Abstract
Hepatitis E virus (HEV) is a hepatotropic virus that is a major public health concern worldwide. Autochthonous HEV is spread through oral feces in unsanitary environments, as well as vertical and, occasionally, blood transfusion. HEV is more common in developing countries, but it has recently become more widespread in developed countries as well. The Middle East (ME) has long been an endemic location for HEV infection. Therefore, the aim of this systematic review and meta-analysis was to assess the seroprevalence of anti-HEV antibodies in ME countries. The author systematically searched five databases, namely ScienceDirect, EMBASE, Scopus, PubMed, and Google Scholar, to identify English-language articles published on or before 25 April 2022. Comprehensive meta-analysis software was used for all statistical analyses (CMA, version 3, BioStat, Englewood, CO, USA). After quality control and exclusion of irrelevant studies, 80 studies were included in the qualitative synthesis and meta-analysis. A forest plot showed that the overall pooled seroprevalence of HEV infection in ME countries in the fixed-effect and random-effect models were 21.3% (95% CI: 0.209–0.216) and 11.8% (95% CI: 0.099–0.144), respectively. Furthermore, the findings showed a high level of heterogeneity (I2 = 98.733%) among the included studies. In both fixed-effect and random-effect models, the seroprevalence of HEV infection by country was high in Egypt as compared to other regions, at 35.0% (95% CI: 0.342–0.359), and 34.7% (95% CI: 0.153–0.611), respectively. The seroprevalence of HEV infection by country was high among pregnant women, at 47.9% (95% CI: 0.459–0.499) in the fixed-effect model, and in renal transplant recipients, at 30.8% (95% CI: 0.222–0.410) in the random-effect model. The seroprevalence of HEV infection varies by country and study population in the Middle East. More research is needed to determine the disease’s incidence, morbidity, and mortality in the region, where it is prevalent.
1. Introduction
The World Health Organization (WHO) launched a global strategy to stop viral hepatitis transmission in 2016, recommending that persons with viral hepatitis have access to safe, accessible, and effective prevention, care, and treatment services []. By 2030, the goals are to reduce the number of new instances of hepatitis by 90 percent, treat 80 percent of eligible patients infected with viral hepatitis, and reduce the number of hepatitis-related fatalities by 65 percent []. Globally, nearly 1.34 million deaths were attributed to viral hepatitis in 2015, with 95 percent of those deaths attributed to chronic hepatitis B and C infections and the remainder to hepatitis A and E infections [,].
Global estimates suggest that more than 20 million new instances of hepatitis E virus (HEV) infections occur each year, with 3.3 million of those becoming symptomatic []. In 2015, the WHO reported 44,000 fatal HEV infections, accounting for about 3.3 percent of all viral hepatitis-related deaths [].
HEV is a water- and food-borne illness that can cause severe epidemics in areas where sanitation is lacking [,]. However, there has been evidence of zoonotic and transfusion-related transmission [,]. Because there is no specific treatment for HEV infection, it is managed mostly through supportive care [,]. Prevention, on the other hand, focuses on limiting exposure through improved sanitation, clean food and drinking water, and vaccination []. In comparison to hepatitis B and C, HEV infection is less likely to cause chronic liver damage, and the development of fulminant hepatitis, albeit rare, is mostly influenced by host-specific rather than virus-specific variables [].
Clinical signs and symptoms such as myalgia, arthralgia, anorexia, hepatomegaly, fever, weakness, vomiting, and jaundice emerge two to nine weeks after HEV exposure. In rare and severe cases, HEV can cause abrupt liver failure. Chronic instances are uncommon; however, they can occur in immunocompromised persons [,]. There is a variety of laboratory tests for HEV infection diagnosis, which can be divided into direct (detection of HEV or viral protein via polymerase chain reaction or enzyme immunoassay) and indirect (detection of anti-HEV antibodies) approaches [,]. Recent HEV infection is linked to the existence of IgM anti-HEV antibodies. Furthermore, the presence of anti-HEV IgG antibodies is indicative of recent or distant HEV exposure. Both antibodies are critical for HEV infection diagnosis and can be linked to long-term infection [,].
The majority of people in Middle Eastern (ME) countries live in middle-income countries, where viral hepatitis is a major health concern []. Furthermore, HEV infection is highly endemic in most of the countries in this region [,]. Given these countries’ changing socioeconomic conditions, identifying the epidemiological pattern of HEV infection will assist healthcare policymakers in making better decisions regarding future strategies for controlling this virus, as well as selecting and implementing cost-effective preventative methods [,].
Furthermore, to the very best of our knowledge, there remains a dearth of knowledge with respect to the prevalence of HEV-infected people with anti-HEV antibodies (IgG) in ME countries. Therefore, this systematic review and meta-analysis is the first attempt to provide a summarized and up-to-date estimation of the seroprevalence of HEV infection in ME countries.
2. Materials and Methods
2.1. Data Sources and Literature Search Strategy
The author systematically searched five databases, namely ScienceDirect, EMBASE, Scopus, PubMed, and Google Scholar, to identify English-language articles published on or before 25 April 2022 that originally reported data on the prevalence of HEV infection in ME countries. The following keywords were used: “Hepatitis E virus”, “HEV”, and “Prevalence”, combined with the names of ME countries, namely Akrotiri and Dhekelia, Bahrain, Cyprus, Egypt, Iran, Iraq, Israel, Jordan, Kuwait, Lebanon, Oman, Palestine, Qatar, Saudi Arabia, Syria, Turkey, United Arab Emirates, and Yemen.
The current systematic review and meta-analysis was conducted according to the PRISMA recommendations (Supplementary Material S1) and was registered with the International Prospective Register of Systematic Reviews (PROSPERO, registration No. CRD42022330216).
2.2. Eligibility Criteria
The author included all observational studies conducted in ME countries that had, at least, an English abstract and reported on the prevalence of HEV-infected people with anti-HEV antibodies (IgG) among the general population, blood donors, hemodialysis patients, children, acute viral hepatitis patients, pregnant women, male blood donors, drug addicts, HIV positive individuals, thalassemia patients, soldiers, hemophiliac patients, renal transplant recipients, non-A-C hepatitis patients, and solid organ recipients. The systematic review and meta-analysis were designed to include people of all ages. Case reports, case series, letters, commentaries, editorials, non-human studies, symposia, correspondences, and citations without full text were all excluded from the study.
2.3. Study Screening and Data Extraction
The article screening process and removal of duplicates were managed using EndNote V.X8 software. Furthermore, two researchers (F.Q. and S.K.) meticulously and manually treated the data to reduce the chance of duplication.
The following details were extracted from the included articles using a standardized data collection form: first-author name, publication year, study sample, study country, sampling year, study population, type of study, participants’ age (range), study city, percentage of male participants, percentage of female participants, and prevalence of HEV-infected people with anti-HEV antibodies (IgG).
2.4. Quality Assessment
The quality of the included articles was assessed using the National Institute of Health quality assessment technique [,]. This assessment tool was used because it allows for a thorough evaluation of the quality of the research included. Furthermore, the general quality of the studies was graded as good, fair, or poor, and these ratings were incorporated into the meta-analytic results. The two researchers (F.Q. and R.A.) compared their evaluations for each study, and any disagreements were handled through a joint discussion.
2.5. Data Synthesis and Statistical Analysis
Comprehensive meta-analysis software was used for all statistical analyses (CMA, version 3, BioStat, USA). To reset the effect size value obtained from the meta-analysis, the fail-safe N approach was used to determine the number of studies that should be added to the meta-analysis. The average effect size of the meta-analysis studies was computed. The seroprevalence of HEV infection in ME countries was pooled and investigated using a random-effect model, with the results displayed in forest plots. Using the extracted data, the rate of events, their 95 percent confidence intervals, and their p-values were determined. The I2 statistic was used to assess the degree of heterogeneity among the included studies, with I2 values of 0–40%, 25–50%, 50–75%, and >75% indicating trivial, low, moderate, and high heterogeneity, respectively []. A non-significant degree of statistical heterogeneity was assumed when p < 0.1 or I2 < 50 percent []. Because of the considerable heterogeneity, a random-effects model was adopted. A funnel plot was used to discover potential signs of publication bias between included papers, as detected by Begg’s and Mazumdar’s rank correlation tests.
3. Results
3.1. Search Outcomes
The search yielded a total of 14,497 articles from five databases: ScienceDirect (n = 1816), EMBASE (n = 2326), Scopus (n = 2354), PubMed (n = 3328), and Google Scholar (n = 4673). After duplicates were excluded, 6539 articles remained. A further 3257 articles were excluded due to the studies being conducted in non-ME countries, in addition to 1965 studies deemed irrelevant after screening the titles and abstracts. Then, we reviewed the full text of the remaining 1317 articles and excluded 1237 studies for not fulfilling our inclusion criteria. Ultimately, 80 studies were included in the qualitative synthesis and meta-analysis. The PRISMA flow chart for the process of article screening and selection is presented in Figure 1.
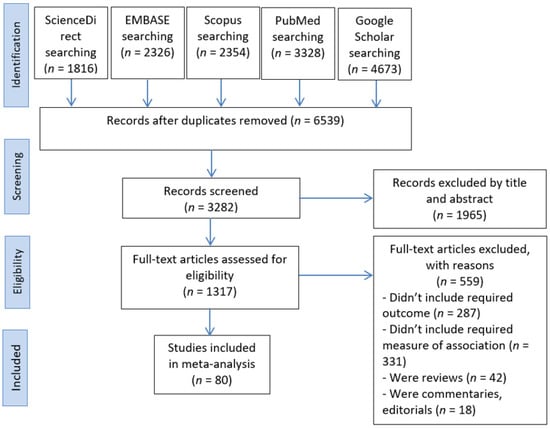
Figure 1.
PRISMA flow chart of study identification and study selection process.
3.2. Characteristics of the Included Studies
Of the 80 included studies, 41 were conducted in Iran, 14 in Turkey, 8 in Egypt, 4 in Israel, 3 in Saudi Arabia, 3 in Iraq, 2 in Qatar, 1 in Kuwait, 1 in Syria, 1 in Yemen, 1 in the United Arab Emirates, 1 in Lebanon, 1 in Palestine, and 1 in Jordan. The prevalence of HEV IgG antibodies in the included studies ranged from 0.8% to 84.3% (range = 14.9). The targeted populations in the included studies were the general population (15 studies), blood donors (12 studies), hemodialysis patients (12 studies), children (11 studies), acute viral hepatitis patients (8 studies), pregnant women (7 studies), male blood donors (3 studies), drug addicts (3 studies), HIV-positive individuals (3 studies), thalassemia patients (2 studies), soldiers (1 study), hemophilia patients (1 study), renal transplant recipients (1 study), non-A-C hepatitis patients (1 study), and solid organ recipients (1 study). The sample size of the included articles ranged from 43 to 11,604 (average = 844) (Table 1).

Table 1.
Characteristics of the included studies in the systematic review and meta-analysis.
3.3. Overall Pooled Seroprevalence of Hepatitis E Virus Infection in Middle Eastern Countries
All eighty included studies were pooled for meta-analysis; the forest plot showed that the overall pooled seroprevalence of HEV infection in ME countries in the fixed-effect and random-effect models was 21.3% (95% CI: 0.209–0.216), and 11.8% (95% CI: 0.099–0.144), respectively. Furthermore, the findings showed a high level of heterogeneity (I2 = 98.733%) among the included studies. Furthermore, the overall pooled seroprevalence of HEV infection in ME countries was statistically significant (pooled p-value < 0.001) in both fixed-effect and random-effect models (Figure 2). Table 2 shows the mean effect size and confidence intervals based on the random effect analysis of the studies in the meta-analysis.
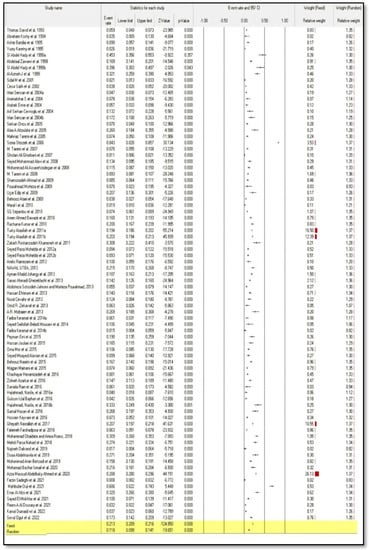
Figure 2.
Forest plot meta-analysis of seroprevalence of hepatitis E virus infection in Middle Eastern countries [,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,].
Table 2.
Meta-analysis and effect analysis values of included studies, homogeneous distribution value, average effect size, and confidence intervals.
3.4. Subgroup Analysis
In both fixed-effect and random-effect models, the seroprevalence of HEV infection by country was highest in Egypt as compared to other countries, at 35.0% (95% CI: 0.342–0.359) and 34.7% (95% CI: 0.153–0.611), respectively (Figure 3).
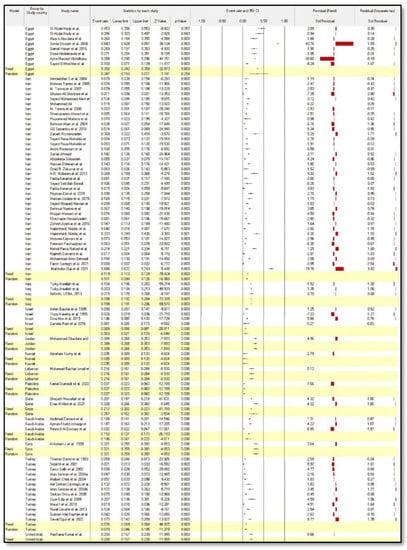
Figure 3.
Forest plot meta-analysis of seroprevalence of hepatitis E virus infection by country [,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,].
The seroprevalence of HEV infection by the study population was highest in pregnant women 47.9% (95% CI: 0.459–0.499) in the fixed-effect model and in renal transplant recipients, 30.8% (95% CI: 0.222–0.410) in the random-effect model, as compared to other populations (Figure 4).
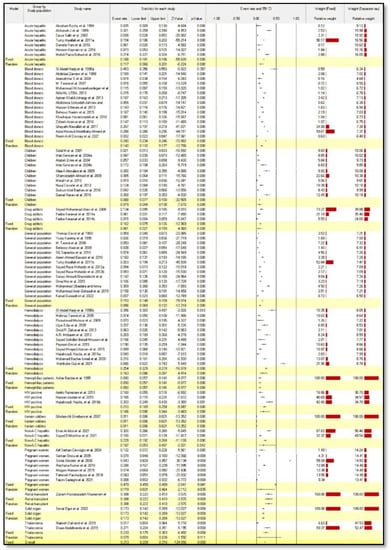
Figure 4.
Forest plot meta-analysis of seroprevalence of hepatitis E virus infection by study population [,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,].
3.5. Publication Bias
The results of Begg’s and Mazumdar’s rank correlation tests revealed a dispersed distribution, implying publication bias. The p-values for Kendall’s tau without continuity and Kendall’s tau with continuity were both 0.001 (Table 3). Figure 5 depicts a funnel plot of the seroprevalence of HEV infection in ME countries with publication bias.
Table 3.
Begg’s and Mazumdar’s rank correlation.
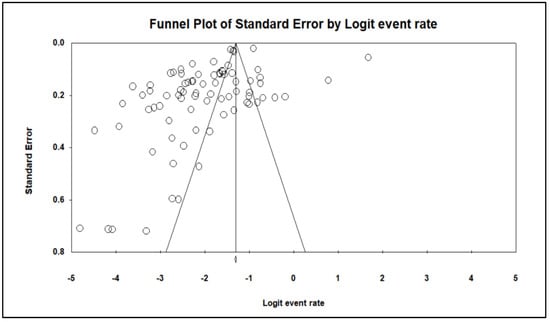
Figure 5.
Publication bias of the seroprevalence of hepatitis E virus infection in Middle Eastern countries.
4. Discussion
Worldwide, seroprevalence-based studies have received increased attention in recent years. However, due to incorrect diagnosis, underestimation, and a lack of awareness among clinicians about HEV, the published literature contains considerable gaps [,]. As a result, the goal of this study was to determine the seroprevalence of HEV infection in ME countries. Researchers and policymakers may benefit from the information in this systematic review and meta-analysis in order to better understand disease spread and develop effective control and prevention methods, particularly in ME countries.
Our findings showed that the seroprevalence of HEV infection in ME countries ranged from 0.8% among Iranian pregnant women [] to 84.3% among Egyptian pregnant women []. Different test methodologies and geographic locations, research sample size, surveillance year, and other factors could explain these observed differences in HEV seroprevalence. However, in our study, in the fixed-effect and random-effect models, the overall pooled seroprevalence of HEV infection in ME countries was 21.3% and 11.8%, respectively. According to a recent systematic review and meta-analysis, the overall pooled prevalence of HEV infection in pregnant women around the world was 16.51% []. A systematic review of HEV seroprevalence in thirteen African nations found that it ranged from zero to eighty-four percent, with pregnant women and rural areas having higher immunoglobulin levels than other areas []. The estimated pooled seroprevalence of HEV in Chinese blood donors was 30%. In European countries, the estimated seroprevalence of HEV ranged from 0.6% to 52.5% []. Another comprehensive evaluation of the Brazilian population found a 6.0% overall seroprevalence of HEV infection []. Furthermore, the pooled prevalence in our study is higher than in certain primary studies conducted among pregnant women in different countries, such as Serbian blood donors (15.0%) [], as well as in Mexico (5.7%) [], Pakistan (8.86%) [], and Sudan (10.3%) [].
Our analysis showed that Egypt has the highest seroprevalence of HEV infections compared to other countries. In Egypt, HEV infection is a neglected disease. In Egyptian hospitals, HEV testing is not frequently used for the diagnosis of suspected hepatitis patients []. Anti-HEV IgG seroprevalence in Egyptians is among the highest in the world, at up to 84 percent [,]. Furthermore, an HEV outbreak was previously observed in Assiut governorate rural villages [].
Despite the fact that the incidence of HEV has declined significantly in recent years as a result of improved hygiene conditions [], our analysis revealed that the seroprevalence of HEV infection was higher in pregnant women when compared to other populations. There is a considerable chance of vertical transmission of these viruses from the mother to the fetus, which can result in maternal and fetal problems, such as abortion, neonatal mortality, and early labor []. To avoid any negative consequences, it is critical to diagnose HEV infections in pregnant women.
An increasing number scientists and researchers are becoming aware of the repercussions of HEV infection, which include severe liver impairment and a high rate of morbidity and mortality, particularly in pregnant women. As a result, the pathophysiology and immunology of HEV interaction during pregnancy have received increased attention. However, especially in HEV endemic areas, it is critical to investigate genetic and environmental causes. To control and stop the disease in the near future, immunological research and prevention, as well as treatment measures, must be enhanced. In addition, in countries where the disease is endemic, cost-effective immunization efforts are required.
Despite the fact that the current meta-analysis has a large sample size and includes all ME countries and populations previously researched, it is subject to numerous limitations. The majority of the studies reviewed used distinct anti-HIV IgG ELISA kits with varying specificity and sensitivity, which could impair the reliability and accuracy of the tests. Only the anti-HEV IgG antibody level, which appears mainly after infection, was used to determine seroprevalence. Furthermore, the studies included in this systematic review and meta-analysis were observational, with a wide range of baseline characteristics, sample sizes, and sampling years.
5. Conclusions
The seroprevalence of HEV infection varies by country and study population in the ME and is highest in Egypt as compared to other countries and is highest in pregnant women and in renal transplant recipients as compared to other populations. More research is needed to determine the disease’s incidence, morbidity, and mortality in the region, where it is prevalent. In addition, essential steps should be taken to control and prevent HEV infection in general and in pregnant women in particular. Visiting endemic areas requires extra attention, especially when it comes to drinking water and food safety.
Supplementary Materials
The following supporting information can be downloaded at: https://www.mdpi.com/article/10.3390/medicina58070905/s1, Supplementary Material S1: The PRISMA recommendations checklist [].
Funding
This research received no external funding.
Institutional Review Board Statement
The protocol of the study was registered with the International Prospective Register of Systematic Reviews (PROSPERO, registration No. CRD42022330216).
Informed Consent Statement
Not applicable.
Data Availability Statement
Not applicable.
Acknowledgments
The author thanks Samer Abuzerr, Saeed M. Kabrah, and Radi T. Assafi for their help with data analysis, article screening, data extraction, and review of the manuscript. The author also extends his gratitude to Umm Al Qura University for supplying the analysis program.
Conflicts of Interest
The author declares that there is no conflict of interest related to this work.
References
- WHO. Global Health Sector Strategy on Viral Hepatitis 2016–2021: Towards Ending Viral Hepatitis; World Health Organization: Geneva, Switzerland, 2016.
- WHO. Global Hepatitis Report 2017; World Health Organization: Geneva, Switzerland, 2017.
- Bigna, J.J.; Modiyinji, A.F.; Nansseu, J.R.; Amougou, M.A.; Nola, M.; Kenmoe, S.; Temfack, E.; Njouom, R. Burden of hepatitis E virus infection in pregnancy and maternofoetal outcomes: A systematic review and meta-analysis. BMC Pregnancy Childbirth 2020, 20, 426. [Google Scholar] [CrossRef] [PubMed]
- Dalton, H.R.; Izopet, J. Transmission and epidemiology of hepatitis E virus genotype 3 and 4 infections. Cold Spring Harb. Perspect. Med. 2018, 8, a032144. [Google Scholar] [CrossRef] [PubMed]
- Izopet, J.; Lhomme, S.; Chapuy-Regaud, S.; Mansuy, J.-M.; Kamar, N.; Abravanel, F. HEV and transfusion-recipient risk. Transfus. Clin. Biol. 2017, 24, 176–181. [Google Scholar] [CrossRef] [PubMed]
- Smith, D.B.; Simmonds, P. Hepatitis E virus and fulminant hepatitis—A virus or host-specific pathology? Liver Int. 2015, 35, 1334–1340. [Google Scholar] [CrossRef] [PubMed]
- Mirazo, S.; Ramos, N.; Mainardi, V.; Gerona, S.; Arbiza, J. Transmission, diagnosis, and management of hepatitis E: An update. Hepatic Med. Evid. Res. 2014, 6, 45. [Google Scholar] [CrossRef]
- Pérez-Gracia, M.T.; Suay, B.; Mateos-Lindemann, M.L. Hepatitis E: An emerging disease. Infect. Genet. Evol. 2014, 22, 40–59. [Google Scholar] [CrossRef]
- Fujiwara, S.; Yokokawa, Y.; Morino, K.; Hayasaka, K.; Kawabata, M.; Shimizu, T. Chronic hepatitis E: A review of the literature. J. Viral Hepat. 2014, 21, 78–89. [Google Scholar] [CrossRef]
- Aggarwal, R. Diagnosis of hepatitis E. Nat. Rev. Gastroenterol. Hepatol. 2013, 10, 24–33. [Google Scholar] [CrossRef]
- Alavian, S.M.; Rezaee-Zavareh, M.S. The Middle East and hepatitis C virus infection: Does it need special attention? Lancet Infect. Dis. 2016, 16, 1006–1007. [Google Scholar] [CrossRef][Green Version]
- Tufenkeji, H. Hepatitis A shifting epidemiology in the Middle East and Africa. Vaccine 2000, 18, S65–S67. [Google Scholar] [CrossRef]
- Mahboobi, N.; Alavian, S.M. Hepatitis A in the Eastern Mediterranean region: A review on the prevalence. Scimetr 2014, 2, e87346. [Google Scholar] [CrossRef]
- Franco, E.; Bagnato, B.; Marino, M.G.; Meleleo, C.; Serino, L.; Zaratti, L. Hepatitis B: Epidemiology and prevention in developing countries. World J. Hepatol. 2012, 4, 74. [Google Scholar] [CrossRef] [PubMed]
- Rezaee-Zavareh, M.S.; Karimi-Sari, H.; Dolatimehr, F.; Alavian, S.M. Hepatitis A virus infection, vaccination and Iranian healthcare workers. Hepat. Mon. 2015, 15, e35238. [Google Scholar] [CrossRef] [PubMed]
- NHLBI. Quality Assessment Tool for Observational Cohort and Cross-Sectional Studies; National Heart, Lung, and Blood Institute: Bethesda, MA, USA, 2014.
- NHLBI. National Institute of Health Study Quality Assessment Tool; National Heart, Lung, and Blood Institute: Bethesda, MA, USA, 2017.
- Higgins, J.P.; Thompson, S.G. Quantifying heterogeneity in a meta-analysis. Stat. Med. 2002, 21, 1539–1558. [Google Scholar] [CrossRef]
- DerSimonian, R.; Kacker, R. Random-effects model for meta-analysis of clinical trials: An update. Contemp. Clin. Trials 2007, 28, 105–114. [Google Scholar] [CrossRef]
- Thomas, D.L.; Quinn, T.; Mahley, R.; Palaoglu, K.E.; Badur, S. Epidemiology of hepatitis E virus infection in Turkey. Lancet 1993, 341, 1561–1562. [Google Scholar] [CrossRef]
- Koshy, A.; Richards, A.L.; Al-Mufti, S.; Grover, S.; Shabrawy, M.A.; Pacsa, A.; Al-Anezi, A.A.H.; Al-Nakib, B.; Burans, J.; Carl, M. Acute sporadic hepatitis E in Kuwait. J. Med. Virol. 1994, 42, 405–408. [Google Scholar] [CrossRef]
- Barzilai, A.; Schulman, S.; Karetnyi, Y.V.; Favorov, M.O.; Levin, E.; Mendelson, E.; Weiss, P.; Fields, H.A.; Varon, D.; Martinowitz, U. Hepatitis E virus infection in hemophiliacs. J. Med. Virol. 1995, 46, 153–156. [Google Scholar] [CrossRef]
- Karetnyi, Y.V.; Handsher, R.; Aboudy, Y.; Varsano, N.; Mendelson, E.; Weiss, P.; Levin, E.; Bar-Shani, S.; Schwartz, E.; Fields, H.A. Serological evidence for hepatitis E virus infection in Israel. J. Med. Virol. 1995, 45, 316–320. [Google Scholar] [CrossRef]
- Abdelaal, M.; Zawawi, T.; Al Sobhi, E.; Jeje, O.; Gilpin, C.; Kinsara, A.; Osoba, A.; Oni, G. Epidemiology of hepatitis E virus in male blood donors in Jeddah, Saudi Arabia. Ir. J. Med. Sci. 1998, 167, 94–96. [Google Scholar] [CrossRef]
- SI, A.H.; El-Din, M.S.; El-Din, M.E. A high hepatitis E virus (HEV) seroprevalence among unpaid blood donors and haemodialysis patients in Egypt. J. Egypt. Public Health Assoc. 1998, 73, 165–179. [Google Scholar]
- Al-Azmeh, J.; Frösner, G.; Darwish, Z.; Bashour, H.; Monem, F. Hepatitis E in Damascus, Syria. Infection 1999, 27, 221–223. [Google Scholar] [CrossRef] [PubMed]
- Sıdal, M.; Ünüvar, E.; Oğuz, F.; Cihan, C.; Önel, D.; Badur, S. Age-specific seroepidemiology of hepatitis A, B, and E infections among children in Istanbul, Turkey. Eur. J. Epidemiol. 2001, 17, 141–144. [Google Scholar] [CrossRef] [PubMed]
- Colak, D.; Ogunc, D.; Gunseren, F.; Velipasaoglu, S.; Aktekin, M.; Gültekin, M. Seroprevalence of antibodies to hepatitis A and E viruses in pediatric age groups in Turkey. Acta Microbiol. Et Immunol. Hung. 2002, 49, 93–97. [Google Scholar] [CrossRef] [PubMed]
- Cesur, S.; Akin, K.; Doğaroğlu, I.; Birengel, S.; Balik, I. Hepatitis A and hepatitis E seroprevalence in adults in the Ankara area. Mikrobiyoloji Bul. 2002, 36, 79–83. [Google Scholar]
- Cevrioglu, A.S.; Altindis, M.; Tanir, H.M.; Aksoy, F. Investigation of the incidence of hepatitis E virus among pregnant women in Turkey. J. Obstet. Gynaecol. Res. 2004, 30, 48–52. [Google Scholar] [CrossRef]
- Sencan, I.; Sahin, I.; Kaya, D.; Oksuz, S.; Yildirim, M. Assessment of HAV and HEV seroprevalence in children living in post-earthquake camps from Düzce, Turkey. Eur. J. Epidemiol. 2004, 19, 461–465. [Google Scholar] [CrossRef]
- Atabek, M.E.; Fýndýk, D.; Gulyuz, A.; Erkul, I. Prevalence of anti-HAV and anti-HEV antibodies in Konya, Turkey. Health Policy 2004, 67, 265–269. [Google Scholar] [CrossRef]
- Aminiafshar, S.; Alimagham, M.; Gachkar, L.; Yousefi, F.; Attarchi, Z. Anti hepatitis E virus seropositivity in a group of blood donors. Iran. J. Public Health 2004, 33, 53–56. [Google Scholar]
- Oncu, S.; Oncu, S.; Okyay, P.; Ertug, S.; Sakarya, S. Prevalence and risk factors for HEV infection in pregnant women. Med. Sci. Monit. 2006, 12, 39. [Google Scholar]
- Aboulata, A.A.; Ahmad, M.S.; Shaban, M.; Zayd, K.; AM, A.E.-M. Prevalence of hepatitis E virus in Egyptian children presented with minor hepatic disorders. Egypt. J. Immunol. 2005, 12, 71–76. [Google Scholar] [PubMed]
- Taremi, M.; Khoshbaten, M.; Gachkar, L.; EhsaniArdakani, M.; Zali, M. Hepatitis E virus infection in hemodialysis patients: A seroepidemiological survey in Iran. BMC Infect. Dis. 2005, 5, 36. [Google Scholar] [CrossRef]
- Stoszek, S.K.; Abdel-Hamid, M.; Saleh, D.a.A.; Kafrawy, S.E.; Narooz, S.; Hawash, Y.; Shebl, F.M.; El Daly, M.; Said, A.; Kassem, E. High prevalence of hepatitis E antibodies in pregnant Egyptian women. Trans. R. Soc. Trop. Med. Hyg. 2006, 100, 95–101. [Google Scholar] [CrossRef] [PubMed]
- Taremi, M.; Gachkar, L.; MahmoudArabi, S.; Kheradpezhouh, M.; Khoshbaten, M. Prevalence of antibodies to hepatitis E virus among male blood donors in Tabriz, Islamic Republic of Iran. East. Mediterr. Health J. 2007, 13, 98–102. [Google Scholar] [PubMed]
- Ghorbani, G.A.; Alavian, S.-M.; Esfahani, A.A.; Assari, S. Seroepidemiology of hepatitis E virus in Iranian soldiers. Hepat. Mon. 2007, 7, 123–126. [Google Scholar]
- Alavi, S.M.; Ahmadi, F.; Ghasemirad, M.R. Seroepidemiological study of hepatitis E virus in drug addicts in Ahvaz, Southern Iran: 2005–2006. Hepat. Mon. 2008, 8, 263–266. [Google Scholar]
- Assarehzadegan, M.A.; Shakerinejad, G.; Amini, A.; Rezaee, S.R. Seroprevalence of hepatitis E virus in blood donors in Khuzestan Province, southwest Iran. Int. J. Infect. Dis. 2008, 12, 387–390. [Google Scholar] [CrossRef][Green Version]
- Taremi, M.; Alizadeh, A.; Ardalan, A.; Ansari, S.; Zali, M. Seroprevalence of hepatitis E in Nahavand, Islamic Republic of Iran: A population-based study. East. Mediterr. Health J. 2008, 14, 157–162. [Google Scholar]
- Uçar, E.; Cetin, M.; Kuvandik, C.; Helvaci, M.R.; Güllü, M.; Hüzmeli, C. Hepatitis E virus seropositivity in hemodialysis patients in Hatay province, Turkey. Mikrobiyoloji Bul. 2009, 43, 299–302. [Google Scholar]
- Shamsizadeh, A.; Nikfar, R.; Makvandi, M.; Shamsizadeh, N. Seroprevalence of hepatitis E virus infection in children in the Southwest of Iran. Hepat. Mon. 2009, 9, 269–276. [Google Scholar]
- Ataei, B.; Nokhodian, Z.; Javadi, A.A.; Kassaian, N.; Shoaei, P.; Farajzadegan, Z.; Adibi, P. Hepatitis E virus in Isfahan Province: A population-based study. Int. J. Infect. Dis. 2009, 13, 67–71. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Pourahmad, M.; Sotoudeh, J.A.; Nasiri, H. Brief Report: Hepatitis E virus infection in hemodialysis patients: A seroepidemiological survey in Jahrom, Southern Iran. Hepat. Mon. 2009, 9, 232–235. [Google Scholar]
- Maral, I.; Budakoglu, I.; Ceyhan, M.; Atak, A.; Bumin, M. Hepatitis E virus seroepidemiology and its change during 1 year in primary school students in Ankara, Turkey. Clin. Microbiol. Infect. 2010, 16, 831–835. [Google Scholar] [CrossRef] [PubMed]
- Bawazir, A.A.; Hart, C.A.; Sallam, T.A.; Parry, C.M.; Beeching, N.J.; Cuevas, L.E. Seroepidemiology of hepatitis A and hepatitis E viruses in Aden, Yemen. Trans. R. Soc. Trop. Med. Hyg. 2010, 104, 801–805. [Google Scholar] [CrossRef]
- Kumar, R.M.; Uduman, S.; Rana, S.; Kochiyil, J.K.; Usmani, A.; Thomas, L. Sero-prevalence and mother-to-infant transmission of hepatitis E virus among pregnant women in the United Arab Emirates. Eur. J. Obstet. Gynecol. Reprod. Biol. 2001, 100, 9–15. [Google Scholar] [CrossRef]
- Sepanlou, S.G.; Rezvan, H.; Amini-Kafiabad, S.; Dayhim, M.; Merat, S. A population-based seroepidemiological study on hepatitis E virus in Iran. Middle East J. Dig. Dis. 2010, 2, 97. [Google Scholar]
- Turky, A.M.; Akram, W.; Al-Naaimi, A.S.; Omer, A.R.; Al-Rawi, J.R. Analysis of acute viral hepatitis (A and E) in Iraq. Glob. J. Health Sci. 2011, 3, 70. [Google Scholar] [CrossRef]
- Khameneh, Z.R.; Sepehrvand, N.; Masudi, S. Seroprevalence of hepatitis E among Iranian renal transplant recipients. Hepat. Mon. 2011, 11, 646. [Google Scholar] [CrossRef]
- Mohebbi, S.R.; Rostami Nejad, M.; Tahaei, S.M.E.; Pourhoseingholi, M.A.; Habibi, M.; Azimzadeh, P.; Naghoosi, H.; Karayiannis, P.; Zali, M.R. Seroepidemiology of hepatitis A and E virus infections in Tehran, Iran: A population based study. Trans. R. Soc. Trop. Med. Hyg. 2012, 106, 528–531. [Google Scholar] [CrossRef]
- Jahromi, A.S.; Pourahmad, M. Hepatitis E virus and serum level aminotransferases in blood donors. Rep. Biochem. Mol. Biol. 2013, 2, 48. [Google Scholar]
- Ghezeldasht, S.A.; Miri, R.; Hedayatimoghadam, M.; Shamsian, A.; Bidkhori, H.; Fathimoghadam, F.; Rezaee, S.A. Population movement and virus spreading: HEV spreading in a Pilgrimage city, Mashhad in northeast Iran; an example. Hepat. Mon. 2013, 13, e10255. [Google Scholar] [CrossRef] [PubMed]
- Cevahir, N.; Demir, M.; Bozkurt, A.I.; Ergin, A.; Kaleli, I. Seroprevalence of hepatitis e virus among primary school children. Pak. J. Med. Sci. 2013, 29, 629. [Google Scholar] [CrossRef] [PubMed]
- Ehteram, H.; Ramezani, A.; Eslamifar, A.; Sofian, M.; Banifazl, M.; Ghassemi, S.; Aghakhani, A.; Mashayekhi, P. Seroprevalence of Hepatitis E Virus infection among volunteer blood donors in central province of Iran in 2012. Iran. J. Microbiol. 2013, 5, 172. [Google Scholar] [PubMed]
- Zekavat, O.R.; Makarem, A.; Karami, M.Y.; Amanat, A.; Mohandes, M.; Habibagahi, M. Serological investigation for hepatitis E virus infection in the patients with chronic maintenance hemodialysis from southwest of Iran. Asian J. Transfus. Sci. 2013, 7, 21. [Google Scholar]
- Mobaien, A.; Mohammadi, R.; Sorouri, R.; Sadeghi, K. Hepatitis E virus seroprevalence in haemodialysis patients in Zanjan Province, Islamic Republic of Iran. East. Mediterr. Health J. 2013, 19, 608–612. [Google Scholar] [CrossRef]
- Johargy, A.K.; Mahomed, M.F.; Khan, M.M.; Kabrah, S. Anti hepatitis E virus seropositivity in a group of male blood donors in Makkah, Saudi Arabia. J. Pak. Med. Assoc. 2013, 63, 185–189. [Google Scholar]
- Utba, N.M. The prevalence of hepatitis E virus in Al-Sadr City-Baghdad. Clin. Lab. 2013, 59, 115–120. [Google Scholar] [CrossRef]
- Ramezani, A.; Velayati, A.A.; Khorami-Sarvestani, S.; Eslamifar, A.; Mohraz, M.; Banifazl, M.; Bidari-Zerehpoosh, F.; Yaghmaei, F.; McFarland, W.; Foroughi, M. Hepatitis E virus infection in patients infected with human immunodeficiency virus in an endemic area in Iran. Int. J. STD AIDS 2013, 24, 769–774. [Google Scholar] [CrossRef]
- Keramat, F.; Mamani, M.; Samadi, M.; Mohammadnezhad, S.; Eini, P.; Moradi, A. Seroprevalence of hepatitis E Virus among injection drug users and non-injection drug users in Hamadan, west of Iran. Avicenna J. Clin. Microbiol. Infect. 2014, 1, 22343. [Google Scholar] [CrossRef][Green Version]
- Mousavi, S.S.B.; Motemednia, F.; Mousavi, M.B. Epidemiology of hepatitis e virus infection in patients on chronic hemodialysis. Jundishapur J. Microbiol. 2014, 7, e6993. [Google Scholar]
- Eini, P.; Mamani, M.; Javani, M. Seroprevalence of hepatitis e among hemodialysis patients: A report from Hamadan, Iran. Hepat. Mon. 2015, 15, e26260. [Google Scholar] [CrossRef]
- Mor, O.; Bassal, R.; Michaeli, M.; Wax, M.; Ram, D.; Cohen-Ezra, O.; Cohen, D.; Mendelson, E.; Ben-Ari, Z.; Shohat, T. Prevalence of hepatitis E virus antibodies, Israel, 2009–2010. Emerg. Infect. Dis. 2015, 21, 692. [Google Scholar] [CrossRef] [PubMed]
- Mamani, M.; Zamani, M.; Hashemi, S.H.; Keramat, F. Seroprevalence of antibodies to hepatitis E virus among pregnant women. Avicenna J. Clin. Microbiol. Infect. 2015, 2, 25339. [Google Scholar] [CrossRef]
- Alavian, S.M.; Ataei, B.; Ebrahimi, A.; Pirhaji, O.; Azad, R.; Olya, B.; Ataei, A.M. Anti-hepatitis E antibody in hemodialysis patients in Isfahan, Iran: Prevalence and risk factors. Hepat. Mon. 2015, 15, e23633. [Google Scholar] [CrossRef] [PubMed]
- Joulaei, H.; Rudgari, O.; Motazedian, N.; Gorji-Makhsous, S. Hepatitis E virus seroprevalence in HIV positive individuals in Shiraz, Southern Iran. Iran. J. Microbiol. 2015, 7, 103–108. [Google Scholar]
- Naeimi, B.; Kalimani, F.M.; Pourfatolah, A.A.; Azimzadeh, M.; Mankhian, A.; Akbarzadeh, S.; Hajiani, G.; Kooshesh, F.; Khamisipour, G. Hepatitis E Virus seroprevalence among blood donors in Bushehr, South of Iran. Hepat. Mon. 2015, 15, e29219. [Google Scholar] [CrossRef]
- Ram, D.; Manor, Y.; Gozlan, Y.; Schwartz, E.; Ben-Ari, Z.; Mendelson, E.; Mor, O. Hepatitis E virus genotype 3 in sewage and genotype 1 in acute hepatitis cases, Israel. Am. J. Trop. Med. Hyg. 2016, 95, 216–220. [Google Scholar] [CrossRef]
- Keyvani, H.; Shamabadi, M.S.; Najafifard, S.; Hajibeigi, B.; Fallahian, F.; Alavian, S.-M. Seroprevalence of anti-HEV and HEV RNA among volunteer blood donors and patients with Hepatitis B and C in Iran. Bangladesh Liver J. 2009, 1, 34–37. [Google Scholar] [CrossRef]
- Hajiahmadi, N.; Moradi, A.; Vakili, M.A.; Javid, N.; Kelishadi, M.; Bazouri, M.; Tabarraei, A. Hepatitis E virus Seroprevalence and viremia in hemodialysis and HIV infected patients in Iran. Iran. J. Virol. 2016, 10, 12–17. [Google Scholar] [CrossRef]
- Hesamizadeh, K.; Sharafi, H.; Keyvani, H.; Alavian, S.M.; Shabankareh, A.N.-T.; Olyaie, R.S.; Keshvari, M. Hepatitis A virus and hepatitis E virus seroprevalence among blood donors in Tehran, Iran. Hepat. Mon. 2016, 16, e32215. [Google Scholar] [CrossRef]
- Azarkar, Z.; Miri, M.R.; Arjmand, S. Investigating the seroprevalence of hepatitis E among blood donors referring to blood donation centers in Birjand county in Iran. Mod. Care J. 2016, 13, e9456. [Google Scholar] [CrossRef]
- Hasan, G.; Assiri, A.; Marzuuk, N.; Daef, E.; Abdelwahab, S.; Ahmed, A.; Mohamad, I.; Al-Eyadhy, A.; Alhaboob, A.; Temsah, M.-H. Incidence and characteristics of hepatitis E virus infection in children in Assiut, Upper Egypt. J. Int. Med. Res. 2016, 44, 1115–1122. [Google Scholar] [CrossRef] [PubMed]
- Bayhan, G.İ.; Demiören, K.; Güdücüoğlu, H. Epidemiology of hepatitis E virus in children in the province of Van, Turkey. Turk. Arch. Pediatrics 2016, 51, 148. [Google Scholar] [CrossRef] [PubMed]
- Nasrallah, G.K.; Al Absi, E.S.; Ghandour, R.; Ali, N.H.; Taleb, S.; Hedaya, L.; Ali, F.; Huwaidy, M.; Husseini, A. Seroprevalence of hepatitis E virus among blood donors in Qatar (2013–2016). Transfusion 2017, 57, 1801–1807. [Google Scholar] [CrossRef] [PubMed]
- Obaidat, M.M.; Roess, A.A. Seroprevalence and risk factors of Hepatitis E infection in Jordan’s population: First report. Int. J. Infect. Dis. 2018, 66, 121–125. [Google Scholar] [CrossRef]
- Farshadpour, F.; Taherkhani, R.; Ravanbod, M.R.; Eghbali, S.S.; Taherkhani, S.; Mahdavi, E. Prevalence, risk factors and molecular evaluation of hepatitis E virus infection among pregnant women resident in the northern shores of Persian Gulf, Iran. PLoS ONE 2018, 13, e0191090. [Google Scholar] [CrossRef]
- Parsa Nahad, M.; Bavi, A.; Zandi, M.; Nejati, M.; Rabie Rudsari, M.; Dehghani, M.A.; Kiani, H.; Ramezani, A.; Khosravi Seftejani, S.; Omidi, N. Seroprevalence of Hepatitis E Virus Infection among Patients with Acute Hepatitis Symptoms in Ahvaz, Iran. Int. J. Med. Lab. 2018, 5, 11–18. [Google Scholar]
- Dalvand, N.; Dalvand, A.; Sharifi, Z.; Hosseini, S.M. Prevalence of hepatitis E virus in thalassemia patients with hepatitis C in Tehran, Iran. Iran. J. Microbiol. 2019, 11, 535. [Google Scholar] [CrossRef]
- Behzadi, M.A.; Leyva-Grado, V.H.; Namayandeh, M.; Ziyaeyan, A.; Feyznezhad, R.; Dorzaban, H.; Jamalidoust, M.; Ziyaeyan, M. Seroprevalence of viral hepatitis A, B, C, D and E viruses in the Hormozgan province southern Iran. BMC Infect. Dis. 2019, 19, 1027. [Google Scholar] [CrossRef]
- Abdelmawla, D.; Moemen, D.; Darwish, A.; Mowafy, W. Hepatitis E virus prevalence in Egyptian children with transfusion-dependent thalassemia. Braz. J. Infect. Dis. 2019, 23, 40–44. [Google Scholar] [CrossRef]
- Ismail, M.B.; Al Kassaa, I.; El Safadi, D.; Al Omari, S.; Mallat, H.; Dabboussi, F.; Hamze, M. Prevalence of anti-hepatitis E virus IgG antibodies in sera from hemodialysis patients in Tripoli, Lebanon. PLoS ONE 2020, 15, e0233256. [Google Scholar] [CrossRef] [PubMed]
- Ahmed, A.M.A.; Temerk, H.A.; Galal, H.R.; Bazeed, S.E.S.; Sultan, S. The seropervelance of infectious hepatitis viruses (HBV, HCV and HEV) among blood donors and their correlation to risk factors in Qena governorate, Upper Egypt. Virusdisease 2020, 31, 292–298. [Google Scholar] [CrossRef] [PubMed]
- Ouji, M.; Taherkhani, R.; Farshadpour, F. High prevalence of hepatitis E among regular hemodialysis patients in South of Iran. Int. J. Artif. Organs 2021, 44, 658–663. [Google Scholar] [CrossRef] [PubMed]
- Sadeghi, F.; Golchob, Z.; Javadian, M.; Barary, M.; Sabbagh, P.; Ebrahimpour, S.; Bayani, M. Seroprevalence of hepatitis A and hepatitis E viruses among pregnant women in Northern Iran. Infect. Dis. Obstet. Gynecol. 2021, 2021, 5130586. [Google Scholar] [CrossRef] [PubMed]
- Al Dossary, R.A.; Alnafie, A.N.; Aljaroodi, S.A.; Rahman, J.U.; Hunasemarada, B.C.; Alkharsah, K.R. Prevalence of Hepatitis E Virus Infection Among Blood Donors in the Eastern Province of Saudi Arabia. J. Multidiscip. Healthc. 2021, 14, 2381. [Google Scholar] [CrossRef]
- Sayed, I.M.; El-Mokhtar, M.A.; Mahmoud, M.A.R.; Elkhawaga, A.A.; Gaber, S.; Seddek, N.H.; Abdel-Wahid, L.; Ashmawy, A.M.; Alkareemy, E.A.R. Clinical outcomes and prevalence of Hepatitis E Virus (HEV) among non-AC hepatitis patients in egypt. Infect. Drug Resist. 2021, 14, 59. [Google Scholar] [CrossRef]
- Al Absi, E.S.; Al-Sadeq, D.W.; Khalili, M.; Younes, N.; Al-Dewik, N.; Abdelghany, S.K.; Abouzid, S.S.; Al Thani, A.A.; Yassine, H.M.; Coyle, P.V. The prevalence of HEV among non-AC hepatitis in Qatar and efficiency of serological markers for the diagnosis of hepatitis E. BMC Gastroenterol. 2021, 21, 266. [Google Scholar] [CrossRef]
- Dumaidi, K.; Abudamous, A.M.; Abu-Helu, R.; Al-Jawabreh, H.; Dumaidi, Y.; Al-Jawabreh, A. First Report of the HEV Seroprevalence and the Risk Factor Assessment in the West Bank, Palestine, during the Period of 2015–2017. Can. J. Infect. Dis. Med. Microbiol. 2022, 2022, 4935811. [Google Scholar] [CrossRef]
- Öğüt, S.; Sayıner, A.A.; Otlu, B.; Bozdayı, G.; Zeytinoğlu, A.; Aksaray, S.; Çolak, D.; Gökahmetoğlu, S.; Aysın, M. Hepatitis E Infection in Solid Organ Transplant Recipients in Turkey. Turk. J. Gastroenterol. Off. J. Turk. Soc. Gastroenterol. 2022, 33, 68–73. [Google Scholar] [CrossRef]
- Farshadpour, F.; Taherkhani, S.; Taherkhani, R. Hepatitis E virus infection during pregnancy: The overlooked cause of maternal and fetal mortality. Infect. Disord. Drug Targets 2019, 19, 334–336. [Google Scholar] [CrossRef]
- Ahmad, T.; Hui, J.; Musa, T.H.; Behzadifar, M.; Baig, M. Seroprevalence of hepatitis E virus infection in pregnant women: A systematic review and meta-analysis. Ann. Saudi Med. 2020, 40, 136–146. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.-H.; Nelson, K.E.; Panzner, U.; Kasture, Y.; Labrique, A.B.; Wierzba, T.F. A systematic review of the epidemiology of hepatitis E virus in Africa. BMC Infect. Dis. 2014, 14, 308. [Google Scholar] [CrossRef] [PubMed]
- Hartl, J.; Otto, B.; Madden, R.G.; Webb, G.; Woolson, K.L.; Kriston, L.; Vettorazzi, E.; Lohse, A.W.; Dalton, H.R.; Pischke, S. Hepatitis E seroprevalence in Europe: A meta-analysis. Viruses 2016, 8, 211. [Google Scholar] [CrossRef] [PubMed]
- Tengan, F.M.; Figueiredo, G.M.; Nunes, A.K.; Manchiero, C.; Dantas, B.P.; Magri, M.C.; Prata, T.V.; Nascimento, M.; Mazza, C.C.; Abdala, E. Seroprevalence of hepatitis E in adults in Brazil: A systematic review and meta-analysis. Infect. Dis. Poverty 2019, 8, 3. [Google Scholar] [CrossRef]
- Petrović, T.; Lupulović, D.; de Oya, N.J.; Vojvodić, S.; Blázquez, A.-B.; Escribano-Romero, E.; Martín-Acebes, M.A.; Potkonjak, A.; Milošević, V.; Lazić, S. Prevalence of hepatitis E virus (HEV) antibodies in Serbian blood donors. J. Infect. Dev. Ctries. 2014, 8, 1322–1327. [Google Scholar] [CrossRef]
- Alvarado-Esquivel, C.; Sánchez-Anguiano, L.F.; Hernández-Tinoco, J. Hepatitis E virus exposure in pregnant women in rural Durango, Mexico. Ann. Hepatol. 2015, 13, 510–517. [Google Scholar] [CrossRef]
- Khaskheli, M.-N.; Baloch, S.; Sheeba, A.; Baloch, S. Hepatitis E–A preventable health issue–Endangering pregnant women’s life and foetal outcomes. J. Pak. Med. Assoc. 2015, 65, 655–659. [Google Scholar]
- Elduma, A.H.; Osman, W.M. Dengue and hepatitis E virus infection in pregnant women in Eastern Sudan, a challenge for diagnosis in an endemic area. Pan Afr. Med. J. 2014, 19, 391. [Google Scholar] [CrossRef]
- Stoszek, S.K.; Engle, R.E.; Abdel-Hamid, M.; Mikhail, N.; Abdel-Aziz, F.; Medhat, A.; Fix, A.D.; Emerson, S.U.; Purcell, R.H.; Strickland, G.T. Hepatitis E antibody seroconversion without disease in highly endemic rural Egyptian communities. Trans. R. Soc. Trop. Med. Hyg. 2006, 100, 89–94. [Google Scholar] [CrossRef]
- Shata, M.T.; Daef, E.A.; Zaki, M.E.; Abdelwahab, S.F.; Marzuuk, N.M.; Sobhy, M.; Rafaat, M.; Abdelbaki, L.; Nafeh, M.A.; Hashem, M. Protective role of humoral immune responses during an outbreak of hepatitis E in Egypt. Trans. R. Soc. Trop. Med. Hyg. 2012, 106, 613–618. [Google Scholar] [CrossRef]
- Hartl, J.; Wehmeyer, M.H.; Pischke, S. Acute hepatitis E: Two sides of the same coin. Viruses 2016, 8, 299. [Google Scholar] [CrossRef] [PubMed]
- Krain, L.J.; Atwell, J.E.; Nelson, K.E.; Labrique, A.B. Fetal and neonatal health consequences of vertically transmitted hepatitis E virus infection. Am. J. Trop. Med. Hyg. 2014, 90, 365. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. The PRISMA Group. Preferred Reporting Items for Systematic Reviews and Meta-Analyses: The PRISMA Statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [PubMed]
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).