

Radiographic Evaluation of the Gap between Cemented Post and Remaining Gutta-Percha in Endodontically Treated Teeth Performed by Undergraduate Students: A Retrospective Cross-Sectional Study

 , ,
, ,  , , and
, , and 
Abstract
:1. Introduction
2. Materials and Methods
- Only patients treated for root canal treatment and post and core by the undergraduate students.
- Only patient records containing digital periapical radiographs taken immediately after the post and core treatment present.
- Patients treated by the specialists.
- Cases in which there were additional factors that could influence the outcome of the root-canal treatment, such as broken instruments in the root canal, over- or under-extension of the root canal filling, or root fracture, were excluded.
- Group I: no gap between the cemented post and the gutta-percha.
- Group II: a gap of more than 0 but less than 2 mm between the gutta-percha and the post.
- Group III: a gap of more than 2 mm between the gutta-percha and the post.
- Group IV: less than 3 mm of gutta-percha remaining.
- Group V: 3 to 5 mm of gutta-percha remaining.
- Group IV: more than 5 mm of gutta-percha remaining.
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Sjogren, U.; Hagglund, B.; Sundqvist, G.; Wing, K. Factors affecting the long-term results of endodontic treatment. J. Endod. 1990, 16, 498–504. [Google Scholar] [CrossRef] [PubMed]
- Friedman, S.; Abitbol, S.; Lawrence, H.P. Treatment outcome in endodontics. The Toronto study. Phase I: Initial treatment. J. Endod. 2003, 29, 787–793. [Google Scholar] [CrossRef] [PubMed]
- Ray, H.A.; Trope, M. Periapical status of endodontically treated teeth in relation to the technical quality of the root filling and the coronal restoration. Int. Endod. J. 1995, 28, 12–18. [Google Scholar] [CrossRef] [PubMed]
- Fernandes, A.S.; Dessai, G.S. Factors affecting the fracture resistance of post-core reconstructed teeth: A review. Int. J. Prosthodont. 2001, 14, 355–363. [Google Scholar]
- Alves, J.; Walton, R.; Drake, D. Coronal leakage: Endotoxin penetration from mixed bacterial communities through obturated, post-prepared root canals. J. Endod. 1998, 24, 587–591. [Google Scholar] [CrossRef]
- Heling, I.; Gorfil, C.; Slutzky, H.; Kopolovic, K.; Zalkind, M.; Slutzky-Goldberg, I. Endodontic failure caused by inadequate restorative procedures: Review and treatment recommendations. Prosthet. Dent. 2002, 87, 674–678. [Google Scholar] [CrossRef]
- Haddix, J.E.; Mattison, G.D.; Shulman, C.A.; Pink, F.E. Post preparation techniques and their effect on the apical seal. J. Prosthet. Dent. 1990, 64, 515–519. [Google Scholar] [CrossRef]
- Karapanou, V.; Vera, J.; Cabrera, P.; White, R.R.; Goldman, M. Effect of immediate and delayed post preparation on apical dye leakage using two different sealers. J. Endod. 1996, 22, 583–585. [Google Scholar] [CrossRef]
- Hiltner, R.S.; Kulild, J.C.; Weller, R.N. Effect of mechanical versus thermal removal of gutta-percha on the quality of the apical seal following post space preparation. J. Endod. 1992, 18, 451–454. [Google Scholar] [CrossRef]
- Abramovitz, I.; Tagger, M.; Tamse, A.; Metzger, Z. The effect of immediate vs. delayed post space preparation on the apical seal of a root canal filling: A study in an increased sensitivity pressure-driven system. J. Endod. 2000, 26, 435–439. [Google Scholar] [CrossRef] [Green Version]
- Fan, B.; Wu, M.K.; Wesselink, P.R. Coronal leakage along apical rootfillings after immediate and delayed post space preparation. Endod. Dent. Traumatol. 1999, 15, 124–126. [Google Scholar] [CrossRef]
- Bachicha, W.S.; Di Fiore, P.M.; Miller, D.A.; Lautenschlager, E.P.; Pashley, D.H. Microleakage of endodontically treated teeth restored with posts. J. Endod. 1998, 24, 703–708. [Google Scholar] [CrossRef]
- Fox, K.; Gutteridge, D.L. An in vitro study of coronal microleakage in root-canal treated teeth restored by the post and core technique. Int. Endod. J. 1997, 30, 361–368. [Google Scholar] [CrossRef]
- Joshua, M.; Iris, S.G.; Ayelet, G.; Benny, P. The Effect of the Distance between Post and Residual Gutta-Percha on the Clinical Outcome of Endodontic Treatment. J. Endod. 2005, 31, 177–179. [Google Scholar]
- Baruah, K.; Mirdha, N.; Gill, B.; Bishnoi, N.; Gupta, T.; Baruah, Q. Comparative Study of the Effect on Apical Sealability with Different Levels of Remaining Gutta-Percha in Teeth Prepared to Receive Posts: An in vitro Study. Contemp Clin Dent. 2018, 9 (Suppl. 2), S261–S265. [Google Scholar]
- Reyhani, M.F.; Yavari, H.; Ghasemi, N.; Rahimi, S.; Barhaghi, M.H.; Mokhtari, H.; Sarikhani, P. Comparing the Coronal Seal of Different Thicknesses of MTA with Gutta-Percha after Post Space Preparation. Sci. World J. 2015, 2015, 708639. [Google Scholar]
- Hommez, G.M.; Coppens, C.R.; De Moor, R.J. Periapical health related to the quality of coronal restorations and root fillings. Int. Endod. J. 2002, 35, 680–689. [Google Scholar] [CrossRef] [Green Version]
- Iqbal, M.K.; Johansson, A.A.; Akeel, R.F.; Bergenholtz, A.; Omar, R. A rretrospective analysis of factors associated with the periapical status of restored, endodontically treated teeth. Int. J. Prosthodont. 2003, 16, 31–38. [Google Scholar]
- Goodacre, C.J.; Spolnik, K.J. The prosthodontic management of endodontically treated teeth: A literature review. Part III. Tooth preparation considerations. J. Prosthodont. 1995, 4, 122–128. [Google Scholar] [CrossRef]
- Sorensen, J.A.; Martinoff, J.T. Clinically significant factors in dowel design. J. Prosthet. Dent. 1984, 52, 28–35. [Google Scholar] [CrossRef]
- Neagley, R.L. The effect of dowel preparation on apical seal of end- odontically treated teeth. Oral. Surg. Oral. Med. Oral. Pathol. 1969, 28, 739–745. [Google Scholar] [CrossRef] [PubMed]
- Mattison, G.D.; Delivanis, P.D.; Thacker, R.W.; Hassel, K.J. Effect of post preparation on the apical seal. J. Prosthet. Dent. 1984, 51, 785–789. [Google Scholar] [CrossRef] [PubMed]
- Goodacre, C.J.; Spolnik, K.J. The prosthodontic management of endodontically treated teeth: A literature review. Part II. Maintaining the apical seal. J. Prosthodont. 1995, 4, 51–53. [Google Scholar] [CrossRef] [PubMed]
- Madison, S.; Zakariasen, K.L. Linear and volumetric analysis of apical leakage in teeth prepared for posts. J. Endod. 1984, 10, 422–427. [Google Scholar] [CrossRef] [PubMed]
- Abramovitz, L.; Lev, R.; Fuss, Z.; Metzger, Z. The unpredictability of seal after post space preparation: A fluid transport study. J. Endod. 2001, 27, 292–295. [Google Scholar] [CrossRef]
- Swanson, K.; Madison, S. An evaluation of coronal microleakage in endodontically treated teeth. Part 1. Time periods. J. Endod. 1987, 13, 56–59. [Google Scholar] [CrossRef]
- Magura, M.E.; Kafrawy, A.H.; Brown, C.E.; Newton, C.W. Human saliva coronal microleakage in obturated root canals: An in vitro study. J. Endod. 1991, 17, 324–331. [Google Scholar] [CrossRef]
- Ozkurt, Z.; Mehmet, B.K.; Hakki, S.; Ender, K.; Gündüz, B. The effect of the gap between the post restoration and the remaining root canal filling on the periradicular status in a Turkish subpopulation. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 2010, 110, 131–135. [Google Scholar] [CrossRef]
- Kvist, T.; Rydin, E.; Reit, C. The relative frequency of periapical lesions in teeth with root canal-retained posts. J. Endod. 1989, 15, 578–580. [Google Scholar] [CrossRef]
- De Cleen, M.J. The relationship between the root canal filling and post space preparation. Int. Endod. J. 1993, 26, 53–58. [Google Scholar] [CrossRef]
- Chugal, N.M.; Clive, J.M.; Spångberg, L.S. A prognostic model for assessment of the outcome of endodontic treatment: Effect of biologic and diagnostic variables. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 2001, 91, 342–352. [Google Scholar] [CrossRef]
- Haralur, S.B.; Al-Malki, A.E. Student perception about efficacy of preclinical fixed prosthodontic training to facilitate smooth transition to clinical context. J. Educ. Health Promot. 2014, 3, 73. [Google Scholar]
- Velayo, B.C.; Stark, P.C.; Eisen, S.E.; Kugel, G. Using dental students’ preclinical performance as an indicator of clinical success. J. Dent. Educ. 2014, 78, 823–828. [Google Scholar] [CrossRef]
- Jacobs, R.; Salmon, B.; Codari, M.; Hassan, B.; Bornstein, M.M. Cone beam computed tomography in implant dentistry: Recommendations for clinical use. BMC Oral Health 2018, 18, 88. [Google Scholar] [CrossRef] [Green Version]
- Pauwels, R.; Zhang, G.; Theodorakou, C.; Walker, A.; Bosmans, H.; Jacobs, R.; Bogaerts, R.; Horner, K.; The SEDENTEXCT Project Consortium. Effective radiation dose and eye lens dose in dental cone beam CT: Effect of field of view and angle of rotation. Br. J. Radiol. 2014, 87, 20130654. [Google Scholar] [CrossRef] [Green Version]
- Menezes, R.F.; Araújo, N.C.; Santa Rosa, J.M.; Carneiro, V.S.; Santos Neto, A.P.; Costa, V.; Moreno, L.M.; Miranda, J.M.; de Albuquerque, D.S.; Albuquerque, M.; et al. Detection of vertical root fractures in endodontically treated teeth in the absence and in the presence of metal post by cone-beam computed tomography. BMC Oral Health 2016, 16, 48. [Google Scholar] [CrossRef] [Green Version]
- Patel, S.; Brady, E.; Wilson, R.; Brown, J.; Mannocci, F. The detection of vertical root fractures in root filled teeth with periapical radiographs and CBCT scans. Int. Endod. J. 2013, 46, 1140–1152. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
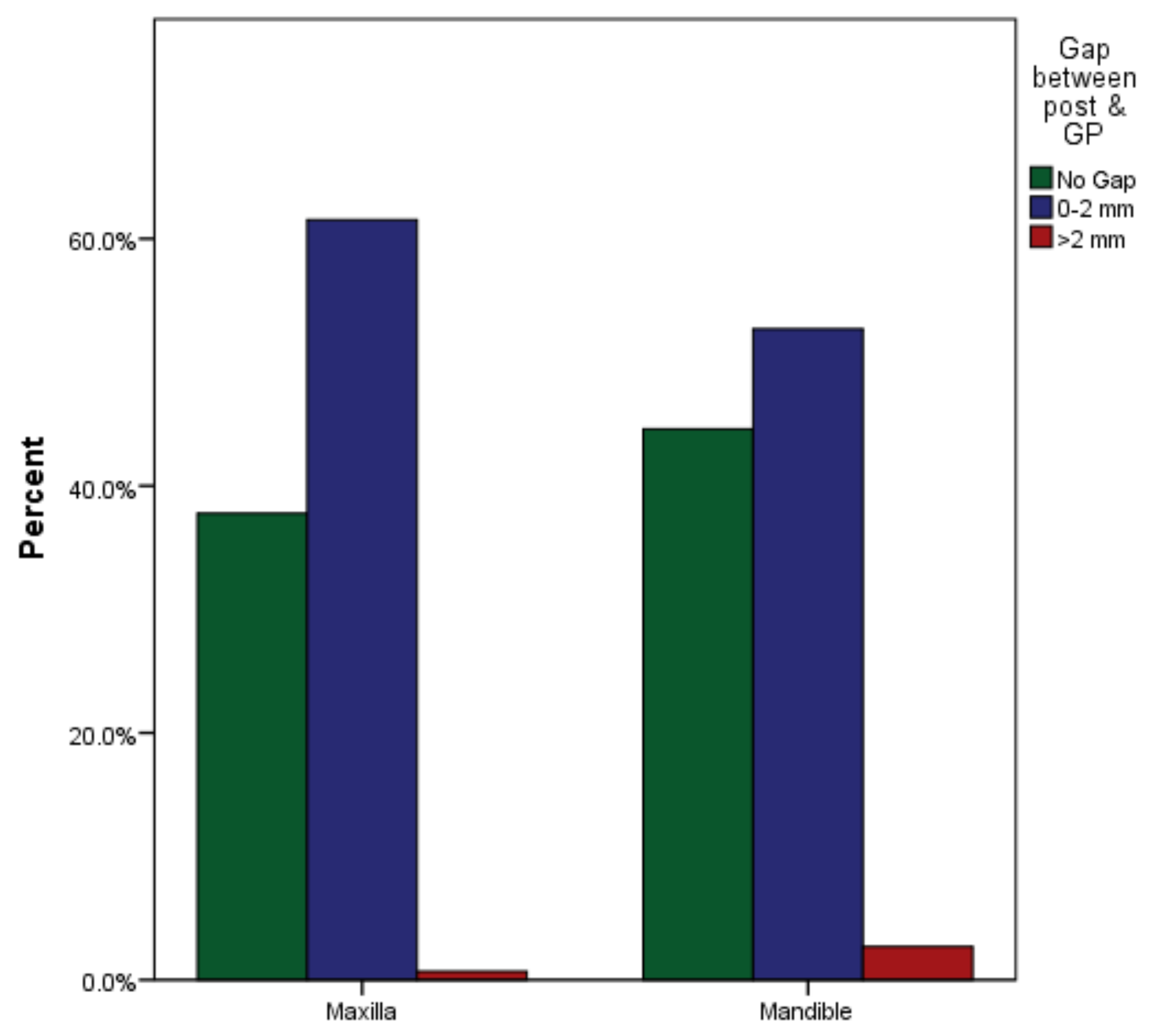
| Arch | Gap between Post & Remaining Gutta-Percha | Total | p Value | ||
|---|---|---|---|---|---|
| No Gap | >0 to 2 mm | >2 mm | |||
| Maxilla | 54 (38%) | 88 (62%) | 1 (0.7%) | 143 (100%) | 0.268 |
| Mandible | 33 (45%) | 39 (53%) | 2 (2.7%) | 74 (100%) | |
| Total | 87 (40%) | 127 (59%) | 3 (1.4%) | 217 (100%) | |
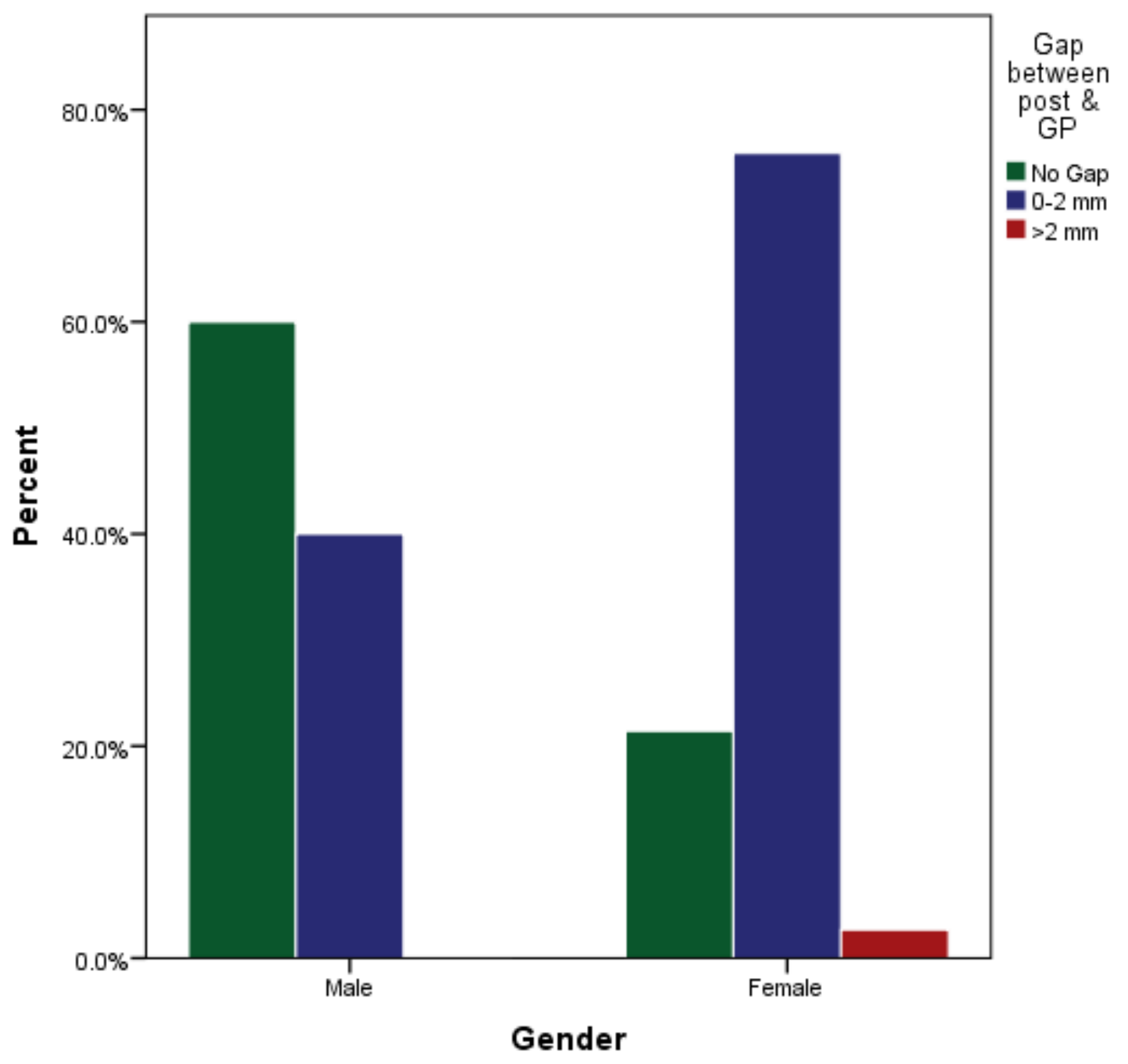
| Gender | Gap between Post & Remaining Gutta-Percha | Total | p Value | ||
|---|---|---|---|---|---|
| No Gap | >0 to 2 mm | >2 mm | |||
| Male | 63 (60%) | 42 (40%) | 0 (0%) | 105 (100%) | p < 0.001 |
| Female | 24 (21%) | 85 (76%) | 3 (3%) | 112 (100%) | |
| Total | 87 (40%) | 127 (59%) | 3 (1%) | 217 (100%) | |
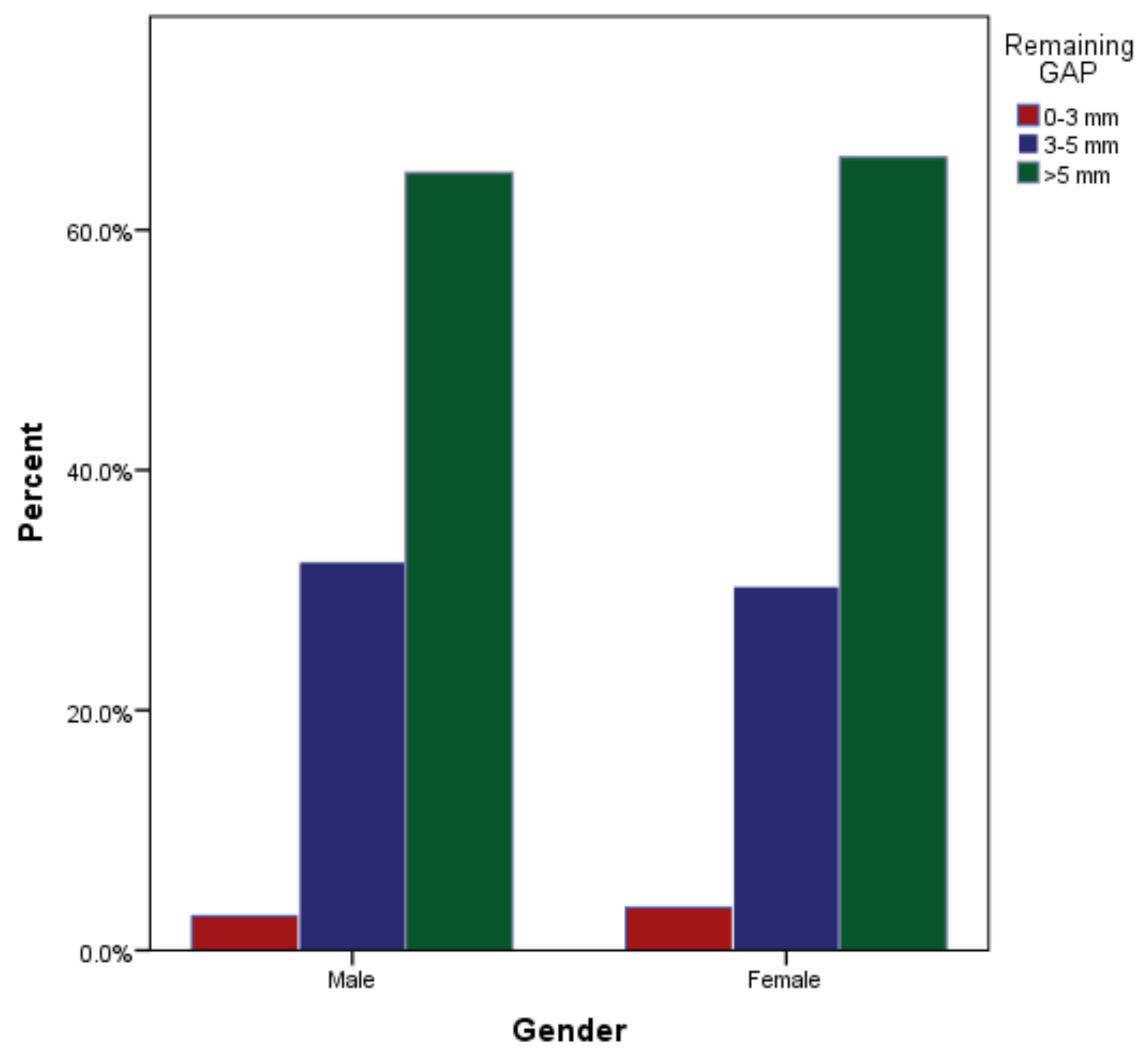
| Gender | Remaining Gutta-Percha after Post Cementation | Total | p Value | ||
|---|---|---|---|---|---|
| 0–3 mm | 3–5 mm | >5 mm | |||
| Male | 3 (3%) | 34 (32%) | 68 (65%) | 105 (100%) | 0.918 |
| Female | 4 (4%) | 34 (30%) | 74 (66%) | 112 (100%) | |
| Total | 7 (3%) | 68 (31%) | 142 (65%) | 217 (100%) | |
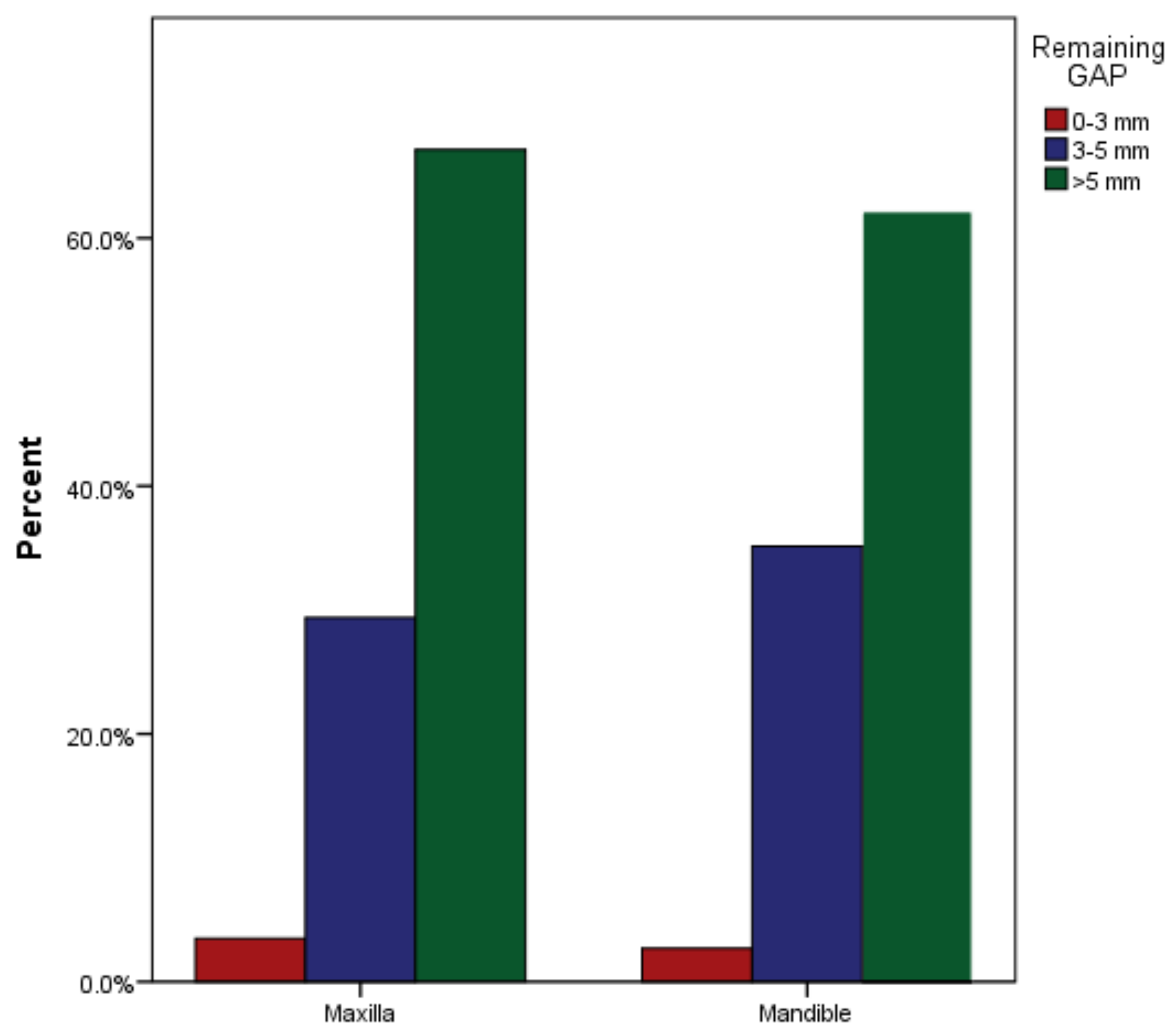
| Arch | Remaining Gutta-Percha after Post Cementation | Total | p Value | ||
|---|---|---|---|---|---|
| 0–3 mm | 3–5 mm | >5 mm | |||
| Maxilla | 5 (4%) | 42 (29%) | 96 (67%) | 143 (100%) | 0.671 |
| Mandible | 2 (3%) | 26 (35%) | 46 (62%) | 74 (100%) | |
| Total | 7 (3%) | 68 (31%) | 142 (65%) | 217 (100%) | |
| Arch | Gap between Post & Remaining Gutta-Percha | Total | p Value | ||
|---|---|---|---|---|---|
| No Gap | >0 to 2 mm | >2 mm | |||
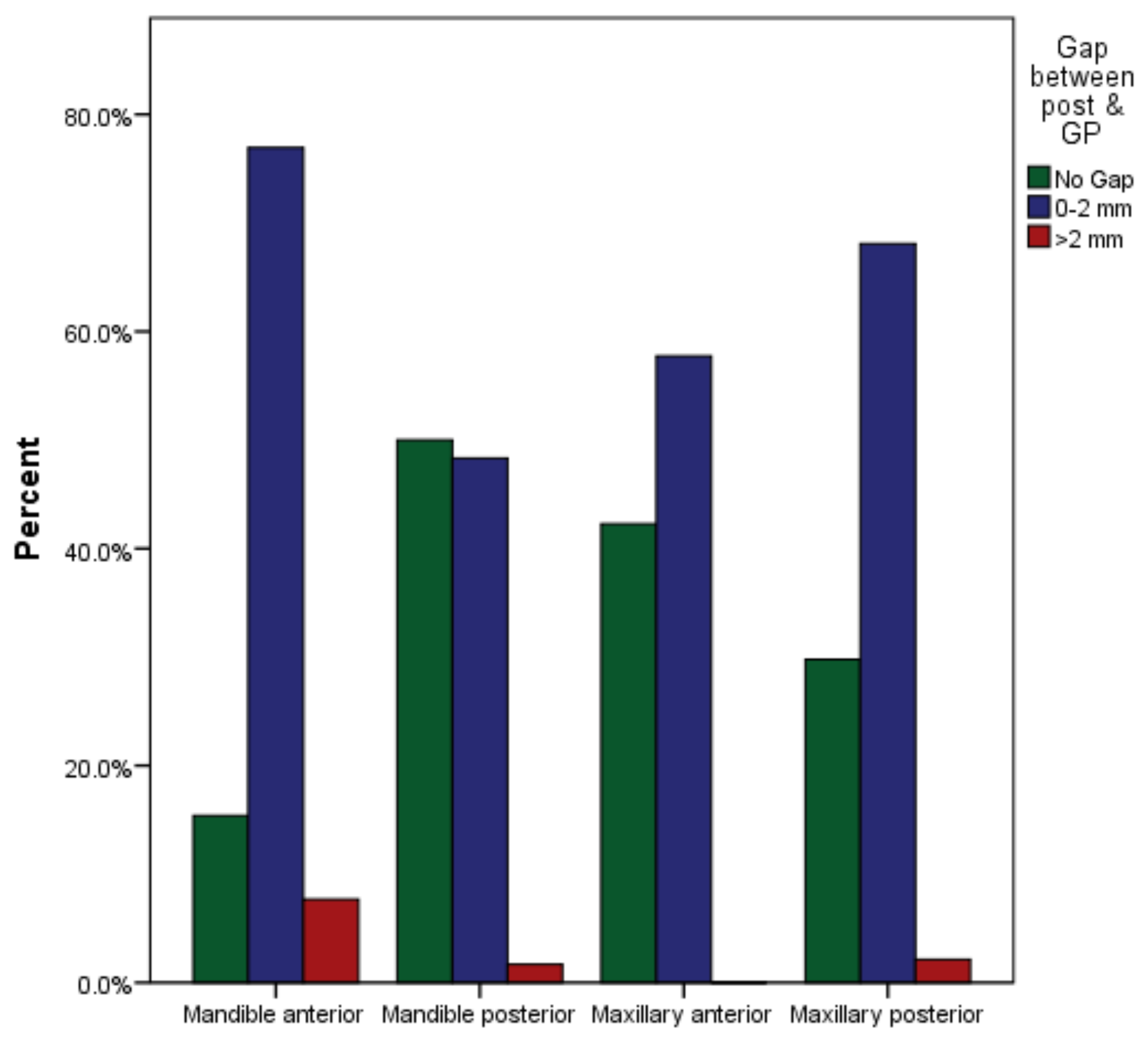
| Maxillary anterior | 41 (42%) | 56 (58%) | 0 (0%) | 97 (100%) | 0.048 |
| Maxillary posterior | 14 (30%) | 32 (68%) | 1 (2%) | 47 (100%) | |
| Mandibular anterior | 2 (15%) | 10 (77%) | 1 (8%) | 13 (100%) | |
| Mandibular posterior | 30 (50%) | 29 (48%) | 1 (2%) | 60 (100%) | |
| Total | 87 (40%) | 127 (59%) | 3 (1.4%) | 217 (100%) | |
| Arch | Remaining Gutta-Percha after Post Cementation | Total | p Value | ||
|---|---|---|---|---|---|
| 0–3 mm | 3–5 mm | >5 mm | |||
| Maxillary anterior | 3 (3%) | 23 (24%) | 71 (73%) | 97 (100%) | 0.151 |
| Maxillary posterior | 2 (4%) | 20 (43%) | 25 (53%) | 47 (100%) | |
| Mandibular anterior | 0 (0%) | 2 (15%) | 11 (85%) | 13 (100%) | |
| Mandibular posterior | 2 (3%) | 23 (38%) | 35 (58%) | 60 (100%) | |
| Total | 7 (3%) | 68 (31%) | 142 (65%) | 217 (100%) | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Naim, H.; Ahmad, M.; Ageeli, A.A.; Abuarab, R.K.; Sayed, M.E.; Dewan, H.; Chohan, H.; Alshehri, A.H.; Wadei, M.H.D.A.; Alqahtani, S.M.; et al. Radiographic Evaluation of the Gap between Cemented Post and Remaining Gutta-Percha in Endodontically Treated Teeth Performed by Undergraduate Students: A Retrospective Cross-Sectional Study. Medicina 2023, 59, 502. https://doi.org/10.3390/medicina59030502
Naim H, Ahmad M, Ageeli AA, Abuarab RK, Sayed ME, Dewan H, Chohan H, Alshehri AH, Wadei MHDA, Alqahtani SM, et al. Radiographic Evaluation of the Gap between Cemented Post and Remaining Gutta-Percha in Endodontically Treated Teeth Performed by Undergraduate Students: A Retrospective Cross-Sectional Study. Medicina. 2023; 59(3):502. https://doi.org/10.3390/medicina59030502
Chicago/Turabian StyleNaim, Hina, Manawar Ahmad, Abrar A. Ageeli, Raghad K. Abuarab, Mohammed E. Sayed, Harisha Dewan, Hitesh Chohan, Abdullah Hasan Alshehri, Mohammed Hussain Dafer Al Wadei, Saeed M. Alqahtani, and et al. 2023. "Radiographic Evaluation of the Gap between Cemented Post and Remaining Gutta-Percha in Endodontically Treated Teeth Performed by Undergraduate Students: A Retrospective Cross-Sectional Study" Medicina 59, no. 3: 502. https://doi.org/10.3390/medicina59030502