
(Low) Energy Availability and Its Association with Injury Occurrence in Competitive Dance: Cross-Sectional Analysis in Female Dancers



 , ,
, ,  , ,
, ,  and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants and Design of the Study
2.2. Variables and Measurement
2.3. Statistics
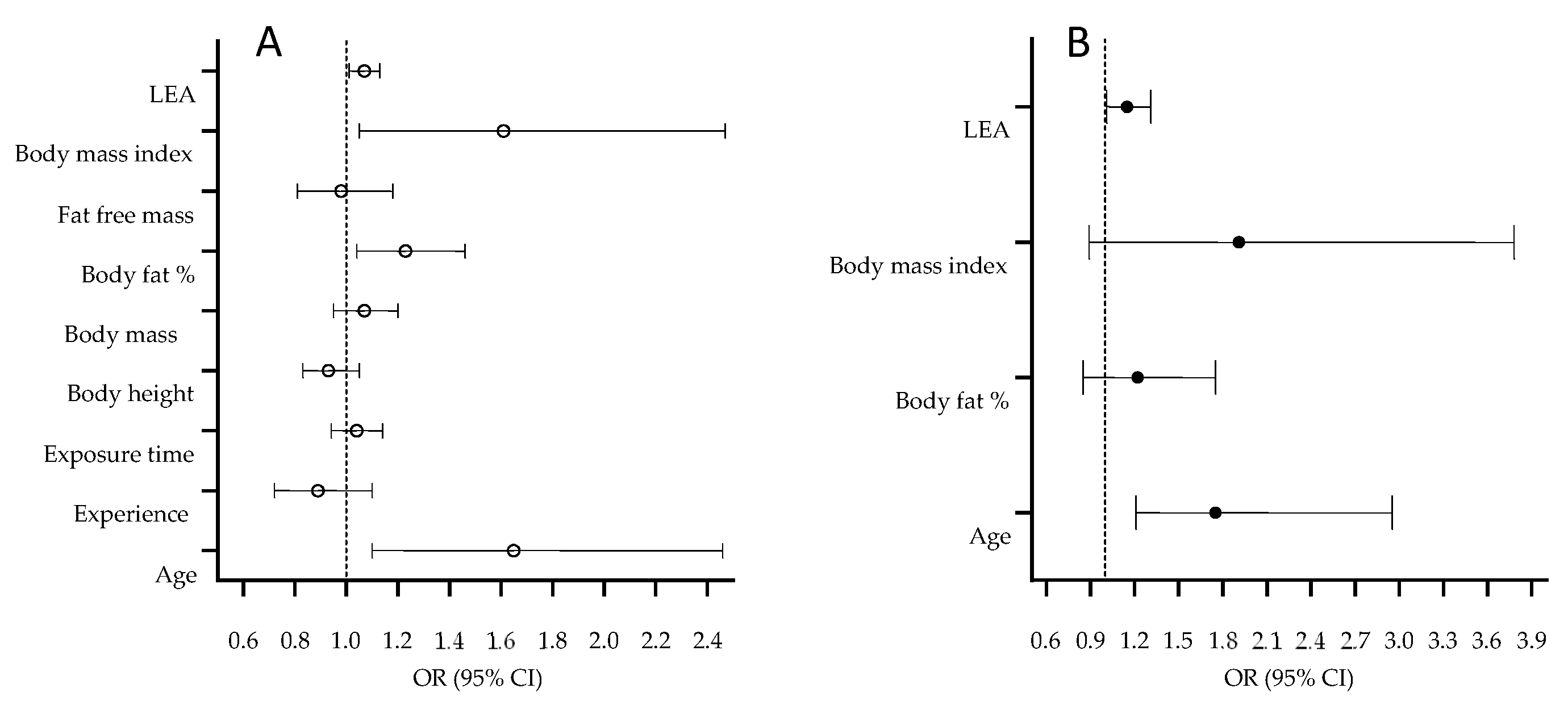
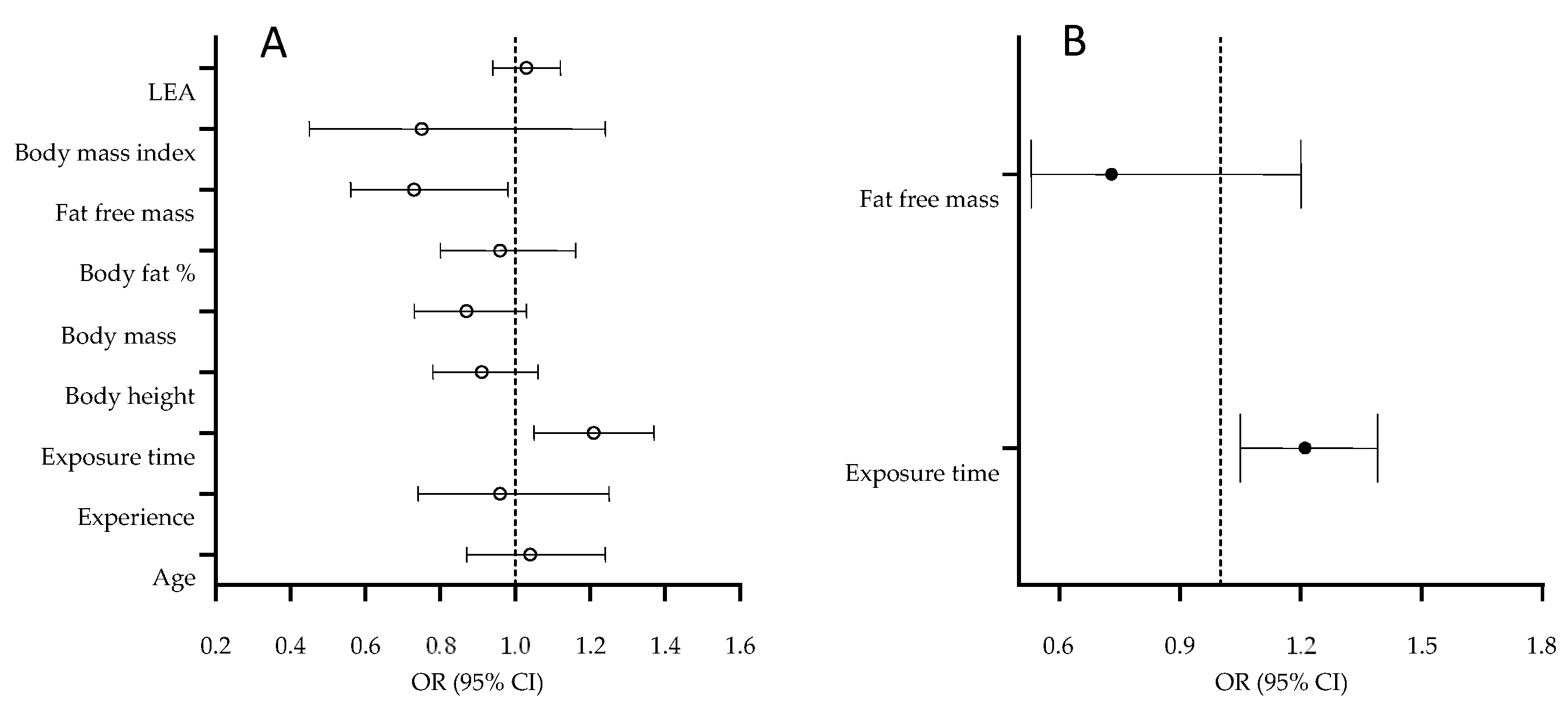
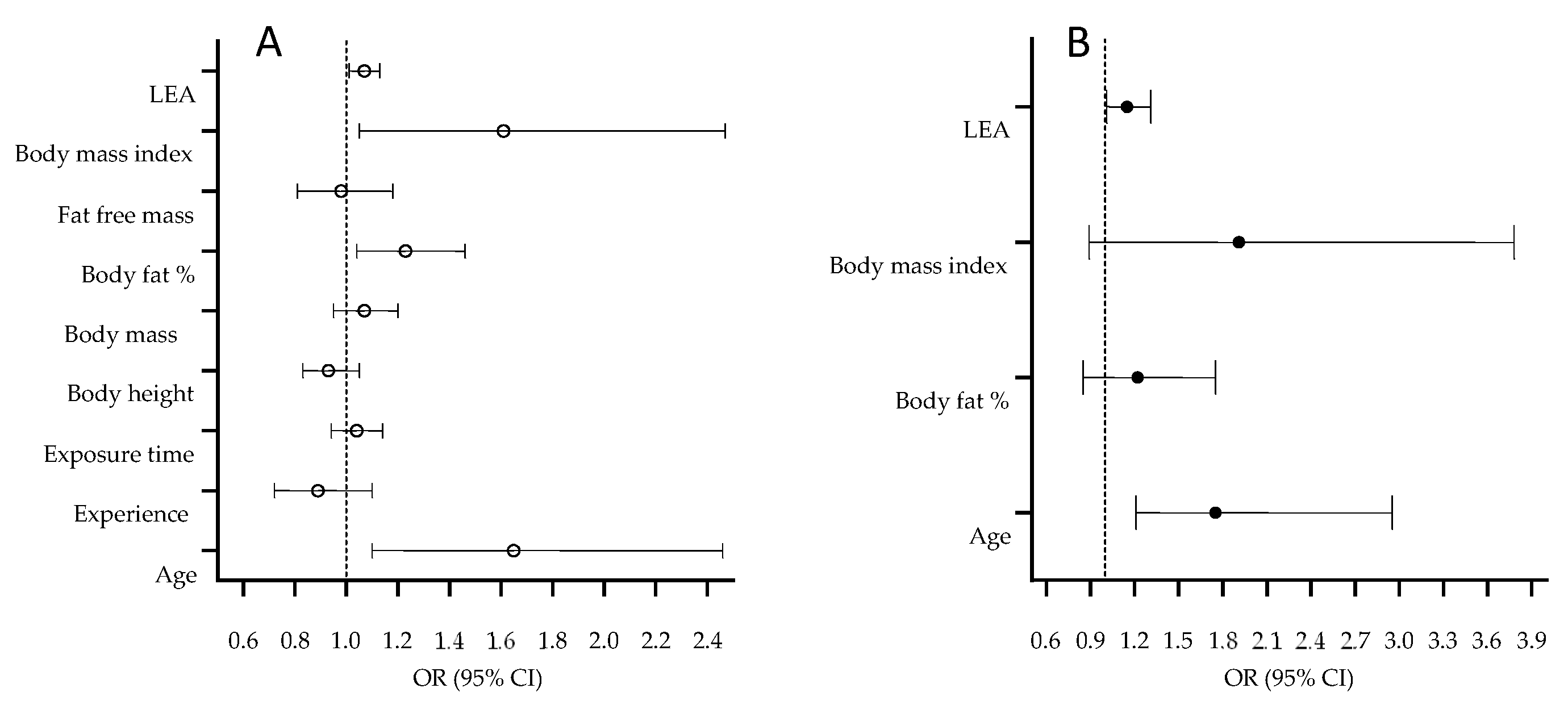
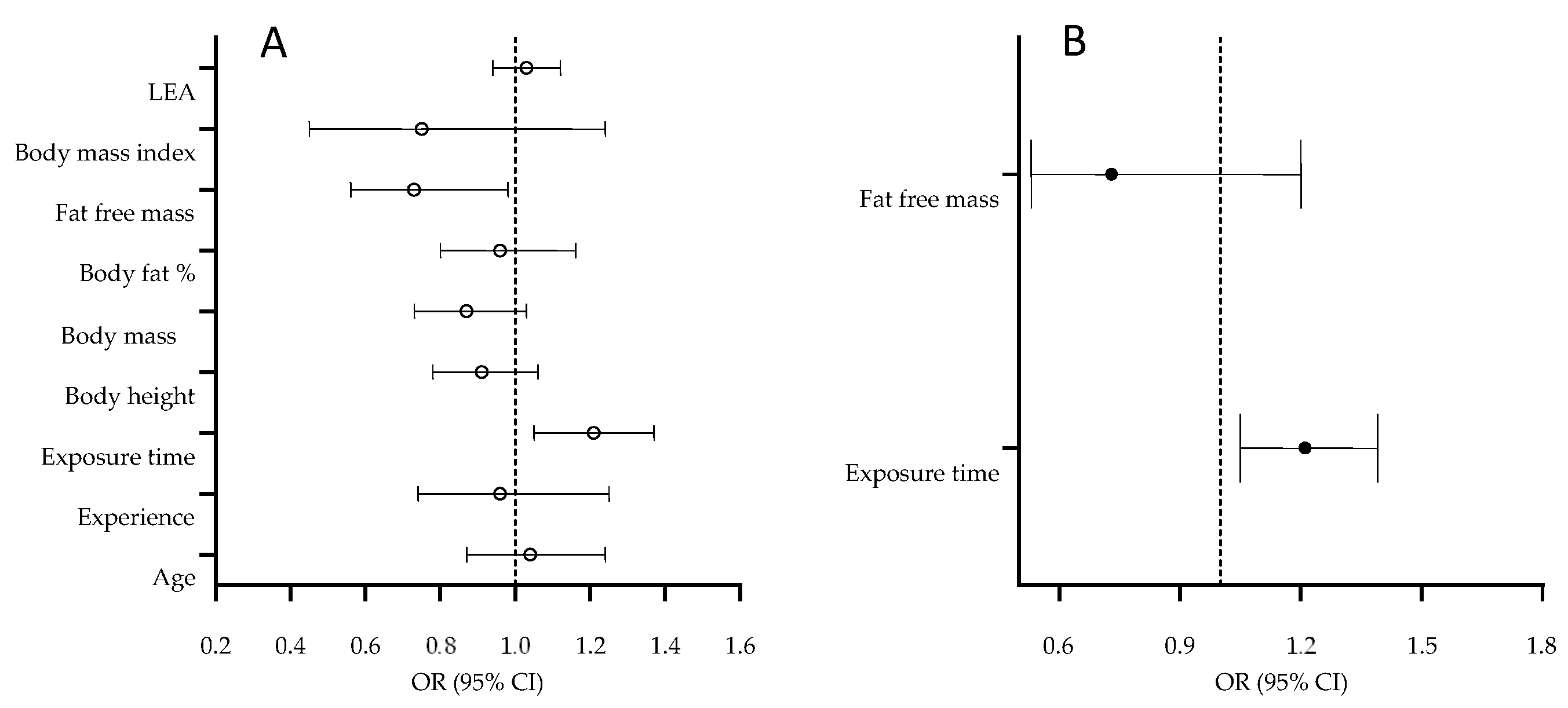
3. Results
4. Discussion
4.1. Dancers’ Age and Injury Occurrence
4.2. Training Volume and Bone Injuries
4.3. Anthropometric/Body Composition and Injury Occurrence
4.4. (Low) Energy Availability and Soft-Tissue Injuries
4.5. Multivariate Associations
4.6. Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Askling, C.; Lund, H.; Saartok, T.; Thorstensson, A. Self-reported hamstring injuries in student-dancers. Scand. J. Med. Sci. Sports 2002, 12, 230–235. [Google Scholar] [CrossRef] [PubMed]
- Hincapié, C.A.; Morton, E.J.; Cassidy, J.D. Musculoskeletal injuries and pain in dancers: A systematic review. Arch. Phys. Med. Rehabil. 2008, 89, 1819–1829.e1816. [Google Scholar] [CrossRef]
- Marusic, J.; Dolenc, P.; Sarabon, N. Psychological Aspect of Rehabilitation and Return to Sport Following Lower Limb Injuries. Montenegrin J. Sports Sci. Med. 2020, 9, 59. [Google Scholar] [CrossRef]
- Ramel, E.; Moritz, U. Self-reported musculoskeletal pain and discomfort in professional ballet dancers in Sweden. Scand. J. Rehabil. Med. 1994, 26, 11–16. [Google Scholar] [PubMed]
- Evans, R.W.; Evans, R.I.; Carvajal, S. Survey of injuries among West End performers. Occup. Environ. Med. 1998, 55, 585–593. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liederbach, M.; Compagno, J.M. Psychological aspects of fatigue-related injuries in dancers. J. Danc. Med. Sci. 2001, 5, 116–120. [Google Scholar]
- Hamilton, L.H.; Hamilton, W.G.; Meltzer, J.D.; Marshall, P.; Molnar, M. Personality, stress, and injuries in professional ballet dancers. Am. J. Sports Med. 1989, 17, 263–267. [Google Scholar] [CrossRef]
- To, W.K.; Wong, M.; Chan, K. The effect of dance training on menstrual function in collegiate dancing students. Aust. N. Zeal. J. Obstet. Gynaecol. 1995, 35, 304–309. [Google Scholar] [CrossRef]
- Chmelar, R.D.; Fitt, S.S.; Schultz, B.B.; Ruhling, R.O.; Zupan, M.F. A survey of health, training, and injuries in different levels and styles of dancers. Med. Probl. Perform. Art 1987, 2, 61–66. [Google Scholar]
- Hiller, C.E.; Refshauge, K.M.; Beard, D.J. Sensorimotor control is impaired in dancers with functional ankle instability. Am. J. Sports Med. 2004, 32, 216–223. [Google Scholar] [CrossRef]
- Soares Campoy, F.A.; Raquel de Oliveira Coelho, L.; Bastos, F.N.; Júnior, J.N.; Marques Vanderlei, L.C.; Luiz Monteiro, H.; Padovani, C.R.; Pastre, C.M. Investigation of Risk Factors and Characteristics of Dance Injuries. Clin. J. Sport Med. 2011, 21, 493–498. [Google Scholar] [CrossRef] [PubMed]
- Burke, L.M. Energy needs of athletes. Can. J. Appl. Physiol. 2001, 26, S202–S219. [Google Scholar] [CrossRef] [PubMed]
- Meng, K.; Qiu, J.; Benardot, D.; Carr, A.; Yi, L.; Wang, J.; Liang, Y. The risk of low energy availability in Chinese elite and recreational female aesthetic sports athletes. J. Int. Soc. Sports Nutr. 2020, 17, 13. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rodriguez, N.R.; Di Marco, N.M.; Langley, S. American College of Sports Medicine position stand. Nutrition and athletic performance. Med. Sci. Sports Exerc. 2009, 41, 709–731. [Google Scholar] [PubMed]
- Baranauskas, M.; Jablonskienė, V.; Abaravičius, J.A.; Stukas, R. Actual Nutrition and Dietary Supplementation in Lithuanian Elite Athletes. Medicina 2020, 56, 247. [Google Scholar] [CrossRef] [PubMed]
- Dobrowolski, H.; Karczemna, A.; Włodarek, D. Nutrition for Female Soccer Players—Recommendations. Medicina 2020, 56, 28. [Google Scholar] [CrossRef] [Green Version]
- Torres-McGehee, T.M.; Emerson, D.M.; Pritchett, K.; Moore, E.M.; Smith, A.B.; Uriegas, N.A. Energy availability with or without eating disorder risk in collegiate female athletes and performing artists. J. Athl. Train. 2021, 56, 993–1002. [Google Scholar] [CrossRef]
- Sekulic, D.; Prus, D.; Zevrnja, A.; Peric, M.; Zaletel, P. Predicting Injury Status in Adolescent Dancers Involved in Different Dance Styles: A Prospective Study. Children 2020, 7, 297. [Google Scholar] [CrossRef]
- Statuta, S.M.; Asif, I.M.; Drezner, J.A. Relative energy deficiency in sport (RED-S). Br. J. Sports Med. 2017, 51, 1570–1571. [Google Scholar] [CrossRef]
- Bone, J.L.; Burke, L.M. No difference in young adult athletes’ resting energy expenditure when measured under inpatient or outpatient conditions. Int. J. Sport Nutr. Exerc. Metab. 2018, 28, 464–467. [Google Scholar] [CrossRef]
- Varga, T.V.; Ali, A.; Herrera, J.A.; Ahonen, L.L.; Mattila, I.M.; Al-Sari, N.H.; Legido-Quigley, C.; Skouby, S.; Brunak, S.; Tornberg, Å.B. Lipidomic profiles, lipid trajectories and clinical biomarkers in female elite endurance athletes. Sci. Rep. 2020, 10, 2349. [Google Scholar] [CrossRef]
- Loucks, A.; Verdun, M.; Heath, E. Low energy availability, not stress of exercise, alters LH pulsatility in exercising women. J. Appl. Physiol. 1998, 84, 37–46. [Google Scholar] [CrossRef] [PubMed]
- Mountjoy, M.; Sundgot-Borgen, J.; Burke, L.; Ackerman, K.E.; Blauwet, C.; Constantini, N.; Lebrun, C.; Lundy, B.; Melin, A.; Meyer, N. International Olympic Committee (IOC) consensus statement on relative energy deficiency in sport (RED-S): 2018 update. Int. J. Sport Nutr. Exerc. Metab. 2018, 28, 316–331. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Otis, C.L.; Drinkwater, B.; Johnson, M.; Loucks, A.; Wilmore, J. American College of Sports Medicine position stand. The female athlete triad. Med. Sci. Sports Exerc. 1997, 29, i–ix. [Google Scholar] [CrossRef] [PubMed]
- Logue, D.; Madigan, S.M.; Delahunt, E.; Heinen, M.; Mc Donnell, S.-J.; Corish, C.A. Low energy availability in athletes: A review of prevalence, dietary patterns, physiological health, and sports performance. Sports Med. 2018, 48, 73–96. [Google Scholar] [CrossRef]
- Heikura, I.A.; Uusitalo, A.L.; Stellingwerff, T.; Bergland, D.; Mero, A.A.; Burke, L.M. Low energy availability is difficult to assess but outcomes have large impact on bone injury rates in elite distance athletes. Int. J. Sport Nutr. Exerc. Metab. 2018, 28, 403–411. [Google Scholar] [CrossRef] [Green Version]
- Ackerman, K.E.; Holtzman, B.; Cooper, K.M.; Flynn, E.F.; Bruinvels, G.; Tenforde, A.S.; Popp, K.L.; Simpkin, A.J.; Parziale, A.L. Low energy availability surrogates correlate with health and performance consequences of Relative Energy Deficiency in Sport. Br. J. Sports Med. 2019, 53, 628–633. [Google Scholar] [CrossRef]
- Sipers, W.M.; Dorge, J.; Schols, J.M.; Verdijk, L.B.; Van Loon, L.J. Multifrequency bioelectrical impedance analysis may represent a reproducible and practical tool to assess skeletal muscle mass in euvolemic acutely ill hospitalized geriatric patients. Eur. Geriatr. Med. 2020, 11, 155–162. [Google Scholar] [CrossRef] [Green Version]
- Longland, T.M.; Oikawa, S.Y.; Mitchell, C.J.; Devries, M.C.; Phillips, S.M. Higher compared with lower dietary protein during an energy deficit combined with intense exercise promotes greater lean mass gain and fat mass loss: A randomized trial. Am. J. Clin. Nutr. 2016, 103, 738–746. [Google Scholar] [CrossRef]
- Heil, D.P. Predicting Activity Energy Expenditure Using the Actical® Activity Monitor. Res. Q. Exerc. Sport 2006, 77, 64–80. [Google Scholar] [CrossRef]
- Mountjoy, M.; Sundgot-Borgen, J.K.; Burke, L.M.; Ackerman, K.E.; Blauwet, C.; Constantini, N.; Lebrun, C.; Lundy, B.; Melin, A.K.; Meyer, N.L.; et al. IOC consensus statement on relative energy deficiency in sport (RED-S): 2018 update. Br. J. Sports Med. 2018, 52, 687–697. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Civil, R.; Lamb, A.; Loosmore, D.; Ross, L.; Livingstone, K.; Strachan, F.; Dick, J.R.; Stevenson, E.J.; Brown, M.A.; Witard, O.C. Assessment of Dietary Intake, Energy Status, and Factors Associated With RED-S in Vocational Female Ballet Students. Front. Nutr. 2019, 5, 136. [Google Scholar] [CrossRef] [PubMed]
- Keay, N.; Overseas, A.; Francis, G. Indicators and correlates of low energy availability in male and female dancers. BMJ Open Sport Exerc. Med. 2020, 6, e000906. [Google Scholar] [CrossRef]
- Zaletel, P.; Sekulic, D.; Zenic, N.; Esco, M.R.; Sajber, D.; Kondric, M. The association between body-built and injury occurrence in pre-professional ballet dancers - Separated analysis for the injured body-locations. Int. J. Occup. Med. Environ. Health 2017, 30, 151–159. [Google Scholar] [CrossRef]
- Solomon, R.; Micheli, L.J.; Solomon, J.; Kelley, T. The “cost” of injuries in a professional ballet company: A three-year perspective. Med. Probl. Perform. Artist. 1996, 11, 67–74. [Google Scholar]
- Solomon, R.; Solomon, J.; Micheli, L.J.; McGray, E. The “cost” of injuries in a professional ballet company: A five-year study. Med. Probl. Perform. Artist. 1999, 14, 164–170. [Google Scholar]
- Östenberg, A.; Roos, H. Injury risk factors in female European football. A prospective study of 123 players during one season. Scand. J. Med. Sci. Sports 2000, 10, 279–285. [Google Scholar] [CrossRef] [PubMed]
- Mijatovic, D.; Krivokapic, D.; Versic, S.; Dimitric, G.; Zenic, N. Change of direction speed and reactive agility in prediction of injury in football; prospective analysis over one half-season. Healthcare 2022, 10, 440. [Google Scholar] [CrossRef]
- Nilsson, C.; Leanderson, J.; Wykman, A.; Strender, L.-E. The injury panorama in a Swedish professional ballet company. Knee Surg. Sports Traumatol. Arthrosc. 2001, 9, 242–246. [Google Scholar] [CrossRef]
- Novosel, B.; Sekulic, D.; Peric, M.; Kondric, M.; Zaletel, P. Injury occurrence and return to dance in professional ballet: Prospective analysis of specific correlates. Int. J. Environ. Res. Public Health 2019, 16, 765. [Google Scholar] [CrossRef] [Green Version]
- Ursej, E.; Sekulic, D.; Prus, D.; Gabrilo, G.; Zaletel, P. Investigating the Prevalence and Predictors of Injury Occurrence in Competitive Hip Hop Dancers: Prospective Analysis. Int. J. Environ. Res. Public Health 2019, 16, 3214. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Carey, K.; Moran, A.; Rooney, B. Learning Choreography: An Investigation of Motor Imagery, Attentional Effort, and Expertise in Modern Dance. Front. Psychol. 2019, 10, 422. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Steinberg, N.; Aujla, I.; Zeev, A.; Redding, E. Injuries among talented young dancers: Findings from the UK Centres for Advanced Training. Int. J. Sports Med. 2014, 35, 238–244. [Google Scholar] [CrossRef] [PubMed]
- Kadel, N.J.; Teitz, C.C.; Kronmal, R.A. Stress fractures in ballet dancers. Am. J. Sports Med. 1992, 20, 445–449. [Google Scholar] [CrossRef] [PubMed]
- Kiesel, K.; Plisky, P.J.; Voight, M.L. Can serious injury in professional football be predicted by a preseason functional movement screen? N. Am. J. Sports Phys. Ther. NAJSPT 2007, 2, 147. [Google Scholar]
- Steinberg, N.; Siev-Ner, I.; Peleg, S.; Dar, G.; Masharawi, Y.; Zeev, A.; Hershkovitz, I. Extrinsic and intrinsic risk factors associated with injuries in young dancers aged 8–16 years. J. Sports Sci. 2012, 30, 485–495. [Google Scholar] [CrossRef]
- Twitchett, E.; Angioi, M.; Metsios, G.S.; Koutedakis, Y.; Wyon, M. Body composition and ballet injuries: A preliminary study. Med. Probl. Perform. Artist. 2008, 23, 93–98. [Google Scholar] [CrossRef]
- Koutedakis, Y.; Khaloula, M.; Pacy, P.; Murphy, M.; Dunbar, G. Thigh peak torques and lower-body injuries in dancers. J. Danc. Med. Sci. 1997, 1, 12–15. [Google Scholar]
- Kim, H.-C.; Park, K.-J. Correlation analysis of sports injuries and body composition and bone density in national water pool players. J. Korean Soc. Phys. Med. 2019, 14, 134–141. [Google Scholar] [CrossRef]
- Wahner, H.W. Measurements of bone mass and bone density. Endocrinol. Metab. Clin. N. Am. 1989, 18, 995–1012. [Google Scholar] [CrossRef]
- Benson, J.E. Relationship between nutrient intake, body mass index, menstrual function, and ballet injury. J. Am. Diet. Assoc. 1989, 89, 58–63. [Google Scholar] [CrossRef]
- Twitchett, E.; Brodrick, A.; Nevill, A.M.; Koutedakis, Y.; Angioi, M.; Wyon, M. Does physical fitness affect injury occurrence and time loss due to injury in elite vocational ballet students? J. Danc. Med. Sci. 2010, 14, 26–31. [Google Scholar]
- Dane, Ş.; Can, S.; Karsan, O. Relations of body mass index, body fat, and power of various muscles to sport injuries. Percept. Mot. Ski. 2002, 95, 329–334. [Google Scholar] [CrossRef] [PubMed]
- Toomey, C.M.; Whittaker, J.L.; Nettel-Aguirre, A.; Reimer, R.A.; Woodhouse, L.J.; Ghali, B.; Doyle-Baker, P.K.; Emery, C.A. Higher fat mass is associated with a history of knee injury in youth sport. J. Orthop. Sports Phys. Ther. 2017, 47, 80–87. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Melin, A.; Tornberg, Å.B.; Skouby, S.; Faber, J.; Ritz, C.; Sjödin, A.; Sundgot-Borgen, J. The LEAF questionnaire: A screening tool for the identification of female athletes at risk for the female athlete triad. Br. J. Sports Med. 2014, 48, 540–545. [Google Scholar] [CrossRef] [PubMed]
- Keay, N.; Rankin, A. Infographic. Relative energy deficiency in sport: An infographic guide. Br. J. Sports Med. 2019, 53, 1307–1309. [Google Scholar] [CrossRef] [PubMed]
- Meczekalski, B.; Podfigurna-Stopa, A.; Genazzani, A.R. Hypoestrogenism in young women and its influence on bone mass density. Gynecol. Endocrinol. 2010, 26, 652–657. [Google Scholar] [CrossRef]
- Thein-Nissenbaum, J.M.; Rauh, M.J.; Carr, K.E.; Loud, K.J.; McGuine, T.A. Menstrual irregularity and musculoskeletal injury in female high school athletes. J. Athl. Train. 2012, 47, 74–82. [Google Scholar] [CrossRef]
- Donaldson, A.A.; Gordon, C.M. Skeletal complications of eating disorders. Metabolism 2015, 64, 943–951. [Google Scholar] [CrossRef] [Green Version]
- Shimokata, H.; Andres, R.; Coon, P.; Elahi, D.; Muller, D.; Tobin, J. Studies in the distribution of body fat. II. Longitudinal effects of change in weight. Int. J. Obes. 1989, 13, 455–464. [Google Scholar]
- Zamboni, M.; Armellini, F.; Harris, T.; Turcato, E.; Micciolo, R.; Bergamo-Andreis, I.A.; Bosello, O. Effects of age on body fat distribution and cardiovascular risk factors in women. Am. J. Clin. Nutr. 1997, 66, 111–115. [Google Scholar] [CrossRef] [PubMed] [Green Version]

{kind=link}
{kind=link}
| Mean | Minimum | Maximum | Std. Dev. | |
|---|---|---|---|---|
| Age (years) | 19.86 | 15.00 | 33.00 | 4.05 |
| Experience in dance (years) | 11.32 | 8.00 | 17.00 | 2.45 |
| Exposure time per week (hours) | 15.85 | 8.00 | 39.50 | 6.76 |
| Body height (cm) | 165.95 | 154.40 | 179.10 | 5.09 |
| Body mass (kg) | 57.02 | 48.30 | 70.90 | 5.52 |
| Body mass index (kg/m2) | 20.68 | 17.50 | 25.70 | 1.70 |
| Body fat (%) | 19.31 | 10.89 | 29.86 | 4.20 |
| Free fat mass (kg) | 45.85 | 39.36 | 52.70 | 3.18 |
| Energy availability score (kcal·(kg/free fat mass·day−1) | 31.39 | 15.35 | 54.59 | 9.77 |
| Injured (N = 33) | Non-Injured (N = 17) | ANOVA | ||||
|---|---|---|---|---|---|---|
| Mean | Std. Dev. | Mean | Std. Dev. | F test | p | |
| Age (years) | 21.06 | 4.38 | 17.53 | 1.77 | 10.11 | 0.001 |
| Experience in dance (years) | 11.65 | 3.33 | 10.73 | 2.61 | 10.57 | 0.001 |
| Exposure time per week (hours) | 16.38 | 7.69 | 14.82 | 4.46 | 0.59 | 0.45 |
| Body height (cm) | 165.37 | 4.83 | 167.09 | 5.52 | 1.29 | 0.26 |
| Body mass (kg) | 57.67 | 5.46 | 55.75 | 5.57 | 1.36 | 0.25 |
| Body mass index (kg/m2) | 21.07 | 1.72 | 19.93 | 1.41 | 5.58 | 0.02 |
| Body fat (%) | 20.39 | 3.98 | 17.22 | 3.92 | 7.15 | 0.01 |
| Free fat mass (kg) | 45.78 | 3.33 | 45.98 | 2.97 | 0.04 | 0.83 |
| Energy availability score (kcal·(kg/free fat mass·day−1) | 27.89 | 12.62 | 33.20 | 7.54 | 4.47 | 0.03 |
| Injured (N = 8) | Non-Injured (N = 42) | ANOVA | ||||
|---|---|---|---|---|---|---|
| Mean | Std. Dev. | Mean | Std. Dev. | F test | p | |
| Age (years) | 20.38 | 5.04 | 19.76 | 3.90 | 0.15 | 0.70 |
| Experience in dance (years) | 10.63 | 6.12 | 9.67 | 4.85 | 0.24 | 0.63 |
| Exposure time per week (hours) | 23.19 | 9.72 | 14.45 | 5.10 | 14.25 | 0.001 |
| Body height (cm) | 163.93 | 4.19 | 166.34 | 5.19 | 1.53 | 0.22 |
| Body mass (kg) | 54.05 | 4.84 | 57.58 | 5.51 | 2.86 | 0.10 |
| Body mass index (kg/m2) | 20.06 | 1.78 | 20.80 | 1.67 | 1.29 | 0.26 |
| Body fat (%) | 18.80 | 4.56 | 19.41 | 4.18 | 0.14 | 0.71 |
| Free fat mass (kg) | 43.74 | 2.48 | 46.25 | 3.16 | 4.49 | 0.04 |
| Energy availability score (kcal·(kg/free fat mass·day−1) | 33.19 | 10.40 | 31.05 | 9.74 | 0.32 | 0.58 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Prus, D.; Mijatovic, D.; Hadzic, V.; Ostojic, D.; Versic, S.; Zenic, N.; Jezdimirovic, T.; Drid, P.; Zaletel, P. (Low) Energy Availability and Its Association with Injury Occurrence in Competitive Dance: Cross-Sectional Analysis in Female Dancers. Medicina 2022, 58, 853. https://doi.org/10.3390/medicina58070853
Prus D, Mijatovic D, Hadzic V, Ostojic D, Versic S, Zenic N, Jezdimirovic T, Drid P, Zaletel P. (Low) Energy Availability and Its Association with Injury Occurrence in Competitive Dance: Cross-Sectional Analysis in Female Dancers. Medicina. 2022; 58(7):853. https://doi.org/10.3390/medicina58070853
Chicago/Turabian StylePrus, Dasa, Dragan Mijatovic, Vedran Hadzic, Daria Ostojic, Sime Versic, Natasa Zenic, Tatjana Jezdimirovic, Patrik Drid, and Petra Zaletel. 2022. "(Low) Energy Availability and Its Association with Injury Occurrence in Competitive Dance: Cross-Sectional Analysis in Female Dancers" Medicina 58, no. 7: 853. https://doi.org/10.3390/medicina58070853