Abstract
Objective: The aim of this paper is to assess parents’ knowledge about early orthodontic consultation and treatment, and to determine the association of this knowledge with number of children, monthly income, children’s age and perceived dental problems. Methods: A questionnaire was distributed to 3000 school children aged 6–11 years. The children were asked to take the questionnaire to their parents and bring it back the next day. It consisted of 13 questions. Some of these questions were related to the gender of the child, number of children, and parents’ monthly income. The remaining questions assessed the parents’ awareness of their children’s need for orthodontic treatment. Results: In total, 2538 parents completed the questionnaire. Of these, 2014 (79%) of the parents thought that their children’s teeth would have a significant impact on their personality. Moreover, 1637 (64.5%) parents thought that their children had a problem with their teeth; 1080 (66%) of these parents consulted a dentist. Of these 1080 parents, 821 (76%) consulted an orthodontist, and of these 821 parents, 449 (55%) initiated the required orthodontic treatment. The number of children who visited an orthodontist was found to increase with an increase in age (p = 0.0057). Moreover, a perceived overjet was associated with a higher number of orthodontic consultations (p = 0.0326). Conclusion: Although parents’ awareness regarding their children’s orthodontic treatment is important, other factors, such as the age of the child, the severity of the malocclusion and the consulted dentist, play a role in initiating orthodontic treatment.
1. Introduction
Occlusal development begins in the sixth week of intrauterine life and continues until 24 years of age. The sequence of development proceeds in an orderly and timely manner, which is controlled by environmental and genetic factors [1]. An aesthetic occlusion is important for an individual’s self-esteem, attractiveness and acceptance among peers [2,3,4]. Children with malocclusion are reported to be teased, bullied and socially rejected, which may lead to psychological problems [2,3,4]. It is important to diagnose and manage the developing occlusion during primary, mixed and permanent dentition [1]. Early treatment (during the transitional period) can reduce the severity of the malocclusion and the complexity of the treatment [1]. Orthodontic treatment has different effects, including improved aesthetics, function and psychosocial wellbeing [5,6].
Although most patients referred to orthodontic professionals are children, the preadolescent stage is also important as dental development occurs during this period. Moreover, seeking proper management during this period is critical to achieve better dentofacial health and function. Parents play a vital role in their children’s orthodontic management [2,7]. They choose orthodontic treatment to improve their children’s oral health function and reduce social stigma [2,7]. Previous studies revealed that parents who have been former orthodontic patients or are willing to undergo orthodontic treatment are more approving of this treatment for their children [8,9,10]. Malocclusion is not considered a dental problem by most parents [11]. Many factors play a major role in determining parents’ perceptions and attitudes towards seeking orthodontic care for their children. These include the funding of orthodontic treatment, socioeconomic status, ethnic origin, availability of resources, literacy rate and knowledge on malocclusion [12]. Therefore, as a result of lack of knowledge and awareness, parents may not seek orthodontic treatment at the right time for their children. The aim of the present study is to evaluate parents’ knowledge about early orthodontic consultation and treatment and the association of this knowledge with their level of education, number of children, children’s age and perceived dental problems.
2. Materials and Methods
The present cross-sectional study protocol was approved by the Institutional Review Board (19/0067/IRB), King Saud University, College of Medicine, Riyadh, Saudi Arabia., before beginning the study. The questionnaire used in the present study was taken from a previous study conducted by Hassan et al. [13]. A pilot study on 30 parents was first carried out to assess its clarity. Results of the pilot study revealed that the questionnaire was easy to understand and parents did not face any difficulty filling it in.
The distribution of questionnaire was conducted using stratified random sampling, in which Riyadh was divided into 5 regions, middle, east, west, south and north, to avoid selection bias. The questionnaire was distributed randomly to 3000 children belonging to schools in these different regions in Riyadh, Saudi Arabia, between December 2019 and February 2020. The inclusion criteria for those included in the study were male and female students aged 6–11 years (according to schools’ records). The exclusion criteria were male and female students younger than 6 and older than 11 years of age, and students with craniofacial anomalies and syndromes.
The students were asked to take the questionnaire to their parents and bring it back the next day. It consisted of 13 questions. Some of these questions were related to the gender of the child “since females found to be more concerned about their appearance”, number of children “as it affects the parents’ knowledge and experience than parents with one child”, and parents’ monthly income (“orthodontic treatment is not free for every case, parents with higher monthly income will be able to pay for their children treatment”). The remaining questions assessed the parents’ awareness of their children’s oral health and need for orthodontic treatment. The outcomes were the parent’s knowledge of their children’s early orthodontic consultation, as well as their oral health. The exposures were monthly income, age, perceived malalignment and perceived overjet.
2.1. Sample Size
The sample size was calculated using the R statistical package, version 3.3.1 (20 December 2018, © 2018, R Foundation for Statistical Computing, Vienna, Austria) [14]. Cochran’s sample size formula for prevalence studies was used to determine the proper sample size [15]. The expected proportion of participants who consulted an orthodontist for their perceived dental problems was determined according to the study of Alnaafa et al. [16], assuming a proportion of 72.6%. A more conservative expected proportion of 30% was considered in the present study.
At a 95% confidence interval and 2% margin of error, the estimated sample size was 2017 participants. An additional 50% contingency for non-response increased the sample size to 3000 participants.
2.2. Statistical Analysis
Data regarding the responses to the survey questions are presented as frequencies and percentages. Pearson’s chi-squared test of independence was used to assess whether the responses to two questions were independent of each other. The result was verified at p ≤ 0.05. The data were considered to be statistically significant if the p-value was less than 0.05. The regression logistic model was applied using the stepwise method of variable selection to understand which demographic characteristics had an effect on consulting a dentist or an orthodontist and the treatment adherence. The concordance index, which is a standard measure of the predictive accuracy of a logistic regression model, was calculated for each model. The statistical package used in the present study was R statistical package, version 3.3.1 (20 December 2018, © 2018, R Foundation for Statistical Computing Vienna, Austria) [14].
3. Results
Out of the 3000 parents, 2538 completed the questionnaire (Figure 1).
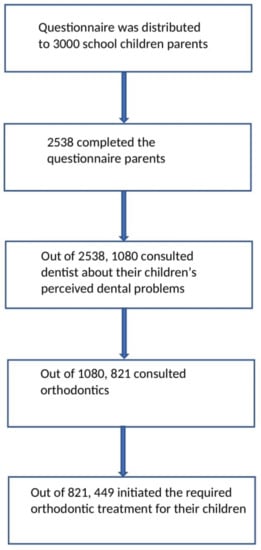
Figure 1.
Flow diagram of the questionnaire distribution and respondent.
Of these, 2414 (95%) were mothers and 149 (5%) were fathers. In total, 1374 (54%) of the children included in the present study were females and 1164 (46%) were males. Their mean age was 9.02 (±1.89) years (range: 6–11 years). Most children (860 (34%)) were aged 11 years. A total of 31% of the families had more than 4 children. Furthermore, 46% of the families had a monthly income between USD 2500–5000 (Table 1).

Table 1.
Demographic information and characteristics of participants in the study (n = 2538).
In total, 2014 (79%) of the parents thought that their children’s teeth would have a significant impact on their personality. While 1637 (64.5%) parents thought that their children had a problem with their teeth, 546 (33%) thought that their children’s teeth were not properly aligned; 1080 (66%) of these parents consulted a dentist regarding their children’s perceived dental problems. Of these 1080 parents, 821 (76%) consulted an orthodontist, and of these 821 parents, 449 (55%) initiated the required orthodontic treatment for their children (Table 2). No data was missing.
Table 2.
Responses of the participants regarding the perceived dental and orthodontic needs and consultation.
The association between the number of children per family and dental consultation was statistically insignificant (p = 0.6745), while the association between the monthly income of the family and dental consultation was statistically significant (p = 0.002) (Table 3).
Table 3.
Assessing the association between the demographic information and dentist consultation in children with perceived dental problems (N = 1637).
The Pearson’s chi-squared test revealed that none of the demographic data had a significant association with orthodontic consultation (p > 0.05). Forty percent of the parents who initiated the required orthodontic treatment for their children after the orthodontic consultation had more than four children. There was a statistically significant association between the number of children per family and initiating the required orthodontic treatment (p = 0.0039). The assessment of the association of age and perceived dental problems with the orthodontic consultation revealed that the number of children who consulted an orthodontist increased with an increase in age (p = 0.0057); 391 (79.63%) of the children were aged 11 years when they consulted an orthodontist. In addition, a perceived overjet was associated with a higher number of orthodontic consultations (p = 0.0326). The remaining perceived dental problems were not associated with orthodontic consultations (Table 4).
Table 4.
Assessing the association between age and perceived dental problems with orthodontist consultation in children (N = 1080).
Age and perceived dental problems were not associated with the initiation of orthodontic treatment (p < 0.05). Stepwise logistic regression analysis was performed to identify the predictors of dental consultation, orthodontic consultation and the initiation of the required orthodontic treatment. The results revealed that with each increase in the monthly income category of the family, the chance of consulting a dentist increased by 19%. With each increase in the age category, the chance of consulting an orthodontist increased by 11%. In addition, children with a perceived overjet were found to be 1.5 times more likely to consult an orthodontist than those without a perceived overjet. Children with perceived malalignment were found to be 1.25 times more likely to consult an orthodontist than those without perceived malalignment. The assessment of the predictors of initiating the required orthodontic treatment revealed that the chance of initiating the required orthodontic treatment increased by 16% with each increase in the age category. Moreover, the children with a perceived overjet were found to be 1.34 times more likely to initiate the required orthodontic treatment than those without a perceived overjet (Table 5).
Table 5.
Stepwise logistic regression.
4. Discussion
At present, preventive and interceptive treatment approaches play an important role in modern medicine. Interceptive orthodontics is defined as the phase of the science and art of orthodontics that is employed to recognize and eliminate potential irregularities and malpositions in the developing dentofacial complex [17]. Early orthodontic consultation is important for children. The American Association of Orthodontists states that the ideal time for a child to have his/her first orthodontic visit is at the age of 7 years [18]. Malocclusion can be caused by different factors, such as oral habits, dental anomalies and developmental position of the teeth. Periodontal problems, caries and temporomandibular joint problems can be caused by malocclusion [3]. Therefore, the awareness of malocclusion is extremely important. Most orthodontic patients are children and adolescents; therefore, their parents’ awareness of malocclusion is a very important factor influencing their motivation during orthodontic treatment [19].
In the present study, most parents believed that their children’s teeth would have a significant impact on their lives. This was in accordance with the findings of Hassan et al., [13] Alnaafa et al. [6] and Dann et al. [20], who reported that dentofacial appearance plays an important role in determining an individual’s attractiveness. In the present study, more than half of the parents 1637 (64.5%) reported that their children had a problem with their teeth; this was similar to the findings of previous studies [13,16,21]. Of these 1637 parents, 1080 (65.97%) consulted a dentist regarding the existing problems. Moreover, 821 (76.02%) of the 1080 parents consulted an orthodontist; this percentage was higher than that reported in previous studies [13,16]. This may be due to differences in the sample size.
The parents’ decision of initiating orthodontic treatment for their children is not merely their own and is affected by other factors, such as the dentist, speech therapist and other physicians [22]. Most (54.69%) parents who consulted an orthodontist reported that their children underwent orthodontic treatment. This was in accordance with the finding of Hassan et al.; in their study, 58.1% of the participants underwent orthodontic treatment [13].
In the present study, an association was noted between orthodontic consultation and the age of the child (p = 0.0057) and a perceived overjet (p = 0.0326); however, there was no effect of social class on orthodontic consultation. This was in accordance with the finding of a Finnish study, in which no association was noted between the orthodontic treatment and social class [23]. Meanwhile, King et al. reported that children with a high socio-economic status had a higher attendance for orthodontic consultations. However, their study had a low participation rate (143 (29%)) [24]. Kilpeläinen et al. reported that the parents of children with an overjet >7 mm were 5.5 times more likely to report that their children had been teased than those of children with a lesser overjet [25]. Dias and Gleiser found a relationship between crowding and increased overjet and orthodontic concern [26]. Similarly, we found that the parents of children with a perceived overjet were 1.5 times more likely to consult an orthodontist than those without a perceived overjet. The reason is that the increased overjet as well as crowding are at the anterior region, and this is usually associated with an unpleasing aesthetic [26].
In the present study, we found that the chance of consulting an orthodontist increased by 11% with each increase in the age category. Moreover, 79.63% of the children were aged 11 years when they consulted an orthodontist. The parents’ decision is important as the ability of a child to form his/her own opinion regarding orthodontic treatment is not developed until 10 to 11 years of age.
The present study has some limitations. The study included different parents belonging to different regions in Riyadh. In addition, the present study did not include questions assessing the parents’ knowledge about the right time to initiate orthodontic treatment. Future researchers should concentrate on evaluating parents’ knowledge about the right time to start orthodontic treatment, their knowledge about different types of orthodontic treatment options and awareness of the availability of different orthodontic appliances. The results of the current study cannot be generalized since a larger sample with parents from different regions and cities should be included.
5. Conclusions
In the present study, most parents believed that their children’s teeth would have a significant impact on their lives. The children’s age and a perceived overjet had an association with orthodontic consultation. Most (54.69%) parents who consulted an orthodontist reported that their children underwent orthodontic treatment. Children with a perceived overjet were found to be 1.5 times more likely to consult an orthodontist than those without a perceived overjet, while children with perceived malalignment were found to be 1.25 times more likely to consult an orthodontist than those without perceived malalignment. The orthodontic treatment predictors were age and a perceived overjet. With each increase in the age category, the chance of initiating the required orthodontic treatment increased by 16%. In addition, children with a perceived overjet were 1.34 times more likely to initiate the required orthodontic treatment than those without a perceived overjet. Although the parents’ awareness regarding their children’s orthodontic treatment is important, other factors, such as the age of the child, the severity of the malocclusion and the consulted dentist, play a role in initiating orthodontic treatment.
Author Contributions
Conceptualization, A.H.A. and A.A.B.G.; methodology, A.H.A. and A.A.B.G.; software, A.A.A. and B.M.A.; validation, A.H.A., A.A.A. and B.M.A.; formal analysis, S.F.A.; investigation, A.A.B.G. and S.F.A.; resources, A.H.A. and S.F.A.; data curation, A.H.A.; writing—original draft preparation, A.H.A., A.A.A. and B.M.A.; writing—review and editing, A.H.A., A.A.B.G. and S.F.A.; visualization, A.H.A.; supervision, A.H.A. and S.F.A.; project administration, A.A.B.G.; funding acquisition, S.F.A. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted according to the guidelines of the Declaration of Helsinki and approved by the present cross-sectional study protocol, which was approved by the Institutional Review Board (19/0067/IRB, 31 October 2019), King Saud University, College of Medicine, Riyadh, Saudi Arabia.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study (Table A1).
Data Availability Statement
Data supporting reported results are available upon request (Table A2).
Conflicts of Interest
The authors declare no conflict of interest.
Appendix A
Table A1.
Consent Form.
Table A1.
Consent Form.
| INFORMED CONSENT FOR QUESTIONNAIRE-BASED STUDYForm # KSU-REC 006QS-E King Saud University, Riyadh, Kingdom of Saudi Arabia | |
|---|---|
| Research Project Title: | Parents’ awareness of interceptive orthodontic treatment: a questionnaire study |
| Name of Principal Investigator: | Dr. Aljazi Aldweesh |
| Name and Address of Institution: | King Saud University |
| Contact No: | |
| Dear Participants, | |
| I would like to take this opportunity to ask if you are willing to take part in this questionnaire-based survey. Please answer the questions to the best of your knowledge. All the requested information in this study questionnaire will be treated as confidential. If you are willing to voluntarily participate in this study, please tick the appropriate box below and sign this form and you will be given a copy for your own records. | |
| Signed by: | |
| Investigator’s Complete Name: | |
| Study Designation: | |
| Signature: | |
| Date (dd/mm/yyyy): | |
| [ ] I agree to participate in this study survey, and to utilize the information for scientific research purposes. | |
| Signed by: | |
| Participant’s Name: | |
| Signature: | |
| Date (dd/mm/yyyy): | |
Table A2.
STROBE Checklist.
Table A2.
STROBE Checklist.
| Title and abstract | Item No | Recommendation | Page No |
| 1 | (a) Indicate the study’s design with a commonly used term in the title or the abstract | 1 | |
| (b) Provide in the abstract an informative and balanced summary of what was conducted and what was found | 1 | ||
| Introduction | |||
| Background/rationale | 2 | Explain the scientific background and rationale for the investigation being reported | 1 and 2 |
| Objectives | 3 | State the specific objectives, including any prespecified hypotheses | 2 |
| Methods | |||
| Study design | 4 | Present the key elements of the study design early in the paper | 2 |
| Setting | 5 | Describe the setting, locations and relevant dates, including the periods of recruitment, exposure, follow-up and data collection | 2 |
| Participants | 6 | (a) Give the eligibility criteria, and the sources and methods of selection of participants | 2 |
| Variables | 7 | Clearly define all outcomes, exposures, predictors, potential confounders and effect modifiers. Give the diagnostic criteria, if applicable | 2 |
| Data sources/measurement | 8 * | For each variable of interest, give sources of data and details of methods of assessment (measurement). Describe comparability of assessment methods if there is more than one group | NA |
| Bias | 9 | Describe any efforts to address the potential sources of bias | 2 |
| Study size | 10 | Explain how the study size was obtained | 2 |
| Quantitative variables | 11 | Explain how the quantitative variables were handled in the analyses. If applicable, describe which groupings were chosen and why | NA |
| Statistical methods | 12 | (a) Describe all the statistical methods, including those used to control for confounding | 3 |
| (b) Describe any methods used to examine the subgroups and interactions | 3 | ||
| (c) Explain how missing data were addressed | NA | ||
| (d) If applicable, describe the analytical methods taking account of sampling strategy | NA | ||
| (e) Describe any sensitivity analyses | NA | ||
| Results | |||
| Participants | 13 * | (a) Report the numbers of individuals at each stage of study, e.g., numbers potentially eligible, examined for eligibility, confirmed eligibility, included in the study, completing follow-up and analyzed | 3 and 4 |
| (b) Give reasons for non-participation at each stage | NA | ||
| (c) Consider the use of a flow diagram | 3 | ||
| Descriptive data | 14 * | (a) Present the characteristics of study participants (e.g., demographic, clinical, social) and information on the exposures and potential confounders | 4 |
| (b) Indicate the number of participants with missing data for each variable of interest | NA | ||
| Outcome data | 15 * | Report the numbers of the outcome events or summary measures | 4–7 |
| Main results | 16 | (a) Present the unadjusted estimates and, if applicable, confounder-adjusted estimates and their precision (e.g., 95% confidence interval). Make clear which confounders were adjusted for and why they were included | NA |
| (b) Report the category boundaries when continuous variables were categorized | 4–7 | ||
| (c) If relevant, consider translating the estimates of relative risk into absolute risk for a meaningful time period | NA | ||
| Other analyses | 17 | Report other analyses conducted, e.g., analyses of subgroups and interactions, and sensitivity analyses | NA |
| Discussion | |||
| Key results | 18 | Summarize the key results with reference to the study objectives | 7 and 8 |
| Limitations | 19 | Discuss the limitations of the study, taking into account the sources of potential bias or imprecision. Discuss both the direction and magnitude of any potential bias | 8 |
| Interpretation | 20 | Present a cautious overall interpretation of the results considering the objectives, limitations, multiplicity of analyses, results from similar studies and other relevant evidence | 7 and 8 |
| Generalizability | 21 | Discuss the generalizability (external validity) of the study results | 8 |
| Other information | |||
| Funding | 22 | Present the source of funding and the role of the funders for the present study and, if applicable, for the original study on which the present article is based | 8 |
* Give information separately for the exposed and unexposed groups. Note: “An Explanation and Elaboration” article discusses each checklist item and presents the methodological background and published examples of the transparent reporting. The STROBE checklist is best used in conjunction with this article (freely available on the Web sites of PLoS Medicine at www.plosmedicine.org Medicine at http://www.annals.org/, and Epidemiology at http://www.epidem.com/ accessed on 4 January 2022). Information on the STROBE Initiative is available at www.strobe-statement.org.
References
- Bahreman, A. Early-Age Orthodontic Treatment, Introduction, 1st ed.; Quintessence Pub Co.: Berlin, Germany, 2013. [Google Scholar]
- Al-Sarheed, M.; Bedi, R.; Hunt, N.P. The views and attitudes of parents of children with a sensory impairment towards orthodontic care. Eur. J. Orthod. 2004, 2, 87–91. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Abu Alhaija, E.S.; Al-Nimri, K.S.; Al-Khateeb, S.N. Self-perception of malocclusion among north Jordanian school children. Eur. J. Orthod. 2005, 27, 292–295. [Google Scholar] [CrossRef] [PubMed]
- Nagarajan, S.; Pushpanjali, K. The relationship of malocclusion as assessed by the Dental Aesthetic Index (DAI) with perceptions of aesthetics, function, speech and treatment needs among 14- to 15- year-old schoolchildren of Bangalore, India. Oral Health Prev. Dent. 2010, 8, 221–228. [Google Scholar] [PubMed]
- Abeleira, M.T.; Pazos, E.; Ramos, I.; Outumuro, M.; Limeres, J.; Seoane-Romero, J.; Diniz, M.; Diz, P. Orthodontic treatment for disabled children: A survey of parents’ attitudes and overall satisfaction. BMC Oral Health 2014, 14, 98. [Google Scholar] [CrossRef] [PubMed]
- Tessarollo, F.R.; Feldens, C.A.; Closs, L.Q. The impact of malocclusion on adolescents’ dissatisfaction with dental appearance and oral functions. Angle Orthod. 2012, 82, 403–409. [Google Scholar] [CrossRef] [PubMed]
- Pratelli, P.; Gelbier, S.; Gibbons, D.E. Parental perceptions and attitudes on orthodontic care. Br. J. Orthod. 1998, 25, 41–46. [Google Scholar] [CrossRef] [PubMed]
- Dogan, A.A.; Sari, E.; Uskun, E.; Saglam, A.M. Comparison of orthodontic treatment need by professionals and parents with different socio-demographic characteristics. Eur. J. Orthod. 2010, 32, 672–676. [Google Scholar] [CrossRef] [PubMed]
- Wedrychowska-Szulc, B.; Syrynska, M. Patient and parent motivation for orthodontic treatment—A questionnaire study. Eur. J. Orthod. 2010, 32, 447–452. [Google Scholar] [CrossRef] [PubMed]
- Momeni Danaei, S.; Salehi, P. Association between normative and self-perceived orthodontic treatment need among 12- to 15-year-old students in Shiraz, Iran. Eur. J. Orthod. 2010, 32, 530–534. [Google Scholar] [CrossRef] [PubMed]
- Siddegowda, R.; Rani, M.S. Awareness of orthodontic treatment in school children of Karnataka state—A survey. IOSR J. Appl. Phys. 2013, 4, 1–5. [Google Scholar] [CrossRef]
- Ulrich, K.; Aladar, B.; Andrej, Z. Dental esthetics, self-awareness, oral health related quality of life in young adults. Eur. J. Orthod. 2004, 26, 507–514. [Google Scholar]
- Hassan, F.; Shafique, U.; Mahmood, A. Parental motivation for orthodontic consultation during their child’s mixed dentition phase: A questionnaire study. Pak. Orthod. J. 2016, 7, 51–55. [Google Scholar]
- R Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2018; Available online: https://www.R-project.org/ (accessed on 4 July 2020).
- Cochran, W.G. Sampling Techniques, 3rd ed.; John Wiley & Sons Inc.: New York, NY, USA, 1977. [Google Scholar]
- Alnaafa, M.; Altamimi, Y.; Alajlan, S.; Alateeq, N.; Almarshedi, A.; Alsaleh, M.; Alsuwailem, R.; Patil, S.; Alam, M.K. The parental awareness regarding early orthodontic treatment in Hail city. Int. Med. J. 2020, 27, 220–223. [Google Scholar]
- Lahcen, O.; Laila, L. Early treatments in orthodontics. In Principles in Contemporary Orthodontics; Naretto, S., Ed.; InTech Publisher: London, UK, 2011; pp. 251–276. [Google Scholar]
- American Medical Association [Homepage on the Internet]. Chicago: The Association; c1995–2002 [Updated 2001 Aug 23; Cited 2002 Aug 12]. AMA Office of Group Practice Liaison; [About 2 Screens]. Available online: https://www3.aaoinfo.org/blog/parent-s-guide-post/first-visit/ (accessed on 10 June 2021).
- American Association of Orthodontics [Homepage on the Internet]. St. Louis Missouri: The Association; [Updated 2020 Nov 12; Cited 2021 May 6]. Early Orthodontic Care May Help You Avoid Costly Treatments. Available online: https://www.aaoinfo.org/blog/early-orthodontic-care-may-help-you-avoid-costly-treatments// (accessed on 10 June 2021).
- Moshkelgosha, V.; Kazemi, M.; Pakshir, H.; Safari, R. Parental knowledge and attitude towards early orthodontic treatment for their primary school children. Iran. J. Orthod. 2017, 12, e7377. [Google Scholar] [CrossRef]
- Dann, C.; Phillips, C.; Broder, H.L.; Tulloch, C. Self-concept, Class II malocclusion, and early treatment. Angle Orthod. 1995, 65, 411–416. [Google Scholar] [PubMed]
- Birkeland, K.; Bøe, O.E.; Wisth, P.J. Orthodontic concern among 11-year-old children and their parents compared with orthodontic treatment need assessed by index of orthodontic treatment need. Am. J. Orthod. Dentofac. Orthop. 1996, 110, 197–205. [Google Scholar] [CrossRef]
- Milen, A.; Tala, H.; Hausen, H. Dental Health Status, Habits and Care of Finnish Children and Youths in 1981–82: A Feasibility Study of An Information System; Health Services Research by the National Board of Health: Finland, Helsinki, 1986. [Google Scholar]
- King, T.; Jiang, Y.; Fowler, P.V.; Lee, M. Accessing orthodontic advice following referral: A survey of parents’ perceptions. N. Z. Dent. J. 2019, 115, 66–69. [Google Scholar]
- Kilpeläinen, P.V.; Phillips, C.; Tulloch, J.F. Anterior tooth position and motivation for early treatment. Angle Orthod. 1993, 63, 171–174. [Google Scholar] [PubMed]
- Dias, P.F.; Gleiser, R. Orthodontic concerns of Brazilian children and their parents compared to the normative treatment need. J. Oral Sci. 2010, 52, 101–107. [Google Scholar] [CrossRef] [PubMed]

Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).