
Findings and Outcome of Transcatheter Right Ventricular Endomyocardial Biopsy and Hemodynamic Assessment in Children with Suspected Myocarditis or Cardiomyopathy

 , , and
, , and
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Cardiac Catheterisation
2.3. Clinical Data
2.4. Histological/Immunohistological Analyses
2.5. Statistics and Ethics
3. Results
3.1. Clinical, Echocardiographic Findings and Cardiac Biomarker at Hospital Admission
3.2. Periprocedural Management
3.3. Histological Findings
3.4. Diagnostic and Therapeutical Impact of Right Ventricular Endomyocardial Biopsy
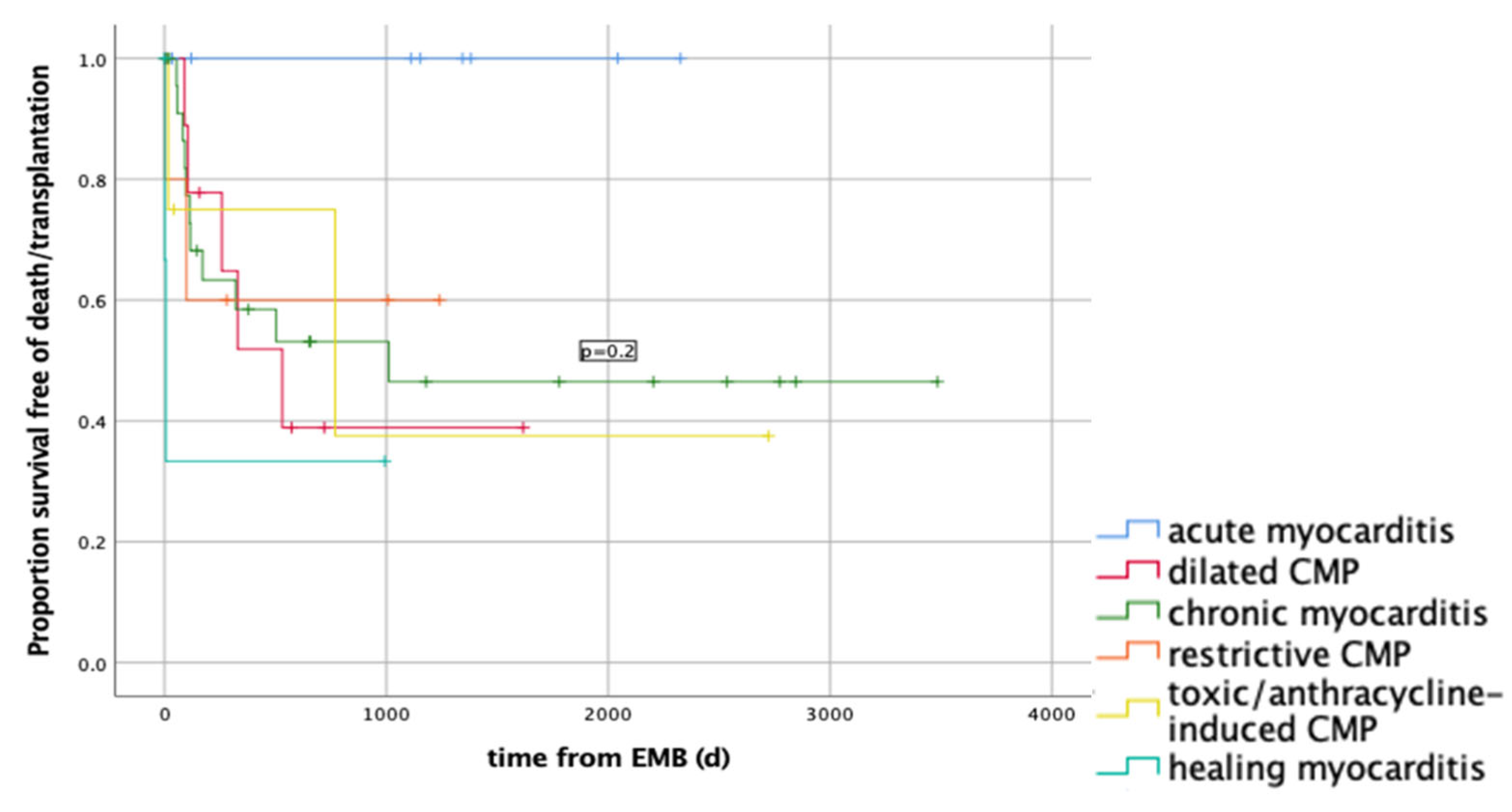
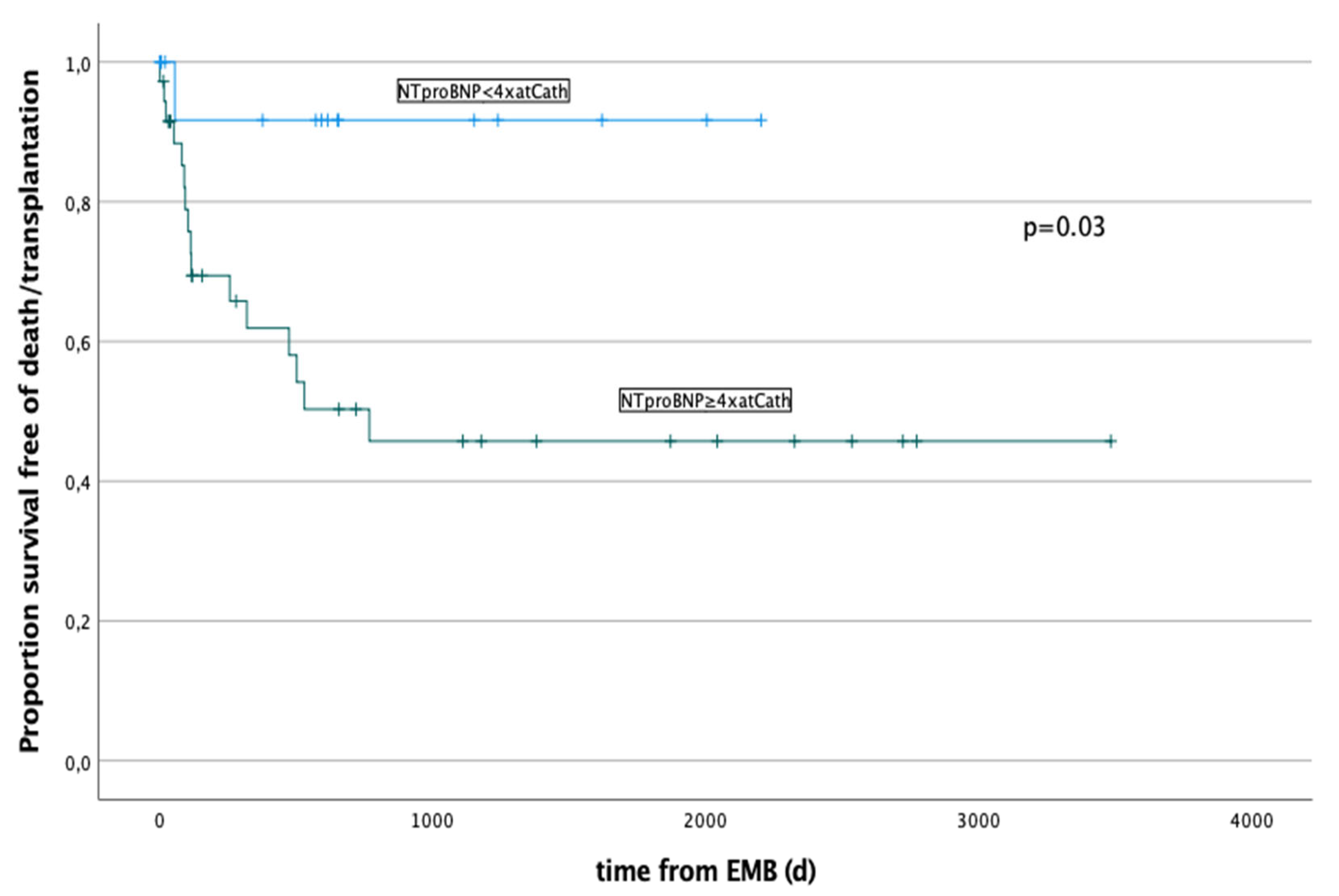
3.5. Outcome and Outcome’s Predictors
4. Discussion
4.1. Periprocedural Anaesthesiologic Management
4.2. Complications during CC and RV-EMB
4.3. Histological and Serological Findings
4.4. Outcome and Outcome’s Predictors
4.5. Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Ghelani, S.J.; Spaeder, M.C.; Pastor, W.; Spurney, C.F.; Klugman, D. Demographics, trends, and outcomes in pediatric acute myocarditis in the United States, 2006 to 2011. Circ. Cardiovasc. Qual. Outcomes 2012, 5, 622–627. [Google Scholar] [CrossRef] [PubMed]
- Durani, Y.; Giordano, K.; Goudie, B.W. Myocarditis and Pericarditis in Children. Pediatr. Clin. N. Am. 2010, 57, 1281–1303. [Google Scholar] [CrossRef] [PubMed]
- Ammirati, E.; Veronese, G.; Cipriani, M.; Moroni, F.; Garascia, A.; Brambatti, M.; Adler, E.D.; Frigerio, M. Acute and Fulminant Myocarditis: A Pragmatic Clinical Approach to Diagnosis and Treatment. Curr. Cardiol. Rep. 2018, 20, 114. [Google Scholar] [CrossRef] [PubMed]
- Ammirati, E.; Veronese, G.; Bottiroli, M.; Wang, D.W.; Cipriani, M.; Garascia, A.; Pedrotti, P.; Adler, E.D.; Frigerio, M. Update on Acute Myocarditis. Trends Cardiovasc. Med. 2020; Epub ahead of print. [Google Scholar]
- Rodriguez-Gonzalez, M.; Sanchez-Codez, M.I.; Lubian-Gutierrez, M.; Castellano-Martinez, A. Clinical presentation and early predictors for poor outcomes in pediatric myocarditis: A retrospective study. World J. Clin. Cases 2019, 7, 548–561. [Google Scholar] [CrossRef] [PubMed]
- Ammirati, E.; Kaski, J.P. Resident inflammatory cells in the myocardium of children: On the way to set histologic reference standards to differentiate normal myocardium from myocarditis. Int. J. Cardiol. 2020, 303, 64–65. [Google Scholar] [CrossRef]
- Teele, S.A.; Allan, C.K.; Laussen, P.C.; Newburger, J.W.; Gauvreau, K.; Thiagarajan, R.R. Management and outcomes in pediatric patients presenting with acute fulminant myocarditis. J. Pediatr. 2011, 158, 638–643.e1. [Google Scholar] [CrossRef]
- Canter, C.E.; Simpson, K.E.; Simpson, K.P. Diagnosis and treatment of myocarditis in children in the current era. Circulation 2014, 129, 115–128. [Google Scholar] [CrossRef]
- Alexander, P.M.A.; Nugent, A.W.; Daubeney, P.E.F.; Lee, K.J.; Sleeper, L.A.; Schuster, T.; Turner, C.; Davis, A.M.; Semsarian, C.; Colan, S.D.; et al. Long-Term Outcomes of Hypertrophic Cardiomyopathy Diagnosed During Childhood: Results From a National Population-Based Study. Circulation 2018, 138, 29–36. [Google Scholar] [CrossRef]
- Saji, T.; Matsuura, H.; Hasegawa, K.; Nishikawa, T.; Yamamoto, E.; Ohki, H.; Yasukochi, S.; Arakaki, Y.; Joo, K.; Nakazawa, M. Comparison of the Clinical Presentation, Treatment, and Outcome of Fulminant and Acute Myocarditis in Children. Circ. J. 2012, 76, 1222–1228. [Google Scholar] [CrossRef]
- Masarone, D.; Valente, F.; Rubino, M.; Vastarella, R.; Gravino, R.; Rea, A.; Russo, M.G.; Pacileo, G.; Limongelli, G. Pediatric Heart Failure: A Practical Guide to Diagnosis and Management. Pediatr. Neonatol. 2017, 58, 303–312. [Google Scholar] [CrossRef]
- Caforio, A.L.P.; Pankuweit, S.; Arbustini, E.; Basso, C.; Gimeno-Blanes, J.; Felix, S.B.; Fu, M.; Heliö, T.; Heymans, S.; Jahns, R.; et al. Current state of knowledge on aetiology, diagnosis, management, and therapy of myocarditis: A position statement of the European Society of Cardiology Working Group on Myocardial and Pericardial Diseases. Eur. Heart J. 2013, 34, 2636–2648, 2648a–2648d. [Google Scholar] [CrossRef]
- Mahrholdt, H.; Wagner, A.; Deluigi, C.C.; Kispert, E.; Hager, S.; Meinhardt, G.; Vogelsberg, H.; Fritz, P.; Dippon, J.; Bock, C.T.; et al. Presentation, patterns of myocardial damage, and clinical course of viral myocarditis. Circulation 2006, 114, 1581–1590. [Google Scholar] [CrossRef]
- Imanaka-Yoshida, K. Inflammation in myocardial disease: From myocarditis to dilated cardiomyopathy. Pathol. Int. 2020, 70, 1–11. [Google Scholar] [CrossRef]
- Li, G.; Fontaine, G.H.; Saguner, A.M. Endomyocardial biopsy in patients with acute myocarditis, idiopathic dilated cardiomyopathy, and arrhythmogenic right ventricular dysplasia. Int. J. Clin. Exp. Pathol. 2018, 11, 4270–4275. [Google Scholar]
- Pophal, S.G.; Sigfusson, G.; Booth, K.L.; Bacanu, S.A.; Webber, S.A.; Ettedgui, J.A.; Neches, W.H.; Park, S.C. Complications of endomyocardial biopsy in children. J. Am. Coll. Cardiol. 1999, 34, 2105–2110. [Google Scholar] [CrossRef]
- Cowley, C.G.; Lozier, J.S.; Orsmond, G.S.; Shaddy, R.E. Safety of endomyocardial biopsy in children. Cardiol. Young 2003, 13, 404–407. [Google Scholar] [CrossRef]
- Brighenti, M.; Donti, A.; Gagliardi, M.G.; Maschietto, N.; Marini, D.; Lombardi, M.; Vairo, U.; Agnoletti, G.; Milanesi, O.; Pongiglione, G.; et al. Endomyocardial biopsy safety and clinical yield in pediatric myocarditis: An Italian perspective. Catheter. Cardiovasc. Interv. 2016, 87, 762–767. [Google Scholar] [CrossRef]
- Webber, S.A.; Boyle, G.J.; Jaffe, R.; Pickering, R.M.; Beerman, L.B.; Fricker, F.J. Role of right ventricular endomyocardial biopsy in infants and children with suspected or possible myocarditis. Br. Heart J. 1994, 72, 360–363. [Google Scholar] [CrossRef]
- Chang, J.S.; Chiou, P.Y.; Yao, S.H.; Chou, I.C.; Lin, C.Y. Regression of Neonatal Cardiac Rhabdomyoma in Two Months Through Low-Dose Everolimus Therapy: A Report of Three Cases. Pediatr. Cardiol. 2017, 38, 1478–1484. [Google Scholar] [CrossRef]
- Pettersen, M.D.; Du, W.; Skeens, M.E.; Humes, R.A. Regression equations for calculation of z scores of cardiac structures in a large cohort of healthy infants, children, and adolescents: An echocardiographic study. J. Am. Soc. Echocardiogr. 2008, 21, 922–934. [Google Scholar] [CrossRef]
- Kindermann, I.; Kindermann, M.; Kandolf, R.; Klingel, K.; Bültmann, B.; Müller, T.; Lindinger, A.; Böhm, M. Predictors of outcome in patients with suspected myocarditis. Circulation 2008, 118, 639–648. [Google Scholar] [CrossRef] [PubMed]
- Richardson, P.; McKenna, W.; Bristow, M.; Maisch, B.; Mautner, B.; O’Connell, J.; Olsen, E.; Thiene, G.; Goodwin, J.; Gyarfas, I.; et al. Report of the 1995 World Health Organization/International Society and Federation of Cardiology Task Force on the Definition and Classification of cardiomyopathies. Circulation 1996, 93, 841–842. [Google Scholar] [PubMed]
- Lurz, P.; Eitel, I.; Adam, J.; Steiner, J.; Grothoff, M.; Desch, S.; Fuernau, G.; de Waha, S.; Sareban, M.; Luecke, C.; et al. Diagnostic Performance of CMR Imaging Compared With RV-EMB in Patients With Suspected Myocarditis. JACC Cardiovasc. Imaging 2012, 5, 513–524. [Google Scholar] [CrossRef] [PubMed]
- Baccouche, H.; Mahrholdt, H.; Meinhardt, G.; Merher, R.; Voehringer, M.; Hill, S.; Klingel, K.; Kandolf, R.; Sechtem, U.; Yilmaz, A. Diagnostic synergy of non-invasive cardiovascular magnetic resonance and invasive endomyocardial biopsy in troponin-positive patients without coronary artery disease. Eur. Heart J. 2009, 30, 2869–2879. [Google Scholar] [CrossRef]
- Bock, C.T.; Klingel, K.; Kandolf, R. Human parvovirus B19-associated myocarditis. N. Engl. J. Med. 2010, 362, 1248–1249. [Google Scholar] [CrossRef]
- Mueller, G.C.; Michel-Behnke, I.; Knirsch, W.; Haas, N.A.; Abdul-Khaliq, H.; Gitter, R. Feasibility, Safety and Diagnostic Impact of Endomyocardial Biopsies for the Diagnosis of Myocardial Disease in Children and Adolescents [Internet]. EuroIntervention. Available online: https://eurointervention.pcronline.com/article/feasibility-safety-and-diagnostic-impact-of-endomyocardial-biopsies-for-the-diagnosis-of-myocardial-disease-in-children-and-adolescents (accessed on 4 August 2022).
- Wagner, K.; Oliver, M.C.; Boyle, G.J.; Miller, S.A.; Law, Y.M.; Pigula, F.; Webber, S.A. Endomyocardial biopsy in pediatric heart transplant recipients: A useful exercise? (Analysis of 1169 biopsies). Pediatr. Transplant. 2000, 4, 186–192. [Google Scholar] [CrossRef]
- Daly, K.P.; Marshall, A.C.; Vincent, J.A.; Zuckerman, W.A.; Hoffman, T.M.; Canter, C.E.; Blume, E.D.; Bergersen, L. Endomyocardial biopsy and selective coronary angiography are low-risk procedures in pediatric heart transplant recipients: Results of a multicenter experience. J. Heart Lung Transplant. 2012, 31, 398–409. [Google Scholar] [CrossRef]
- Das, B.B. Role of endomyocardial biopsy for children presenting with acute systolic heart failure. Pediatr. Cardiol. 2014, 35, 191–196. [Google Scholar] [CrossRef]
- Jayaram, N.; Spertus, J.A.; Kennedy, K.F.; Vincent, R.; Martin, G.R.; Curtis, J.P.; Nykanen, D.; Moore, P.M.; Bergersen, L. Modeling Major Adverse Outcomes of Pediatric and Adult Patients With Congenital Heart Disease Undergoing Cardiac Catheterization: Observations From the NCDR IMPACT Registry (National Cardiovascular Data Registry Improving Pediatric and Adult Congenital Treatment). Circulation 2017, 136, 2009–2019. [Google Scholar]
- Holzmann, M.; Nicko, A.; Kühl, U.; Noutsias, M.; Poller, W.; Hoffmann, W.; Morguet, A.; Witzenbichler, B.; Tschöpe, C.; Schultheiss, H.P.; et al. Complication Rate of Right Ventricular Endomyocardial Biopsy via the Femoral Approach: A Retrospective and Prospective Study Analyzing 3048 Diagnostic Procedures Over an 11-Year Period. Circulation 2008, 118, 1722–1728. [Google Scholar] [CrossRef]
- Foerster, S.R.; Canter, C.E.; Cinar, A.; Sleeper, L.A.; Webber, S.A.; Pahl, E.; Kantor, P.F.; Alvarez, J.A.; Colan, S.D.; Jefferies, J.L.; et al. Ventricular remodeling and survival are more favorable for myocarditis than for idiopathic dilated cardiomyopathy in childhood: An outcomes study from the Pediatric Cardiomyopathy Registry. Circ. Heart Fail. 2010, 3, 689–697. [Google Scholar] [CrossRef]
- Hill, K.D.; Atkinson, J.B.; Doyle, T.P.; Dodd, D. Routine performance of endomyocardial biopsy decreases the incidence of orthotopic heart transplant for myocarditis. J. Heart Lung Transplant. 2009, 28, 1261–1266. [Google Scholar] [CrossRef]
- Pietra, B.A.; Kantor, P.F.; Bartlett, H.L.; Chin, C.; Canter, C.E.; Larsen, R.L.; Edens, R.E.; Colan, S.D.; Towbin, J.A.; Lipshultz, S.E.; et al. Early Predictors of Survival to and After Heart Transplantation in Children with Dilated Cardiomyopathy. Circulation 2012, 126, 1079–1086. [Google Scholar] [CrossRef]
- Sachdeva, S.; Song, X.; Dham, N.; Heath, D.M.; DeBiasi, R.L. Analysis of clinical parameters and cardiac magnetic resonance imaging as predictors of outcome in pediatric myocarditis. Am. J. Cardiol. 2015, 115, 499–504. [Google Scholar] [CrossRef]
- Schultz, J.C.; Hilliard, A.A.; Cooper, L.T.; Rihal, C.S. Diagnosis and Treatment of Viral Myocarditis. Mayo Clin. Proc. 2009, 84, 1001–1009. [Google Scholar] [CrossRef]
- Magnani, J.W.; Danik, H.J.S.; Dec, G.W.; DiSalvo, T.G. Survival in biopsy-proven myocarditis: A long-term retrospective analysis of the histopathologic, clinical, and hemodynamic predictors. Am. Heart J. 2006, 151, 463–470. [Google Scholar] [CrossRef]
- Yoldaş, T.; Örün, U.A. What is the Significance of Elevated Troponin I in Children and Adolescents? A Diagnostic Approach. Pediatr. Cardiol. 2019, 40, 1638–1644. [Google Scholar] [CrossRef]
- Chen, W.C.; Tran, K.D.; Maisel, A.S. Biomarkers in heart failure. Heart 2010, 96, 314–320. [Google Scholar] [CrossRef][Green Version]
- Abrar, S.; Ansari, M.J.; Mittal, M.; Kushwaha, K.P. Predictors of Mortality in Paediatric Myocarditis. J. Clin. Diagn Res. 2016, 10, SC12–SC16. [Google Scholar] [CrossRef]
- Miller, W.L.; Hartman, K.A.; Burritt, M.F.; Burnett, J.C.; Jaffe, A.S. Troponin, B-type natriuretic peptides and outcomes in severe heart failure: Differences between ischemic and dilated cardiomyopathies. Clin Cardiol. 2007, 30, 245–250. [Google Scholar] [CrossRef]
- Noori, N.M.; Mahjoubifard, M.; Shahramian, I.; Teimouri, A.; Jahangirifard, A. Comparison between procalcitonin, brain natriuretic peptide, and uric acid in children with cardiomyopathy and controls. Biomed. Res. Int. 2015, 2015, 510450. [Google Scholar] [CrossRef] [PubMed]
- Sitte, V.; Burkhardt, B.; Weber, R.; Kretschmar, O.; Hersberger, M.; Bergsträsser, E.; Christmann, M. Advanced Imaging and New Cardiac Biomarkers in Long-term Follow-up After Childhood Cancer. J. Pediatr. Hematol. Oncol. 2021, 44, e374–e380. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Median (IQR)/n (%) | |
|---|---|
| Patients caractheristics | 81 (100) |
| Age (years) | 6.8 (9.9) |
| Weight (kg) | 20.0 (32.2) |
| Body surface area (BSA) | 0.8 (0.8) |
| Clinical symptoms | 6 (7) |
| Fatigue (n) | 55 (65) |
| Tachypnoea (n) | 46 (54) |
| Cardiac murmur (n) | 43 (51) |
| Hepatomegaly (n) | 39 (46) |
| Tachycardia (n) | 34 (40) |
| Cardiopulmonary decompensation (n) | 18 (21) |
| Echocardiographic findings | |
| LV-ejection fraction (EF) (%) | 35 (28) |
| LV-SF of 20% (%) | 20 (16.5) |
| LVEDD z-score | +2.61 (3.73) |
| LVES z-score | +4.30 (4.83) |
| Complications | Median (IQR)/n (%) |
|---|---|
| 3 (3) |
| Myocardial perforation | 2 (2) |
| Temporary complete AV block | 1 (1) |
| 6 (7) |
| Hemodynamic findings | |
| LVEDP (mmHg) | 17 (9) |
| LAP (mmHg) | 15 (10) |
| mPAP ≥ 25 mmHg (n) | 33 (34) |
| PVR (Wood Units/m2) | 1.83 (1.87) |
| ScvO2 (%) | 70 (13) |
| PCR from RV-EMB (n = 79) | n | % |
Positive
| 16 1 | 20 1 |
| 1 | 1 |
| 7 | 9 |
| 6 | 8 |
| 1 | 1 |
| Negative | 63 | 80 |
| PCR from peripheral lymphocytes (n = 77) | n | % |
Positive
| 33 1 | 43 1 |
| 3 | 4 |
| 4 | 5 |
| 1 | 1 |
| 1 | 1 |
| 2 | 3 |
| 8 | 10 |
| 2 | 3 |
| 6 | 8 |
| 1 | 1 |
| Negative | 44 | 57 |
| Positive PCR from RV-EMB in myocarditis cases (n = 42) | n/n | % |
| Myocarditis | 14/42 | 33 |
| 7/28 | 25 |
| 2/5 | 40 |
| 5/9 | 56 |
| Same virus in RV-EMB and Lymphocytes | 9/77 | 12 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Callegari, A.; Quandt, D.; Schmitz, A.; Klingel, K.; Balmer, C.; Dave, H.; Kretschmar, O.; Knirsch, W. Findings and Outcome of Transcatheter Right Ventricular Endomyocardial Biopsy and Hemodynamic Assessment in Children with Suspected Myocarditis or Cardiomyopathy. Int. J. Environ. Res. Public Health 2022, 19, 10406. https://doi.org/10.3390/ijerph191610406
Callegari A, Quandt D, Schmitz A, Klingel K, Balmer C, Dave H, Kretschmar O, Knirsch W. Findings and Outcome of Transcatheter Right Ventricular Endomyocardial Biopsy and Hemodynamic Assessment in Children with Suspected Myocarditis or Cardiomyopathy. International Journal of Environmental Research and Public Health. 2022; 19(16):10406. https://doi.org/10.3390/ijerph191610406
Chicago/Turabian StyleCallegari, Alessia, Daniel Quandt, Achim Schmitz, Karin Klingel, Christian Balmer, Hitendu Dave, Oliver Kretschmar, and Walter Knirsch. 2022. "Findings and Outcome of Transcatheter Right Ventricular Endomyocardial Biopsy and Hemodynamic Assessment in Children with Suspected Myocarditis or Cardiomyopathy" International Journal of Environmental Research and Public Health 19, no. 16: 10406. https://doi.org/10.3390/ijerph191610406
APA StyleCallegari, A., Quandt, D., Schmitz, A., Klingel, K., Balmer, C., Dave, H., Kretschmar, O., & Knirsch, W. (2022). Findings and Outcome of Transcatheter Right Ventricular Endomyocardial Biopsy and Hemodynamic Assessment in Children with Suspected Myocarditis or Cardiomyopathy. International Journal of Environmental Research and Public Health, 19(16), 10406. https://doi.org/10.3390/ijerph191610406