
Emphysema Quantification Using Ultra-Low-Dose Chest CT: Efficacy of Deep Learning-Based Image Reconstruction

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Subjects
2.2. CT Data Acquisition and Reconstruction
2.3. Image Analysis
2.4. Statistical Analysis
3. Results
3.1. Radiation Dose
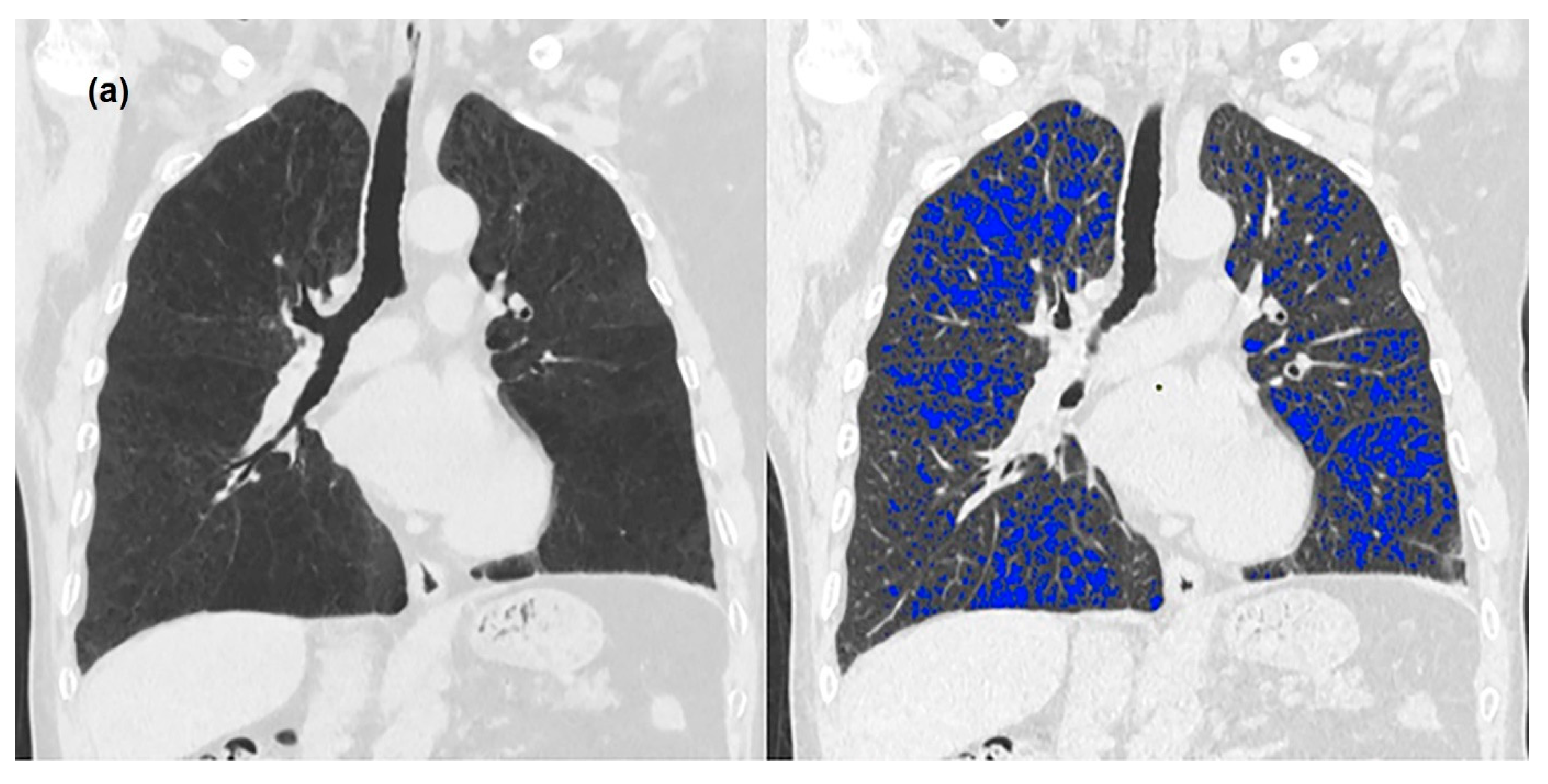
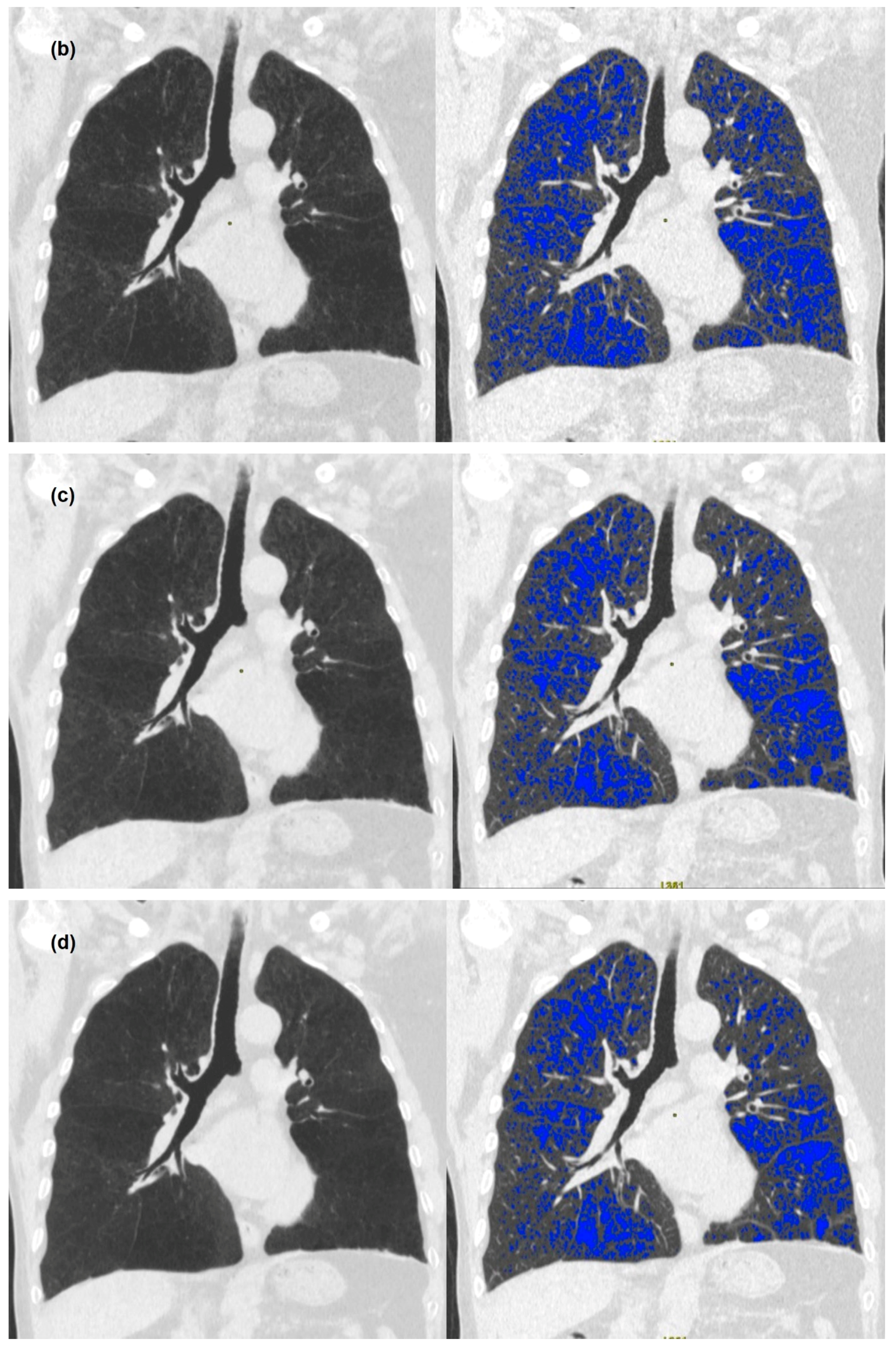
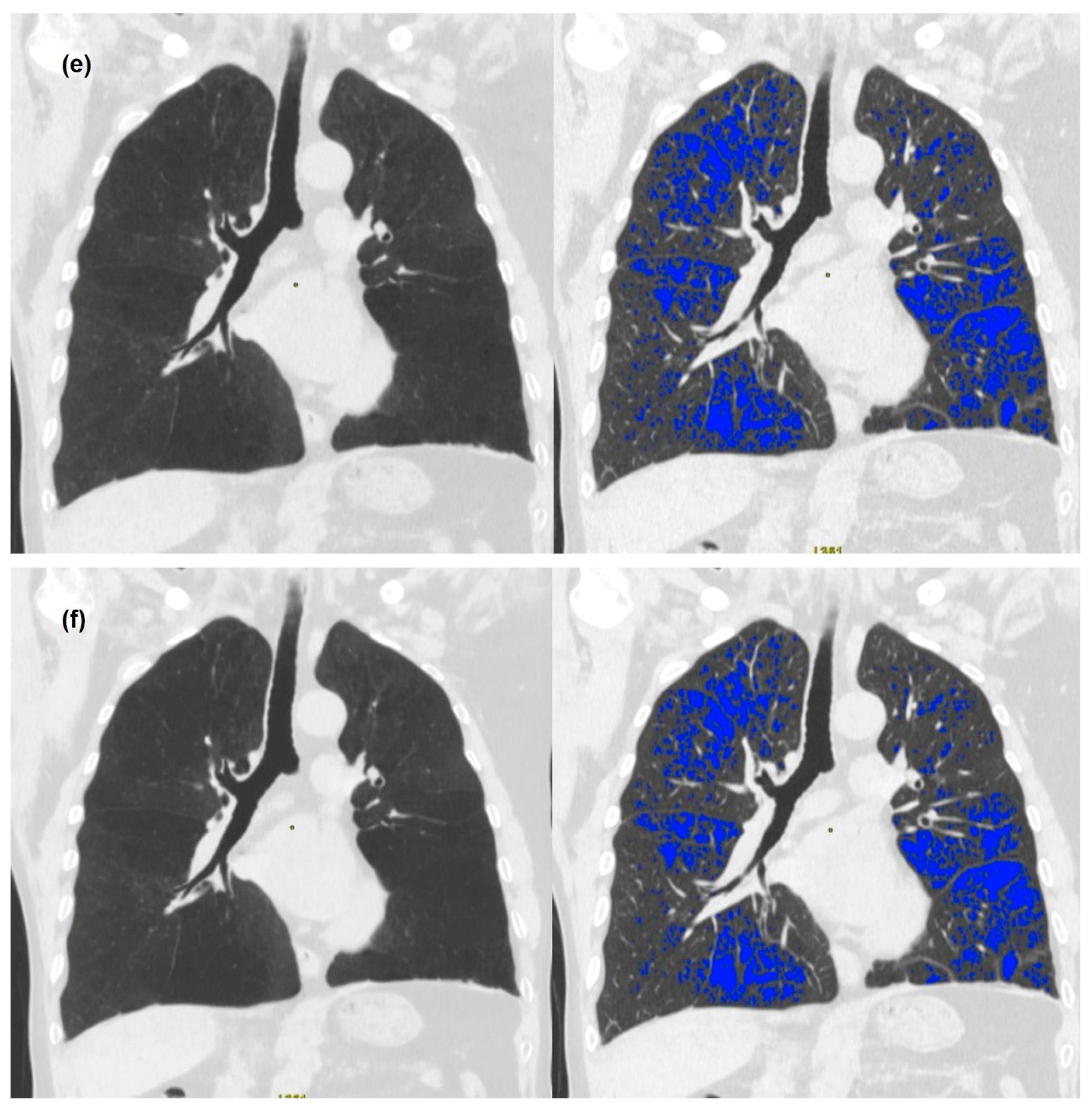
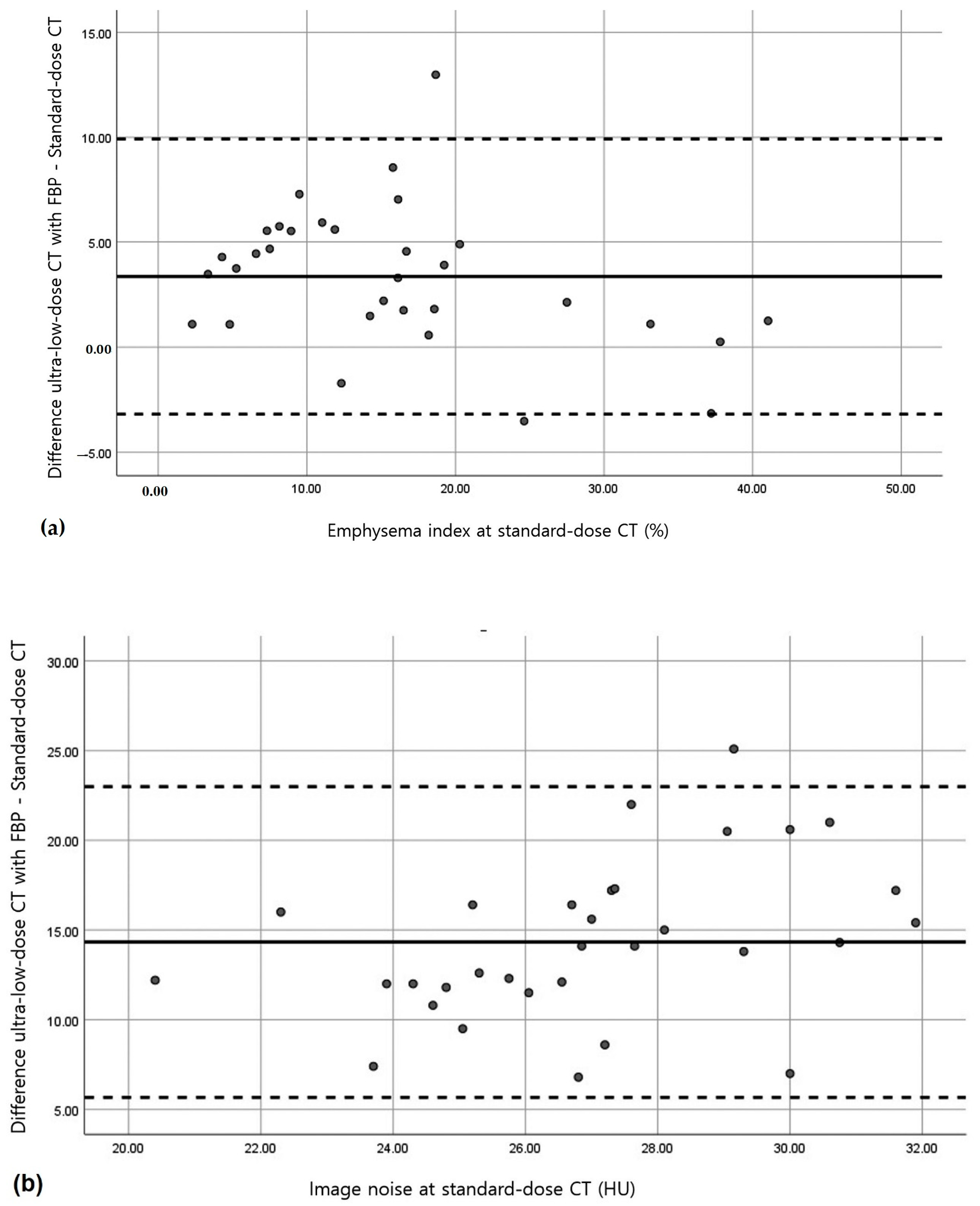
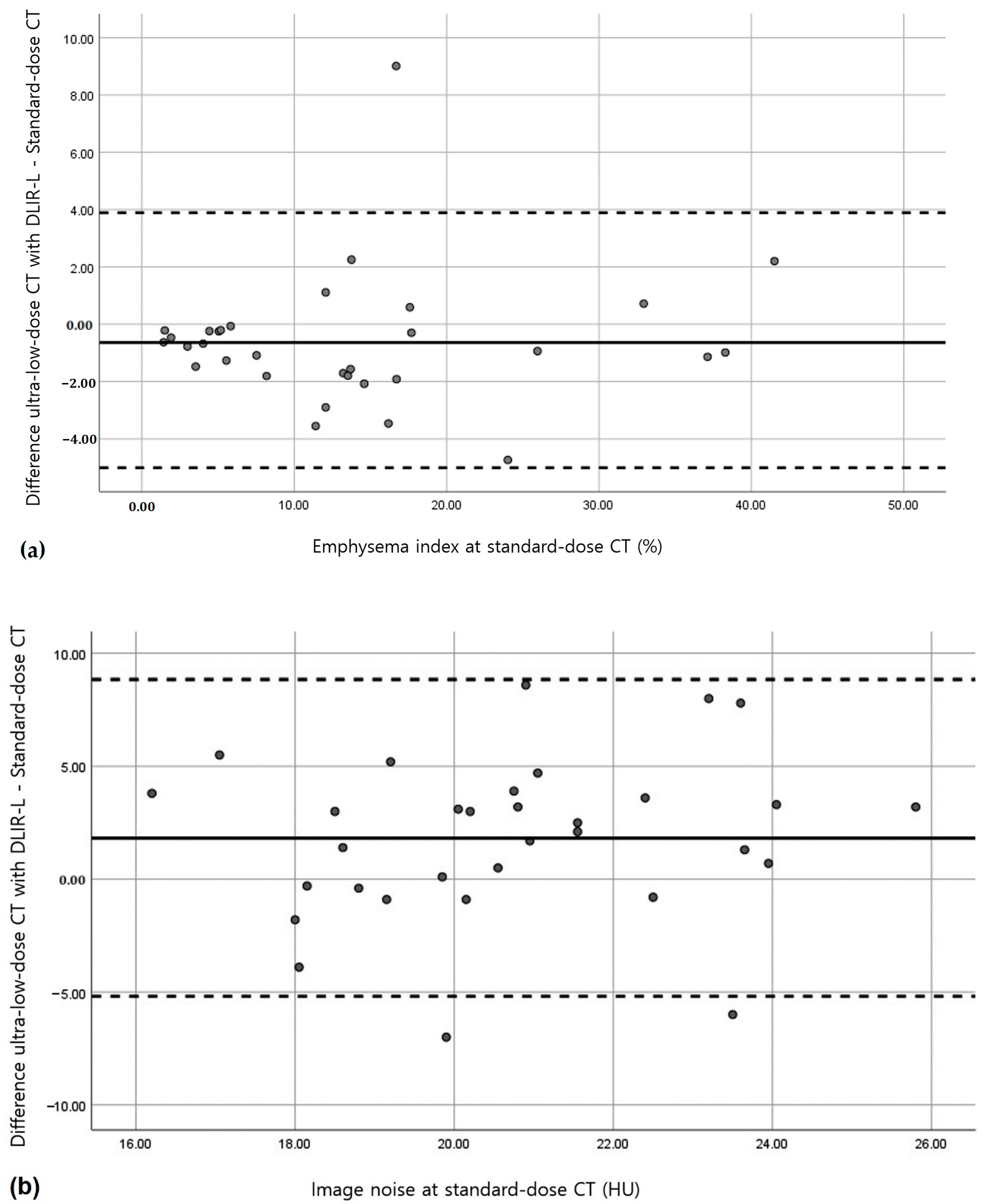
3.2. Quantitative Measurements of Standard-Dose and Ultra-Low-Dose CT
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Global Strategy for the Diagnosis, Management, and Prevention of Chronic Obstructive Pulmonary Disease. 2021 Report. Available online: https://goldcopd.org/wp-content/uploads/2020/11/GOLD-REPORT-2021-v1.1-25Nov20_WMV.pdf (accessed on 29 September 2021).
- Sanders, C.; Nath, P.H.; Bailey, W.C. Detection of emphysema with computed tomography. Correlation with pulmonary function tests and chest radiography. Investig. Radiol. 1988, 23, 262–266. [Google Scholar] [CrossRef]
- Madani, A.; Keyzer, C.; Gevenois, P.-A. Quantitative computed tomography assessment of lung structure and function in pulmonary emphysema. Eur. Respir. J. 2001, 18, 720–730. [Google Scholar] [CrossRef] [Green Version]
- Kinsella, M.; Müller, N.L.; Abboud, R.T.; Morrison, N.J.; DyBuncio, A. Quantitation of emphysema by computed tomography using a “density mask” program and correlation with pulmonary function tests. Chest 1990, 97, 315–321. [Google Scholar] [CrossRef] [Green Version]
- Watanuki, Y.; Suzuki, S.; Nishikawa, M.; Miyashita, A.; Okubo, T. Correlation of quantitative CT with selective alveolobronchogram and pulmonary function tests in emphysema. Chest 1994, 106, 806–813. [Google Scholar] [CrossRef]
- Gevenois, P.A.; de Vuyst, P.D.; de Maertelaer, V.; Zanen, J.; Jacobovitz, D.; Cosio, M.G.; Yernault, J.-C. Comparison of computed density and microscopic morphometry in pulmonary emphysema. Am. J. Respir. Crit. Care Med. 1996, 154, 187–192. [Google Scholar] [CrossRef]
- Bankier, A.A.; de Maertelaer, V.; Keyzer, C.; Gevenois, P.A. Pulmonary emphysema: Subjective visual grading versus objective quantification with macroscopic morphometry and thin-section CT densitometry. Radiology 1999, 211, 851–858. [Google Scholar] [CrossRef]
- Madani, A.; Zanen, J.; de Maertelaer, V.; Gevenois, P.A. Pulmonary emphysema: Objective quantification at multi—Detector row CT—Comparison with macroscopic and microscopic morphometry. Radiology 2006, 238, 1036–1043. [Google Scholar] [CrossRef]
- Ostridge, K.; Wilkinson, T.M. Present and future utility of computed tomography scanning in the assessment and management of COPD. Eur. Resiratory J. 2016, 48, 216–228. [Google Scholar] [CrossRef]
- Mascalchi, M.; Camiciottoli, G.; Diciotti, S. Lung densitometry: Why, how and when. J. Thorac. Dis. 2017, 9, 3319. [Google Scholar] [CrossRef] [Green Version]
- Yuan, R.; Mayo, J.R.; Hogg, J.C.; Pare, P.D.; McWilliams, A.M.; Lam, S.; Coxson, H.O. The effects of radiation dose and CT manufacturer on measurements of lung densitometry. Chest 2007, 132, 617–623. [Google Scholar] [CrossRef]
- Gierada, D.S.; Pilgram, T.K.; Whiting, B.R.; Hong, C.; Bierhals, A.J.; Kim, J.H.; Bae, K.T. Comparison of standard-and low-radiation-dose CT for quantification of emphysema. Am. J. Roentgenol. 2007, 188, 42–47. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.Y.; Chung, M.J.; Chin, A.Y.; Lee, K.S. Ultra-low-dose MDCT of the chest: Influence on automated lung nodule detection. Korean J. Radiol. 2008, 9, 95–101. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Akagi, M.; Nakamura, Y.; Higaki, T.; Narita, K.; Honda, Y.; Zhou, J.; Yu, Z.; Akino, N.; Awai, K. Deep learning reconstruction improves image quality of abdominal ultra-high-resolution CT. Eur. Radiol. 2019, 29, 6163–6171. [Google Scholar] [CrossRef] [PubMed]
- Hata, A.; Yanagawa, M.; Yoshida, Y.; Miyata, T.; Kikuchi, N.; Honda, O.; Tomiyama, N. The image quality of deep-learning image reconstruction of chest CT images on a mediastinal window setting. Clin. Radiol. 2021, 76, 155.e115–155.e123. [Google Scholar] [CrossRef]
- Nishio, M.; Matsumoto, S.; Ohno, Y.; Sugihara, N.; Inokawa, H.; Yoshikawa, T.; Sugimura, K. Emphysema quantification by low-dose CT: Potential impact of adaptive iterative dose reduction using 3D processing. Am. J. Roentgenol. 2012, 199, 595–601. [Google Scholar] [CrossRef]
- Wang, R.; Sui, X.; Schoepf, U.J.; Song, W.; Xue, H.; Jin, Z.; Schmidt, B.; Flohr, T.G.; Canstein, C.; Spearman, J.V. Ultralow-radiation-dose chest CT: Accuracy for lung densitometry and emphysema detection. Am. J. Roentgenol. 2015, 204, 743–749. [Google Scholar] [CrossRef]
- Nishio, M.; Koyama, H.; Ohno, Y.; Negi, N.; Seki, S.; Yoshikawa, T.; Sugimura, K. Emphysema quantification using ultralow-dose CT with iterative reconstruction and filtered back projection. Am. J. Roentgenol. 2016, 206, 1184–1192. [Google Scholar] [CrossRef]
- Messerli, M.; Ottilinger, T.; Warschkow, R.; Leschka, S.; Alkadhi, H.; Wildermuth, S.; Bauer, R.W. Emphysema quantification and lung volumetry in chest X-ray equivalent ultralow dose CT—Intra-individual comparison with standard dose CT. Eur. J. Radiol. 2017, 91, 1–9. [Google Scholar] [CrossRef]
- Wisselink, H.; Pelgrim, G.; Rook, M.; Imkamp, K.; van Ooijen, P.; van den Berge, M.; de Bock, G.; Vliegenthart, R. Ultra-low-dose CT combined with noise reduction techniques for quantification of emphysema in COPD patients: An intra-individual comparison study with standard-dose CT. Eur. J. Radiol. 2021, 138, 109646. [Google Scholar] [CrossRef]
- Choo, J.Y.; Goo, J.M.; Lee, C.H.; Park, C.M.; Park, S.J.; Shim, M.-S. Quantitative analysis of emphysema and airway measurements according to iterative reconstruction algorithms: Comparison of filtered back projection, adaptive statistical iterative reconstruction and model-based iterative reconstruction. Eur. Radiol. 2014, 24, 799–806. [Google Scholar] [CrossRef]
- Choi, H.; Kim, H.; Jin, K.N.; Jeong, Y.J.; Chae, K.J.; Lee, K.H.; Yong, H.S.; Gil, B.; Lee, H.-J.; Lee, K.Y.; et al. A challenge for emphysema quantification using a deep learning algorithm with low-dose chest computed tomography. J. Thorac. Imaging 2022, 37, 253–261. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Value | Standard-Dose CT | Ultra-Low-Dose CT | |||||
|---|---|---|---|---|---|---|---|
| FBP | FBP | ASIR-V 50 | DLIR-L | DLIR-M | DLIR-H | p | |
| EI, % | 14.26 (11.02) | 17.62 (9.77) | 14.81 (10.86) | 13.62 (11.23) | 12.29 (11.53) | 11.76 (11.74) | <0.001 |
| TLV, L | 5.46 (1.09) | 5.55 (1.13) | 5.57 (1.16) | 5.57 (1.16) | 5.57 (1.16) | 5.57 (1.16) | 0.150 |
| MLA, HU | −851.05 (24.44) | −849.41 (27.57) | −850.85 (27.67) | −851.25 (27.98) | −851.24 (27.88) | −850.58 (27.65) | 0.380 |
| Image noise, HU | 19.80 (2.68) | 34.13 (4.12) | 25.38 (3.38) | 21.62 (3.10) | 16.27 (2.17) | 10.47 (2.49) | <0.001 |
| Value | Standard-Dose CT | Ultra-Low-Dose CT | |||||
|---|---|---|---|---|---|---|---|
| FBP | FBP | ASIR-V 50 | DLIR-L | DLIR-M | DLIR-H | p | |
| EI | 1 | 0.955 | 0.977 | 0.979 | 0.981 | 0.978 | <0.001 |
| TLV | 1 | 0.925 | 0.933 | 0.932 | 0.933 | 0.934 | <0.001 |
| MLA | 1 | 0.924 | 0.926 | 0.925 | 0.927 | 0.926 | <0.001 |
| Image noise | 1 | 0.210 | 0.227 | 0.239 | 0.346 | 0.406 | >0.05 * |
| Value | Ultra-Low-Dose CT | ||||
|---|---|---|---|---|---|
| FBP | ASIR-V 50 | DLIR-L | DLIR-M | DLIR-H | |
| Emphysema index | 3.36 (3.35) | 0.55 (2.33) * | −0.64 (2.31) * | −1.97 (2.24) | −2.50 (2.48) |
| Total lung volume | 0.09 (0.43) * | 0.11 (0.42) * | 0.11 (0.42) * | 0.12 (0.42) * | 0.11 (0.41) * |
| Mean lung attenuation | 1.65 (10.59) * | 0.20 (10.49) * | −0.19 (10.74) * | −0.19 (10.55) * | 0.48 (10.53) * |
| Image noise | 14.33 (4.42) | 5.58 (3.81) * | 1.82 (3.58) * | −3.53 (2.80) * | −9.33 (2.82) * |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yeom, J.-A.; Kim, K.-U.; Hwang, M.; Lee, J.-W.; Kim, K.-I.; Song, Y.-S.; Lee, I.-S.; Jeong, Y.-J. Emphysema Quantification Using Ultra-Low-Dose Chest CT: Efficacy of Deep Learning-Based Image Reconstruction. Medicina 2022, 58, 939. https://doi.org/10.3390/medicina58070939
Yeom J-A, Kim K-U, Hwang M, Lee J-W, Kim K-I, Song Y-S, Lee I-S, Jeong Y-J. Emphysema Quantification Using Ultra-Low-Dose Chest CT: Efficacy of Deep Learning-Based Image Reconstruction. Medicina. 2022; 58(7):939. https://doi.org/10.3390/medicina58070939
Chicago/Turabian StyleYeom, Jeong-A, Ki-Uk Kim, Minhee Hwang, Ji-Won Lee, Kun-Il Kim, You-Seon Song, In-Sook Lee, and Yeon-Joo Jeong. 2022. "Emphysema Quantification Using Ultra-Low-Dose Chest CT: Efficacy of Deep Learning-Based Image Reconstruction" Medicina 58, no. 7: 939. https://doi.org/10.3390/medicina58070939