
Postoperative Pain Following Eye Enucleation: A Prospective Observational Study
 , , , , , ,
, , , , , ,
Abstract
:What Is Already Known on This Topic
What This Study Adds
How This Study Might Affect Research, Practice, or Policy
1. Introduction
2. Materials and Methods
2.1. Ethics Committee Approval
2.2. Patient and Data Selection—Inclusion Criteria
- Informed patient consent
- Body weight between 50 and 120 kg
- Age over 18 years
- American Society of Anesthesiologists (ASA) score 1 to 3.
2.3. Anesthesia and Recovery Room
2.4. Surgery
2.5. Detection of Patients’ Pain Intensity and Well-Being
2.6. In-House Daily Pain Questionnaire
2.7. QUIPS Questionnaire
2.8. painDETECT® Questionnaire
2.9. Statistical Analysis
3. Results
3.1. Demographic Data
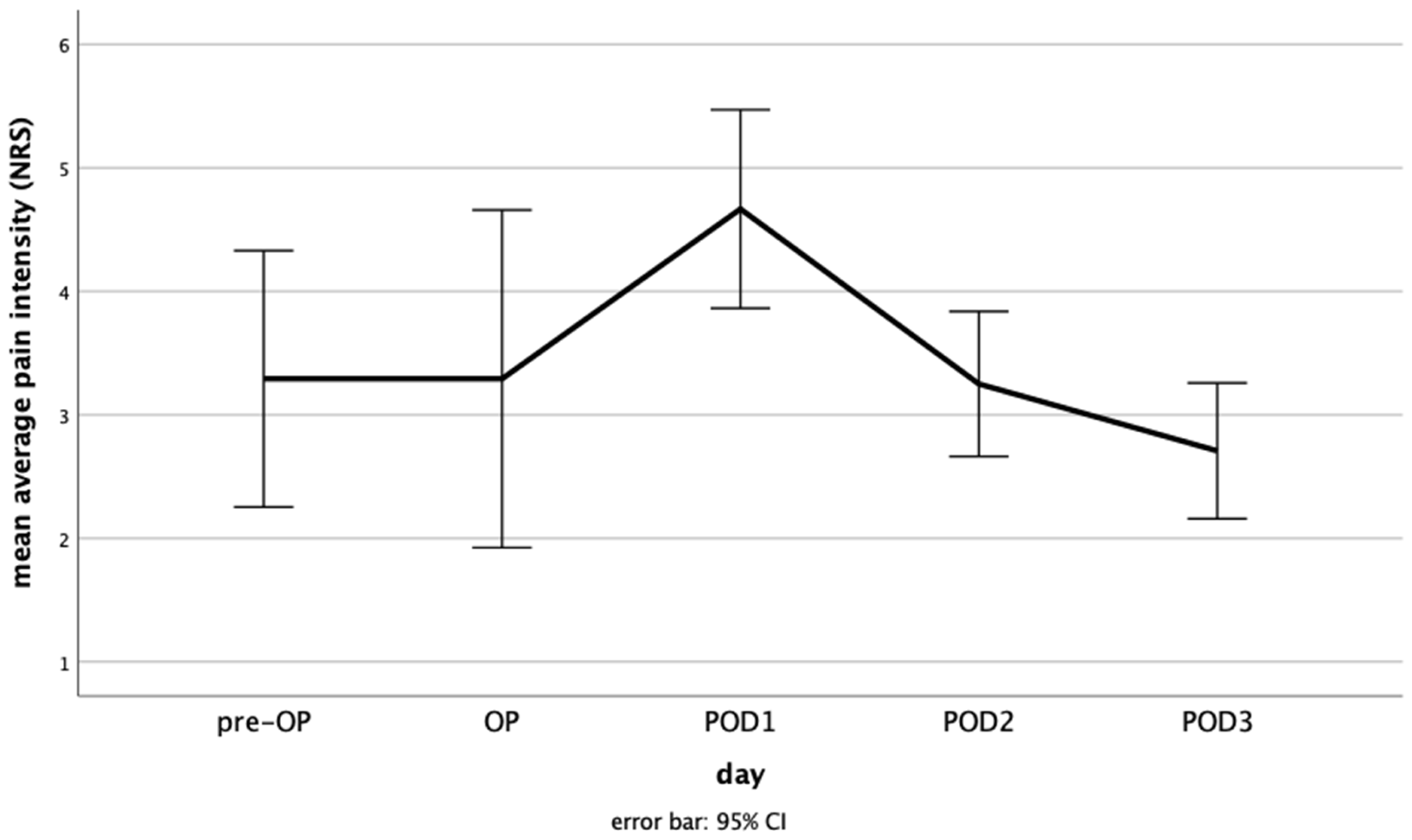
3.2. Average Pain
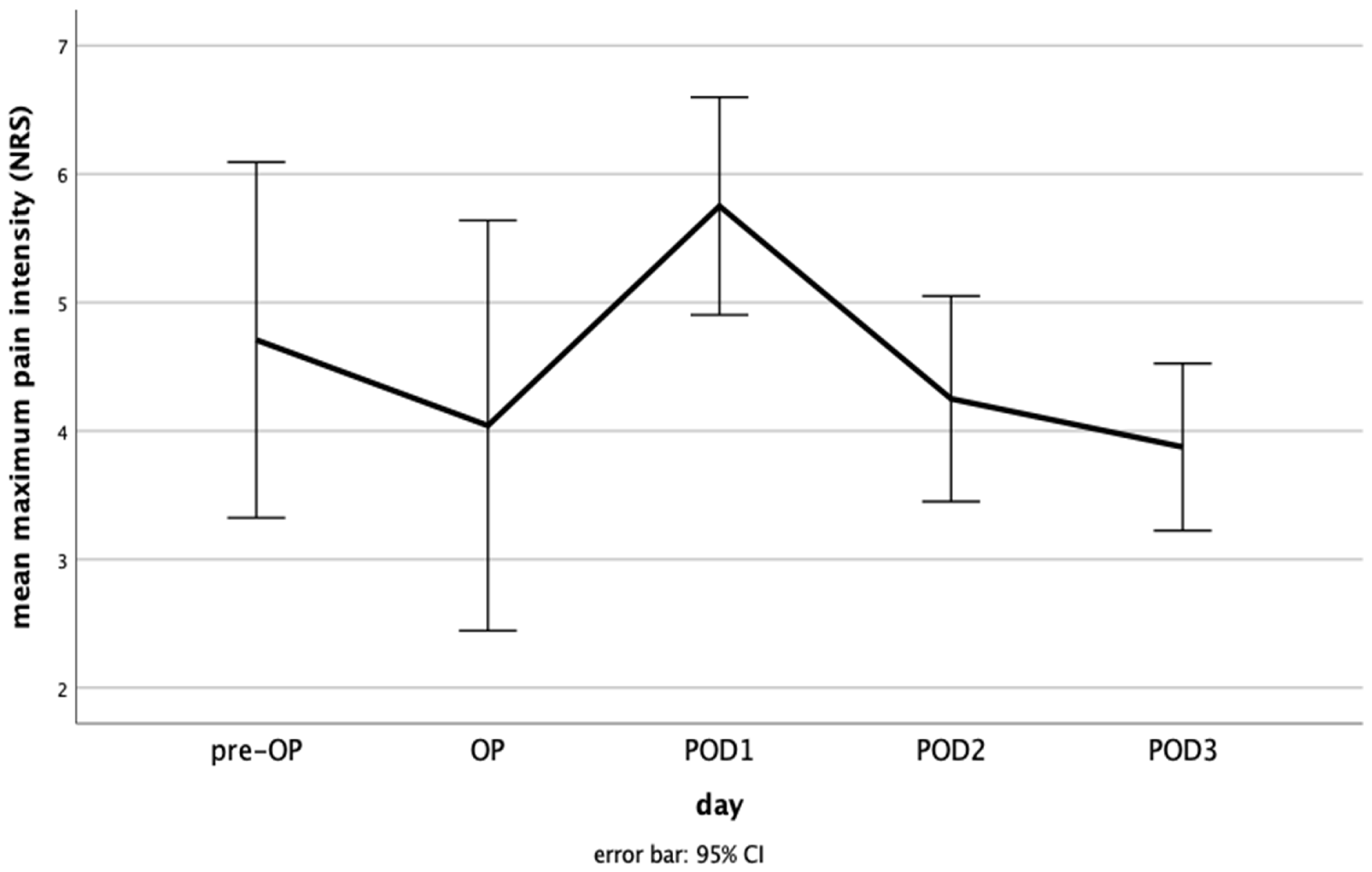
3.3. Maximum Pain
3.4. QUIPS Questionnaire
3.5. PainDETECT® Questionnaire
3.6. Perioperative Consumption of Analgesics
3.7. Desire for Further Pain Therapy
3.8. Treatment-Related Side-Effects
3.8.1. Nausea
3.8.2. Emesis
3.8.3. Constipation
3.8.4. Fatigue
3.8.5. Concentration Disorders
3.8.6. Sleep Disorders
3.8.7. Vertigo
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Adewara, B.A.; Badmus, S.A.; Adegbehingbe, B.O.; Awe, O.O.; Onakpoya, O.H.; Adeoye, A.O. Trends in Eye Removal Surgeries at a Tertiary Care Hospital Over Three Decades. West. Afr. J. Med. 2022, 39, 1068–1074. [Google Scholar]
- Ibanga, A.; Asana, U.; Nkanga, D.; Duke, R.; Etim, B.; Oworu, O. Indications for eye removal in southern Nigeria. Int. Ophthalmol. 2013, 33, 355–360. [Google Scholar] [CrossRef] [PubMed]
- Vemuganti, G.K.; Jalali, S.; Honavar, S.G.; Shekar, G.C. Enucleation in a tertiary eye care centre in India: Prevalence, current indications and clinicopathological correlation. Eye 2001, 15, 760–765. [Google Scholar] [CrossRef] [PubMed]
- O’Donnell, B.A.; Kersten, R.; McNab, A.; Rose, G.; Rosser, P. Enucleation versus evisceration. Clin. Exp. Ophthalmol. 2005, 33, 5–9. [Google Scholar] [CrossRef] [PubMed]
- Martel, A.; Baillif, S.; Thomas, P.; Almairac, F.; Galatoire, O.; Hamedani, M.; Fontaine, D.; Lanteri-Minet, M. Phantom vision after eye removal: Prevalence, features and related risk factors. Br. J. Ophthalmol. 2022, 106, 1603–1609. [Google Scholar] [CrossRef] [PubMed]
- Ababneh, O.H.; AboTaleb, E.A.; Abu Ameerh, M.A.; Yousef, Y.A. Enucleation and evisceration at a tertiary care hospital in a developing country. BMC Ophthalmol. 2015, 15, 120. [Google Scholar] [CrossRef] [PubMed]
- Ahn, J.M.; Lee, S.Y.; Yoon, J.S. Health-related quality of life and emotional status of anophthalmic patients in Korea. Am. J. Ophthalmol. 2010, 149, 1005–1011.e1. [Google Scholar] [CrossRef] [PubMed]
- Rasmussen, M.L.; Ekholm, O.; Prause, J.U.; Toft, P.B. Quality of life of eye amputated patients. Acta Ophthalmol. 2012, 90, 435–440. [Google Scholar] [CrossRef] [PubMed]
- Rokohl, A.C.; Koch, K.R.; Adler, W.; Trester, M.; Trester, W.; Pine, N.S.; Pine, K.R.; Heindl, L.M. Concerns of anophthalmic patients-a comparison between cryolite glass and polymethyl methacrylate prosthetic eye wearers. Graefes. Arch. Clin. Exp. Ophthalmol. 2018, 256, 1203–1208. [Google Scholar] [CrossRef] [PubMed]
- Haroutiunian, S.; Nikolajsen, L.; Finnerup, N.B.; Jensen, T.S. The neuropathic component in persistent postsurgical pain: A systematic literature review. Pain 2013, 154, 95–102. [Google Scholar] [CrossRef] [PubMed]
- Johansen, A.; Romundstad, L.; Nielsen, C.S.; Schirmer, H.; Stubhaug, A. Persistent postsurgical pain in a general population: Prevalence and predictors in the Tromso study. Pain 2012, 153, 1390–1396. [Google Scholar] [CrossRef] [PubMed]
- Reddi, D.; Curran, N. Chronic pain after surgery: Pathophysiology, risk factors and prevention. Postgrad Med. J. 2014, 90, 222–227; quiz 226. [Google Scholar] [CrossRef] [PubMed]
- Soros, P.; Vo, O.; Husstedt, I.W.; Evers, S.; Gerding, H. Phantom eye syndrome: Its prevalence, phenomenology, and putative mechanisms. Neurology 2003, 60, 1542–1543. [Google Scholar] [CrossRef] [PubMed]
- Martel, A.; Baillif, S.; Thomas, P.; Almairac, F.; Galatoire, O.; Hamedani, M.; Fontaine, D.; Lanteri-Minet, M. Phantom eye pain: A multicentric study in 100 patients. Acta Ophthalmol. 2021, 99, e753–e760. [Google Scholar] [CrossRef] [PubMed]
- Loeser, J.; Schwemmer, J.; Gostian, A.O.; Gostian, M.; Bachmann, B.; Cursiefen, C.; Heindl, L.M. Postoperative pain following Descemet membrane endothelial keratoplasty (DMEK): A prospective study. Graefes Arch. Clin. Exp. Ophthalmol. 2019, 257, 2203–2211. [Google Scholar] [CrossRef] [PubMed]
- Erlenwein, J.; Meissner, W.; Heindl, L.M.; Leister, N.; Castello, R.; Feltgen, N. Resolution of the Federal Joint Committee on the mandatory introduction and implementation of acute pain management concepts-Importance and consequences for ophthalmology. Ophthalmologie 2022, 120, 620–627. [Google Scholar] [CrossRef] [PubMed]
- Meissner, W.; Stamer, U.; Erlenwein, J.; Hoffmann, E.; Brunsmann, F. The guidelines of the Federal Joint Committee on acute pain management: Background and consequences for the practice in hospitals. Anaesthesiologie 2022, 71, 579–585. [Google Scholar] [CrossRef] [PubMed]
- Meissner, W.; Mescha, S.; Rothaug, J.; Zwacka, S.; Goettermann, A.; Ulrich, K.; Schleppers, A. Quality improvement in postoperative pain management: Results from the QUIPS project. Dtsch. Arztebl. Int. 2008, 105, 865–870. [Google Scholar] [CrossRef] [PubMed]
- Freynhagen, R.; Baron, R.; Gockel, U.; Tolle, T.R. painDETECT: A new screening questionnaire to identify neuropathic components in patients with back pain. Curr. Med. Res. Opin. 2006, 22, 1911–1920. [Google Scholar] [CrossRef] [PubMed]
- Tampin, B.; Bohne, T.; Callan, M.; Kvia, M.; Melsom Myhre, A.; Neoh, E.C.; Bharat, C.; Slater, H. Reliability of the English version of the painDETECT questionnaire. Curr. Med. Res. Opin. 2017, 33, 741–748. [Google Scholar] [CrossRef] [PubMed]
- Mellin-Olsen, J.; Staender, S.; Whitaker, D.K.; Smith, A.F. The Helsinki Declaration on Patient Safety in Anaesthesiology. Eur. J. Anaesthesiol. 2010, 27, 592–597. [Google Scholar] [CrossRef] [PubMed]
- Rokohl, A.C.; Trester, M.; Guo, Y.; Adler, W.; Jaeger, V.K.; Loreck, N.; Mor, J.M.; Pine, K.R.; Heindl, L.M. Dry anophthalmic socket syndrome-Standardized clinical evaluation of symptoms and signs. Ocul. Surf. 2020, 18, 453–459. [Google Scholar] [CrossRef] [PubMed]
- Ghanem, V.C.; Ghanem, R.C.; de Oliveira, R. Postoperative pain after corneal collagen cross-linking. Cornea 2013, 32, 20–24. [Google Scholar] [CrossRef]
- Porela-Tiihonen, S.; Kaarniranta, K.; Kokki, H. Postoperative pain after cataract surgery. J. Cataract. Refract. Surg. 2013, 39, 789–798. [Google Scholar] [CrossRef] [PubMed]
- Chowdhury, N.I.; Turner, J.H.; Dorminy, C.; Wu, J.; Chandra, R.K. Preoperative quality-of-life measures predict acute postoperative pain in endoscopic sinus surgery. Laryngoscope 2019, 129, 1274–1279. [Google Scholar] [CrossRef] [PubMed]
- Kubiliute, E.; Venskutonis, D.; Parseliunas, A.; Margelis, E.; Kiudelis, M. Risk factors predicting acute postoperative pain immediately after minimally invasive inguinal hernia repair. Wideochir. Inne. Tech. Maloinwazyjne 2023, 18, 475–480. [Google Scholar] [CrossRef] [PubMed]
- van Helmond, N.; Timmerman, H.; van Dasselaar, N.T.; van de Pol, C.C.; Olesen, S.S.; Drewes, A.M.; Vissers, K.; Wilder-Smith, O.H.; Steegers, M.A. High Body Mass Index Is a Potential Risk Factor for Persistent Postoperative Pain after Breast Cancer Treatment. Pain Physician 2017, 20, E661–E671. [Google Scholar] [PubMed]
- Springborg, A.H.; Visby, L.; Kehlet, H.; Foss, N.B. Psychological predictors of acute postoperative pain after total knee and hip arthroplasty: A systematic review. Acta Anaesthesiol. Scand. 2023, 67, 1322–1337. [Google Scholar] [CrossRef] [PubMed]
- Granot, M.; Ferber, S.G. The roles of pain catastrophizing and anxiety in the prediction of postoperative pain intensity: A prospective study. Clin. J. Pain 2005, 21, 439–445. [Google Scholar] [CrossRef] [PubMed]
- Ye, H.; Chen, R.; Lian, X.; Huang, J.; Mao, Y.; Lu, R.; Ai, S.; Ma, W.; Lin, J.; Yang, H.; et al. Risk factors associated with postoperative pain and discomfort in oculoplastic surgery with general anesthesia: A prospective study. J. Pain Res. 2018, 11, 407–415. [Google Scholar] [CrossRef] [PubMed]
- Mohan, B.; Kumar, R.; Attri, J.P.; Chatrath, V.; Bala, N. Anesthesiologist’s Role in Relieving Patient’s Anxiety. Anesth. Essays Res. 2017, 11, 449–452. [Google Scholar] [CrossRef] [PubMed]
- Laubenthal, H.; Becker, M.; Neugebauer, E. Guideline: “Treatment of acute perioperative and posttraumatic pain”-Updating from the S2- to the S3-level: A preliminary report. Anasthesiol. Intensivmed. Notfallmed. Schmerzther. 2006, 41, 470–472. [Google Scholar] [CrossRef] [PubMed]
- Ayuse, T.; Kurata, S.; Mishima, G.; Tachi, M.; Suzue, E.; Kiriishi, K.; Ozaki-Honda, Y.; Ayuse, T. Influence of general anesthesia on the postoperative sleep cycle in patients undergoing surgery and dental treatment: A scoping review on the incidence of postoperative sleep disturbance. J. Dent. Anesth. Pain Med. 2023, 23, 59–67. [Google Scholar] [CrossRef] [PubMed]
- Cronin, A.J.; Keifer, J.C.; Davies, M.F.; King, T.S.; Bixler, E.O. Melatonin secretion after surgery. Lancet 2000, 356, 1244–1245. [Google Scholar] [CrossRef] [PubMed]
- Mizuno, T.; Higo, S.; Kamei, N.; Mori, K.; Sakamoto, A.; Ozawa, H. Effects of general anesthesia on behavioral circadian rhythms and clock-gene expression in the suprachiasmatic nucleus in rats. Histochem. Cell Biol. 2022, 158, 149–158. [Google Scholar] [CrossRef]
- Chahin, S.; Morse, M.; Qaddoumi, I.; Phipps, S.; Crabtree, V.M.; Brennan, R.C.; Wilson, M.W.; Rodriguez-Galindo, C.; Russell, K.M.; Parris, K.; et al. An exploratory study of sleep habits in school-aged survivors of retinoblastoma. Sleep Med. 2023, 103, 123–130. [Google Scholar] [CrossRef] [PubMed]
- Fezza, J.P.; Klippenstein, K.A.; Wesley, R.E. Use of an orbital epidural catheter to control pain after orbital implant surgery. Arch. Ophthalmol. 1999, 117, 784–788. [Google Scholar] [CrossRef]
- Samimi, D.B.; Erb, M.H.; Perry, A.C.; Burnstine, M.A.; Dresner, S.C. On-Q pump for pain control after orbital implant surgery. Ophthalmic Plast. Reconstr. Surg. 2014, 30, 396–399. [Google Scholar] [CrossRef] [PubMed]
- Merbs, S.L.; Grant, M.P.; Iliff, N.T. Simple outpatient postoperative analgesia using an orbital catheter after enucleation. Arch. Ophthalmol. 2004, 122, 349–352. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Indication | Number |
|---|---|
| Bacterial infection | 1 |
| Ciliary body tumor | 1 |
| Conjunctival tumor | 1 |
| Autoimmune inflammation | 2 |
| Perforating trauma | 3 |
| Glaucoma (phthisis bulbi) | 6 |
| Choroidal melanoma | 10 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Leister, N.; Löser, J.; Gostian, A.-O.; Gostian, M.; Rokohl, A.C.; Fieber, M.A.; Alkan, D.; Schumacher, C.; Löw, V.; Gordon, E.; et al. Postoperative Pain Following Eye Enucleation: A Prospective Observational Study. Medicina 2024, 60, 614. https://doi.org/10.3390/medicina60040614
Leister N, Löser J, Gostian A-O, Gostian M, Rokohl AC, Fieber MA, Alkan D, Schumacher C, Löw V, Gordon E, et al. Postoperative Pain Following Eye Enucleation: A Prospective Observational Study. Medicina. 2024; 60(4):614. https://doi.org/10.3390/medicina60040614
Chicago/Turabian StyleLeister, Nicolas, Johannes Löser, Antoniu-Oreste Gostian, Magdalena Gostian, Alexander C. Rokohl, Marc A. Fieber, Deniz Alkan, Christine Schumacher, Vanessa Löw, Erik Gordon, and et al. 2024. "Postoperative Pain Following Eye Enucleation: A Prospective Observational Study" Medicina 60, no. 4: 614. https://doi.org/10.3390/medicina60040614