelling by granulomatous inflammation: A potential mimicker of IgG4-related disease. Ann. Rheum. Dis. 2022, 81, e121. [Google Scholar] [CrossRef]
- Suzuki, T.; Moriyama, M.; Takano, I.; Miyajima, N.; Yoshioka, Y.; Honda, M.; Kondo, M.; Shokei, S.; Araki, A.; Kadota, K.; et al. Eosinophilic granulomatous with polyangiitis complicated by swelling of the oral cavity floor and cervical soft tissue as initial manifestation mimicking IgG4-related disease: A case report. Mod. Rheumatol. Case Rep. 2023, 8, 178–181. [Google Scholar] [CrossRef]
- Mello, F.W.; Miguel, A.F.P.; Dutra, K.L.; Porporatti, A.L.; Warnakulasuriya, S.; Guerra, E.N.S.; Rivero, E.R.C. Prevalence of oral potentially malignant disorders: A systematic review and meta-analysis. J. Oral. Pathol. Med. 2018, 47, 633–640. [Google Scholar] [CrossRef]
- Wetzel, S.L.; Wollenberg, J. Oral Potentially Malignant Disorders. Dent. Clin. N. Am. 2020, 64, 25–37. [Google Scholar] [CrossRef] [PubMed]
- Madhura, M.G.; Gajalakshmi, S.; Kumar, B.V.; Suma, S.; Sarita, Y.; Shweta, R.D. Role of tissue eosinophils in oral Leukoplakia: A pilot study. J. Oral Maxillofac. Pathol. 2015, 19, 286–290. [Google Scholar] [CrossRef]
- Deepthi, G.; Kulkarni, P.G.; Nandan, S.R.K. Eosinophils: An imperative histopathological prognostic indicator for oral squamous cell carcinoma. J. Oral Maxillofac. Pathol. 2019, 23, 307. [Google Scholar] [CrossRef] [PubMed]
- Kaur, N.; Zaheer, S.; Sangwan, S.; Ranga, S. To evaluate eosinophilia (tissue eosinophilia, blood eosinophilia and tissue eosinophilia/blood eosinophilia ratio) in increasing grades/severity of oral neoplastic lesions. J. Cancer Res. Ther. 2023, 19 (Suppl. S1), S206–S211. [Google Scholar]
- Martinelli-Kläy, C.P.; Lombardi, T.; Mendis, B.; Soares, E.G.; Salvado, F.; Courvoisier, D.S.; Mauricio, P. Tissue eosinophilia in oral intraepithelial neoplasia as a probable indicator of invasion. Oral Dis. 2018, 24, 103–108. [Google Scholar] [CrossRef]
- Jain, M.; Kasetty, S.; Sudheendra, U.S.; Tijare, M.; Khan, S.; Desai, A. Assessment of tissue eosinophilia as a prognosticator in oral epithelial dysplasia and oral squamous cell carcinoma—An image analysis study. Pathol. Res. Int. 2014, 2014, 507512. [Google Scholar] [CrossRef]
- Kargahi, N.; Razavi, S.M.; Deyhimi, P.; Homayouni, S. Comparative evaluation of eosinophils in normal mucosa, dysplastic mucosa and oral squamous cell carcinoma with hematoxylin-eosin, Congo red, and EMR1 immunohistochemical staining techniques. Electron. Physician 2015, 7, 1019–1026. [Google Scholar] [PubMed]
- Poncin, A.; Onesti, C.E.; Josse, C.; Boulet, D.; Thiry, J.; Bours, V.; Jerusalem, G. Immunity and Breast Cancer: Focus on Eosinophils. Biomedicines 2021, 9, 1087. [Google Scholar] [CrossRef] [PubMed]
- Fernández-Aceñero, M.J.; Galindo-Gallego, M.; Sanz, J.; Aljama, A. Prognostic influence of tumor-associated eosinophilic infiltrate in colorectal carcinoma. Cancer 2000, 88, 1544–1548. [Google Scholar] [CrossRef]
- Luna-Moré, S.; Florez, P.; Ayala, A.; Diaz, F.; Santos, A. Neutral and acid mucins and eosinophil and argyrophil crystalloids in carcinoma and atypical adenomatous hyperplasia of the prostate. Pathol. Res. Pract. 1997, 193, 291–298. [Google Scholar] [CrossRef] [PubMed]
- Takeuchi, E.; Ogino, H.; Kondo, K.; Okano, Y.; Ichihara, S.; Kunishige, M.; Kadota, N.; Machida, H.; Hatakeyama, N.; Naruse, K.; et al. An increased relative eosinophil count as a predictive dynamic biomarker in non-small cell lung cancer patients treated with immune checkpoint inhibitors. Thorac. Cancer 2024, 15, 248–257. [Google Scholar] [CrossRef] [PubMed]
- Ishibashi, S.; Ohashi, Y.; Suzuki, T.; Miyazaki, S.; Moriya, T.; Satomi, S.; Sasano, H. Tumor-associated tissue eosinophilia in human esophageal squamous cell carcinoma. Anticancer Res. 2006, 26, 1419–1424. [Google Scholar] [PubMed]
- Siddiqui, S.; Jaiswal, R.; Hashmi, G.S. Quantitative analysis of tumor-associated tissue eosinophils and tumor-associated blood eosinophils in oral squamous cell carcinoma. J. Oral Maxillofac. Pathol. 2020, 24, 131–137. [Google Scholar] [CrossRef] [PubMed]
- Molin, D.; Glimelius, B.; Sundström, C.; Venge, P.; Enblad, G. The serum levels of eosinophil cationic protein (ECP) are related to the infiltration of eosinophils in the tumours of patients with Hodgkin’s disease. Leuk. Lymphoma 2001, 42, 457–465. [Google Scholar] [CrossRef] [PubMed]
- Crusz, S.M.; Balkwill, F.R. Inflammation and cancer: Advances and new agents. Nat. Rev. Clin. Oncol. 2015, 12, 584–596. [Google Scholar] [CrossRef]
- Leighton, S.E.; Teo, J.G.; Leung, S.F.; Cheung, A.Y.; Lee, J.C.; van Hasselt, C.A. Prevalence and prognostic significance of tumor-associated tissue eosinophilia in nasopharyngeal carcinoma. Cancer 1996, 77, 436–440. [Google Scholar] [CrossRef]
- Lorena, S.C.; Dorta, R.G.; Landman, G.; Nonogaki, S.; Oliveira, D.T. Morphometric analysis of the tumor associated tissue eosinophilia in the oral squamous cell carcinoma using different staining techniques. Histol. Histopathol. 2003, 18, 709–713. [Google Scholar]
- Goldsmith, M.M.; Belchis, D.A.; Cresson, D.H.; Merritt, W.D., 3rd; Askin, F.B. The importance of the eosinophil in head and neck cancer. Otolaryngol. Head Neck Surg. 1992, 106, 27–33. [Google Scholar] [CrossRef]
- Lowe, D.; Fletcher, C.D. Eosinophilia in squamous cell carcinoma of the oral cavity, external genitalia and anus—Clinical correlations. Histopathology 1984, 8, 627–632. [Google Scholar] [CrossRef] [PubMed]
- Davoine, F.; Sim, A.; Tang, C.; Fisher, S.; Ethier, C.; Puttagunta, L.; Wu, Y.; McGaw, W.T.; Yu, D.; Cameron, L.; et al. Eosinophils in human oral squamous carcinoma; role of prostaglandin D2. J. Inflamm. 2013, 10, 4. [Google Scholar] [CrossRef] [PubMed]
- Ellyard, J.I.; Simson, L.; Parish, C.R. Th2-mediated anti-tumour immunity: Friend or foe? Tissue Antigens 2007, 70, 1–11. [Google Scholar] [CrossRef]
- Hogan, S.P. Recent advances in eosinophil biology. Int. Arch. Allergy Immunol. 2007, 143 (Suppl. S1), 3–14. [Google Scholar] [CrossRef]
- Munitz, A.; Levi-Schaffer, F. Eosinophils: ‘New’ roles for ‘old’ cells. Allergy 2004, 59, 268–275. [Google Scholar] [CrossRef] [PubMed]
- Grisaru-Tal, S.; Itan, M.; Klion, A.D.; Munitz, A. A new dawn for eosinophils in the tumour microenvironment. Nat. Rev. Cancer 2020, 20, 594–607. [Google Scholar] [CrossRef] [PubMed]
- Sakkal, S.; Miller, S.; Apostolopoulos, V.; Nurgali, K. Eosinophils in Cancer: Favourable or Unfavourable? Curr. Med. Chem. 2016, 23, 650–666. [Google Scholar] [CrossRef]
- Dorta, R.G.; Landman, G.; Kowalski, L.P.; Lauris, J.R.; Latorre, M.R.; Oliveira, D.T. Tumour-associated tissue eosinophilia as a prognostic factor in oral squamous cell carcinomas. Histopathology 2002, 41, 152–157. [Google Scholar] [CrossRef]
- Goldsmith, M.M.; Cresson, D.H.; Askin, F.B. The prognostic significance of stromal eosinophilia in head and neck cancer. Otolaryngol. Head Neck Surg. 1987, 96, 319–324. [Google Scholar] [CrossRef] [PubMed]
- Sahni, P.; Patel, A.; Md, S.; Hallur, J.; Gujjar, P.K. Tumor Associated Tissue Eosinophilia in Oral Squamous Cell Carcinoma: A Histo-Chemical Analysis. Malays. J. Med. Sci. 2015, 22, 21–25. [Google Scholar] [PubMed]
- Alrawi, S.J.; Tan, D.; Stoler, D.L.; Dayton, M.; Anderson, G.R.; Mojica, P.; Douglas, W.; Hicks, W., Jr.; Rigual, N.; Loree, T. Tissue eosinophilic infiltration: A useful marker for assessing stromal invasion, survival and locoregional recurrence in head and neck squamous neoplasia. Cancer J. 2005, 11, 217–225. [Google Scholar] [CrossRef]
- Falconieri, G.; Luna, M.A.; Pizzolitto, S.; DeMaglio, G.; Angione, V.; Rocco, M. Eosinophil-rich squamous carcinoma of the oral cavity: A study of 13 cases and delineation of a possible new microscopic entity. Ann. Diagn. Pathol. 2008, 12, 322–327. [Google Scholar] [CrossRef] [PubMed]
- Horiuchi, K.; Mishima, K.; Ohsawa, M.; Sugimura, M.; Aozasa, K. Prognostic factors for well-differentiated squamous cell carcinoma in the oral cavity with emphasis on immunohistochemical evaluation. J. Surg. Oncol. 1993, 53, 92–96. [Google Scholar] [CrossRef] [PubMed]
- Wong, D.T.; Bowen, S.M.; Elovic, A.; Gallagher, G.T.; Weller, P.F. Eosinophil ablation and tumor development. Oral Oncol. 1999, 35, 496–501. [Google Scholar] [CrossRef]
- Tostes Oliveira, D.; Tjioe, K.C.; Assao, A.; Sita Faustino, S.E.; Lopes Carvalho, A.; Landman, G.; Kowalski, L.P. Tissue eosinophilia and its association with tumoral invasion of oral cancer. Int. J. Surg. Pathol. 2009, 17, 244–249. [Google Scholar] [CrossRef]
- Rakesh, N.; Devi, Y.; Majumdar, K.; Reddy, S.S.; Agarwal, K. Tumour associated tissue eosinophilia as a predictor of locoregional recurrence in oral squamous cell carcinoma. J. Clin. Exp. Dent. 2015, 7, e1–e6. [Google Scholar] [CrossRef]
- Debta, P.; Debta, F.M.; Chaudhary, M.; Bussari, S. Evaluation of myeloid cells (tumor-associated tissue eosinophils and mast cells) infiltration in different grades of oral squamous cell carcinoma. Indian J. Med. Paediatr. Oncol. 2016, 37, 158–167. [Google Scholar] [CrossRef]
- Sethi, A.; Shetty, D.C.; Rathore, A.S.; Tandon, A.; Juneja, S.; Gulati, N. Quantitative assessment of CD15 positive tissue eosinophils in Oral Squamous Cell Carcinoma: Effects on mast cells and tumor angiogenesis. Minerva Stomatol. 2020, 69, 133–140. [Google Scholar] [CrossRef]
- Joshi, P.S.; Kaijkar, M.S. A histochemical study of tissue eosinophilia in oral squamous cell carcinoma using Congo red staining. Dent. Res. J. 2013, 10, 784–789. [Google Scholar]
- Yu, Y.R.; Hotten, D.F.; Malakhau, Y.; Volker, E.; Ghio, A.J.; Noble, P.W.; Kraft, M.; Hollingsworth, J.W.; Gunn, M.D.; Tighe, R.M. Flow Cytometric Analysis of Myeloid Cells in Human Blood, Bronchoalveolar Lavage, and Lung Tissues. Am. J. Respir. Cell Mol. Biol. 2016, 54, 13–24. [Google Scholar] [CrossRef] [PubMed]
- Hassani, M.; van Staveren, S.; van Grinsven, E.; Bartels, M.; Tesselaar, K.; Leijte, G.; Kox, M.; Pickkers, P.; Vrisekoop, N.; Koenderman, L. Characterization of the phenotype of human eosinophils and their progenitors in the bone marrow of healthy individuals. Haematologica 2020, 105, e52–e56. [Google Scholar] [CrossRef] [PubMed]
- Reddy, C.N.; Belaldavar, B.P.; Havaldar, R.R. Study of Efficacy of Intraoral Submucosal Injections of Corticosteroids and Placentrex in the Management of Oral Submucous Fibrosis. Indian J. Otolaryngol. Head Neck Surg. 2022, 74 (Suppl. S2), 1996–2001. [Google Scholar] [CrossRef] [PubMed]
- Lowe, D.; Jorizzo, J.; Hutt, M.S. Tumour-associated eosinophilia: A review. J. Clin. Pathol. 1981, 34, 1343–1348. [Google Scholar] [CrossRef] [PubMed]
- Conticello, C.; Pedini, F.; Zeuner, A.; Patti, M.; Zerilli, M.; Stassi, G.; Messina, A.; Peschle, C.; De Maria, R. IL-4 protects tumor cells from anti-CD95 and chemotherapeutic agents via up-regulation of antiapoptotic proteins. J. Immunol. 2004, 172, 5467–5477. [Google Scholar] [CrossRef] [PubMed]
- Kumar, V.A.A.; Fausto, N. Pathologic Basis of Disease; W.B. Saunders: Philadelphia, PA, USA, 2010; pp. 79–109, 259–330. [Google Scholar]
- Martinelli-Kläy, C.P.; Mendis, B.R.; Lombardi, T. Eosinophils and oral squamous cell carcinoma: A short review. J. Oncol. 2009, 2009, 310132. [Google Scholar] [CrossRef] [PubMed]
- Ishikawa, T.; Yu, M.C.; Arbesman, C.E. Electron microscopic demonstration of phagocytosis of Candida albicans by human eosinophilic leukocytes. J. Allergy Clin. Immunol. 1972, 50, 183–187. [Google Scholar] [CrossRef]
- Macchia, I.; La Sorsa, V.; Urbani, F.; Moretti, S.; Antonucci, C.; Afferni, C.; Schiavoni, G. Eosinophils as potential biomarkers in respiratory viral infections. Front. Immunol. 2023, 14, 1170035. [Google Scholar] [CrossRef]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Systemic Diseases Associated with Oral Lesions and Eosinophilia | |
|---|---|
| Disease | Oral Manifestations |
| Crohn’s disease (cd) | Ulcers, fissuring of the lip, cobblestoning of the buccal mucosa, angular cheilitis, mucosal polyps and perioral erythema |
| Kimura’s disease | A non-tender subcutaneous lesion in the head and neck region |
| Hypereosinophilic syndrome (HES) | Painful mucosal lesions presenting as ulcerations and erosions localised to the lips, gingiva, tongue, and palatal mucosa |
| IgG4-related disease | Tumefactive or erosive lesions on the tongue or palate |
| Eosinophilic granulomatosis with polyangiitis (EGPA) | Ulcers involving the palate, tongue, and floor of the mouth, gingival bleeding, and tongue blisters |
| Study | Premalignant Lesion Sample Size (n): (Type) | Method of Counting Eosinophils | Main Findings | Probability (p-Value) |
|---|---|---|---|---|
| Jain et al., 2014 [72] | 20: (dysplasia) | Congo red stain | No significant difference in the degree of dysplasia and eos count. | (p = 0.652). |
| Madhura et al., 2015 [68] | 59: (leukoplakia) | H&E | ↑ TEC in oral leukoplakia compared to normal tissues. Oral leukoplakia versus control | (p = 0.001). |
| Kargahi et al., 2015 [73] | 20: (dysplasia) | H&E, Congo red stain and IHC | ↑ Number of eosinophils in dysplastic mucosa compared to normal mucosa and in OSCC compared to dysplastic mucosa | (p < 0.001). |
| Martinelli-Kläy et al., 2018 [71] | 16: (OIN-1), 18: (OIN-2), 17: (OIN-3) | H&E | Eos distribution is associated with diagnosis severity | (p < 0.01). |
| Deepthi et al., 2019 [69] | 20: ( OED and oral leukoplakia) | Congo red stain | TATE may play a role in stromal invasion | (p < 0.05). |
| Kaur et al., 2023 [70] | 38: (leukoplakia) 32: (dysplasia) | H&E | TATE with TABE are independent prognostic markers in premalignant and malignant OSCC. ↑ tissue eos is a favourable pre-malignancy prognosis; ↑ TABE is a poor prognosis in high-grade OSCC. | (p < 0.001). |
| Study | Oral Cancer Sample Size (n) | Method of Diagnosis | Main Findings | Probability (p-Value) |
|---|---|---|---|---|
| Lowe and Fletcher, 1984 [85] | 136 | N/R | ↑ tissue eosinophilia is related to tumour histological differentiation and is associated with favourable prognosis. ↑ Circulating eosinophilia is associated with metastatic disease and poor prognosis. | (p value; N/R). |
| Goldsmith et al., 1987 [93] | 16 | H&E | Stromal eosinophilia is significantly correlated with a favourable outcome. | (p = 0.018). |
| Goldsmith et al., 1992 [84] | 51 | H&E | ↑eosinophilia in HNSCC stroma is a favourable prognostic indicator. Furthermore, high-grade TATE may have a protective effect on the development of distant metastasis. | (p < 0.001), (p < 0.05), respectively. |
| Horiuchi et al., 1993 [97] | 31 | H&E | ↑ eos infiltration and the expression of the HLA-DR antigen on tumour cells shows an unfavourable prognosis. | (p < 0.05). |
| Dorta et al., 2002 [92] | 125 | Morphometric analysis. (a 25-point ocular graticle under 800 magnification) | Blood eosinophilia was present in 34.4% of cases; tissue eosinophilia was present in 45.6% of cases. ↑ TATE is a possible favourable prognostic factor in OSCC clinical TNM stages II/III. | (p = 0.015). |
| Alrawi et al., 2005 [95] | 4 | H&E | ↑ TEC is a histopathologic marker associated with tumour invasion and is a clinical predictor for aggressive tumourigenesis. | (p < 0.005). |
| Falconieri et al., 2008 [96] | 13 | H&E | ↑ eos infiltrate is associated with stromal invasion in OSCC. | (p value; N/R). |
| Tostes Oliveira et al., 2009 [99] | 43 | H&E | No statistically significant association between ↑ TATE and muscular infiltration in OSCC. The close relationship between eosinophils and striated muscular fibre damage is frequently observed; this suggests that ↑ TATE is associated with OSCC invasiveness. Overall survival and disease-free survival rates were equivalent for both OSCC with intense and absent/mild tissue eosinophilia. | (p = 0.009). |
| Jain et al., 2014 [72] | 40 | Congo red stain | ↑ TEC in OSCC compared to dysplasia suggests its role in the stromal invasion; non-metastatic cases showed ↑ eso counts more than metastatic carcinomas. Eosinophilia showed a favourable histopathological prognostic factor in OSCC. | p < 0.0001, (p < 0.0001), respectively |
| Sahni et al., 2015 [94] | 24 | Congo red stain | ↑ eos infiltration in the well-differentiated lesions compared to the lower grades. Eosinophils play a positive role in circumventing tumour invasion | (p = 0.006). |
| Kargahi et al., 2015 [73] | 20 | H&E, Congo red, and IHC | ↑ TEC in dysplastic mucosa compared to normal mucosa. | (p < 0.001). |
| Rakesh et al., 2015 [100] | 14 | H&E | ↑ TATE was significantly associated with Loco regional recurrence. | (p < 0.001). |
| Debta et al., 2016 [101] | 30 | H&E | Among 30 cases of OSCC, 63.33% were TATE+, and 36.66% were TATE-. Eosinophil infiltrates ↓, from tumour Stage 1 to Stage 3 and ↓ from well to poorly differentiated carcinoma. | (p < 0.05). |
| Martinelli-Kläy et al., 2018 [71] | 32 | H&E | The distribution of eosinophils per 10 hpf was significantly associated with the severity of the diagnosis. Moreover, although not significantly different, non-metastatic invasive OSCC had a higher number of cases (68.2%) with ≥22 eos/10 hpf contrasting with 50% in metastatic OSCC | (p < 0.01). |
| Peurala et al., 2018 [20] | 83 (oral cavity); 16 (lip SCC) | H&E | ↑ TATE showed significantly better survival than ↓ TATE. TATE is a prognostic marker for oral and lip SCC: more than 4 eosinophils/HPF may predict a more favourable prognosis | (p = 0.0136). |
| Deepthi et al., 2019 [69] | 50 | Congo red stain | ↑ TEC in OSCC compared to OED. Mean TEC = 2.12 in OED and 4.31 in OSCC. ↑ TEC is a poor prognosis in OSCC. | (p = 0.000026). |
| Siddiqui et al., 2020 [79] | 30 | H&E | ↑ TATE value associated with poorly differentiated carcinoma. Statistically significant correlation between TATE and OSCC histological grade. Eosinophilia of the peripheral blood = adverse sign in OSCC patients | (p ≤ 0.001). |
| Sethi et al., 2020 [102] | 60 | IHC (anti-CD15 ab) | Eosinophil count correlates with tumour differentiation. Quantification did not correlate with clinical staging. The mean numbers of eosinophils in well to moderately differentiated OSCC = 15.37 ± 11.86. The mean numbers of eosinophils in poorly differentiated OSCC = 12.62 ± 14.30. | (p; no access to full text article) |
| Kaur et al., 2023 [70] | 80 | H&E | ↑ TATE showed a favourable prognosis; ↑ TATE in premalignant conditions (leucoplakia > dysplasia) was followed by WDSCC, MDSCC, and PDSCC, respectively. ↑ TABE shows poor prognosis in high-grade OSCC and follow-ups. | (p < 0.001). |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Al-Azzawi, H.M.A.; Paolini, R.; Cirillo, N.; O’Reilly, L.A.; Mormile, I.; Moore, C.; Yap, T.; Celentano, A. Eosinophils in Oral Disease: A Narrative Review. Int. J. Mol. Sci. 2024, 25, 4373. https://doi.org/10.3390/ijms25084373
Al-Azzawi HMA, Paolini R, Cirillo N, O’Reilly LA, Mormile I, Moore C, Yap T, Celentano A. Eosinophils in Oral Disease: A Narrative Review. International Journal of Molecular Sciences. 2024; 25(8):4373. https://doi.org/10.3390/ijms25084373
Chicago/Turabian StyleAl-Azzawi, Huda Moutaz Asmael, Rita Paolini, Nicola Cirillo, Lorraine Ann O’Reilly, Ilaria Mormile, Caroline Moore, Tami Yap, and Antonio Celentano. 2024. "Eosinophils in Oral Disease: A Narrative Review" International Journal of Molecular Sciences 25, no. 8: 4373. https://doi.org/10.3390/ijms25084373
APA StyleAl-Azzawi, H. M. A., Paolini, R., Cirillo, N., O’Reilly, L. A., Mormile, I., Moore, C., Yap, T., & Celentano, A. (2024). Eosinophils in Oral Disease: A Narrative Review. International Journal of Molecular Sciences, 25(8), 4373. https://doi.org/10.3390/ijms25084373