Abstract
Background and Objectives: The aim of this study was to assess the differences in Doppler indices of the uterine (Ut), umbilical (UA), and middle cerebral artery (MCA) in diabetic versus non-diabetic pregnancies by conducting a comprehensive systematic review of the literature with a meta-analysis. Materials and Methods: PubMed, Web of Science, and SCOPUS were searched for studies that measured the pulsatility index (PI), resistance index (RI), and systolic/diastolic ratio index (S/D ratio) of the umbilical artery, middle cerebral artery, and uterine artery in diabetic versus non-diabetic pregnancies. Two reviewers independently evaluated the eligibility of studies, abstracted data, and performed quality assessments according to standardized protocols. The standardized mean difference (SMD) was used as a measure of effect size. Heterogeneity was assessed using the I2 statistic. Publication bias was evaluated by means of funnel plots. Results: A total of 62 publications were included in the qualitative and 43 in quantitative analysis. The UA-RI, UtA-PI, and UtA-S/D ratios were increased in diabetic compared with non-diabetic pregnancies. Subgroup analysis showed that levels of UtA-PI were significantly higher during the third, but not during the first trimester of pregnancy in diabetic versus non-diabetic pregnancies. No differences were found for the UA-PI, UA-S/D ratio, MCA-PI, MCA-RI, MCA-S/D ratio, or UtA-RI between diabetic and non-diabetic pregnancies. Conclusions: This meta-analysis revealed the presence of hemodynamic changes in uterine and umbilical arteries, but not in the middle cerebral artery in pregnancies complicated by diabetes.
1. Introduction
Pre-gestational (DM) and gestational diabetes mellitus (GDM) are associated with increased risk of adverse perinatal outcomes [1,2]. Maternal hyperglycemia provokes in utero adaptation by fetal hyperinsulinemia, which causes increased nutrient storage, and in turn the development of fetal macrosomia. Fetal macrosomia complicates delivery and might put mother and baby at risk of birth injuries [3]. In a large meta-analysis including 7.5 million pregnancies, GDM was significantly associated with a range of adverse pregnancy outcomes [4]. Women with GDM and no insulin use have increased odds of caesarean section, preterm delivery, macrosomia, infant born large for gestational age and low Apgar score, while for women with GDM using insulin, the odds of having an infant requiring admission to the neonatal intensive care unit, who is large for gestational age, with respiratory distress syndrome, and/or neonatal jaundice were higher than in those without GDM [4]. It is currently common practice to consider earlier labor inductions based on glycemia status in order to reduce this risk of adverse outcomes in pregnancies complicated by GDM [5,6]. It was also shown that a correct pregnancy diet and maternal weight gain could modify the hyperglycemia status and reduce the risk of GDM and its complications [7] and that even moderate changes in pre-pregnancy weight can apparently affect the risk of GDM among obese women [8].
Since hyperglycemia starts its effect during organogenesis, this condition is also known as diabetic embryopathy [9]. It affects the cardiovascular, central nervous, gastrointestinal, genitourinary, and musculoskeletal system, and 6–12% of fetuses with diabetic embryopathy would have congenital problems of this kind [10]. Diabetic embryopathy is also known to be associated with a higher rate of miscarriages [11]. Hyperglycemia creates anaerobic in utero setting, leading to hypoxia and acidosis, which could result in a stillbirth [12]. Complications reported from newborns delivered from diabetic pregnancies are neonatal hypoglycemia, hyperbilirubinemia, hypocalcemia, polycythemia, respiratory distress syndrome [13], as well as increased risk for obesity, diabetes, and hypertension in developing years [14].
During a physiological pregnancy, spiral remodeling modifies arteries from low-flow/high-resistance to high-flow/low-resistance vessels [15,16], but the maternal diabetes may change this process and the functioning of the placenta. Poor nutrient and oxygen transfer across the placenta lead to fetal hypoxia [17], while delayed metabolic products removal increases the risk of fetal asphyxia [18]. Hyperglycemia, both in fetus and mother, leads to changes in vascular condition, higher oxidative stress, and awakening of epigenetic remodeling [19,20]. Changes on the placental level are angiomorphological and pathophysiological with implications on hemodynamics, reducing utero-placental perfusion. The protection mechanism for the fetus is known as the “brain sparing” phenomenon. Blood from the peripheral blood stream is being redistributed to the brain instead of the viscera, which can be seen in a decreased fetal middle cerebral artery resistance and pulsatility index and increased umbilical artery resistance and pulsatility index [21,22]. These hemodynamic changes could be revealed by Doppler ultrasound measurements [18,23]. The predictive power of Doppler US for adverse perinatal outcomes in both high- and low-risk pregnancies has been proven by numerous studies [16]. It still remains uncertain to which extent altered hemodynamics accompanies diabetic pregnancies. Therefore, the aim of this study was to assess the differences in pulsatility (PI), resistance (RI) and systolic/diastolic ratio (S/D ratio) Doppler indices of uterine (Ut), umbilical (U), and middle cerebral artery (MCA) in diabetic versus non-diabetic pregnancies by conducting a comprehensive systematic review of the literature with a meta-analysis.
2. Materials and Methods
2.1. Study Design
This systematic review was registered at PROSPERO (CRD42023409966) and is conducted according to the PRISMA protocol recommendations (Reporting Items for Systematic Reviews and Meta-Analyses) [24] and MOOSE guidelines [25].
2.2. Eligibility Criteria
Original studies that measured Doppler indices (pulsatility, resistance, and systolic/diastolic ratio) of umbilical, uterine, and middle cerebral arteries in pregnant women with pre-gestational or gestational DM were included. The inclusion criteria were developed according to the PICOS system: (P) population: all pregnant women; (E) exposure: pre-gestational DM or GDM; (C) control: non-DM or non-GDM; (O) outcome: pulsatility index (PI), resistance index (RI), or systolic/diastolic ratio (S/D ratio) of umbilical, uterine, and middle cerebral arteries; (S) study design: controlled trials, prospective or retrospective cohort, nested case-control in cohort studies, case-control studies, and cross-sectional studies.
The exclusion criteria were: (i) language: other than English; (ii) not an original article: narrative reviews, systematic reviews, meta-analysis, case reports, case series, editorials, comments, correspondences, books, short, abstracts, etc.; (iii) wrong population: other than humans (animals, cell lines), not pregnant women; (iv) no control group; (v) inadequate control group: not non-DM pregnant women; (vi) wrong outcome: other indices than PI, RI, and S/D ratio for arteries other than umbilical, uterine, and cerebral medial artery.
Two researchers with expertise in conducting systematic reviews and meta-analyses (AC, NM) developed and ran the search. The following databases were electronically searched: PubMed, Web of Science (WoS), and SCOPUS until 6 September 2022. The following search queries were combined to identify all relevant articles that measured Doppler indices among pregnant women with GDM and pregnant women with pregestational-GDM: (Gestational diabetes mellitus and (Color Doppler ultrasonography or Color Doppler ultrasonography or Doppler or Doppler sonography or Doppler velocimetry or Pulse wave Doppler or pulsatility index or peak systolic velocity or systolic/diastolic ratio or S/D ratio or resistance index or resistive index or resistivity index)) or (Diabetes mellitus and pregnancy and (Color Doppler ultrasonography or Doppler or Doppler sonography or Doppler velocimetry or Pulse wave Doppler or pulsatility index or peak systolic velocity or systolic/diastolic ratio or S/D ratio or resistance index or resistive index or resistivity index)) (details are available in Supplementary Materials: Table S1). In addition, reference lists of articles identified through electronic search and relevant reviews and editorials were manually searched to check for more potentially relevant articles.
2.3. Article Screening and Selection
Publications were screened for inclusion by title and abstract reading independently by two reviewers (M.M., K.K.) in the first step, and by full-text reading by two new reviewers (S.P.-K., A.C.). All disagreements were resolved by discussion at each stage with the inclusion of a third reviewer if needed (M.G.D. or D.S. or N.M.). A Rayyan online application was used for the first step of the selection process. Studies were included in the full-text screening if the study was identified as potentially eligible or if the abstract and title did not have sufficient information for exclusion.
2.4. Data Abstraction and Quality Assessment
Two reviewers (S.P., A.C.) independently abstracted the following data: (i) authors, publication year, country, study design, measured Doppler index, and artery; (ii) type of DM, sample size, characteristics of cases and controls, glycaemia, HbA1c, maternal age, gestational age, body weight, body mass index; (iii) criteria for DM; (iv) inclusion and exclusion criteria for cases and controls; and (v) newborns gender, body weight, Apgar score in the 1st and 5th minute. Previously designed protocol was used for data extraction. Authors of relevant articles were contacted to obtain unavailable manuscripts and/or missing data. Each reviewer independently performed a risk of bias and quality assessment of the included articles using an adapted version of the Newcastle-Ottawa tool (NOS) for observational studies [26]. The study quality, according to NOS, was defined: good (3 or 4 stars in selection AND 1 or 2 stars in comparability AND 2 or 3 stars in outcome/exposure domain, or ≥7 stars in total), fair (2 stars in selection AND 1 or 2 stars in comparability AND 2 or 3 stars in outcome/exposure domain, or 5–6 stars in total), or poor (0 or 1 star in selection OR 0 stars in comparability OR 0 or 1 star in outcome/exposure, or ≤4 stars in total). Results of the quality assessment is given in Supplementary Materials: Table S2.
2.5. Statistical Analysis
The primary outcome was the difference in the PI, RI, and S/D ratio Doppler indices of the umbilical, uterine, and middle cerebral artery in diabetic versus non-diabetic pregnancies. While figures were used to present Doppler indices, GraphGrabber was used to read indices values. If data were not presented as an arithmetic mean with standard deviation, the following approximations were used: (1) if median was available, median was used as an approximation of the mean; (2) where z score was available, the mean was calculated according to the following formula [27]: (sd × z) where sd = se × √n; (3) if the multiple of median (MoM) was available, mean was calculated as MoM = median(patient/population value) [27]; (4) if IQR was available, standard deviation (sd) was calculated as sd = IQR/1.35; (5) if standard error (se) was used, sd was obtained by the following formula sd = se × √n; (6) if range was reported, sd was calculated as sd = (max − min)/4, and; (7) if 95%CI was used, sd was calculated as ((Upper limit of 95%CI − ((Upper limit of 95%CI + Lower limit of 95%CI)/2))/1, 96) × √n.
The standardized mean difference (SMD) was used to examine differences in diabetic versus non-diabetic pregnancies, due to different methodologies used for Doppler measurements across the studies included in the meta-analysis. SMD expresses the difference between group means in units of standard deviation and was estimated by pooling individual trial results using random-effects models via the Der Simonian-Laird method. Heterogeneity was assessed using the Chi-square Q and I2 statistic. I2 presents the inconsistency between the study results and quantifies the proportion of observed dispersion that is real, i.e., due to between-study differences and not due to random error. The categorization of heterogeneity was based on the Cochrane Handbook [28]: I2 < 30%, 30–60%, or >60%, correspond to low, moderate, and high heterogeneity, respectively. Forest plots were constructed for each analysis showing the SMD (box), 95% confidence interval (lines), and weight (size of box) for each study. The overall effect size was represented by a diamond. Publication bias was assessed by funnel plots for each defined outcome (Supplementary Materials: Figures S1–S16). Subgroup analysis was performed for (1) pregestational and gestational DM and (2) Doppler indices measured in the 1st, 2nd, and 3rd trimester separately. Sensitivity analyses were conducted to examine the effects of: (1) different DM cases (removing the combination of DM and other diseases like PE, HPD). p value ≤ 0.05 was considered statistically significant. Analyses were performed using Review Manager Version 5.4.
3. Results
3.1. Systematic Review
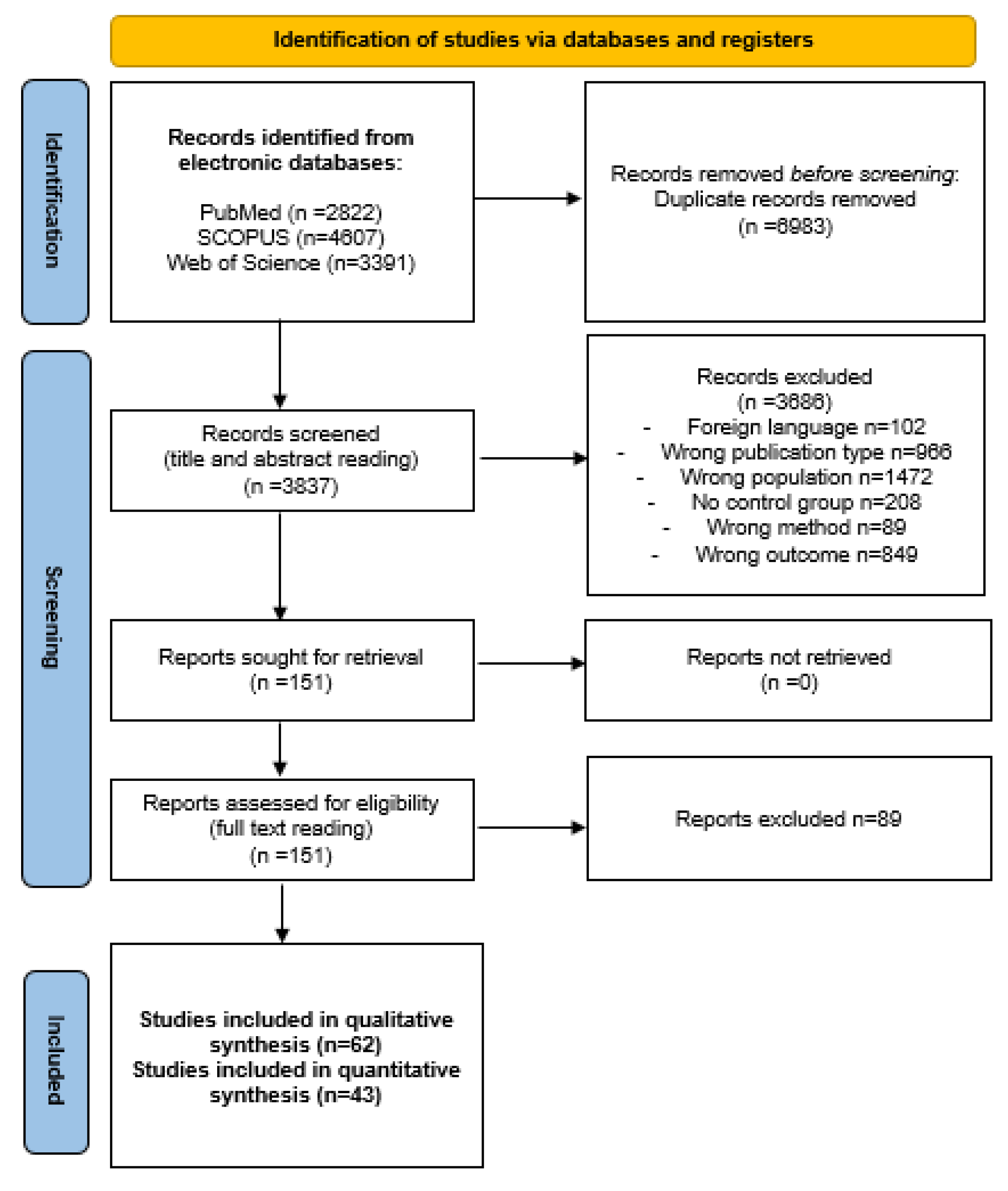
A total of 10,820 potentially eligible articles were found. After removal of 6983 duplicates, 3837 articles were screened for inclusion based on the title and abstract reading. After the exclusion of 3686 articles (due to wrong publication type, population, outcome, method, no presence of control group or language other than English), 151 publications were screened for inclusion based on full-text reading. A total of 62 articles were selected for inclusion in the qualitative and 43 for quantitative synthesis. A flow chart illustrating the selection process is presented in Figure 1.
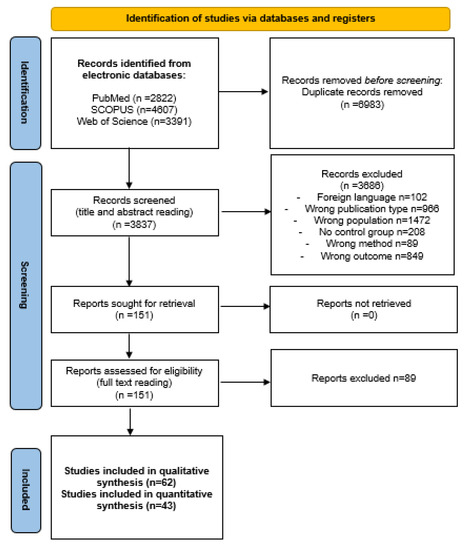
Figure 1.
Flow diagram.
Characteristics of all publications included in the systematic review are presented in detail in Table 1. Studies were published between 1987 and 2022, with a total of 156,166 participants; 9912 women with and 146,254 without DM. The minimum and maximum sample size of the DM group was 9 and 4015, while for the non-DM group it was 10 and 71,565. Matching was applied in 23% of studies only; gestational age at the time of delivery and maternal age were the most commonly used variables for matching (in 9/15 and 6/15 studies, respectively). Other matching variables were: obesity, weight gain during pregnancy, BMI at the time of delivery, chronic hypertension, parity, race, gravidity, past obstetric history, and smoking. Prospective cohort studies were the most common among included studies (20/62); 8 studies were cross-sectional, 7 studies were case-controls, and 1 study was a retrospective cohort. Eleven studies did not correctly report study design and 15 did not report study design at all. Most studies were performed in Europe (23) and Asia (22). There were also studies from North America (9), Africa (4), South America (2), and Australia and Oceania (2). The predominant population included in studies were pregnant women with GDM (39/62). Pregnant women with pre-GDM type 1 were assessed in 21/62 studies, pre-gestational diabetes mellitus type 2 in 9/62, while the type of pre-GDM was not specified in 9 studies. Doppler ultrasonography was performed during the 3rd trimester in 39/62 studies, 2nd trimester in 18/62, and 1st trimester in one study. The exact timing of Doppler measurements was not reported in 12 studies. The most assessed Doppler index was the pulsatility index (33/62); the resistance index was measured in 15 studies, while the S/D ratio index was used in 11 studies. All 33 studies that assessed PI performed measurement on the umbilical artery; PI was measured on the middle cerebral artery in 20/33 and on the uterine artery in 13/33. The umbilical artery RI was measured in 16 studies, middle cerebral artery RI in 10/15, and uterine artery RI in 3/15. The systolic/diastolic ratio index was measured in all 11 studies on the umbilical artery, while it was measured on the middle cerebral artery in 7/11, and on the uterine artery in 3/11.

Table 1.
Systematic review.
A total of 41/62 of included studies reported specific criteria and 37/41 a definition for DM diagnosis as well. White’s classification of Diabetes in Pregnancy, World Health Organization (WHO), and American Diabetes Association (ADA) criteria were used in 11, 8, and 7 studies, respectively. Other criteria that were applied were: IADPSG (4), O’Sullivan (3), National Diabetes Data group (2), Australian Diabetes in Pregnancy (ADIPS) (2), National Institute for Health and Clinical Excellence (NICE) guidelines, American College of Obstetricians and Gynecologists (ACOG), Fifth International Workshop-Conference on Gestational Diabetes, and the Sixth edition of Obstetrics and Gynecology in one study each. Details regarding DM definitions and the diagnostic criteria used in the included articles are presented in Supplementary Materials: Table S3. The most common exclusion criterium was multiple pregnancy (31/62), while other exclusion criteria were: chronic hypertension (17/62), preeclampsia (14/62), pregnancy-induced hypertension (12/62), smoking (11/62), renal diseases (11/62), cardiovascular diseases (10/62), obesity (4/62), and nulliparity (1/62). Inclusion and exclusion criteria used in included studies are presented in detail in the Supplementary Materials: Table S4. The characteristics of newborns were rarely reported. Birth weight was available in 42/62 studies, gender in 14, while Apgar score was available in 18 studies. Supplementary Materials: Table S5 presents newborns’ characteristics in more detail.
3.2. Meta-Analysis
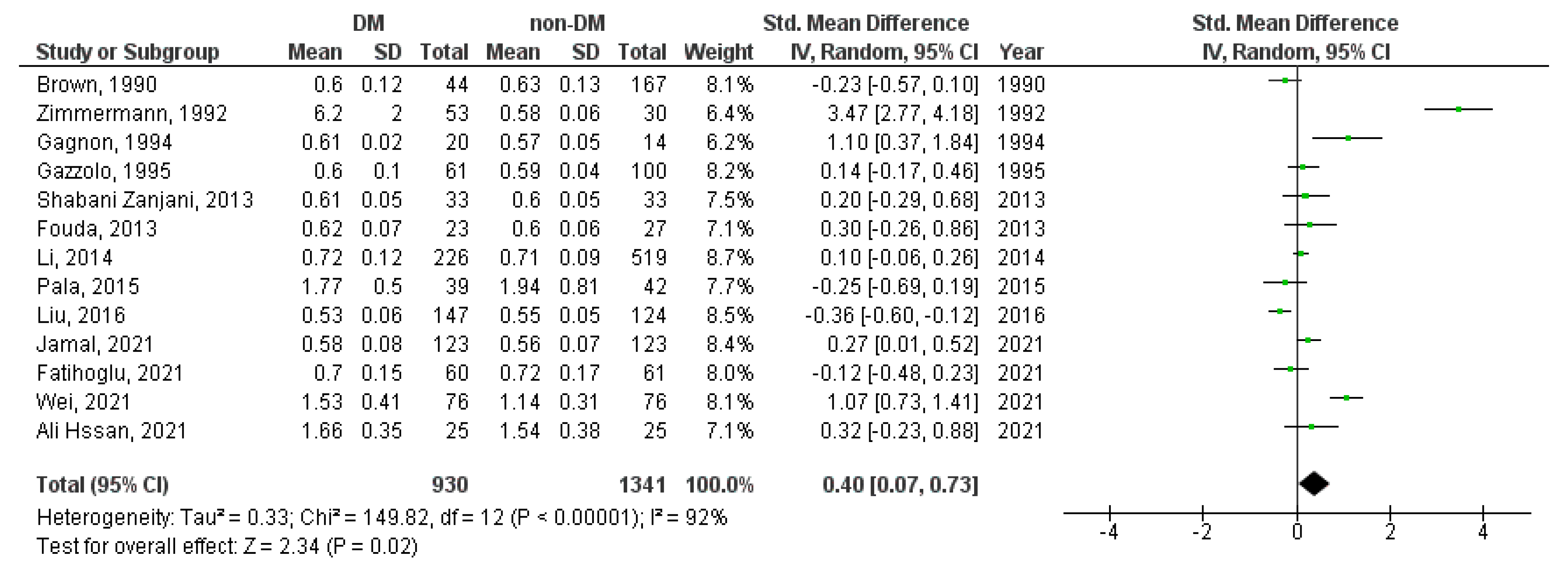
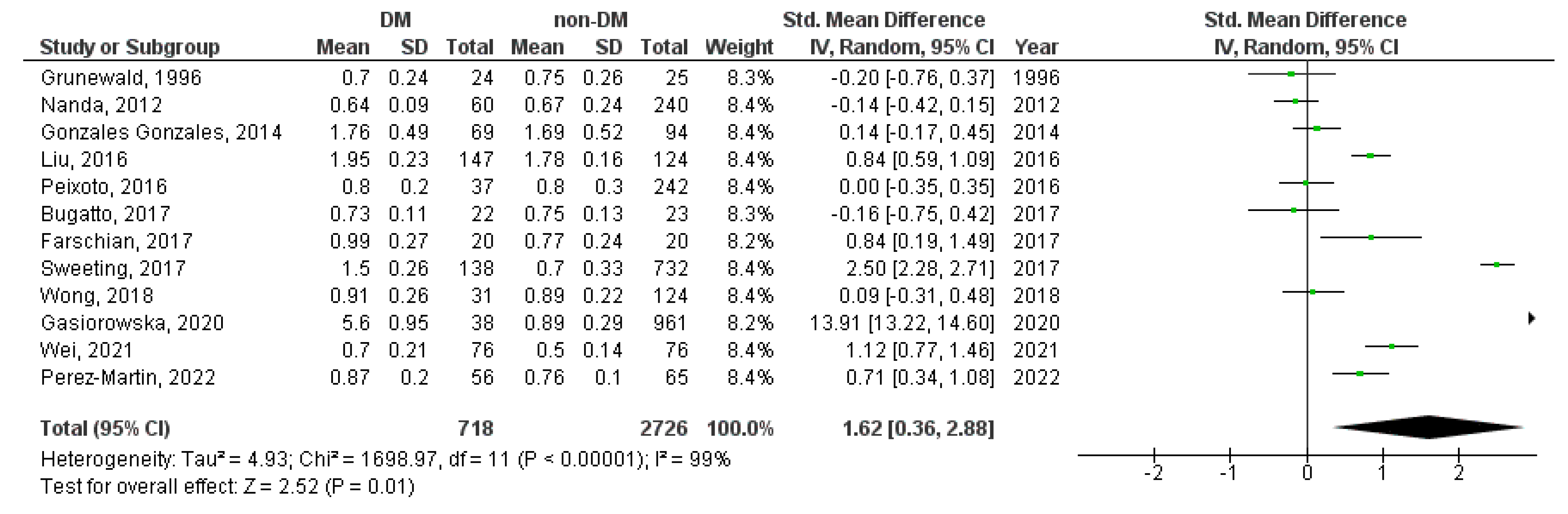
A meta-analysis was performed for the UA-PI, UA-RI, UA-S/D ratio, MCA-PI, MCA-RI, MCA-S/D ratio, UtA-PI, UtA-RI, and UtA-S/D ratio Doppler indices. The UA-RI, UtA-PI, and UtA-S/D ratio were significantly higher in diabetic in contrast to non-diabetic pregnancies (SMD = 0.40, 95%CI = 0.07–0.73, p = 0.020 (Figure 2); SMD = 1.62, 95%CI = 0.36–2.88, p = 0.010 (Figure 3), and SMD = 1.02, 95%CI = 0.02–2.03, p = 0.050 (Figure 4), respectively).
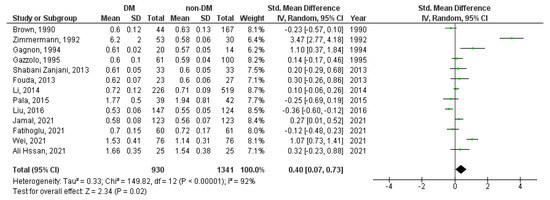
Figure 2.
UA-RI Doppler index in diabetic versus non-diabetic pregnancies. The green squares represent each study individual SMD and the extending lines the 95% confidence intervals. The black diamond represents the overall estimate result [18,21,32,34,36,39,53,56,60,61,80,82,83].
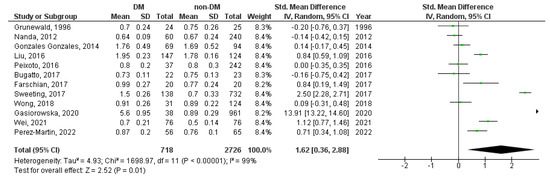
Figure 3.
UtA-PI Doppler index in diabetic versus non-diabetic pregnancies. The green squares represent each study individual SMD and the extending lines the 95% confidence intervals. The black diamond represents the overall estimate result [14,18,41,52,57,61,62,63,64,67,70,84].

Figure 4.
UtA-S/D ratio Doppler index in diabetic versus non-diabetic pregnancies. The green squares represent each study individual SMD and the extending lines the 95% confidence intervals. The black diamond represents the overall estimate result [18,32,61].
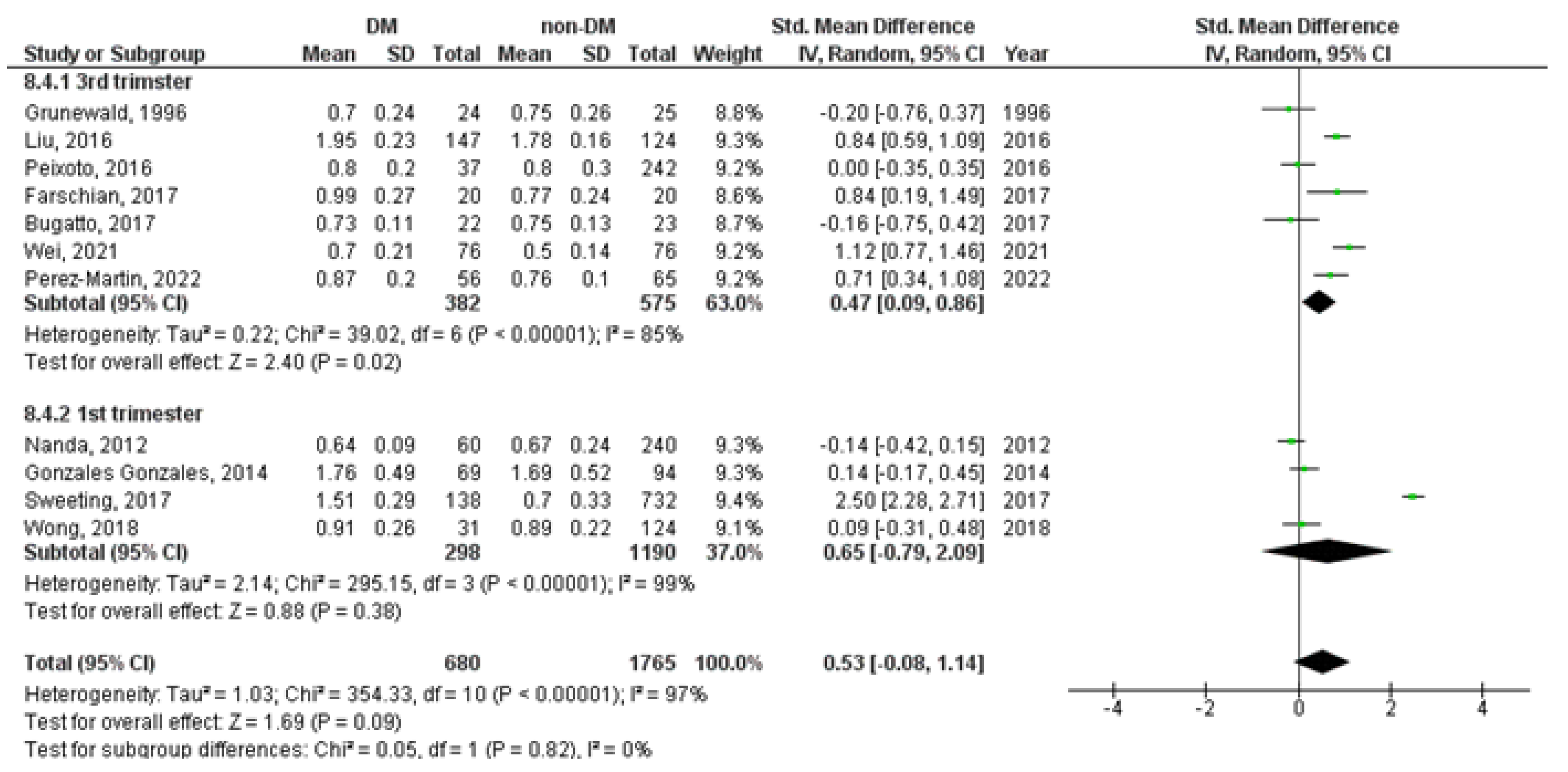
Subgroup analysis showed increased levels of UtA-PI measured during the 3rd trimester (SMD = 0.47, 95%CI = 0.09–0.86, p = 0.020), but not during the 1st trimester of pregnancy (SMD = 0.65, 95%CI = −0.79–2.09, p = 0.380), in diabetic versus non-diabetic pregnancies (Figure 5).
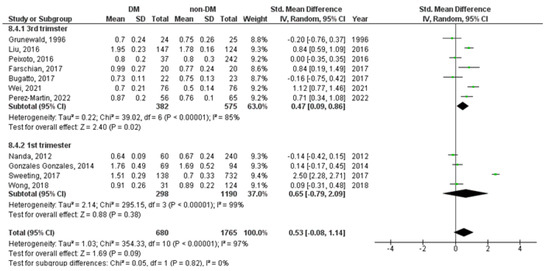
Figure 5.
UtA-PI Doppler index in diabetic versus non-diabetic pregnancies according to the time of Doppler measurements. The green squares represent each study individual SMD and the extending lines the 95% confidence intervals. The black diamond represents the overall estimate result [14,18,41,52,57,61,62,63,64,67,70,84].
The following Doppler indices were not significantly different in diabetic versus non-diabetic pregnancies: UA-PI (SMD = 0.12, 95%CI = −0.05–0.29, p = 0.170) (Supplementary Materials: Figure S17), UA-S/D ratio (SMD = 0.01, 95%CI = −0.37–0.39, p = 0.960) (Supplementary Materials: Figure S18), MCA-PI (SMD = 0.15, 95%CI = −0.12–0.42, p = 0.280) (Supplementary Materials: Figure S19), MCA-RI (SMD = 0.21, 95%CI = −0.57–0.98, p = 0.600) (Supplementary Materials: Figure S20), MCA-S/D ratio (SMD = −0.28, 95%CI = −1.07–0.51, p = 0.480) (Supplementary Materials: Figure S21), and UtA-RI (SMD = 0.66, 95%CI = −0.40–1.73, p = 0.220) (Supplementary Materials: Figure S22).
Sensitivity analysis including studies of gestational versus non-GDM pregnancies presented no significant differences in the following Doppler indices: UA-PI (SMD = 0.04, 95%CI = −0.10–0.19, p = 0.540) (Supplementary Materials: Figure S23), UA-RI (SMD = 0.16, 95%CI = −0.08–0.41, p = 0.190) (Supplementary Materials: Figure S24), UA-S/D ratio (SMD = 0.18, 95%CI = −0.19–0.54, p = 0.340) (Supplementary Materials: Figure S25), MCA-PI (SMD = 0.15, 95%CI = −0.13–0.43, p = 0.300) (Supplementary Materials: Figure S26), MCA-RI (SMD = 0.28, 95%CI = −0.71–1.27, p = 0.580) (Supplementary Materials: Figure S27), MCA-S/D ratio (SMD = −0.28, 95%CI = −1.07–0.51, p = 0.480) (Supplementary Materials: Figure S28), and UtA-PI (SMD = 0.63, 95%CI = −0.13–1.38, p = 0.100) (Supplementary Materials: Figure S29).
4. Discussion
This is the first systematic review with a meta-analysis assessing differences in pulsatility, resistance, and systolic/diastolic ratio Doppler indices of the uterine, umbilical, and middle cerebral artery between pregnant women with and without diabetes mellitus. The UA-RI, UtA-PI, and UtA-S/D ratio had higher values in pregnant women with than without DM. Subgroup analysis showed that levels of UtA-PI were significantly higher in DM than in non-DM pregnant women during the 3rd, but not during the 1st trimester.
The maternal body goes through many physiological adaptations to fulfill pregnancy requirements. Healthy pregnancy is a state of mild insulin resistance that becomes obvious in the late 2nd trimester due to the dysfunction of beta cells in the mother’s pancreas resulting in higher blood glucose levels. These changes occur due to hormonal secretion of the placenta, weight gain, and endothelial dysfunction through enhanced inflammation and a Th-2 predominant immune response [87]. Intensive production of human placental lactogen, estrogen, progesterone, prolactin, and cortisol [19,88], as well as adipocytokines (leptin, tumor necrosis factor alpha, interleukin-6, resistin, visfatin, apelin, and retinol-binding protein 4) are contributing the most to disrupted glucose homeostasis during pregnancy [19,87]. Morphology changes in placenta in terms of infarctions, retroplacental hemorrhage, distal villous hypoplasia, and decidual arteriopathy are induced by the aforementioned processes [89]. The endothelial dysfunction together with higher blood glucose concentrations produce higher blood flow viscosity, thus the blood flow resistance increases while blood flow speed decreases, which easily leads to abnormal blood perfusion [18]. During the course of pregnancy, changes in the uteroplacental, fetoplacental, and fetal circulation, representing the oxygen metabolism in between the three compartments maternal, feto-maternal, and fetal, become more detectable [21]. Reference ranged Doppler values measured on uterine, umbilical, and cerebral media arteries are the mirror of efficient circulation necessary for adequate fetal development and growth [90].
Our study demonstrated increased UA-RI, UtA-PI, and UtA-S/D ratio Doppler indices in pregnant women with DM in contrast to those without DM. Previous studies reported inconsistent results regarding the arteries and Doppler indices measured, time of Doppler measurements, different forms of DM, and diabetes severity. Nicolaides et al. found no relation between UtA and UA with neither short-term nor long-term maternal glycemic control [91], and therefore concluded that impedance to flow in the uterine artery is normal in diabetic pregnancy, even in patients complicated with nephropathy and vasculopathy [91]. This was not the case with the umbilical artery, in the study by Gazzolo, where the increase in impedance was noticed in the state of maternal vasculopathy [39]. Abnormal UA-RI was associated with birthweights of less than 50th centile seen in diabetic pregnancy [33]. The same authors reported in 1992 that UA-RI declined significantly during the course of T1DM pregnancy [34] and in 1994 that UtA-RI was slightly higher in the presence of evident morphological vasculopathy [92]. Pietryga et al. [93] demonstrated significantly increased uterine artery vascular impedance in pregnant women with T1DM in cases with severe vasculopathy, while Gutaj et al. [94] obtained that the UA-RI increase does not depend on the level of vascular changes in the mother. UA-PI was the highest in pregnant women with T1DM in comparison with T2DM and GDM, while there was no difference in the mean MCA PI between these three groups [95]. Wei et al. [18] had found that the increase in the PI, RI, and S/D value during pregnancy were positively correlated with the onset of GDM, indicating that the arterial blood flow condition during pregnancy can reflect the formation process of GDM, and has certain clinical significance for GDM diagnosis and disease monitoring.
However, materno-fetal Doppler parameters can be affected not only by DM but by many other factors. Systemic diseases like hypertensive disorders in pregnancy and cardiovascular diseases have a lot of overlapping risk factors (age, smoking, obesity, etc.) with DM [96]. Inadequate vascular dilatation and angiogenesis are common pathohistological causes of hypertension in pregnancy, preeclampsia and GDM, denoting a failed response to the vasodilatory and pro-angiogenic challenge imposed by pregnancy, especially if multifetal [97]. GDM is also known to be a risk factor for later onset of gestational hypertension. The relationship between inadequate glucose milieu and higher blood pressure lies in reshaped uteroplacental vascularization [98], which results further on with abnormal uteroplacental blood flow [99]. In these cases, Doppler velocimetry measurements may have an important role in real-time antepartum surveillance as they have the ability to detect high-risk pregnancies in disrupted oxygenation states such as in hypoxemia, anemia, preeclampsia, IUGR, and DM [39,100,101]. It is also known that doppler velocimetry as a tool is very helpful in predicting adverse outcomes in twin pregnancies [102]. Although some of these factors like chronic diseases, preeclampsia, fetal growth retardation, and drug use, that may affect Doppler parameters, are stated as exclusion criteria in some studies included in our meta-analysis, the absence of such exclusion criteria (or not reporting them) in others may affect the results of our meta-analysis. Fouda et al. found that HgA1c was higher in pregestational diabetic women with chronic hypertension. Also, UA-RI was higher in diabetic pregnancies with hypertension, but not in diabetic pregnancies without hypertension, in comparison to uncomplicated pregnancies as controls [53]. Hssan et al. reported higher UA-PI levels in diabetic pregnancies complicated by preeclampsia [82]. In a recent study, tobacco combustion was associated with higher uterine and umbilical PI, RI, and S/D ratio Doppler indices with a strong association between indices values and the number of cigarettes smoked per day [103].
Results of our meta-analysis presented no significant differences between the DM and non-DM groups in terms of fetal MCA Doppler parameters. It is known that long-term uncontrolled hyperglycemia, chronic hypertension, preeclampsia, and IUGR can lead to placental vascular dysfunction with changes even in fetal circulation [53,82,104,105,106]. But the effect of metabolic changes due to diabetes mellitus during pregnancy on the fetus may be acidemia without hypoxemia, thus that redistribution seen in fetal hypoxemia may not occur even in severely compromised fetuses; and, therefore, it is of huge importance not to misrepresent this state by apparently normal fetal Doppler results [80].
This study has several limitations that should be considered when interpreting the results. First, the absence of exclusion criteria such as additional chronic diseases, preeclampsia and/or fetal growth retardation, and drug use in some of the included studies may affect the overall pooled estimate of this meta-analysis. Second, some patients with DM included in studies are followed by using insulin, and some are followed only by appropriate diet. This broad range of therapy regimens might also affect the results of the meta-analysis. Third, although the pregnancy trimesters are specified in some studies, it is possible that the differences between the gestational weeks of Doppler measurements applied in the studies affects the overall results.
5. Conclusions
This meta-analysis revealed the presence of hemodynamic changes in uterine and umbilical arteries, but not in middle cerebral artery in pregnancies complicated by diabetes. UtA-PI, UtA-S/D ratio, and UA-RI Doppler indices are higher in diabetic versus non-diabetic pregnancies. More studies are needed to distinguish effects of pregestational versus gestational diabetes on hemodynamic changes during pregnancy.
Supplementary Materials
The following supporting information can be downloaded at: https://www.mdpi.com/article/10.3390/medicina59081502/s1, File S1. Search strategy, Table S1. Quality assessment, Figures S1–S16. Funnel plots, Table S2. Definitions and criteria of pregestational and gestational diabetes mellitus used in included studies, Table S3. Inclusion and exclusion criteria used in included studies, Table S4. Characteristics of newborns reported in included studies, Figure S17. UA-PI Doppler index in pregnant women with vs. pregnant women without diabetes mellitus, Figure S18. UA-S/D ratio Doppler index in pregnant women with vs. pregnant women without diabetes mellitus, Figure S19. MCA-PI Doppler index in pregnant women with vs. pregnant women without diabetes mellitus, Figure S20. MCA-RI Doppler index in pregnant women with vs. pregnant women without diabetes mellitus, Figure S21. MCA-S/D ratio Doppler index in pregnant women with vs. pregnant women without diabetes mellitus, Figure S22. UtA-RI Doppler index in pregnant women with vs. pregnant women without diabetes mellitus, Figure S23. UA-PI Doppler index in pregnant women with GDM vs. women without GDM, Figure S24. UA-RI Doppler index in pregnant women with GDM vs. women without GDM, Figure S25. UA-S/D ratio Doppler index in pregnant women with GDM vs. women without GDM, Figure S26. MCA-PI Doppler index in pregnant women with GDM vs. women without GDM, Figure S27. MCA-RI Doppler index in pregnant women with GDM vs. women without GDM, Figure S28. MCA-S/D ratio Doppler index in pregnant women with GDM vs. women without GDM, Figure S29. UtA-PI Doppler index in pregnant women with GDM vs. women without GDM.
Author Contributions
Conceptualization: S.P.-K., A.C., N.M. (Natasa Milic), D.S. and M.G.D.; Data curation: S.P.-K., A.C., S.D., M.M., K.K., N.M. (Nikola Milic), J.T., K.M. and N.A.G.; Formal analysis: S.P.-K., A.C., N.M. (Natasa Milic), D.S. and M.G.D.; Investigation: S.P.-K., A.C., S.D., M.M., K.K., N.M. (Nikola Milic), J.T., K.M. and N.A.G.; Methodology: A.C., N.M. (Natasa Milic), D.S., S.D., M.M., K.K., N.M. (Nikola Milic), J.T., K.M., N.A.G. and M.G.D. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
All additional data are available as Supplementary Materials.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Farrar, D.; Simmonds, M.; Bryant, M.; Sheldon, T.A.; Tuffnell, D.; Golder, S.; Dunne, F.; Lawlor, D.A. Hyperglycaemia and Risk of Adverse Perinatal Outcomes: Systematic Review and Meta-Analysis. BMJ 2016, 354, i4694. [Google Scholar] [PubMed]
- Franzago, M.; Fraticelli, F.; Stuppia, L.; Vitacolonna, E. Nutrigenetics, Epigenetics and Gestational Diabetes: Consequences in Mother and Child. Epigenetics 2019, 14, 215–235. [Google Scholar] [CrossRef] [PubMed]
- Turkmen, S.; Johansson, S.; Dahmoun, M. Foetal Macrosomia and Foetal-Maternal Outcomes at Birth. J. Pregnancy 2018, 2018, 4790136. [Google Scholar] [CrossRef] [PubMed]
- Ye, W.; Luo, C.; Huang, J.; Li, C.; Liu, Z.; Liu, F. Gestational Diabetes Mellitus and Adverse Pregnancy Outcomes: Systematic Review and Meta-Analysis. BMJ 2022, 377, e067946. [Google Scholar]
- Hochberg, A.; Pardo, A.; Oron, G.; Krispin, E.; Amikam, U.; Wiznitzer, A.; Hadar, E.; Salman, L. Perinatal Outcome Following Induction of Labor in Patients with Good Glycemic Controlled Gestational Diabetes: Does Timing Matter? Arch. Gynecol. Obstet. 2019, 300, 299–303. [Google Scholar] [PubMed]
- Melamed, N.; Ray, J.G.; Geary, M.; Bedard, D.; Yang, C.; Sprague, A.; Murray-Davis, B.; Barrett, J.; Berger, H. Induction of Labor before 40 Weeks Is Associated with Lower Rate of Cesarean Delivery in Women with Gestational Diabetes Mellitus. Am. J. Obstet. Gynecol. 2016, 214, e1–e364. [Google Scholar]
- MacDonald, S.C.; Bodnar, L.M.; Himes, K.P.; Hutcheon, J.A. Patterns of Gestational Weight Gain in Early Pregnancy and Risk of Gestational Diabetes Mellitus. Epidemiology 2017, 28, 419–427. [Google Scholar] [CrossRef]
- Glazer, N.L.; Hendrickson, A.F.; Schellenbaum, G.D.; Mueller, B.A. Weight change and the risk of gestational diabetes in obese women. Epidemiology 2004, 15, 733–737. [Google Scholar] [CrossRef]
- Zhao, Z.; Reece, E.A. New Concepts in Diabetic Embryopathy. Clin. Lab. Med. 2013, 33, 207–233. [Google Scholar]
- Kallem, V.R.; Pandita, A.; Pillai, A. Infant of Diabetic Mother: What One Needs to Know? J. Matern.-Fetal Neonatal Med. 2020, 33, 482–492. [Google Scholar]
- Malaza, N.; Masete, M.; Adam, S.; Dias, S.; Nyawo, T.; Pheiffer, C. A Systematic Review to Compare Adverse Pregnancy Outcomes in Women with Pregestational Diabetes and Gestational Diabetes. Int. J. Environ. Res. Public Health 2022, 19, 10846. [Google Scholar] [CrossRef] [PubMed]
- Mistry, S.K.; Das Gupta, R.; Alam, S.; Kaur, K.; Shamim, A.A.; Puthussery, S. Gestational Diabetes Mellitus (GDM) and Adverse Pregnancy Outcome in South Asia: A Systematic Review. Endocrinol. Diabetes Metab. 2021, 4, e00285. [Google Scholar] [PubMed]
- Coustan, D.R. Gestational Diabetes Mellitus. Clin. Chem. 2013, 59, 1310–1321. [Google Scholar]
- Plows, J.F.; Stanley, J.L.; Baker, P.N.; Reynolds, C.M.; Vickers, M.H. The Pathophysiology of Gestational Diabetes Mellitus. Int. J. Mol. Sci. 2018, 19, 3342. [Google Scholar] [CrossRef]
- Allen, R.E.; Morlando, M.; Thilaganathan, B.; Zamora, J.; Khan, K.S.; Thangaratinam, S.; Bhide, A. Predictive Accuracy of Second-Trimester Uterine Artery Doppler Indices for Stillbirth: A Systematic Review and Meta-Analysis. Ultrasound Obstet. Gynecol. 2016, 47, 22–27. [Google Scholar] [PubMed]
- La Verde, M.; Torella, M.; Ronsini, C.; Riemma, G.; Cobellis, L.; Marrapodi, M.M.; Capristo, C.; Rapisarda, A.M.C.; Morlando, M.; De Franciscis, P. The association between fetal Doppler and uterine artery blood volume flow at term of pregnancy: A pilot study. Ultraschall Med. 2023. epub ahead of print. [Google Scholar] [CrossRef]
- Jaiman, S.; Romero, R.; Pacora, P.; Erez, O.; Jung, E.; Tarca, A.L.; Bhatti, G.; Yeo, L.; Kim, Y.M.; Kim, C.J.; et al. Disorders of Placental Villous Maturation Are Present in One-Third of Cases with Spontaneous Preterm Labor. J. Perinat. Med. 2021, 49, 412–430. [Google Scholar]
- Wei, Z.; Mu, M.; Li, M.; Li, J.; Cui, Y. Color Doppler Ultrasound Detection of Hemodynamic Changes in Pregnant Women with GDM and Analysis of Their Influence on Pregnancy Outcomes. Am. J. Transl. Res. 2021, 13, 3330–3336. [Google Scholar]
- Ornoy, A.; Becker, M.; Weinstein-Fudim, L.; Ergaz, Z. Diabetes during Pregnancy: A Maternal Disease Complicating the Course of Pregnancy with Long-Term Deleterious Effects on the Offspring. A Clinical Review. Int. J. Mol. Sci. 2021, 22, 2965. [Google Scholar]
- Schierz, I.A.M.; Pinello, G.; Piro, E.; Giuffrè, M.; La Placa, S.; Corsello, G. Transitional Hemodynamics in Infants of Diabetic Mothers by Targeted Neonatal Echocardiography, Electrocardiography and Peripheral Flow Study. J. Matern. Neonatal Med. 2018, 31, 1578–1585. [Google Scholar]
- Shabani Zanjani, M.; Nasirzadeh, R.; Fereshtehnejad, S.M.; Yoonesi Asl, L.; Alemzadeh, S.A.P.; Askari, S. Fetal Cerebral Hemodynamic in Gestational Diabetic versus Normal Pregnancies: A Doppler Velocimetry of Middle Cerebral and Umbilical Arteries. Acta Neurol. Belg. 2014, 114, 15–23. [Google Scholar] [PubMed]
- Ciobanu, A.; Wright, A.; Syngelaki, A.; Wright, D.; Akolekar, R.; Nicolaides, K.H. Fetal Medicine Foundation Reference Ranges for Umbilical Artery and Middle Cerebral Artery Pulsatility Index and Cerebroplacental Ratio. Ultrasound Obstet. Gynecol. 2019, 53, 465–472. [Google Scholar] [PubMed]
- Altorjay, Á.T.; Surányi, A.; Nyári, T.; Németh, G. Use of Placental Vascularization Indices and Uterine Artery Peak Systolic Velocity in Early Detection of Pregnancies Complicated by Gestational Diabetes, Chronic or Gestational Hypertension, and Preeclampsia at Risk. Croat. Med. J. 2017, 58, 161–169. [Google Scholar] [CrossRef]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gøtzsche, P.C.; Ioannidis, J.P.A.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA Statement for Reporting Systematic Reviews and Meta-Analyses of Studies That Evaluate Health Care Interventions: Explanation and Elaboration. PLoS Med. 2009, 6, e1000100. [Google Scholar] [CrossRef]
- Stroup, D.F.; Berlin, J.A.; Morton, S.C.; Olkin, I.; Williamson, G.D.; Rennie, D.; Moher, D.; Becker, B.J.; Sipe, T.A.; Thacker, S.B. Meta-Analysis of Observational Studies in Epidemiology: A Proposal for Reporting. Meta-Analysis of Observational Studies in Epidemiology (MOOSE) Group. JAMA 2000, 283, 2008–2012. [Google Scholar] [CrossRef] [PubMed]
- Wells, G.A.; Shea, B.; O’Connell, D.; Peterson, J.; Welch, V.; Losos, M.; Tugwell, P. The Newcastle-Ottawa Scale (NOS) for Assessing the Quality of Nonrandomised Studies in Meta-Analyses; Ottawa Hospital Research Institute: Ottawa, ON, Canada, 2014. [Google Scholar]
- Weichert, A.; Hagen, A.; Tchirikov, M.; Fuchs, I.B.; Henrich, W.; Entezami, M. Reference Curve for the Mean Uterine Artery Pulsatility Index in Singleton Pregnancies. Geburtshilfe Frauenheilkd. 2017, 77, 516–523. [Google Scholar] [PubMed]
- Higgins, J.P.; Thomas, J.; Chandler, J.; Cumpston, M.; Li, T.; Page, M.J.; Welch, V.A. Cochrane Handbook for Systematic Reviews of Interventions; John Wiley & Sons: Hoboken, NJ, USA, 2019; ISBN 9780470699515. [Google Scholar]
- Olofsson, P.; Lingman, G.; Marsal, K.; Sjoberg, N.-O. Fetal Blood Flow in Diabetic Pregnancy 545 Fetal Blood Flow in Diabetic Pregnancy. J. Perinat. Med. 1987, 15, 545. [Google Scholar] [CrossRef] [PubMed]
- Landon, M.; Gabbe, S.; Bruner, J.; Ludmir, J. Doppler Umbilical Artery Velocimetry in Pregnancy Complicated by Insulin-Dependent Diabetes Mellitus. Obstet. Gynecol. 1989, 73, 961–965. [Google Scholar]
- Friedman, D.M.; Ehrlich, P.; Hoskins, I.A. Umbilical Artery Doppler Blood Velocity Waveforms in Normal and Abnormal Gestations. J. Ultrasound Med. 1989, 8, 375–380. [Google Scholar] [CrossRef]
- Brown, M.A.; Northz, L.; Hargoodl, J. Uteroplacental Doppler Ultrasound in Routine Antenatal Care. Aust. N. Z. J. Obstet. Gynaecol. 1990, 30, 303–307. [Google Scholar] [CrossRef]
- Johnstone, F.; Steel, J.; Haddad, N.; Hoskins, P.; Greer, I.; Chambers, S. Doppler Umbilical Artery Flow Velocity Waveforms in Diabetic Pregnancy. Br. J. Obstet. Gynaecol. 1992, 99, 135–140. [Google Scholar] [PubMed]
- Zimmermann, P.; Kujansuu, E.; Tuimala, R. Doppler Velocimetry of the Umbilical Artery in Pregnancies Complicated by Insulin-Dependent Diabetes Mellitus. Eur. J. Obstet. Gynecol. Reprod. Biol. 1992, 47, 85–93. [Google Scholar] [CrossRef] [PubMed]
- Pachi, A.; Maggi, E.; Ferrero, A.; Giancotti, A.; Marceca, M.; Matone, M.; Castelli, R. Umbilical Artery Blood Flow in Pregnancies Complicated by Insulin-Dependent Diabetes Mellitus. J. Obstet. Gynaecol. 1993, 13, 423–427. [Google Scholar] [CrossRef]
- Gagnon, R.; Tevaarwerk, G.; Hunse, C.; Connors, G. Longitudinal Doppler Ultrasound Assessment of Fetal Circulation in Diabetic Pregnancies in Relation to Maternal Glycemic Control. J. Matern.-Fetal Med. 1994, 3, 1–8. [Google Scholar] [CrossRef]
- Weber, H.S.; Botti, J.J.; Baylen, B.G.; Weber, H.S. Pediatric Cardiology Sequential Longitudinal Evaluation of Cardiac Growth and Ventricular Diastolic Filling in Fetuses of Well Controlled Diabetic Mothers. Pediatr. Cardiol. 1994, 15, 184–189. [Google Scholar] [CrossRef] [PubMed]
- Santolaya, J.; Kahn, D.; Nobles, G.; Ramakrishnan, V.; Warsof, S. Ultrasonographic Growth and Doppler Hemodynamic Evaluation of Fetuses of Obese Women. J. Reprod. Med. 1994, 39, 690–694. [Google Scholar]
- Gazzolo, D.; Scopes, F.; Russo, A.; Camorlano, R.; Santl, F.; Vlsser, G.; Bruschettlnl, P. Doppler Velocimetry and Behavioural State Development in Relation to Perinatal Outcome in Pregnancies Complicated by Gestational Diabetes. Early Hum. Dev. 1995, 41, 193–201. [Google Scholar] [CrossRef]
- Saldeen, P.; Olofsson, P.; Parhar, R.S.; AI-Sedairy, S. Prostanoid Production in Umbilical Vessels and Its Relation to Glucose Tolerance and Umbilical Artery Flow Resistance. Eur. J. Obstet. Gynecol. Reprod. Biol. 1996, 68, 35–41. [Google Scholar] [CrossRef]
- Grunewald, C.; Divon, M.; Lunell, N.O. Doppler Velocimetry in Last Trimester Pregnancy Complicated by Insulin-Dependent Diabetes Mellitus. Acta Obstet. Gynecol. Scand. 1996, 75, 804–808. [Google Scholar] [CrossRef]
- Weiner, Z.; Thaler, I.; Farmakides, G.; Barnhard, Y.; Maulik, D.; Divon, M. Fetal Heart Rate Patterns in Pregnancies Complicated by Maternal Diabetes. Eur. J. Obstet. Gynecol. Reprod. Biol. 1996, 70, 111–115. [Google Scholar] [CrossRef]
- Ursem, N.T.C.; Clark, E.B.; Keller, B.B.; Wladimiroff, J.W. Fetal Heart Rate and Umbilical Artery Velocity Variability in Pregnancies Complicated by Insulin-Dependent Diabetes Mellitus. Ultrasound Obstet. Gynecol. 1999, 13, 312–316. [Google Scholar] [CrossRef] [PubMed]
- Boito, S.M.; Struijk, P.C.; Ursem, N.T.C.; Stijnen, T.; Wladimiroff, J.W. Assessment of Fetal Liver Volume and Umbilical Venous Volume Flow in Pregnancies Complicated by Insulin-Dependent Diabetes Mellitus. BJOG 2003, 110, 1007–1013. [Google Scholar] [CrossRef]
- Tan, A.E.; Norizah, W.M.; Rahman, H.A.; Aziz, B.A.; Cheah, F.C. Umbilical Artery Resistance Index in Diabetic Pregnancies: The Associations with Fetal Outcome and Neonatal Septal Hypertrophic Cardiomyopathy. J. Obstet. Gynaecol. Res. 2005, 31, 296–301. [Google Scholar] [PubMed]
- Florio, P.; Reis, F.M.; Severi, F.M.; Luisi, S.; Imperatore, A.; Palumbo, M.A.; Bagnoli, F.; Gioffre, W.; Petraglia, F. Umbilical Cord Serum Activin A Levels Are Increased in Pre-Eclampsia with Impaired Blood Flow in the Uteroplacental and Fetal Circulation. Placenta 2006, 27, 432–437. [Google Scholar] [CrossRef] [PubMed]
- Girsen, A.; Ala-Kopsala, M.; Mäkikallio, K.; Vuolteenaho, O.; Räsänen, J. Increased Fetal Cardiac Natriuretic Peptide Secretion in Type-1 Diabetic Pregnancies. Acta Obstet. Gynecol. Scand. 2008, 87, 307–312. [Google Scholar] [CrossRef]
- Russell, N.E.; Higgins, M.F.; Amaruso, M.; Foley, M.; McAuliffe, F.M. Troponin T and Pro-B-Type Natriuretic Peptide in Fetuses of Type 1 Diabetic Mothers. Diabetes Care 2009, 32, 2050–2055. [Google Scholar] [CrossRef]
- To, W.W.K.; Mok, C.K.M. Fetal Umbilical Arterial and Venous Doppler Measurements in Gestational Diabetic and Nondiabetic Pregnancies near Term. J. Matern. Neonatal Med. 2009, 22, 1176–1182. [Google Scholar] [CrossRef]
- Parlakgumus, H.A.; Durukan, T. The Relationship between Cardiac Adaptation to Uteroplacental Doppler Flow and Perinatal Outcome in Pregnant Women with Diabetes. Clin. Exp. Obstet. Gynecol. 2010, 37, 39–42. [Google Scholar]
- Turan, S.; Turan, O.M.; Miller, J.; Harman, C.; Reece, E.A.; Baschat, A.A. Decreased Fetal Cardiac Performance in the First Trimester Correlates with Hyperglycemia in Pregestational Maternal Diabetes. Ultrasound Obstet. Gynecol. 2011, 38, 325–331. [Google Scholar]
- Nanda, S.; Poon, L.C.Y.; Muhaisen, M.; Acosta, I.C.; Nicolaides, K.H. Maternal Serum Resistin at 11 to 13 Weeks’ Gestation in Normal and Pathological Pregnancies. Metabolism 2012, 61, 699–705. [Google Scholar] [CrossRef]
- Fouda, U.M.; Elkassem, M.M.A.; Hefny, S.M.; Hashem, A.T. Role of Middle Cerebral Artery, Umbilical Artery Resistance Indices and Middle Cerebral Artery to Umbilical Artery Resistance Index Ratio in Predicting Unfavorable Perinatal Outcomes of Normotensive and Hypertensive Diabetic Pregnancies. Life Sci. J. 2013, 10, 1097–8135. [Google Scholar]
- Surányi, A.; Kozinszky, Z.; Molnár, A.; Nyári, T.; Bitó, T.; Pál, A. Placental Three-Dimensional Power Doppler Indices in Mid-Pregnancy and Late Pregnancy Complicated by Gestational Diabetes Mellitus. Prenat. Diagn. 2013, 33, 952–958. [Google Scholar] [PubMed]
- Savvidou, M.D.; Syngelaki, A.; Balakitsas, N.; Panaiotova, E.; Nicolaides, K.H. First-Trimester Uterine Artery Doppler Examination in Pregnancies Complicated by Gestational Diabetes Mellitus with or without Pre-Eclampsia. Ultrasound Obstet. Gynecol. 2013, 42, 525–529. [Google Scholar] [CrossRef] [PubMed]
- Li, J.; Chen, Y.P.; Dong, Y.P.; Yu, C.H.; Lu, Y.P.; Xiao, X.M.; Hocher, B. The Impact of Umbilical Blood Flow Regulation on Fetal Development Differs in Diabetic and Non-Diabetic Pregnancy. Kidney Blood Press. Res. 2014, 39, 369–377. [Google Scholar]
- Gonzalez Gonzalez, N.L.; Gonzalez Davila, E.; Castro, A.; Padron, E.; Plasencia, W. Effect of Pregestational Diabetes Mellitus on First Trimester Placental Characteristics: Three-Dimensional Placental Volume and Power Doppler Indices. Placenta 2014, 35, 147–151. [Google Scholar]
- Moran, M.; Mulcahy, C.; Daly, L.; Zombori, G.; Downey, P.; McAuliffe, F.M. Novel Placental Ultrasound Assessment: Potential Role in Pre-Gestational Diabetic Pregnancy. Placenta 2014, 35, 639–644. [Google Scholar]
- Bhorat, I.E.; Bagratee, J.S.; Pillay, M.; Reddy, T. Use of the Myocardial Performance Index as a Prognostic Indicator of Adverse Fetal Outcome in Poorly Controlled Gestational Diabetic Pregnancies. Prenat. Diagn. 2014, 34, 1301–1306. [Google Scholar] [PubMed]
- Pala, H.G.; Artunc-Ulkumen, B.; Koyuncu, F.M.; Bulbul-Baytur, Y. Three-Dimensional Ultrasonographic Placental Volume in Gestational Diabetes Mellitus. J. Matern. Neonatal Med. 2016, 29, 610–614. [Google Scholar] [CrossRef] [PubMed]
- Liu, F.; Liu, Y.; Lai, Y.P.; Gu, X.N.; Liu, D.M.; Yang, M. Fetal Hemodynamics and Fetal Growth Indices by Ultrasound in Late Pregnancy and Birth Weight in Gestational Diabetes Mellitus. Chin. Med. J. 2016, 129, 2109–2114. [Google Scholar]
- Farshchian, N.; Naleini, F.; Jaafarnejhad, A.M. Comparison of the Uterine Artery Doppler Indices during Pregnancy between Gestational Diabetes and Diabetes Mellitus and Healthy Pregnant Women. World Fam. Med./Middle East J. Fam. Med. 2017, 15, 32–35. [Google Scholar] [CrossRef]
- Bugatto, F.; Quintero-Prado, R.; Visiedo, F.M.; Vilar-Sánchez, J.M.; Figueroa-Quiñones, A.; López-Tinoco, C.; Torrejón, R.; Bartha, J.L. The Influence of Lipid and Proinflammatory Status on Maternal Uterine Blood Flow in Women with Late Onset Gestational Diabetes. Reprod. Sci. 2018, 25, 837–843. [Google Scholar]
- Sweeting, A.N.; Wong, J.; Appelblom, H.; Ross, G.P.; Kouru, H.; Williams, P.F.; Sairanen, M.; Hyett, J.A. A First Trimester Prediction Model for Gestational Diabetes Utilizing Aneuploidy and Pre-Eclampsia Screening Markers. J. Matern. Neonatal Med. 2018, 31, 2122–2130. [Google Scholar] [CrossRef] [PubMed]
- Meiramova, A.; Ainabekova, B.; Sadybekova, G.; Akhmetova, Z.; Imangazinova, S.; Omralina, Y. Peculiarities of the Course of Gestation and Pregnancy Outcomes in Women with Gestational Diabetes Mellitus. Acta Endocrinol. 2018, 14, 213–218. [Google Scholar]
- Moodley, S.; Arunamata, A.; Stauffer, K.J.; Nourse, S.E.; Chen, A.; Quirin, A.; Selamet Tierney, E.S. Maternal Arterial Stiffness and Fetal Cardiovascular Physiology in Diabetic Pregnancy. Ultrasound Obstet. Gynecol. 2018, 52, 654–661. [Google Scholar] [CrossRef] [PubMed]
- Wong, C.H.; Chen, C.P.; Sun, F.J.; Chen, C.Y. Comparison of Placental Three-Dimensional Power Doppler Indices and Volume in the First and the Second Trimesters of Pregnancy Complicated by Gestational Diabetes Mellitus. J. Matern. Neonatal Med. 2019, 32, 3784–3791. [Google Scholar] [CrossRef] [PubMed]
- Dantas, A.M.A.; Palmieri, A.B.S.; Vieira, M.R.; Souza, M.L.R.; Silva, J.C. Doppler Ultrasonographic Assessment of Fetal Middle Cerebral Artery Peak Systolic Velocity in Gestational Diabetes Mellitus. Int. J. Gynecol. Obstet. 2019, 144, 174–179. [Google Scholar] [CrossRef]
- Bhorat, I.; Pillay, M.; Reddy, T. Assessment of the Fetal Myocardial Performance Index in Well-Controlled Gestational Diabetics and to Determine Whether It Is Predictive of Adverse Perinatal Outcome. Pediatr. Cardiol. 2019, 40, 1460–1467. [Google Scholar]
- Gasiorowska, A.; Zawiejska, A.; Dydowicz, P.; Wender-Ozegowska, E.; Poprawski, G.; Tobola-Wrobel, K.; Radzicka-Mularczyk, S.; Ziolkowska, K.; Pietryga, M. Mid-Trimester Ultrasound Parameters for Predicting Birth Weight in Low Risk Pregnancies vs. High-Risk Pregnancies Complicated with Pre-Gestational Diabetes Mellitus. Ginekol. Pol. 2020, 91, 216–222. [Google Scholar] [CrossRef]
- McLaren, R.; Kalgi, B.; Ndubizu, C.; Homel, P.; Haberman, S.; Minkoff, H. The Effect of Maternal Position on Fetal Middle Cerebral Artery Doppler Indices and Its Association with Adverse Perinatal Outcomes: A Pilot Study. J. Perinat. Med. 2020, 48, 317–321. [Google Scholar]
- Bachani, S.; Dadhwal, V.; Perumal, V. Correlation of Maternal BMI with Foetal Liver Blood Flow and Neonatal Adiposity in Normal Pregnancies and Pregnancies Complicated by Gestational Diabetes Mellitus and Foetal Growth Restriction. J. Clin. Diagn. Res. 2020, 14, QC08–QC11. [Google Scholar] [CrossRef]
- Tenenbaum-Gavish, K.; Sharabi-Nov, A.; Binyamin, D.; Møller, H.J.; Danon, D.; Rothman, L.; Hadar, E.; Idelson, A.; Vogel, I.; Koren, O.; et al. First Trimester Biomarkers for Prediction of Gestational Diabetes Mellitus. Placenta 2020, 101, 80–89. [Google Scholar] [CrossRef]
- Lehtoranta, L.; Haapsamo, M.; Vuolteenaho, O.; Palo, P.; Ekholm, E.; Räsänen, J. Fetal Cardiovascular Hemodynamics in Type 1 Diabetic Pregnancies at Near-Term Gestation. Acta Obstet. Gynecol. Scand. 2021, 100, 263–271. [Google Scholar] [CrossRef]
- Phadungkiatwattana, P.; Puttanavijarn, L. Comparison of Fetal Cardiac Function between Pregnancies with Diabetes Mellitus and Normal Controls. Thai J. Obstet. Gynaecol. 2021, 29, 264–272. [Google Scholar]
- Zhang, X.; Lou, Y.; Hu, S.; Zhu, D. Backpropagation Neural Network Algorithm-Based Color Doppler Ultrasound Detection of Gestational Diabetes Mellitus and Perinatal Outcomes. Sci. Program. 2021, 2021, 8. [Google Scholar]
- Oncel Alanyali, M.; Alkan, F.; Artunc Ulkumen, B.; Coskun, S. Use of the Modified Myocardial Performance Index for Evaluating Fetal Cardiac Functions in Pregestational Diabetic Pregnancy Babies. J. Obstet. Gynaecol. 2021, 41, 187–192. [Google Scholar] [CrossRef]
- Mecacci, F.; Ottanelli, S.; Vannuccini, S.; Serena, C.; Rambaldi, M.P.; Simeone, S.; Clemenza, S.; Comito, C.; Lisi, F.; Mello, G.; et al. What Is the Role of Glycemic Control in the Development of Preeclampsia among Women with Type 1 Diabetes? Pregnancy Hypertens. 2021, 25, 191–195. [Google Scholar] [CrossRef]
- Liu, H.; Liu, J. Improved Support Vector Machine Algorithm Based on the Influence of Gestational Diabetes Mellitus on the Outcome of Perinatal Outcome by Ultrasound Imaging. Pak. J. Med. Sci. 2021, 37, 1625–1629. [Google Scholar] [CrossRef]
- Fatihoglu, E.; Aydin, S.; Karavas, E.; Kantarci, M. Gestational Diabetes Mellitus and Early Hemodynamic Changes in Fetus. J. Med. Ultrasound 2021, 29, 270–276. [Google Scholar] [PubMed]
- Chen, Y.; Huang, D.; Liu, J.; Zeng, F.; Tang, G.; Lei, W.; Wang, H.; Jiang, Y.; Shentu, W.; Wang, H. Non-Invasive Detection of Fetal Vascular Endothelial Function in Gestational Diabetes Mellitus. Front. Endocrinol. 2021, 12, 763683. [Google Scholar] [CrossRef]
- Hssan, H.; Abd El Wahed, M.; Abdel Aziz, M. Interventricular Septal Thickness and Doppler Indices as Multiparametric Assessment of High-Risk Pregnancy and Their Relation to Fetal Outcome. Egypt. J. Hosp. Med. 2022, 87, 1876–1882. [Google Scholar]
- Jamal, A.S.; Naemi, M.; Eslamian, L.; Marsoosi, V.; Moshfeghi, M.; Nurzadeh, M.; Geran, T.; Ghaemi, M.; Zanbagh, L. The Association between Fetal Renal Artery Indices in Late Pregnancy and Birth Weight in Gestational Diabetes Mellitus: A Cohort Study. Int. J. Reprod. Biomed. 2022, 20, 21–28. [Google Scholar]
- Pérez-Martín, S.M.; Quintero-Prado, R.; Lara-Barea, A.; López-Tinoco, C.; Torrejón, R.; Bugatto, F. Fetal Cerebral Three-Dimensional Power Doppler Vascularization Indices and Their Relationships with Maternal Glucose Levels in Pregnancies Complicated with Gestational Diabetes. Diabetes Vasc. Dis. Res. 2022, 19, 14791641221078108. [Google Scholar] [CrossRef] [PubMed]
- Chatzakis, C.; Sotiriadis, A.; Fatouros, I.G.; Jamurtas, A.Z.; Deli, C.K.; Papagianni, M.; Dinas, K.; Mastorakos, G. The Effect of Physical Exercise on Oxidation Capacity and Utero-Placental Circulation in Pregnancies with Gestational Diabetes Mellitus and Uncomplicated Pregnancies, a Pilot Study. Diagnostics 2022, 12, 1732. [Google Scholar] [CrossRef]
- Karaca Kurtulmus, S.; Sahin Gülec, E.; Sengül, M. Evaluation of the Selected Parameters of the Fetal Diastolic Functions in Normally Grown or Macrosomic Fetuses of Gestational Diabetic Mothers with Poor Glycaemic Control. Cardiol. Young 2022, 32, 1320–1326. [Google Scholar] [CrossRef] [PubMed]
- Abell, S.K.; De Courten, B.; Boyle, J.A.; Teede, H.J. Inflammatory and Other Biomarkers: Role in Pathophysiology and Prediction of Gestational Diabetes Mellitus. Int. J. Mol. Sci. 2015, 16, 13442–13473. [Google Scholar] [PubMed]
- American College of Obstetricians and Gynecologists. ACOG Practice Bulletin Clinical Management Guidelines for Obstetrician-Gynecologists Number 202. Obstet. Gynecol. 2019, 133, e1–e25. [Google Scholar]
- Whittington, J.R.; Cummings, K.F.; Ounpraseuth, S.T.; Aughenbaugh, A.L.; Quick, C.M.; Dajani, N.K. Placental Changes in Diabetic Pregnancies and the Contribution of Hypertension. J. Matern. Neonatal Med. 2022, 35, 486–494. [Google Scholar] [CrossRef]
- Oros, D.; Ruiz-Martinez, S.; Staines-Urias, E.; Conde-Agudelo, A.; Villar, J.; Fabre, E.; Papageorghiou, A.T. Reference Ranges for Doppler Indices of Umbilical and Fetal Middle Cerebral Arteries and Cerebroplacental Ratio: Systematic Review. Ultrasound Obstet. Gynecol. 2019, 53, 454–464. [Google Scholar]
- Nicolaides, K.; Rizzo, G.; Hecher, K.; Ximenes, R. Doppler in Obstetrics; The Fetal Medicine Foundation: London, UK, 2002. [Google Scholar]
- Zimmermann, P.; Kujansuu, E.; Tuimala, R. Doppler Flow Velocimetry of the Uterine and Uteroplacental Circulation in Pregnancies Complicated by Insulin-Dependent Diabetes Mellitus. J. Perinat. Med. 1994, 22, 137–147. [Google Scholar] [CrossRef]
- Pietryga, M.; Brazert, J.; Wender-Ozegowska, E.; Dubiel, M.; Gudmundsson, S. Placental Doppler Velocimetry in Gestational Diabetes Mellitus. J. Perinat. Med. 2006, 34, 108–110. [Google Scholar] [CrossRef]
- Gutaj, P.; Wender-Ozegowska, E. Diagnosis and Management of IUGR in Pregnancy Complicated by Type 1 Diabetes Mellitus. Curr. Diabetes Rep. 2016, 16, 39. [Google Scholar] [CrossRef]
- Gibbons, A.; Flatley, C.; Kumar, S. The Fetal Cerebro-Placental Ratio in Diabetic Pregnancies Is Influenced More by the Umbilical Artery Rather than Middle Cerebral Artery Pulsatility Index. Eur. J. Obstet. Gynecol. Reprod. Biol. 2017, 211, 56–61. [Google Scholar] [PubMed]
- Jiang, L.; Tang, K.; Magee, L.A.; von Dadelszen, P.; Ekeroma, A.; Li, X.; Zhang, E.; Bhutta, Z.A. A Global View of Hypertensive Disorders and Diabetes Mellitus during Pregnancy. Nat. Rev. Endocrinol. 2022, 18, 760–775. [Google Scholar] [PubMed]
- Conti, E.; Zezza, L.; Ralli, E.; Caserta, D.; Musumeci, M.B.; Moscarini, M.; Autore, C.; Volpe, M. Growth Factors in Preeclampsia: A Vascular Disease Model: A Failed Vasodilation and Angiogenic Challenge from Pregnancy Onwards? Cytokine Growth Factor Rev. 2013, 24, 411–425. [Google Scholar] [PubMed]
- Erkamp, J.S.; Geurtsen, M.L.; Duijts, L.; Reiss, I.K.M.; Mulders, A.G.M.G.J.; Steegers, E.A.P.; Gaillard, R.; Jaddoe, V.W.V. Associations of Maternal Early-Pregnancy Glucose Concentrations with Placental Hemodynamics, Blood Pressure and Gestational Hypertensive Disorders. Am. J. Hypertens. 2020, 33, 660–666. [Google Scholar] [CrossRef] [PubMed]
- Contreras, Z.A.; Heck, J.E.; Lee, P.C.; Cui, X.; Hobel, C.J.; Janzen, C.; Lurmann, F.; Ritz, B. Prenatal Air Pollution Exposure, Smoking, and Uterine Vascular Resistance. Environ. Epidemiol. 2018, 2, e017. [Google Scholar] [CrossRef]
- Bhorat, I.; Foolchand, S.; Reddy, T. Cardiac Doppler in Poorly Controlled Gestational Diabetics and Its Link to Markers of Intra-Uterine Hypoxia and Adverse Outcome. J. Obstet. Gynaecol. 2021, 41, 66–72. [Google Scholar] [CrossRef]
- Meler, E.; Martínez, J.; Boada, D.; Mazarico, E.; Figueras, F. Doppler Studies of Placental Function. Placenta 2021, 108, 91–96. [Google Scholar] [CrossRef]
- Mok, T.; Afshar, Y.; Platt, L.D.; Guo, R.; Rao, R.R.; Pluym, I.D.; Silverman, N.S.; Han, C.S. Predicting Adverse Outcomes in Monochorionic-Diamniotic Twins: The Role of Intertwin Discrepancy in Middle Cerebral Artery Doppler Measurements and the Cerebroplacental Ratio. Am. J. Perinatol. 2021, 38, 1348–1357. [Google Scholar]
- Baki Yıldırım, S.; Ayaydın Yılmaz, K.İ.; Gulerman, C. The Effect of Active and Passive Maternal Smoking During Pregnancy on the Uterine Artery Blood Flow and Obstetric Outcomes: A Prospective Study. Cureus 2023, 15, e35270. [Google Scholar]
- Langmia, I.M.; Kräker, K.; Weiss, S.E.; Haase, N.; Schütte, T.; Herse, F.; Dechend, R. Cardiovascular Programming during and after Diabetic Pregnancy: Role of Placental Dysfunction and IUGR. Front. Endocrinol. 2019, 10, 2015. [Google Scholar]
- Misan, N.; Michalak, S.; Kapska, K.; Osztynowicz, K.; Ropacka-Lesiak, M. Blood-Brain Barrier Disintegration in Growth-Restricted Fetuses with Brain Sparing Effect. Int. J. Mol. Sci. 2022, 23, 12349. [Google Scholar] [PubMed]
- Mari, G.; Deter, R.; Carpenter, R.; Rahman, F.; Zimmerman, R.; Moise, K.J.; Dorman, K.; Ludomirsky, A.; Gonzalez, R.; Gomez, R.; et al. Noninvasive Diagnosis by Doppler Ultrasonography of Fetal Anemia Due to Maternal Red-Cell Alloimmunization. Collaborative Group for Doppler Assessment of the Blood Velocity in Anemic Fetuses. N. Engl. J. Med. 2000, 342, 9–14. [Google Scholar] [CrossRef] [PubMed]

Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).