Abstract
Background: The accuracy of multi-parametric MRI (mpMRI) in the pre-operative staging of prostate cancer (PCa) remains controversial. Objective: The purpose of this study was to evaluate the ability of mpMRI to accurately predict PCa extra-prostatic extension (EPE) on a side-specific basis using a risk-stratified 5-point Likert scale. This study also aimed to assess the influence of mpMRI scan quality on diagnostic accuracy. Patients and Methods: We included 124 men who underwent robot-assisted RP (RARP) as part of the NeuroSAFE PROOF study at our centre. Three radiologists retrospectively reviewed mpMRI blinded to RP pathology and assigned a Likert score (1–5) for EPE on each side of the prostate. Each scan was also ascribed a Prostate Imaging Quality (PI-QUAL) score for assessing the quality of the mpMRI scan, where 1 represents the poorest and 5 represents the best diagnostic quality. Outcome measurements and statistical analyses: Diagnostic performance is presented for the binary classification of EPE, including 95% confidence intervals and the area under the receiver operating characteristic curve (AUC). Results: A total of 231 lobes from 121 men (mean age 56.9 years) were evaluated. Of these, 39 men (32.2%), or 43 lobes (18.6%), had EPE. A Likert score ≥3 had a sensitivity (SE), specificity (SP), NPV, and PPV of 90.4%, 52.3%, 96%, and 29.9%, respectively, and the AUC was 0.82 (95% CI: 0.77–0.86). The AUC was 0.76 (95% CI: 0.64–0.88), 0.78 (0.72–0.84), and 0.92 (0.88–0.96) for biparametric scans, PI-QUAL 1–3, and PI-QUAL 4–5 scans, respectively. Conclusions: MRI can be used effectively by genitourinary radiologists to rule out EPE and help inform surgical planning for men undergoing RARP. EPE prediction was more reliable when the MRI scan was (a) multi-parametric and (b) of a higher image quality according to the PI-QUAL scoring system.
1. Introduction
Multi-parametric magnetic resonance imaging (mpMRI) of the prostate is a valuable tool in the prostate cancer (PCa) diagnostic pathway [1]. Once a diagnosis of PCa has been made on biopsy, the correct assessment of the tumour stage, particularly identifying pathological extra-prostatic extension (EPE), is crucial for directing correct surgical planning, including nerve-sparing (NS), bladder neck sparing, and the extent of apical dissection [2,3,4]. These decisions are pivotal in promoting optimal post-operative functional outcomes without compromising cure from PCa [5]. Moreover, the EPE of a tumour is associated with a higher risk of positive surgical margins (PSM), biochemical recurrence, metastatic disease, and cancer-specific mortality [6,7,8].
It is well recognised that prostate mpMRI has good concordance with PCa on the histopathological evaluation of the final RP specimen for lesions that are within the gland [9]. However, the accurate assessment of PCa EPE has proven to be a more challenging domain for all pre-operative radiological imaging modalities, including MRI. In 2016, de Rooij et al. reported their diagnostic meta-analysis on the accuracy of mpMRI for the local staging of PCa [10]. Overall, MRI had a sensitivity (SE) of 55% (95% CI: 47–63%) and a specificity (SP) of 91% (95% CI: 88–93%) for the prediction of stage pT3a disease, though the authors noted considerable heterogeneity in the studies included. Since this review, although use of mpMRI has become vastly more prominent in the PCa diagnostic pathway around the world, a recent review by Abrams-Pompe et al. clearly demonstrates the ongoing challenges of using this modality for staging purposes [11]. In their review, they continued to demonstrate enormous variation in the diagnostic performance with SE ranging from 0–100%, which the authors attribute to differing sample sizes, event rates, reader experience levels, study designs, heterogeneous non-standardized reporting of mpMRI, and even different definitions of histopathological EPE. Interestingly, although clearly a critical part of the performance and interpretation of mpMRI, technical scan quality has never been assessed as a contributing factor to the accuracy of mpMRI for PCa staging, perhaps because until recently there has been little attention to grading mechanisms for scan quality [12,13,14]. Thus, although mpMRI is now routinely used for pre-operative PCa staging, variation in its performance is still huge and, as such, its role in surgical planning remains controversial.
The objective of this study was to assess the accuracy of mpMRI for the pre-operative local staging of PCa for men undergoing RARP at a high-volume UK academic centre whose scans were performed within the regional referral network. A key secondary objective was to evaluate the effect of technical scan quality on the diagnostic accuracy of EPE prediction.
2. Materials and Methods
2.1. Study Design and Patient Population
We undertook a retrospective review of mpMRI performed in men who had already undergone robot-assisted RP (RARP) at our centre as part of the NeuroSAFE PROOF trial (NCT03317990, ethics approval 17/LO/1978; see Supplementary Material File S1 for full inclusion/exclusion criteria). The STROBE checklist for the reporting of observational studies is included as an online Supplementary Material. Though all the men included in this study were participants in the NeuroSAFE PROOF trial, mpMRI scans were performed as part of their routine clinical care. All participants provided written informed consent.
2.2. Standard of Reference
RARP was performed by three experienced surgeons (GS, SN, TB). Histopathologic examination was performed by a consultant genitourinary pathologist according to the International Society of Urological Pathology (ISUP) 2014 consensus statement [15,16]. Pathologic EPE was diagnosed separately for each side of the prostate where cancer cells were seen outside of the prostate capsule or pseudo-capsule. Seminal vesicle invasion (pT3b) on its own was not classified as EPE. Where an intraprostatic PSM was observed with no evidence of ipsilateral EPE elsewhere, the lobe was excluded from analysis as it is not possible to know whether this focus of PCa extended beyond the limit of the prostate.
2.3. Imaging Protocols and Evaluation
Standard of clinical care mpMRI were performed at 13 different locations in the north and east of London as part of the regional NHS hub and spoke model for the referral of PCa cases for surgery at our centre (Supplementary Figure S1). mpMRI was performed without endorectal coil. Scans were performed using a variety of magnets (1.5 T and 3 T) from different vendors (Philips, GE, and Siemens).
All mpMRI scans were reviewed independently by 3 genitourinary radiologists (CA, DH, TS) who were blinded to the RP final pathology results and who reviewed images under invigilated circumstances in the same room at the same time. Reporting was performed on a bespoke MRI EPE case reporting form (Supplementary Figure S2). Images were reviewed and reported in a locked sequential manner such that T2WI was reported first, then DWI (including apparent diffusion coefficient (ADC) reconstruction maps), then DCE, then the blood serum prostate specific antigen (PSA) level was provided, and finally prostate biopsy information was provided. Where DCE sequences were not available for a given scan (biparametric scans), the score for DCE specifically was omitted by radiologists, but scores were still provided after PSA and biopsy information. At each point, the 3 radiologists separately rated the likelihood of EPE using a risk-stratified 5-point Likert scale: 1, highly unlikely; 2, unlikely; 3, equivocal or indeterminate; 4, likely; and 5, highly likely. Once a score had been assigned and the next imaging sequence or information was provided, the radiologist was not allowed to change any preceding score. Radiologists scored for EPE specifically, but not seminal vesicle invasion (pT3b).
The 3 radiologists (CA, DH, TS) were all fellowship trained and had 20, 5, and 1 years of experience as a consultant, reading >3000, >750, and >750 prostate MRI scans per year, respectively. Before initiating interpretation, the radiologists attended an in-person training session where examples of the MRI scans of patients with and without EPE were reviewed alongside whole mount pathological images from the RP specimen.
Separate to the process described above, the quality of all scans was assessed by means of the Prostate Imaging Quality (PI-QUAL) score from 1 to 5, where 1 represents the poorest and 5 represents the best quality scan (Supplementary Table S1 and Figure S3), by two radiologists (CA and FG) [12]. The PI-QUAL score is derived by evaluating mpMRI scans against a defined set of objective quality criteria in line with Prostate Imaging-Reporting and Data System (PI-RADS) v2 guidelines [17] that cover the adequacy of all three of the mpMRI sequences and additional objective criteria considered to be consistent with a high-quality scan. PI-QUAL scores were given blinded to the EPE Likert score and RP pathology after a wash-out period >4 months. In the case of discordance, the PI-QUAL score was discussed until consensus was reached.
2.4. Sample Size and Power Calculation
Based on the performance reported in the meta-analysis by Rooij et al. [10], the 217 prostate lobes reviewed by the three readers within this study provide 90% power to detect a sensitivity of 80% (95% CI: 65–95) and a specificity of 90% (95% CI: 80–100), assuming a 19% EPE prevalence and a 10% loss to follow-up. The sample size and power were calculated in Stata 16 (College Station, TX, USA).
2.5. Statistical Analysis
First, descriptive statistics were used to compare patients with and without EPE. Continuous variables were reported as means and compared by 2-sided independent t tests, whereas categorical data were reported as proportions and were tested using the chi-squared test. For assessing diagnostic accuracy of mpMRI, the prostate lobe was the unit of analysis as treatment planning incorporating mpMRI occurs on a lobe basis. A Likert score ≥3 was considered positive for EPE. Diagnostic accuracy measures (SE, SP, NPV, PPV, and AUC) were calculated for each reader and combined. We based statistical significance on 95% CIs derived from the exact binomial method. All analyses were conducted in SPSS (version 27, IBM).
3. Results
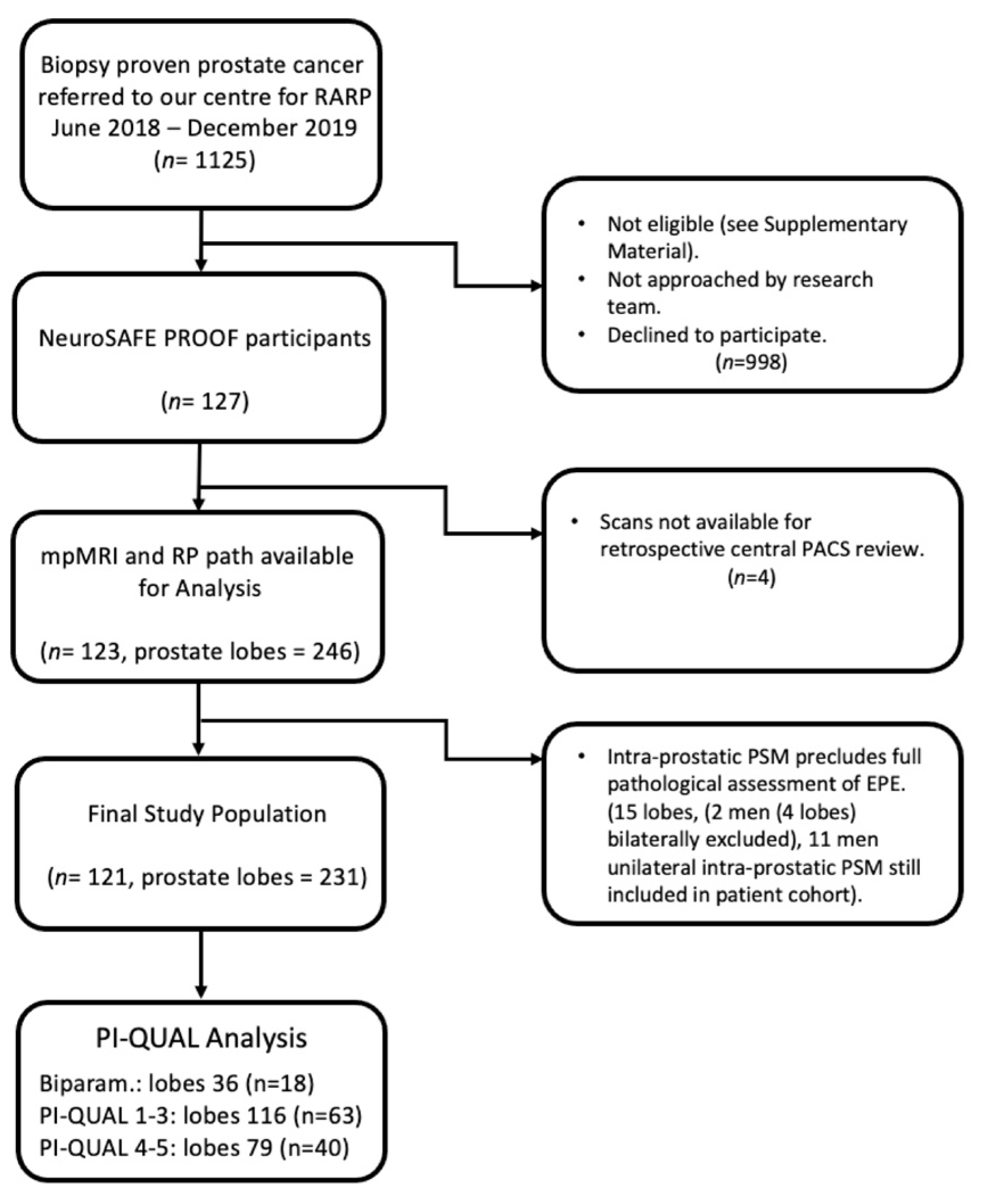
A total of 1125 men underwent RARP at our centre between June 2018 and December 2019. Of these, 127 were participants in the NeuroSAFE PROOF study and eligible for inclusion. Four men were excluded because their mpMRI was not available for review. Of the remaining 123 men, 36 (29.3%) had PSM, of which 13 (10.6%) were ≤1 mm, 3 (2.4%) were 1–3 mm, and 20 (16.3%) were >3 mm or multifocal. Of the 246 lobes available for the purposes of evaluating whether EPE was present or not, a further 15 lobes were excluded because of intra-prostatic PSM (Figure 1), meaning that 121 men and 231 lobes were included in the final analysis. Representative mpMRI and matched patient RP pathology images can be seen in Figure 2.
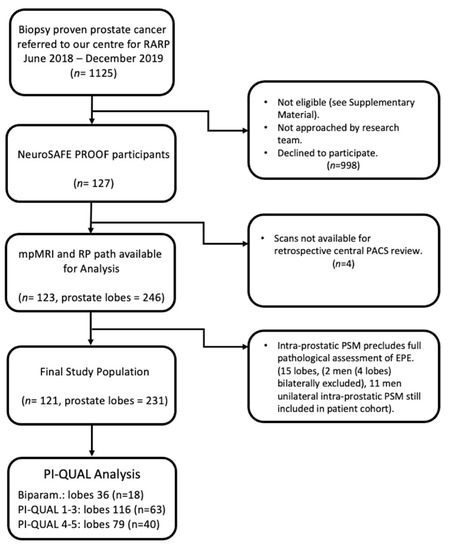
Figure 1.
Flow diagram of patient selection for study. Abbreviations: RARP, robot-assisted radical prostatectomy; PACS, picture archiving and communication system; RP, radical prostatectomy; PSM, positive surgical margin; EPE, extra-prostatic extension, PI-QUAL, Prostate Imaging Quality score; Biparam., bi-parametric MRI scan.
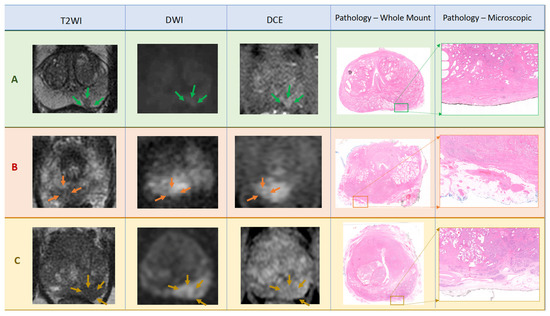
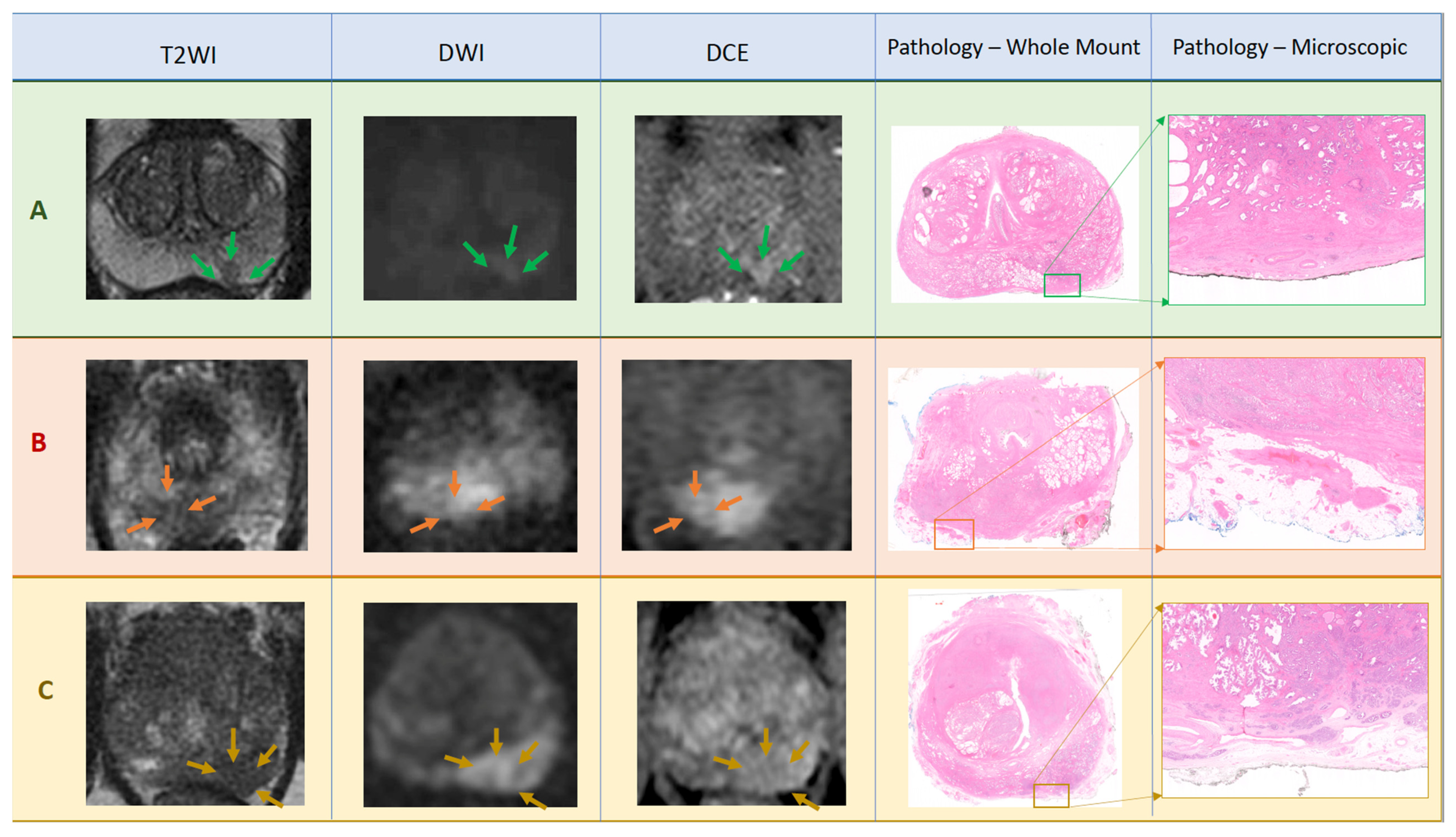
Figure 2.
Panel of example mpMRI scan images with corresponding histological RP whole mount images including areas of interest for EPE displayed in further magnification. Patient A: Images from mid-gland show Likert score 2 Left-lesion in left peripheral zone posterior medial (green arrows). Corresponding pathology panels show pT2c including disease confined to the gland, and not extending to the inked margin, in the left posterior medial peripheral zone (×1.5). Patient B: Images from apex of gland show Likert score 4 Right-lesion in right peripheral zone posterior medial showing irregularity and bulge (orange arrows). Corresponding pathology panels show pT3a including disease extending into the fat for 2 mm but clear of the inked margin (×1.42). Patient C: Images from base of gland show Likert score 5 Left-lesion in left peripheral zone posterior medial and posterior lateral demonstrating abutment, irregularity, bulge, and ‘measurable EPE’ (gold arrows). Corresponding pathology panels show pT3a including disease extending circumferentially beyond capsule and into the fat for 8 mm but clear of the inked margin (×1.5). All DWI images have b value of either b1400 or b2000.
Clinical, radiological, and final pathological characteristics of the patient cohort are shown in Table 1. Mean age was 56.9 years, mean PSA level was 8.9 ng/mL, and mean prostate volume on mpMRI was 36.6 cc ± 15. On final pathology, 82 of 121 (67.8%) men had organ-confined disease (pT2a-pT2c). EPE was seen in 39 of 121 men (32.2%), including in all seven men who had pT3b disease, and 43 of 231 lobes (18.6%). In 35 of 39 men (89.7%), EPE was unilateral. Preoperative PSA, clinical (i.e., biopsy) ISUP score, EAU risk category, DRE, RP specimen tumour volume, and RP ISUP score differed significantly between the groups with EPE and without EPE (all p < 0.05).

Table 1.
Patient, radiological, and pathological characteristics of study cohort.
A total of 112 of the scans used for EPE assessment were original pre-biopsy mpMRI, whilst nine men had mpMRI repeated after their prostate biopsy (Supplementary Table S2). Of these nine men, the mean number of days from biopsy to repeat scan was 163 (range; 63–475). All nine men had their repeat mpMRI scan performed at the academic centre and had a mean of 13 days (range; 2–25) from the repeat scan until RARP.
3.1. mpMRI Prediction of EPE
The diagnostic accuracy of mpMRI for EPE is presented in Table 2. The detection rates of pathological EPE according to each Likert score are presented in Figure 3 and tabulated in Supplementary Table S3. For Likert ≥ 3 on final read (i.e., once all imaging sequences, PSA, and biopsy information was available), there was an SE of 90.4% (CI: 83.8–94.9), SP of 52.3% (48–56.5), PPV of 29.9% (25.3–34.8), and NPV of 96% (93.2–97.9). When analysis was instead performed on a per patient level, for Likert ≥ 3 on final read there was an SE of 97.4%, SP of 24.4%, PPV of 38% and NPV of 95.2% (see Supplementary Table S4). Inter-observer agreement was determined using a weighted Kappa coefficient and is provided in Supplementary Table S5, showing substantial agreement between all readers on the final Likert score for the detection of EPE.
Table 2.
Per prostate lobe analysis of sensitivity (SE), specificity (SP), positive predictive value (PPV), negative predictive value (NPV), and area under the curve (AUC) by individual radiologist and combined where Likert score 3≥ was positive scan for pathological EPE.
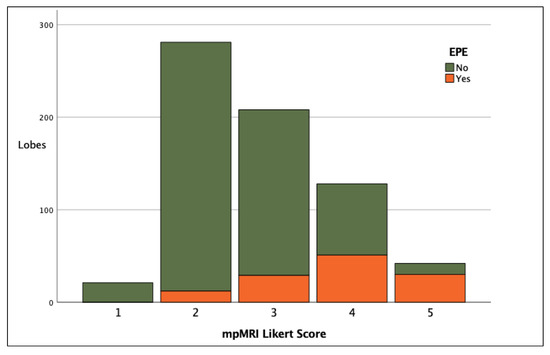
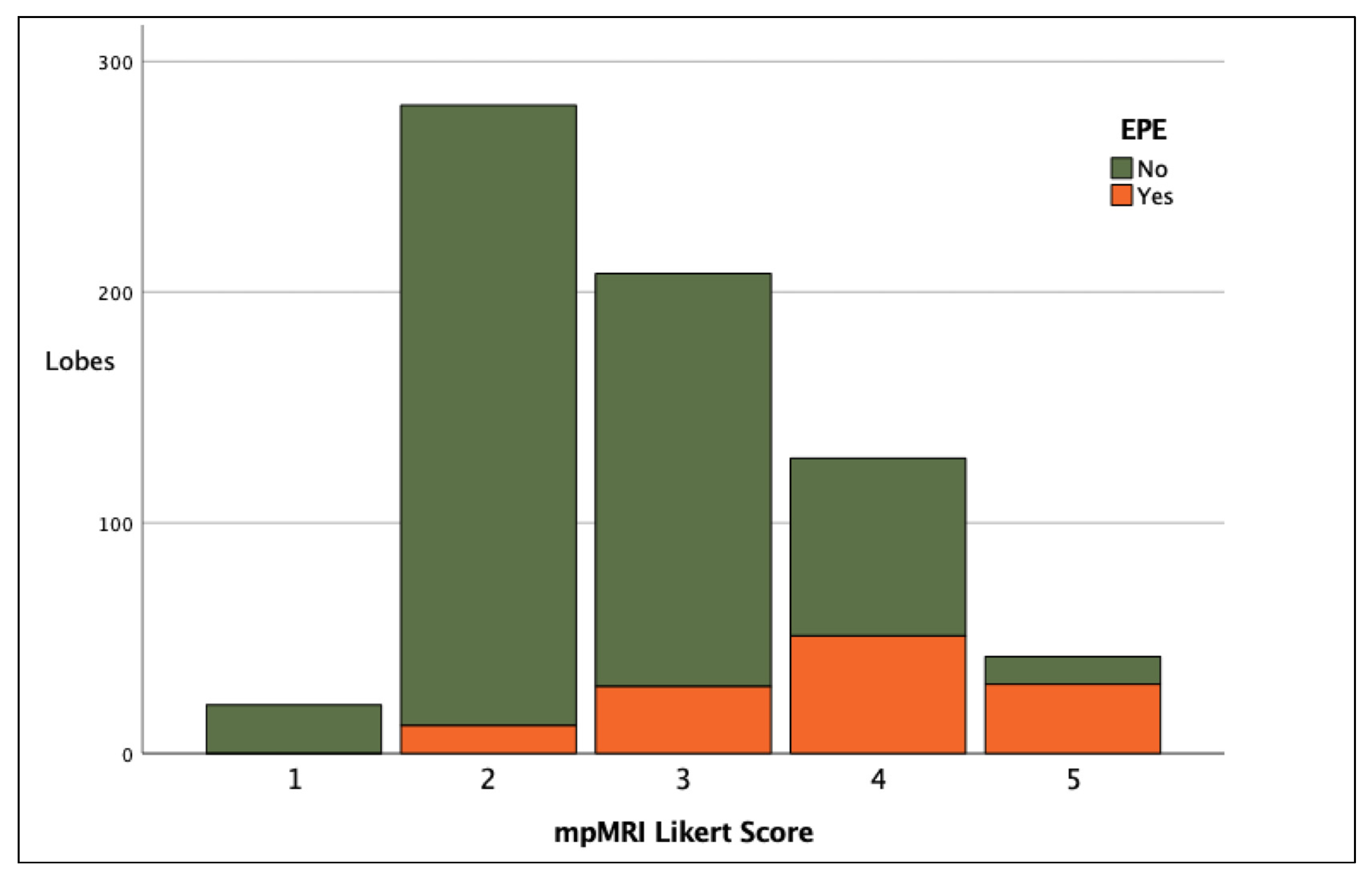
Figure 3.
Stacked bar chart showing clinical detection of EPE per lobe according to final Likert score.
3.2. Scan Quality and Diagnostic Performance
Eighteen scans were biparametric and therefore could not be assigned a PI-QUAL score (Figure 1). A total of 103 scans were scored according to PI-QUAL; 63 and 40 scans were classified with scores of 1–3 and 4–5, respectively. Diagnostic accuracy is presented in Table 3 and Supplementary Figure S4, showing that biparametric scans performed the least well, followed by PI-QUAL 1–3 scans and PI-QUAL 4–5 scans, which were best interpreted. AUCs were 0.76 (95% CI: 0.64–0.88), 0.78 (0.72–0.84), and 0.92 (0.88–0.96) for biparametric scans, PI-QUAL 1–3, and PI-QUAL 4–5 scans, respectively. PI-QUAL 4–5 scans had an SE of 100% (90.3–100) and an SP of 57% (49.7–64.1).
Table 3.
Diagnostic performance of MRI for prediction of EPE final Likert score ≥ 3 for biparametric MRI scans and mpMRI PI-QUAL scores of 1–3 and 4–5.
3.3. Accuracy of EPE with Additional Sequences and Clinical Information
Diagnostic accuracy improved with the addition of each imaging sequence and then further with the provision of PSA and biopsy information. The AUCs for T2WI alone, +DWI, +DCE, +PSA, and final (i.e., +biopsy information), were 0.62 (95% CI: 0.56–0.69), 0.69 (0.64–0.75), 0.76 (0.71–0.82), 0.79 (0.74–0.84), and 0.82 (0.77–0.86), respectively (see Supplementary Figure S5 for ROC curve).
4. Discussion
The accurate and precise prediction of EPE will result in better surgical outcomes by guiding surgeons to achieve the often-competing surgical goals of minimising PSM (by avoiding EPE) whilst maximising safe NS. Our data on EPE prediction by genitourinary radiologists using a Likert scale to attribute EPE status demonstrate the excellent ability of mpMRI to rule out EPE (SE of 90.4%, NPV of 96%).
Our study is the first to demonstrate improved EPE prediction with a higher objectively scored mpMRI scan quality (PI-QUAL). This finding strongly supports the concept that a high SE is dependent on good quality mpMRI scans and, we believe, may explain the poor or heterogeneous correlation of mpMRI and EPE status in previous studies.
The high SE for the prediction of EPE reported in this manuscript (90.4%) appears to come at the cost of a relatively lower SP (52.3%). Arguably, with the primary aim of optimising oncological outcomes by reducing PSM, the interpretation of mpMRI findings should be shifted towards obtaining a high SE in order to accurately rule out EPE, and thus, when a decision for NS is made, this is likely to be appropriate. On the other hand, with a low SP and PPV, if NS is not performed based solely on the mpMRI Likert score (3–5), in this study many men would not receive NS in whom it may have safely been performed, thus potentially negatively and unnecessarily affecting functional outcomes.
These results, a high SE and a lower SP, are at odds with the findings of the systematic review and meta-analysis of MRI for local PCa staging performed by de Rooij et al. in 2016. This review included 75 studies and demonstrated a high SP (91%) with a poor and heterogeneous SE (51%) [10]. Since this review, huge interest has continued in this topic as highlighted by the review by Abrams-Pompe et al., who included a further 48 studies that had been published with a significant ongoing variation in diagnostic accuracy reported [11]. For instance, Davis et al. reported an SE of 13% in their 2016 study of 133 men using scans performed at community radiology centres [18], whereas Alessi et al. reported an SE of 99% in 2019 in a study of 301 men where scans were performed at a single academic centre and reported according to the European Society of Urogenital Radiology (ESUR) PI-RADS EPE score version 2 [19]. In the UK, 98% of hospital trusts now perform pre-biopsy mpMRI for men with suspicion of PCa diagnosis [20]. In 2004, prior to the widespread dissemination and prominence of mpMRI in the diagnostic pathway in the UK, Allen et al. reported on 56 patients and found an SE of 50–72% and an SP of 84–86% for MRI EPE prediction [21].
Possible explanations for this broad variation in the accurate prediction of EPE published in the literature include differences in study design, measurement metrics, definitions of EPE, and clinical practice. In terms of different clinical practices, scans are performed in different settings and on different patient populations with different EPE prevalence. Additionally, scans may be performed before and after biopsy, using different scanners (magnets and manufacturers) and read by radiologists of differing experience. In terms of study design, there are different (and non-standardised) methods for reporting EPE where clinical information may or may not be provided to readers and where analysis can be undertaken in a variety of ways. For example, in our study performing analysis ‘per prostate lobe’ (Table 2) or ‘per patient’ (Supplementary Material Table S4) slightly increased SE, but considerably reduced SP and AUC overall (0.82 to 0.61). Such findings are consistent with the pooled sensitivity analysis performed by de Rooij et al., who demonstrated that the prediction of EPE was more accurate on a ‘region only’ compared to a ‘patient only’ level [10]. Moreover, different patient populations can have a marked effect on diagnostic accuracy. For instance, Falagario et al. demonstrated an AUC for EPE prediction using mpMRI of 0.73 for patients with high-risk PCa compared to 0.52 for patients with low- or very low-risk disease [22]. In the present study, 71.9% of patients had EAU high-risk PCa, which may help to also explain the strong diagnostic accuracy results (AUC of 0.82). The study by Falagario and colleagues may also demonstrate the importance of the definition of EPE on the diagnostic performance of mpMRI. Considering two different definitions of EPE, any EPE (i.e., focal and established) and established EPE only, the SE and AUC in men with unfavourable intermediate-risk PCa differed from 54.2 and 0.659 to 47.1 and 0.582, respectively [22]. An important and novel finding of this study is that MRI scan quality influences the ability of MRI to predict EPE, and therefore this may, for the first time, also help to further explain differing diagnostic accuracy results achieved in the literature until now. This study clearly shows that better mpMRI scans greatly improve the ability to accurately predict EPE.
Thirteen different scanners were used across our referral network. All scans had at least two functional sequences available for review, and 103/121 scans had DCE sequences. Our results show that the AUC improves with each additional imaging sequence reviewed, including DCE sequences. This finding is supported by the sub-analysis performed by de Rooij et al. within their systematic review, who noted that the SE for EPE improved from 53%, to 62%, to 69% for T2WI, to T2WI + one functional technique, to T2WI + two functional techniques, respectively, with no decrease in SP [10]. Additionally, similar to our results, the incorporation of clinical information is known to improve diagnostic accuracy compared to studies where mpMRI images alone are used [11]. Moreover, only once clinical information and all MRI sequences were available was inter-observer agreement using the Likert score substantial (i.e., weighted Kappa > 0.6) between all radiologists (see Supplementary Table S5).
With regards to the additional value of DCE sequences in our study, the administration of gadolinium contrast in high quality scans appears to improve diagnostic accuracy considerably, but not when the scan is of a lesser technical quality (PI-QUAL 1–3) (see Table 3 and Figure S4A–C). Caglic et al. showed that mpMRI was no better than biparametric MRI at detecting EPE, but mpMRI was better for detecting seminal vesicle invasion; however, they did not study the impact of an objective quality assessment of the scan [23]. Interestingly, in our study, in scans where DCE sequences were performed, in the locked sequential analysis, the AUC after review of DCE images was 0.76 compared to 0.69 before for T2WI and DWI images only (see Figure S5). Results such as these, which suggest the value of DCE images for the accurate staging of PCa, raise the question of whether men proceeding to RP will require an additional scan including gadolinium contrast in order to best inform the conduct of their surgery if such an mpMRI scan has not been performed in the first instance. Although artefactual changes seen on MRI after biopsy can compromise interpretation, in our study men who had a repeat scan following biopsy had excellent levels of diagnostic accuracy (AUC of 0.93, Supplementary Material Table S2). Notably, all these scans were a minimum of 63 days since biopsy, all had DCE sequences, and all scans were PI-QUAL score 3 or above.
mpMRI for EPE prediction is improved when radiologists use scores that convey the relative likelihood of EPE, rather than relying on binary terms such as ‘present’ or ‘absent’ [10]. The value of a risk-stratified ordinal scale to predict the likelihood of EPE is supported by the findings of this study where detection rates of EPE increased with each increment in the score assigned: 0%, 4.3%, 13.9%, 41.4%, and 73.8% for scores 1, 2, 3, 4, and 5, respectively (p < 0.0001) (Figure 3 and Supplementary Table S3). Risk-based grading systems have been described in the successful prediction of other features of PCa aggressiveness, such as biopsy ISUP score [24]. Indeed, there are several other methods of providing risk-stratified prediction scales for EPE based on mpMRI reported in the literature. These include (but are not limited to) EPE grade [25], ESUR [26], curvilinear contact length (CCL) [27], and tumour capsule length (TCL) [28]. The EPE Grade system has been externally validated with promisingly similar results [29]. Importantly, Park et al. have shown that different methods can perform similarly [30], and there is good evidence to consistently suggest that the incorporation of clinical details alongside mpMRI interpretation (such as in our study) may also improve diagnostic accuracy. In our study, we also collected information on the visual features observed in each scan, including tumour capsule abutment, prostate irregularity, NVB thickening, capsule bulge, and ‘measurable EPE’ in accordance with the 2012 ESUR guidance [26]. The frequency of these visual features according to positive scan (Likert ≥ 3) and positive pathology (EPE) can be viewed in the Supplementary Tables S6 and S7.
Interest in mpMRI has led to its inclusion into multivariable EPE prediction models. A model by Gandaglia et al. has been presented and externally validated [31], but their nomogram does not provide EPE likelihood on a side-specific basis [32], whereas NS decisions are made on a side-by-side basis. The SE for pathological EPE according to mpMRI prediction alone in 333 patients analysed in their series was 25% and provided a limited improvement in the accuracy of their model: an AUC of 0.67 without mpMRI data vs. 0.7 with. Other nomograms, such as those presented by Soeterik et al. and Nyarangi-Dix et al. that include mpMRI EPE information in a side-specific fashion (as in our study), perform better, with AUCs of 0.82 and 0.86, respectively [33,34]. Radiomic platforms using MRI prostate features combined with machine learning and clinical information have already shown a comparable diagnostic performance to radiologists and perform better than clinical nomograms, with AUCs of 0.74, 0.75, and 0.67 for radiomic evaluation, radiologist interpretation, and MSKCC nomogram, respectively [35].
If the threshold used to classify EPE prediction is modified to allow a higher SP with the Likert threshold moved to 4 instead of 3, the SE, SP, PPV, and NPV would change to 67.2%, 84.5%, 49.4%, and 92%, respectively (Supplementary Material Table S8). This would potentially facilitate more aggressive NS decision-making, but at the same time more men may incur PSM as a result. Another option when there is concern but uncertainty for EPE is intra-operative margin assessment, such as the NeuroSAFE technique or others [36,37]. However, when teams have evaluated their own performance and EPE is highly likely (for instance, 73.8% in Likert 5 in this series), aggressive ipsilateral NS may not be warranted.
This work has some limitations. Firstly, our centre benefits from radiologists with high levels of mpMRI expertise. A consideration of paramount importance for any team using mpMRI for EPE prediction to help guide the NS decision is that they must evaluate and understand their own diagnostic performance. Conversely, the MRIs in this study were carried out at a number of community hospitals, which improves the external generalisability of these results. Secondly, though blinded to the final histology, our radiologists reviewed scans retrospectively. Prospective validation studies with a larger pool of contributing radiologists are planned. Thirdly, our cohort is limited to patients undergoing RP and to those included in the NeuroSAFE PROOF study. Thus, the cohort is biased towards younger patients who had good erectile function at baseline. As such, these findings may not readily transfer to patient cohorts such as undiagnosed men or men undergoing other treatments, though the availability of a reference test for pathological EPE is not possible in these men. Fourthly, by excluding from our analysis lobes wherein an intra-prostatic PSM was noted without EPE elsewhere on the ipsilateral side, we may have introduced some bias in our study population, though the absence of a valid reference standard in these lobes prevented their inclusion. Fifthly, this is a retrospective study with a relatively small number of patients and as a consequence of the small numbers, we report broad confidence intervals in relation to the diagnostic performance parameters. In the future, the authors intend to incorporate more participants, centres, and radiologists using previously unseen mpMRI scans to prospectively validate whether the same results can be achieved in external settings but using the same interpretation methods. Moreover, small numbers of participants may contribute to some results which lie outside expected references, for instance the high proportion of men with biopsy ISUP 3 and 4 disease had EPE.
5. Conclusions
Likert score can be used very effectively by expert genitourinary radiologists to rule out EPE on a side-specific basis in men undergoing RARP. The diagnostic accuracy of mpMRI for predicting pathological EPE improves with the availability of additional MRI sequences, sight of clinical information, and better quality mpMRI scans.
Supplementary Materials
The following supporting information can be downloaded at: https://www.mdpi.com/article/10.3390/diagnostics12051057/s1, Table S1. Summary for Assessment of the diagnostic quality of mpMRI scans using the PI-QUAL score. Table S2. Clinical and Radiological features of the 9 men who had mpMRI repeated following prostate biopsy. Table S3. Pathological EPE according to final Likert score by individual radiologist per prostate lobe. Table S4. Per patient analysis of Sensitivity (SE), specificity (SP), positive predictive value (PPV), negative predictive value (NPV) and area under the curve (AUC) by individual radiologist and combined where Likert score 3≥ was positive scan for pathological. Table S5. Inter-reader agreement (κw) for Likert based mpMRI assessment of EPE. Table S6. Visual features according to radiological interpretation of positive scan for EPE (Likert ≥ 3). Table S7. Visual features according to EPE on final pathological assessment of RP specimen. Table S8. Diagnostic Performance of mpMRI when Likert score ≥4 for final read indicates positive diagnostic test. Figure S1. Locations of MRI Scanners and corresponding numbers of mpMRI Scans Performed. Figure S2. Study Case Reporting Form. Figure S3. Scoring sheet for assessing the quality of mpRMI using the PI-QUAL scoring system. T2-WI = T2-weighted imaging; DWI = diffusion-weighted imaging; DCE = dynamic contrast-enhanced; ADC = apparent diffusion coefficient. Figure S4. Stacked bar charts showing proportion clinical detection of EPE per lobe according to Final Likert score for biparametric scans (A), PI-QUAL score 1–3 scans (B), and PI-QUAL score 4–5 scans (C), respectively. Figure S5. ROC curves for prediction of pathologic EPE using mpMRI for all 3 readers with additional imaging and information in sequence.
Author Contributions
Conceptualization, E.D., C.A., V.K., F.G., G.S. and S.P.; Data curation, E.D., J.B., J.L., J.-P.M. and F.G.; Formal analysis, E.D., A.H., A.A. and T.P.; Funding acquisition, E.D. and G.S.; Investigation, C.A., T.S. and D.H.-H.; Project administration, J.G.; Resources, E.D., T.B., S.N., A.F. and G.S.; Supervision, G.S. and S.P.; Visualization, E.D., C.P. and D.P.; Writing—original draft, E.D. and V.K.; Writing—review & editing, E.D., A.S., J.A., R.P., I.A., L.D. and N.O. All authors have read and agreed to the published version of the manuscript.
Funding
This research was funded by JP Moulton Charitable Trust.
Institutional Review Board Statement
NCT03317990. Regional ethics committee approval 17/LO/1978.
Informed Consent Statement
All participants provided written informed consent.
Data Availability Statement
All datasets generated for this study are included in the manuscript. E.D. had full access to all the data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis.
Acknowledgments
The NeuroSAFE PROOF RCT is funded by the JP Moulton Charitable Foundation, NIHR RfPB (PB-PG-1216-20013) and The Rosetrees Foundation. E.D. is funded by the JP Moulton Charitable Foundation. F.G. is funded by the UCL Graduate Research Scholarship and the Brahm scholarship in memory of Chris Adams. V.K. is an Academic Clinical Lecturer funded by the United Kingdom National Institute for Health Research (NIHR). The views expressed in this publication are those of the authors and not necessarily those of the NHS, the NIHR, or the Department for Health. The NeuroSAFE PROOF team would like to thank the participants, principal investigators, research nurses, clinicians involved in providing care, regional cancer service co-ordinators, data managers, other site staff, and committee members of both the Data Monitoring Committee and the Trial Steering Group.
Conflicts of Interest
The authors have no personal conflicts of interest to disclose. Within NeuroSAFE PROOF, laparoscopic ports are supplied by Applied Medical. Applied Medical had no role in the design, analysis, or collection of the data; in the writing of the manuscript; or in the decision to submit the manuscript for publication.
References
- Kasivisvanathan, V.; Rannikko, A.S.; Borghi, M.; Panebianco, V.; Mynderse, L.A.; Vaarala, M.H.; Briganti, A.; Budäus, L.; Hellawell, G.; Hindley, R.G.; et al. MRI-Targeted or Standard Biopsy for Prostate-Cancer Diagnosis. N. Engl. J. Med. 2018, 378, 1767–1777. [Google Scholar] [CrossRef] [PubMed]
- Walz, J.; Burnett, A.L.; Costello, A.J.; Eastham, J.A.; Graefen, M.; Guillonneau, B.; Menon, M.; Montorsi, F.; Myers, R.P.; Rocco, B.; et al. A Critical Analysis of the Current Knowledge of Surgical Anatomy Related to Optimization of Cancer Control and Preservation of Continence and Erection in Candidates for Radical Prostatectomy. Eur. Urol. 2010, 57, 179–192. [Google Scholar] [CrossRef] [PubMed]
- Schiavina, R.; Bianchi, L.; Borghesi, M.; Dababneh, H.; Chessa, F.; Pultrone, C.V.; Angiolini, A.; Gaudiano, C.; Porreca, A.; Fiorentino, M.; et al. MRI Displays the Prostatic Cancer Anatomy and Improves the Bundles Management Before Robot-Assisted Radical Prostatectomy. J. Endourol. 2018, 32, 315–321. [Google Scholar] [CrossRef]
- Marenco, J.; Orczyk, C.; Collins, T.; Moore, C.; Emberton, M. Role of MRI in planning radical prostatectomy: What is the added value? World J. Urol. 2019, 37, 1289–1292. [Google Scholar] [CrossRef] [PubMed]
- Cathcart, P.; Sridhara, A.; Ramachandran, N.; Briggs, T.; Nathan, S.; Kelly, J. Achieving Quality Assurance of Prostate Cancer Surgery During Reorganisation of Cancer Services. Eur. Urol. 2015, 68, 22–29. [Google Scholar] [CrossRef] [PubMed]
- Mottet, N.; van den Bergh, R.C.N.; Briers, E.; Van den Broeck, T.; Cumberbatch, M.G.; De Santis, M.; Cornford, P. EAU-EANM-ESTRO-ESUR-SIOG Guidelines on Prostate Cancer-2020 Update. Part 1: Screening, Diagnosis, and Local Treatment with Curative Intent. Eur. Urol. 2020, 79, 243–262. [Google Scholar] [CrossRef]
- Ball, M.W.; Partin, A.W.; Epstein, J.I. Extent of Extraprostatic Extension Independently Influences Biochemical Recurrence-free Survival: Evidence for Further pT3 Subclassification. Urology 2015, 85, 161–164. [Google Scholar] [CrossRef]
- Danneman, D.; Wiklund, F.; Wiklund, N.P.; Egevad, L. Prognostic significance of histopathological features of extraprostatic extension of prostate cancer. Histopathology 2013, 63, 580–589. [Google Scholar] [CrossRef]
- Rapisarda, S.; Bada, M.; Crocetto, F.; Barone, B.; Arcaniolo, D.; Polara, A.; Imbimbo, C.; Grosso, G. The role of multiparametric resonance and biopsy in prostate cancer detection: Comparison with definitive histological report after laparoscopic/robotic radical prostatectomy. Abdom. Radiol. 2020, 45, 4178–4184. [Google Scholar] [CrossRef]
- De Rooij, M.; Hamoen, E.H.; Witjes, J.A.; Barentsz, J.O.; Rovers, M.M. Faculty Opinions recommendation of Accuracy of Magnetic Resonance Imaging for Local Staging of Prostate Cancer: A Diagnostic Meta-analysis. Eur. Urol. 2015, 70, 2189. [Google Scholar] [CrossRef]
- Abrams-Pompe, R.S.; Fanti, S.; Schoots, I.G.; Moore, C.M.; Turkbey, B.; Vickers, A.J.; Walz, J.; Steuber, T.; Eastham, J.A. The Role of Magnetic Resonance Imaging and Positron Emission Tomography/Computed Tomography in the Primary Staging of Newly Diagnosed Prostate Cancer: A Systematic Review of the Literature. Eur. Urol. Oncol. 2020, 4, 370–395. [Google Scholar] [CrossRef] [PubMed]
- Giganti, F.; Allen, C.; Emberton, M.; Moore, C.M.; Kasivisvanathan, V. Prostate Imaging Quality (PI-QUAL): A New Quality Control Scoring System for Multiparametric Magnetic Resonance Imaging of the Prostate from the PRECISION trial. Eur. Urol. Oncol. 2020, 3, 615–619. [Google Scholar] [CrossRef] [PubMed]
- Giganti, F.; Dinneen, E.; Kasivisvanathan, V.; Haider, A.; Freeman, A.; Kirkham, A.; Punwani, S.; Emberton, M.; Shaw, G.; Moore, C.M.; et al. Inter-reader agreement of the PI-QUAL score for prostate MRI quality in the NeuroSAFE PROOF trial. Eur. Radiol. 2021, 32, 879–889. [Google Scholar] [CrossRef]
- De Rooij, M.; Barentsz, J.O. PI-QUAL v.1: The first step towards good-quality prostate MRI. Eur Radiol. 2022, 32, 876–878. [Google Scholar] [CrossRef] [PubMed]
- Samaratunga, H.; The ISUP Prostate Cancer Group; Montironi, R.; True, L.; Epstein, I.J.; Griffiths, D.F.; Humphrey, A.P.; van der Kwast, T.; Wheeler, T.M.; Srigley, J.R.; et al. International Society of Urological Pathology (ISUP) Consensus Conference on Handling and Staging of Radical Prostatectomy Specimens. Working group 1: Specimen handling. Mod. Pathol. 2010, 24, 6–15. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Magi-Galluzzi, C.; The ISUP Prostate Cancer Group; Evans, A.J.; Delahunt, B.; Epstein, I.J.; Griffiths, D.F.; van der Kwast, T.H.; Montironi, R.; Wheeler, T.M.; Srigley, J.R.; et al. International Society of Urological Pathology (ISUP) Consensus Conference on Handling and Staging of Radical Prostatectomy Specimens. Working group 3: Extraprostatic extension, lymphovascular invasion and locally advanced disease. Mod. Pathol. 2010, 24, 26–38. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Barentsz, J.O.; Choyke, P.L.; Cornud, F.; Haider, M.A.; Macura, K.J.; Margolis, D.; Shtern, F.; Padhani, A.; Tempany, C.M.; Thoeny, H.C.; et al. PI-RADS Prostate Imaging-Reporting and Data System: 2015, Version 2. Eur. Urol. 2016, 70, e137–e138. [Google Scholar] [CrossRef]
- Davis, R.; Salmasi, A.; Koprowski, C.; Kim, S.; Kwon, Y.S.; Faiena, I.; Patel, N.; Elsamra, S.E.; Kim, I.Y. Accuracy of Multiparametric Magnetic Resonance Imaging for Extracapsular Extension of Prostate Cancer in Community Practice. Clin. Genitourin. Cancer 2016, 14, e617–e622. [Google Scholar] [CrossRef]
- Alessi, S.; Pricolo, P.; Summers, P.; Femia, M.; Tagliabue, E.; Renne, G.; Petralia, G. Low PI-RADS assessment category excludes extraprostatic extension (>/=pT3a) of prostate cancer: A histology-validated study including 301 operated patients. Eur. Radiol. 2019, 29, 5478–5487. [Google Scholar] [CrossRef] [Green Version]
- Audit NPC. Annual Report 2019-Results from the NPCA Prospective Audit in Enhland and Wales; Royal College of Surgeons: London, UK, 2019. [Google Scholar]
- Allen, D.J.; Hindley, R.; Clovis, S.; O’Donnell, P.; Cahill, D.; Rottenberg, G.; Popert, R. Does body-coil magnetic-resonance imaging have a role in the preoperative staging of patients with clinically localized prostate cancer? BJU Int. 2004, 94, 534–538. [Google Scholar] [CrossRef]
- Falagario, U.; Jambor, I.; Ratnani, P.; Martini, A.; Treacy, P.; Lantz, A.; Wajswol, E.; Papastefanou, G.; Giuseppe, C.; Wiklund, P.; et al. Performance of prostate multiparametric MRI for prediction of prostate cancer extra-prostatic extension according to NCCN risk categories: Implication for surgical planning. Eur. Urol. Open Sci. 2020, 19, e1743–e1744. [Google Scholar] [CrossRef]
- Caglic, I.; Sushentsev, N.; Shah, N.; Warren, A.Y.; Lamb, B.W.; Barrett, T. Comparison of biparametric versus multiparametric prostate MRI for the detection of extracapsular extension and seminal vesicle invasion in biopsy naive patients. Eur. J. Radiol. 2021, 141, 109804. [Google Scholar] [CrossRef] [PubMed]
- Boschheidgen, M.; Schimmöller, L.; Arsov, C.; Ziayee, F.; Morawitz, J.; Valentin, B.; Radke, K.L.; Giessing, M.; Esposito, I.; Albers, P.; et al. MRI grading for the prediction of prostate cancer aggressiveness. Eur. Radiol. 2021, 32, 2351–2359. [Google Scholar] [CrossRef] [PubMed]
- Mehralivand, S.; Shih, J.H.; Harmon, S.; Smith, C.; Bloom, J.; Czarniecki, M.; Gold, S.; Hale, G.; Rayn, K.; Merino, M.J.; et al. A Grading System for the Assessment of Risk of Extraprostatic Extension of Prostate Cancer at Multiparametric MRI. Radiology 2019, 290, 709–719. [Google Scholar] [CrossRef]
- Barentsz, J.O.; Richenberg, J.; Clements, R.; Choyke, P.; Verma, S.; Villeirs, G.; Rouviere, O.; Logager, V.; Fütterer, J.J. ESUR prostate MR guidelines 2012. Eur. Radiol. 2012, 22, 746–757. [Google Scholar] [CrossRef] [Green Version]
- Kongnyuy, M.; Sidana, A.; George, A.K.; Muthigi, A.; Iyer, A.; Ho, R.; Chelluri, R.; Mertan, F.; Frye, T.P.; Su, D.; et al. Tumor contact with prostate capsule on magnetic resonance imaging: A potential biomarker for staging and prognosis. Urol. Oncol. Semin. Orig. Investig. 2016, 35, 30.e1–30.e8. [Google Scholar] [CrossRef]
- Bakir, B.; Onay, A.; Vural, M.; Armutlu, A.; Yıldız, S.; Esen, T. Can Extraprostatic Extension Be Predicted by Tumor-Capsule Contact Length in Prostate Cancer? Relationship With International Society of Urological Pathology Grade Groups. Am. J. Roentgenol. 2020, 214, 588–596. [Google Scholar] [CrossRef]
- Reistaeter, L.A.R.H.O.; Beisland, C.; Honore, A.; Gravdal, K.; Losnegard, A.; Monssen, J.; Alslen, L.A.; Biermann, M. Assessing Extraprostatic Extension with Multiparametric MRI of the Prostate: Mehralivand Extraprostatic Extension Grade or Extraprostatic Extension Likert Scale? Radiol. Imaging Cancer 2020, 2, 1. [Google Scholar]
- Park, K.J.; Kim, M.-H.; Kim, J.K. Extraprostatic Tumor Extension: Comparison of Preoperative Multiparametric MRI Criteria and Histopathologic Correlation after Radical Prostatectomy. Radiology 2020, 296, 87–95. [Google Scholar] [CrossRef]
- Diamand, R.; Ploussard, G.; Roumiguié, M.; Oderda, M.; Benamran, D.; Fiard, G.; Quackels, T.; Assenmacher, G.; Simone, G.; Van Damme, J.; et al. External Validation of a Multiparametric Magnetic Resonance Imaging–based Nomogram for the Prediction of Extracapsular Extension and Seminal Vesicle Invasion in Prostate Cancer Patients Undergoing Radical Prostatectomy. Eur. Urol. 2020, 79, 180–185. [Google Scholar] [CrossRef]
- Gandaglia, G.; Ploussard, G.; Valerio, M.; Mattei, A.; Fiori, C.; Roumiguie, M.; Briganti, A. The Key Combined Value of Multiparametric Magnetic Resonance Imaging, and Magnetic Resonance Imaging-targeted and Concomitant Systematic Biopsies for the Prediction of Adverse Pathological Features in Prostate Cancer Patients Undergoing Radical Prostatectomy. Eur. Urol. 2020, 77, 733–741. [Google Scholar] [PubMed]
- Soeterik, T.F.; van Melick, H.H.; Dijksman, L.M.; Küsters-Vandevelde, H.; Stomps, S.; Schoots, I.G.; Biesma, D.H.; Witjes, J.; van Basten, J.-P.A. Development and External Validation of a Novel Nomogram to Predict Side-specific Extraprostatic Extension in Patients with Prostate Cancer Undergoing Radical Prostatectomy. Eur. Urol. Oncol. 2020. [Google Scholar] [CrossRef] [PubMed]
- Nyarangi-Dix, J.; Wiesenfarth, M.; Bonekamp, D.; Hitthaler, B.; Schütz, V.; Dieffenbacher, S.; Mueller-Wolf, M.; Roth, W.; Stenzinger, A.; Duensing, S.; et al. Combined Clinical Parameters and Multiparametric Magnetic Resonance Imaging for the Prediction of Extraprostatic Disease—A Risk Model for Patient-tailored Risk Stratification When Planning Radical Prostatectomy. Eur. Urol. Focus 2018, 6, 1205–1212. [Google Scholar] [CrossRef] [PubMed]
- Losnegård, A.; Reisæter, L.A.R.; Halvorsen, O.J.; Jurek, J.; Assmus, J.; Arnes, J.B.; Honoré, A.; Monssen, J.A.; Andersen, E.; Haldorsen, I.S.; et al. Magnetic resonance radiomics for prediction of extraprostatic extension in non-favorable intermediate- and high-risk prostate cancer patients. Acta Radiol. 2020, 61, 1570–1579. [Google Scholar] [CrossRef]
- Dinneen, E.; Haider, A.; Grierson, J.; Freeman, A.; Oxley, J.; Briggs, T.; Shaw, G. NeuroSAFE frozen section during robot-assisted radical prostatectomy (RARP): Peri-operative and Histopathological Outcomes from the NeuroSAFE PROOF Feasibility Randomised Controlled Trial. BJU Int. 2020, 127, 676–686. [Google Scholar] [CrossRef]
- Petralia, G.; Musi, G.; Padhani, A.R.; Summers, P.; Renne, G.; Alessi, S.; Raimondi, S.; Matei, D.V.; Renne, S.; Jereczek-Fossa, B.A.; et al. Robot-assisted Radical Prostatectomy: Multiparametric MR Imaging–directed Intraoperative Frozen-Section Analysis to Reduce the Rate of Positive Surgical Margins. Radiology 2015, 274, 434–444. [Google Scholar] [CrossRef] [Green Version]
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).