
Evaluation of Oral Mucosal Lesions Using the IllumiScan® Fluorescence Visualisation Device: Distinguishing Squamous Cell Carcinoma

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
Statistical Analysis
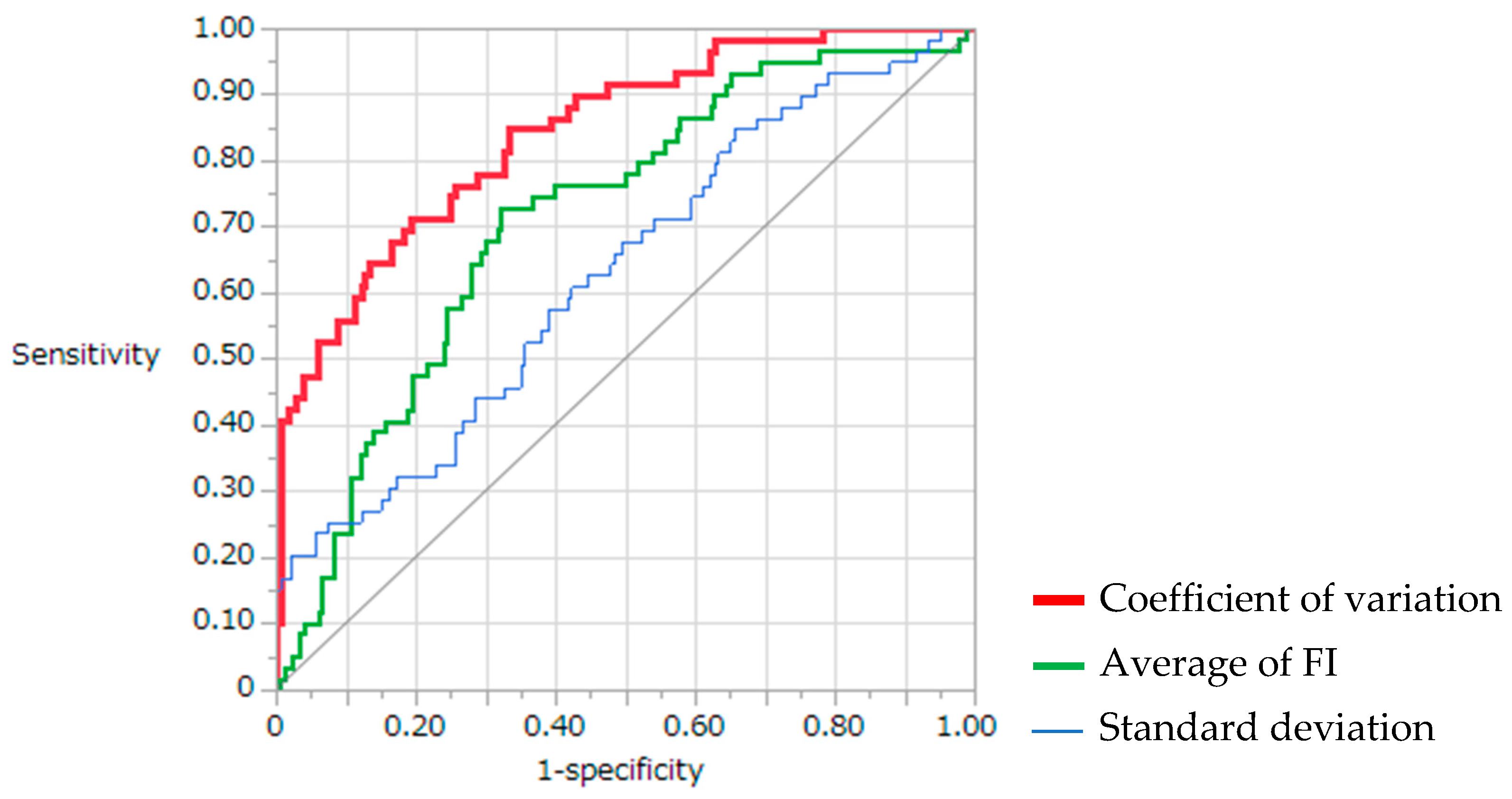
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Nakanishi, Y.; Ochiai, A.; Yoshimura, K.; Kato, H.; Shimoda, T.; Yamaguchi, H.; Tachimori, Y.; Watanabe, H.; Hirohashi, S. The Clinicopathologic Significance of Small Areas Unstained by Lugol’s Iodine in the Mucosa Surrounding Resected Esophageal Carcinoma: An Analysis of 147 Cases. Cancer 1998, 82, 1454–1459. [Google Scholar] [CrossRef]
- Epstein, J.B.; Scully, C.; Spinelli, J. Toluidine Blue and Lugol’s Iodine Application in the Assessment of Oral Malignant Disease and Lesions at Risk of Malignancy. J. Oral Pathol. Med. 1992, 21, 160–163. [Google Scholar] [CrossRef] [PubMed]
- Alsarraf, A.H.; Kujan, O.; Farah, C.S. The utility of oral brush cytology in the early detection of oral cancer and oral potentially malignant disorders: A systematic review. J. Oral Pathol. Med. 2018, 47, 104–116. [Google Scholar] [CrossRef] [PubMed]
- Nagi, R.; Reddy-Kantharaj, Y.B.; Rakesh, N.; Janardhan-Reddy, S.; Sahu, S. Efficacy of Light Based Detection Systems for Early Detection of Oral Cancer and Oral Potentially Malignant Disorders: Systematic Review. Med. Oral Patol. Oral Cir. Bucal. 2016, 21, e447–e455. [Google Scholar] [CrossRef]
- Silverman, S.J.; Barbosa, J.; Kearns, G. Ultrastructural and Histochemical Localization of Glycogen in Human Normal and Hyperkeratotic Oral Epithelium. Arch. Oral Biol. 1971, 16, 423–434. [Google Scholar] [CrossRef]
- Acha, A.; Ruesga, M.T.; Rodríguez, M.J.; Martínez de Pancorbo, M.A.; Aguirre, J.M. Applications of the Oral Scraped (Exfoliative) Cytology in Oral Cancer and Precancer. Med. Oral Patol. Oral Cir. Bucal. 2005, 10, 95–102. [Google Scholar]
- Mehrotra, R.; Singh, M.; Thomas, S.; Nair, P.; Pandya, S.; Nigam, N.S.; Shukla, P. A Cross-Sectional Study Evaluating Chemiluminescence and Autofluorescence in the Detection of Clinically Innocuous Precancerous and Cancerous Oral Lesions. J. Am. Dent. Assoc. 2010, 141, 151–156. [Google Scholar] [CrossRef]
- Lima, I.F.P.; Brand, L.M.; de Figueiredo, J.A.P.; Steier, L.; Lamers, M.L. Use of Autofluorescence and Fluorescent Probes as a Potential Diagnostic Tool for Oral Cancer: A Systematic Review. Photodiagnosis. Photodyn. Ther. 2021, 33, 102073. [Google Scholar] [CrossRef]
- Epstein, J.B.; Güneri, P.; Boyacioglu, H.; Abt, E. The Limitations of the Clinical Oral Examination in Detecting Dysplastic Oral Lesions and Oral Squamous Cell Carcinoma. J. Am. Dent. Assoc. 2012, 143, 1332–1342. [Google Scholar] [CrossRef]
- Paderni, C.; Compilato, D.; Carinci, F.; Nardi, G.; Rodolico, V.; Lo Muzio, L.; Spinelli, G.; Mazzotta, M.; Campisi, G. Direct Visualization of Oral-Cavity Tissue Fluorescence as Novel Aid for Early Oral Cancer Diagnosis and Potentially Malignant Disorders Monitoring. Int. J. Immunopathol. Pharmacol. 2011, 24, 121–128. [Google Scholar] [CrossRef] [Green Version]
- Warburg, O. On the Origin of Cancer Cells. Science 1956, 123, 309–314. [Google Scholar] [CrossRef] [PubMed]
- Sumi, S.; Umemura, N.; Adachi, M.; Ohta, T.; Naganawa, K.; Kawaki, H.; Takayama, E.; Kondoh, N.; Sumitomo, S. The Luminance Ratio of Autofluorescence in a Xenograft Mouse Model Is Stable Through Tumor Growth Stages. Clin. Exp. Dent. Res. 2018, 4, 174–181. [Google Scholar] [CrossRef] [PubMed]
- Richards-Kortum, R.; Sevick-Muraca, E. Quantitative Optical Spectroscopy for Tissue Diagnosis. Annu. Rev. Phys. Chem. 1996, 47, 555–606. [Google Scholar] [CrossRef] [Green Version]
- Svistun, E.; Alizadeh-Naderi, R.; El-Naggar, A.; Jacob, R.; Gillenwater, A.; Richards-Kortum, R. Vision Enhancement System for Detection of Oral Cavity Neoplasia Based on Autofluorescence. Head Neck. 2004, 26, 205–215. [Google Scholar] [CrossRef]
- Brandwein-Gensler, M.; Teixeira, M.S.; Lewis, C.M.; Lee, B.; Rolnitzky, L.; Hille, J.J.; Genden, E.; Urken, M.L.; Wang, B.Y. Oral Squamous Cell Carcinoma: Histologic Risk Assessment, but Not Margin Status, Is Strongly Predictive of Local Disease-Free and Overall Survival. Am. J. Surg. Pathol. 2005, 29, 167–178. [Google Scholar] [CrossRef] [PubMed]
- Sopka, D.M.; Li, T.; Lango, M.N.; Mehra, R.; Liu, J.C.J.; Burtness, B.; Flieder, D.B.; Ridge, J.A.; Galloway, T.J. Dysplasia at the Margin? Investigating the Case for Subsequent Therapy in ‘Low-Risk’ Squamous Cell Carcinoma of the Oral Tongue. Oral Oncol. 2013, 49, 1083–1087. [Google Scholar] [CrossRef] [Green Version]
- Wang, C.; Qi, X.; Zhou, X.; Liu, H.; Li, M. Diagnostic value of objective VELscope fluorescence methods in distinguishing oral cancer from oral potentially malignant disorders (OPMDs). Transl. Cancer Res. 2022, 11, 1603–1615. [Google Scholar] [CrossRef] [PubMed]
- Meleti, M.; Giovannacci, I.; Vescovi, P.; Pedrazzi, G.; Govoni, P.; Magnoni, C. Histopathological Determinants of Autofluorescence Patterns in Oral Carcinoma. Oral Dis. 2020, 26, 1185–1189. [Google Scholar] [CrossRef]
- Kikuta, S.; Iwanaga, J.; Todoroki, K.; Shinozaki, K.; Tanoue, R.; Nakamura, M.; Kusukawa, J. Clinical Application of the IllumiScan Fluorescence Visualization Device in Detecting Oral Mucosal Lesions. Cureus 2018, 10, e3111. [Google Scholar] [CrossRef] [Green Version]
- Ganga, R.S.; Gundre, D.; Bansal, S.; Shirsat, P.M.; Prasad, P.; Desai, R.S. Evaluation of the Diagnostic Efficacy and Spectrum of Autofluorescence of Benign, Dysplastic and Malignant Lesion of the Oral Cavity Using VELscope. Oral Oncol. 2017, 75, 67–74. [Google Scholar] [CrossRef]
- Sreeshyla, H.S.; Jaishankar, H.P.; Shashidara, R.; Usha, H.; Priyanka, N.; Premalatha, B.R.; Srinivas, J. VELscope-Tissue Fluorescence Based Diagnostic Aid in Oral Precancer and Cancer. JMDR 2020, 6, 41–46. [Google Scholar] [CrossRef]
- Abati, S.; Bramati, C.; Bondi, S.; Lissoni, A.; Trimarchi, M. Oral Cancer and Precancer: A Narrative Review on the Relevance of Early Diagnosis. Int. J. Environ. Res. Public Health 2020, 17, 9160. [Google Scholar] [CrossRef] [PubMed]
- Vibhute, N.A.; Jagtap, S.V.; Patil, S.V. Velscope guided oral cancer screening: A ray of hope in early oral cancer diagnosis. J. Oral Maxillofac. Pathol. 2022, 25, 3. [Google Scholar] [CrossRef]
- Ono, K.; Maeyama, E.; Bessho, H.; Yamamoto, N.; Yoshida, S.; Watanabe, A.; Sugahara, K.; Nishiyama, A.; Takagi, R.; Kasahara, K.; et al. Evaluating the practicality of the 8th edition of TNM classification using cases of oral squamous cell carcinoma. Shikwa Gakuho. 2019, 119, 97–104. [Google Scholar] [CrossRef]
- Sugahara, K.; Futoo, E.; Bessho, H.; Sekine, R.; Ohno, K.; Katakura, A.; Shibahara, T. Fluorescence visualization for oral mucosa using an auto-fluorescence imaging analysis software. Jpn. J. Oral Diag. 2017, 30, 168–175. [Google Scholar] [CrossRef]
- Ganjoho.jp. Available online: https://ganjoho.jp/reg_stat/statistics/stat/cancer/3_oral.html (accessed on 10 March 2022).
- Amirchaghmaghi, M.; Mohtasham, N.; Delavarian, Z.; Shakeri, M.T.; Hatami, M.; Mosannen Mozafari, P.M. The Diagnostic Value of the Native Fluorescence Visualization Device for Early Detection of Premalignant/Malignant Lesions of the Oral Cavity. Photodiagnosis. Photodyn. Ther. 2018, 21, 19–27. [Google Scholar] [CrossRef] [PubMed]
- Shah, S.; Waknis, P.; Saha, A.; Setiya, S.; Ratra, T.; Vaswani, V. The use of Velscope to assess cellular changes occurring in oral premalignancy. J. Oral Biol. Craniofacial Res. 2020, 10, 99–103. [Google Scholar] [CrossRef] [PubMed]
- Simonato, L.E.; Tomo, S.; Miyahara, G.I.; Navarro, R.S.; Villaverde, A.G.J.B. Fluorescence Visualization Efficacy for Detecting Oral Lesions More Prone to Be Dysplastic and Potentially Malignant Disorder: A Pilot Study. Photodiagn. Photodyn. Ther. 2017, 17, 1–4. [Google Scholar] [CrossRef]
- Mazur, M.; Ndokaj, A.; Venugopal, D.C.; Roberto, M.; Albu, C.; Jedliński, M.; Tomao, S.; Vozza, I.; Trybek, G.; Ottolenghi, L.; et al. In Vivo Imaging-Based Techniques for Early Diagnosis of Oral Potentially Malignant Disorders-Systematic Review and Meta-Analysis. Int. J. Environ. Res. Public Health 2021, 18, 11775. [Google Scholar] [CrossRef]
- Ikeda, Y.; Suzuki, T.; Saitou, H.; Ogane, S.; Hashimoto, K.; Takano, N.; Nomura, T. Usefulness of fluorescence visualization-guided surgery for early-stage tongue squamous cell carcinoma compared to iodine vital staining. Int. J. Clin. Oncol. 2020, 25, 1604–1611. [Google Scholar] [CrossRef]
- Cicciù, M.; Cervino, G.; Fiorillo, L.; D’Amico, C.; Oteri, G.; Troiano, G.; Zhurakivska, K.; Lo Muzio, L.; Herford, A.S.; Crimi, S.; et al. Early Diagnosis on Oral and Potentially Oral Malignant Lesions: A Systematic Review on the VELscope Fluorescence Method. Dent. J. 2019, 7, 93. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jain, S.; Jain, K.; Bais, P.S.; Shinkar, S.V.; Saify, F. Role of fluorescence imaging device in screening of oral cancer: A cross-sectional study in Chhattisgarh population. Indian J. Community Med. 2021, 46, 622–625. [Google Scholar] [CrossRef] [PubMed]
- Burian, E.; Schulz, C.; Probst, F.; Palla, B.; Tröltzsch, M.; Maglitto, F.; Califano, L.; Ehrenfeld, M.; Otto, S. Fluorescence Based Characterization of Early Oral Squamous Cell Carcinoma Using the Visually Enhanced Light Scope Technique. J. Craniomaxillofac. Surg. 2017, 45, 1526–1530. [Google Scholar] [CrossRef] [PubMed]
- Laronde, D.M.; Williams, P.M.; Hislop, T.G.; Poh, C.; Ng, S.; Bajdik, C.; Zhang, L.; MacAulay, C.; Rosin, M.P. Influence of Fluorescence on Screening Decisions for Oral Mucosal Lesions in Community Dental Practices. J. Oral Pathol. Med. 2014, 43, 7–13. [Google Scholar] [CrossRef]
- Heppner, G.H. Tumor heterogeneity. Cancer Res. 1984, 44, 2259–2265. [Google Scholar]
- Kosugi, A.; Kasahara, M.; Yang, L.; Nakamura-Takahashi, A.; Shibahara, T.; Mori, T. Method for Diagnosing Neoplastic Lesions by Quantitative Fluorescence Value. Sci. Rep. 2019, 9, 7833. [Google Scholar] [CrossRef] [Green Version]
- Masuda, H.; Yamamoto, N.; Shibahara, T. Early Detection of Leukoplakic Oral Squamous Cell Carcinoma Using 4NQO-induced Rat Tongue Cancer Model: Study Utilizing Fluorescence Intensity and Histopathological Evaluation. Bull. Tokyo Dent. Coll. 2022, 63, 1–12. [Google Scholar] [CrossRef]
- Kozakai, A.; Ono, K.; Nomura, T.; Takano, N.; Takano, N.; Shibahara, T. Usefulness of objective evaluations by fluorescence visualization device for differentiating between superficial oral squamous cell carcinoma and oral lichen planus. J. Oral Maxillofac. Surg. Med. Pathol. 2020, 32, 26–32. [Google Scholar] [CrossRef]
- Morikawa, T.; Kosugi, A.; Shibahara, T. The Utility of Optical Instrument “ORALOOK” in the Early Detection of High-risk Oral Mucosal Lesions. Anticancer Res. 2019, 39, 2519–2525. [Google Scholar] [CrossRef]
- Sugahara, K.; Koyama, Y.; Koyachi, M.; Matsunaga, S.; Odaka, K.; Kitamura, K.; Nakajima, K.; Matsuzaka, K.; Abe, S.; Katakura, A. Relationship Between the Immunohistological Examination and Fluorescence Visualization of Oral Squamous Cell Carcinoma. Oncol. Lett. 2020, 20, 2153–2160. [Google Scholar] [CrossRef]
- Morikawa, T.; Kozakai, A.; Kosugi, A.; Bessho, H.; Shibahara, T. Image Processing Analysis of Oral Cancer, Oral Potentially Malignant Disorders, and Other Oral Diseases Using Optical Instruments. Int. J. Oral Maxillofac. Surg. 2020, 49, 515–521. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Morikawa, T.; Bessho, H.; Kozakai, A.; Kosugi, A.; Shibahara, T. Analysis of Oral Squamous Cell Carcinoma and Oral Lichen planus Using the ‘IllumiScan’ Optical Instrument. Shikawa Gakuho. 2017, 117, 383–392. [Google Scholar]
- Rethman, M.P.; Carpenter, W.; Cohen, E.E.; Epstein, J.; Evans, C.A.; Flaitz, C.M.; Graham, F.J.; Hujoel, P.P.; Kalmar, J.R.; Koch, W.M.; et al. Evidence-Based Clinical Recommendations regarding Screening for Oral Squamous Cell Carcinomas. J. Am. Dent. Assoc. 2010, 141, 509–520. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
| Characteristics | SCC | Non-SCC | NOM |
|---|---|---|---|
| Total cases | 59 | 131 | 49 |
| Male | 35 | 50 | 30 |
| Female | 24 | 81 | 19 |
| Median age (range), year | 75 (39–98) | 70 (20–98) | 36 (25–94) |
| Median area, pixels | 5.13 × 104 | 2.09 × 104 | 8.50 × 104 |
| Topographic location | |||
| Buccal | 4 | 53 | 11 |
| Gum | 29 | 42 | 6 |
| Tongue | 21 | 34 | 26 |
| Floor of the mouth | 5 | 0 | 6 |
| Palate | 0 | 2 | 0 |
| Pathological diagnosis | |||
| Squamous cell carcinoma | 59 | ||
| Carcinoma in situ | 16 | ||
| Epithelial dysplasia | 22 | ||
| Hyperplasia | 10 | ||
| Oral lichen Planus | 64 | ||
| Inflammatory lesion | 19 |
| Univariate Analysis | Multivariate Analysis | |||
|---|---|---|---|---|
| p-Value | p-Value | Odds Ratio | 95% CI | |
| Sex, male/female | 0.0033 * | 0.39 | 1.43 | 0.63–3.25 |
| Age | 0.16 | 0.31 | 1.02 | 0.98–1.05 |
| Average of intensity | 0.013 * | 0.57 | 0.99 | 0.95–1.03 |
| Standard deviation | <0.0001 ** | 0.95 | 0.99 | 0.78–1.26 |
| Coefficient of variation × 10 | <0.0001 ** | 0.038 * | 13 | 1.09–154.7 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Taguchi, Y.; Toratani, S.; Matsui, K.; Hayashi, S.; Eboshida, N.; Hamada, A.; Ito, N.; Obayashi, F.; Kimura, N.; Yanamoto, S. Evaluation of Oral Mucosal Lesions Using the IllumiScan® Fluorescence Visualisation Device: Distinguishing Squamous Cell Carcinoma. Int. J. Environ. Res. Public Health 2022, 19, 10414. https://doi.org/10.3390/ijerph191610414
Taguchi Y, Toratani S, Matsui K, Hayashi S, Eboshida N, Hamada A, Ito N, Obayashi F, Kimura N, Yanamoto S. Evaluation of Oral Mucosal Lesions Using the IllumiScan® Fluorescence Visualisation Device: Distinguishing Squamous Cell Carcinoma. International Journal of Environmental Research and Public Health. 2022; 19(16):10414. https://doi.org/10.3390/ijerph191610414
Chicago/Turabian StyleTaguchi, Yuki, Shigeaki Toratani, Kensaku Matsui, Seiya Hayashi, Natsuki Eboshida, Atsuko Hamada, Nanako Ito, Fumitaka Obayashi, Naohiro Kimura, and Souichi Yanamoto. 2022. "Evaluation of Oral Mucosal Lesions Using the IllumiScan® Fluorescence Visualisation Device: Distinguishing Squamous Cell Carcinoma" International Journal of Environmental Research and Public Health 19, no. 16: 10414. https://doi.org/10.3390/ijerph191610414
APA StyleTaguchi, Y., Toratani, S., Matsui, K., Hayashi, S., Eboshida, N., Hamada, A., Ito, N., Obayashi, F., Kimura, N., & Yanamoto, S. (2022). Evaluation of Oral Mucosal Lesions Using the IllumiScan® Fluorescence Visualisation Device: Distinguishing Squamous Cell Carcinoma. International Journal of Environmental Research and Public Health, 19(16), 10414. https://doi.org/10.3390/ijerph191610414