
The Dual Burden of Emerging Adulthood: Assessing Gambling Severity, Gambling-Related Harm, and Mental Health Challenges


Abstract
1. Introduction
2. Materials and Methods
2.1. Sample and Procedure
2.2. Instruments
2.2.1. Gambling Behaviors
2.2.2. The Problem Gambling Severity Index (PGSI)
2.2.3. The Short Gambling Harm Screen (SGHS)
2.2.4. Patient Health Questionnaire-4 (PHQ-4)
2.3. Analytic Strategy
3. Results
3.1. Group Differences
3.2. Mediation Analysis
3.2.1. The Mediating Role of Depression-Anxiety in the Association between Age Group and Gambling-Related Harm
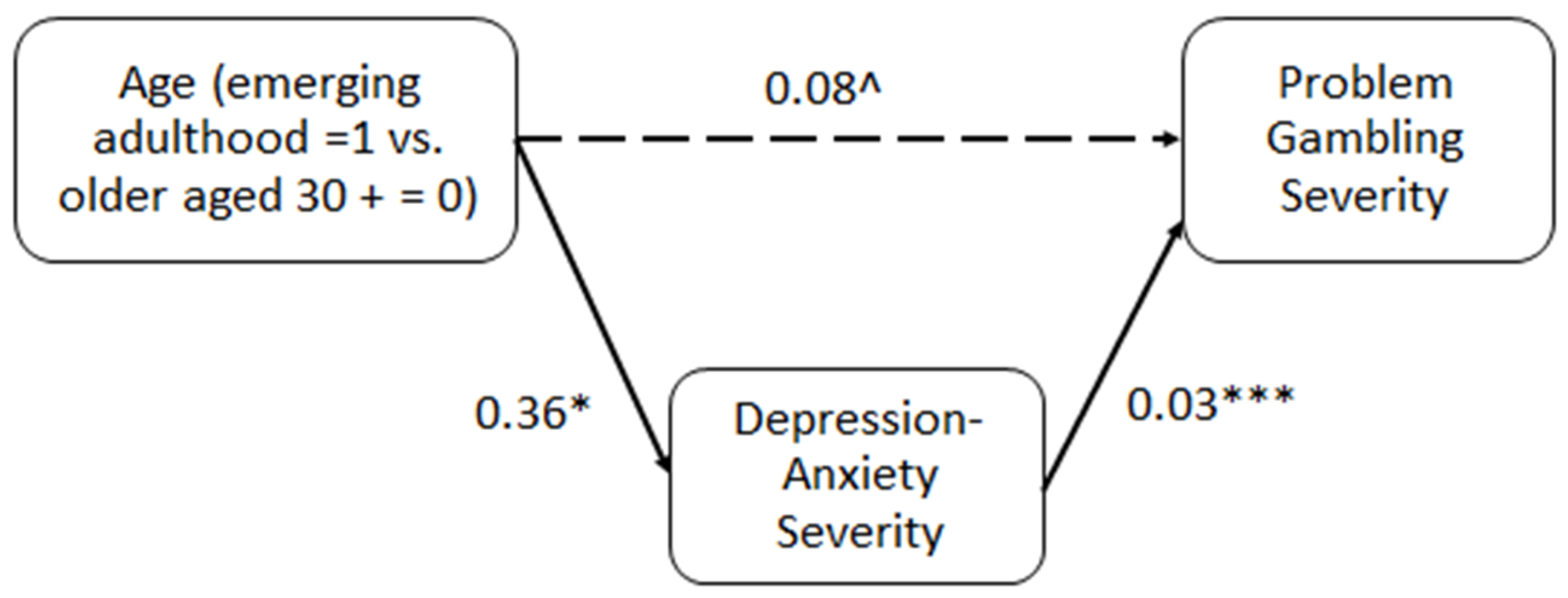
3.2.2. The Mediating Role of Depression-Anxiety in the Association between Age Group and Problem Gambling Severity
3.3. Additional Analyses
4. Discussion
5. Conclusions and Implications
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Price, A.; Hilbrecht, M.; Billi, R. Charting a Path towards a Public Health Approach for Gambling Harm Prevention. J. Public Health 2021, 29, 37–53. [Google Scholar] [CrossRef] [PubMed]
- Allami, Y.; Hodgins, D.C.; Young, M.; Brunelle, N.; Currie, S.; Dufour, M.; Flores-Pajot, M.C.; Nadeau, L. A Meta-Analysis of Problem Gambling Risk Factors in the General Adult Population. Addiction 2021, 116, 2968–2977. [Google Scholar] [CrossRef] [PubMed]
- Grande-Gosende, A.; López-Núñez, C.; García-Fernández, G.; Derevensky, J.; Fernández-Hermida, J.R. Systematic Review of Preventive Programs for Reducing Problem Gambling Behaviors among Young Adults. J. Gambl. Stud. 2020, 36, 1–22. [Google Scholar] [CrossRef] [PubMed]
- Arnett, J.J. Emerging Adulthood: The Winding Road from the Late Teens through the Twenties, 3rd ed.; Oxford University Press: Oxford, UK, 2024. [Google Scholar]
- Seiffge-Krenke, I. Developmental Changes and Their Impact on Psychoanalytic Technique with Emerging Adults. Scand. Psychoanal. Rev. 2022, 45, 128–139. [Google Scholar] [CrossRef]
- Arnett, J.J.; Žukauskiene, R.; Sugimura, K. The New Life Stage of Emerging Adulthood at Ages 18–29 Years: Implications for Mental Health. Lancet Psychiatry 2014, 1, 569–576. [Google Scholar] [CrossRef] [PubMed]
- Shulman, S.; Blatt, S.; Walsh, S. The Extended Journey and Transition to Adulthood: The Case of Israeli Backpackers. J. Youth Stud. 2006, 9, 231–246. [Google Scholar] [CrossRef]
- Arnett, J.J. The Developmental Context of Substance Use in Emerging Adulthood. J. Drug Issues 2005, 35, 235–254. [Google Scholar] [CrossRef]
- Wong, G.; Zane, N.; Saw, A.; Chan, A.K.K. Examining Gender Differences for Gambling Engagement and Gambling Problems among Emerging Adults. J. Gambl. Stud. 2013, 29, 171–189. [Google Scholar] [CrossRef] [PubMed]
- Steinberg, L. A Social Neuroscience Perspective on Adolescent Risk-Taking. Dev. Rev. 2008, 28, 78–106. [Google Scholar] [CrossRef]
- Arnett, J.J.; Mitra, D. Are the Features of Emerging Adulthood Developmentally Distinctive? A Comparison of Ages 18–60 in the United States. Emerg. Adulthood 2020, 8, 412–419. [Google Scholar] [CrossRef]
- Emond, A.; Griffiths, M.D.; Hollén, L. Problem Gambling in Early Adulthood: A Population-Based Study. Int. J. Ment. Health Addict. 2022, 20, 754–770. [Google Scholar] [CrossRef]
- Jun, H.-J.; Sacco, P.; Cunningham-Williams, R.M. Gambling in Emerging Adulthood: The Role of Adolescent Depressive Symptoms, Antisocial Behaviors, and Alcohol Use. Int. J. Ment. Health Addict. 2021, 19, 494–507. [Google Scholar] [CrossRef]
- Richard, J.; King, S.M. Annual Research Review: Emergence of Problem Gambling from Childhood to Emerging Adulthood: A Systematic Review. J. Child Psychol. Psychiatry 2023, 64, 645–688. [Google Scholar] [CrossRef]
- Welte, J.W.; Barnes, G.M.; Tidwell, M.-C.O.; Hoffman, J.H. Gambling and Problem Gambling across the Lifespan. J. Gambl. Stud. 2011, 27, 49–61. [Google Scholar] [CrossRef]
- LeBlanc, N.J.; Brown, M.; Henin, A. Anxiety Disorders in Emerging Adulthood. In Clinical Handbook of Anxiety Disorders; Bui, E., Charney, M.E., Baker, A.W., Eds.; Humana Press: Totowa, NJ, USA, 2020; pp. 157–173. [Google Scholar]
- Potterton, R.; Austin, A.; Robinson, L.; Webb, H.; Allen, K.L.; Schmidt, U. Identity Development and Social-Emotional Disorders during Adolescence and Emerging Adulthood: A Systematic Review and Meta-Analysis. J. Youth Adolesc. 2022, 51, 16–29. [Google Scholar] [CrossRef]
- Richard, J.; Fletcher, É.; Boutin, S.; Derevensky, J.; Temcheff, C. Conduct Problems and Depressive Symptoms in Association with Problem Gambling and Gaming: A Systematic Review. J. Behav. Addict. 2020, 9, 497–533. [Google Scholar] [CrossRef]
- Blaszczynski, A.; Nower, L. A Pathways Model of Problem and Pathological Gambling. Addiction 2002, 97, 487–499. [Google Scholar] [CrossRef]
- Jauregui, P.; Onaindia, J.; Estévez, A. Adaptive and Maladaptive Coping Strategies in Adult Pathological Gamblers and Their Mediating Role with Anxious-Depressive Symptomatology. J. Gambl. Stud. 2017, 33, 1081–1097. [Google Scholar] [CrossRef]
- Dowling, N.A.; Butera, C.A.; Merkouris, S.S.; Youssef, G.J.; Rodda, S.N.; Jackson, A.C. The Reciprocal Association between Problem Gambling and Mental Health Symptoms/Substance Use: Cross-Lagged Path Modelling of Longitudinal Cohort Data. J. Clin. Med. 2019, 8, 1888. [Google Scholar] [CrossRef]
- Chinneck, A.; Mackinnon, S.P.; Stewart, S.H. Investigating Possible Reciprocal Relations between Depressive and Problem Gambling Symptoms in Emerging Adults. Can. J. Psychiatry 2016, 61, 93–101. [Google Scholar] [CrossRef] [PubMed]
- Sagoe, D.; Pallesen, S.; Hanss, D.; Leino, T.; Molde, H.; Mentzoni, R.A.; Torsheim, T. The Relationships between Mental Health Symptoms and Gambling Behavior in the Transition from Adolescence to Emerging Adulthood. Front. Psychol. 2017, 8, 478. [Google Scholar] [CrossRef]
- Edgerton, J.D.; Keough, M.T.; Roberts, L.W. Co-Development of Problem Gambling and Depression Symptoms in Emerging Adults: A Parallel-Process Latent Class Growth Model. J. Gambl. Stud. 2018, 34, 949–968. [Google Scholar] [CrossRef]
- Parke, A.; Griffiths, M.; Pattinson, J.; Keatley, D. Age-Related Physical and Psychological Vulnerability as Pathways to Problem Gambling in Older Adults. J. Behav. Addict. 2018, 7, 137–145. [Google Scholar] [CrossRef]
- Christie-Mizell, C.A.; Hearne, B.N.; Talbert, R.D.; Frazier, C.G. Romantic Relationships, Parenthood, and the Personal Sense of Mastery: The Consequences of Gender among Young Adults. Sociol. Focus 2023, 56, 172–191. [Google Scholar] [CrossRef]
- Kirwan, E.M.; O’Súilleabháin, P.S.; Burns, A.; Ogoro, M.; Allen, E.; Creaven, A.M. Exploring Loneliness in Emerging Adulthood: A Qualitative Study. Emerg. Adulthood 2023, 11, 1433–1445. [Google Scholar] [CrossRef]
- Vuorinen, I.; Oksanen, A.; Savolainen, I.; Sirola, A.; Kaakinen, M.; Paek, H.J.; Zych, I. The Mediating Role of Psychological Distress in Excessive Gambling among Young People: A Four-Country Study. Int. J. Environ. Res. Public Health 2021, 18, 6973. [Google Scholar] [CrossRef]
- Ferris, J.; Wynne, H. The Canadian Problem Gambling Index; Canadian Center on Substance Abuse: Ottawa, ON, Canada, 2001. [Google Scholar]
- Farrell, L.; Fry, J.M. Australia’s Gambling Epidemic and Energy Poverty. Energy Econ. 2021, 97, 105218. [Google Scholar] [CrossRef]
- Gavriel-Fried, B.; Loewenthal, A.; Vana, N. Problem Gambling Severity in a Nationally Representative Sample of the Israeli Population: The Moderating Role of Ethnonational Affiliation. Front. Public Health 2023, 11, 1233301. [Google Scholar] [CrossRef]
- Minutillo, A.; Mastrobattista, L.; Pichini, S.; Pacifici, R.; Genetti, B.; Vian, P.; Andreotti, A.; Mortali, C. Gambling Prevalence in Italy: Main Findings on Epidemiological Study in the Italian Population Aged 18 and Over. Minerva Forensic Med. 2022, 141, 171–178. [Google Scholar] [CrossRef]
- van der Maas, M.; Nower, L. Gambling and Military Service: Characteristics, Comorbidity, and Problem Severity in an Epidemiological Sample. Addict. Behav. 2021, 114, 106725. [Google Scholar] [CrossRef] [PubMed]
- Pchajek, J.; Edgerton, J.D.; Sanscartier, M.; Keough, M. Exploring the Impact of Shame and Guilt on Coping with Gambling Problems among Emerging Adult Gamblers. Can. J. Behav. Sci. 2023, 55, 177–188. [Google Scholar] [CrossRef]
- Wardle, H.; Tipping, S. The Relationship between Problematic Gambling Severity and Engagement with Gambling Products: Longitudinal Analysis of the Emerging Adults Gambling Survey. Addiction 2023, 118, 1127–1139. [Google Scholar] [CrossRef]
- Angus, D.J.; Anjoul, F.; Shannon, K.; Blaszczynski, A. Gambling Related Harms–Community and Clinical Comparisons. Addict. Res. Theory 2020, 28, 194–203. [Google Scholar] [CrossRef]
- Browne, M.; Goodwin, B.C.; Rockloff, M.J. Validation of the Short Gambling Harm Screen (SGHS): A Tool for Assessment of Harms from Gambling. J. Gambl. Stud. 2018, 34, 499–512. [Google Scholar] [CrossRef]
- Svetieva, E.; Walker, M. Inconsistency between Concept and Measurement: The Canadian Problem Gambling Index (CPGI). J. Gambl. Issues 2008, 22, 157–173. [Google Scholar] [CrossRef]
- Alon, S.; Oren, A.; Blannero, K. The First Probabilistic Web-Based Panel in Israel: Representativeness, Probability Sampling, and the Extended Panel Recruitment Process. Isr. Sociol. 2022, 23, 145–157. [Google Scholar]
- Hajek, A.; Heinrich, F.; van Rüth, V.; Kretzler, B.; Langenwalder, F.; Püschel, K.; Bertram, F.; König, H.-H. Prevalence and Determinants of Depression and Anxiety Measured by the PHQ-4 among Homeless Individuals during the COVID-19 Pandemic. Evidence from the Hamburg Survey of Homeless Individuals. Psychiatry Res. 2022, 308, 114350. [Google Scholar] [CrossRef]
- Hayes, A.F. Introduction to Mediation, Moderation, and Conditional Process Analysis: A Regression-Based Approach; Guilford Press: New York, NY, USA, 2013. [Google Scholar]
- Martin, R.J.; Usdan, S.; Cremeens, J.; Vail-Smith, K. Disordered Gambling and Co-Morbidity of Psychiatric Disorders among College Students: An Examination of Problem Drinking, Anxiety and Depression. J. Gambl. Stud. 2014, 30, 321–333. [Google Scholar] [CrossRef]
- Valleur, M.; Codina, I.; Vénisse, J.-L.; Romo, L.; Magalon, D.; Fatséas, M.; Chéreau-Boudet, I.; Gorsane, M.-A.; Guilleux, A.; Grall-Bronnec, M.; et al. Towards a Validation of the Three Pathways Model of Pathological Gambling. J. Gambl. Stud. 2016, 32, 757–771. [Google Scholar] [CrossRef] [PubMed]
- Torrado, M.; Bacelar-Nicolau, L.; Skryabin, V.; Teixeira, M.; Eusébio, S.; Ouakinin, S. Emotional Dysregulation Features and Problem Gambling in University Students: A Pilot Study. J. Addict. Dis. 2020, 38, 550–566. [Google Scholar] [CrossRef] [PubMed]
- Smith, L.L.; Yan, F.; Charles, M.; Mohiuddin, K.; Tyus, D.; Adekeye, O.; Holden, K.B. Exploring the Link between Substance Use and Mental Health Status: What Can We Learn from the Self-Medication Theory? J. Health Care Poor Underserved 2017, 28, 113–131. [Google Scholar] [CrossRef] [PubMed]
- Rogier, G.; Picci, G.; Velotti, P. Struggling with Happiness: A Pathway Leading Depression to Gambling Disorder. J. Gambl. Stud. 2019, 35, 293–305. [Google Scholar] [CrossRef] [PubMed]
- Marchica, L.A.; Keough, M.T.; Montreuil, T.C.; Derevensky, J.L. Emotion Regulation Interacts with Gambling Motives to Predict Problem Gambling among Emerging Adults. Addict. Behav. 2020, 106, 106378. [Google Scholar] [CrossRef] [PubMed]
- Medeiros, G.C.; Sampaio, D.G.; Leppink, E.W.; Chamberlain, S.R.; Grant, J.E. Anxiety, Gambling Activity, and Neurocognition: A Dimensional Approach to a Non-Treatment-Seeking Sample. J. Behav. Addict. 2016, 5, 261–270. [Google Scholar] [CrossRef] [PubMed]
- Sher, K.J.; Trull, T.J.; Bartholow, B.D.; Vieth, A. Personality and Alcoholism: Issues, Methods, and Etiological Processes. In Psychological Theories of Drinking and Alcoholism; Leonard, K.E., Blane, H.T., Eds.; Guildford Press: New York, NY, USA, 1999; pp. 54–105. [Google Scholar]
- Robinson, T.E.; Berridge, K.C. The Incentive Sensitization Theory of Addiction: Some Current Issues. Philos. Trans. R. Soc. B Biol. Sci. 2008, 363, 3137–3146. [Google Scholar] [CrossRef] [PubMed]
- Bylsma, L.M.; Morris, B.H.; Rottenberg, J. A Meta-Analysis of Emotional Reactivity in Major Depressive Disorder. Clin. Psychol. Rev. 2008, 28, 676–691. [Google Scholar] [CrossRef] [PubMed]
- Dowling, N.A.; Greenwood, C.J.; Merkouris, S.S.; Youssef, G.J.; Browne, M.; Rockloff, M.; Myers, P. The Identification of Australian Low-Risk Gambling Limits: A Comparison of Gambling-Related Harm Measures. J. Behav. Addict. 2021, 10, 21–34. [Google Scholar] [CrossRef]
- Browne, M.; Russell, A.M.T.; Begg, S.; Rockloff, M.J.; Li, E.; Rawat, V.; Hing, N. Benchmarking Gambling Screens to Health-State Utility: The PGSI and the SGHS Estimate Similar Levels of Population Gambling-Harm. BMC Public Health 2022, 22, 839. [Google Scholar] [CrossRef]
- Raybould, J.N.; Larkin, M.; Tunney, R.J. Is There a Health Inequality in Gambling Related Harms? A Systematic Review. BMC Public Health 2021, 21, 305. [Google Scholar] [CrossRef]
- Li, E.; Browne, M.; Rawat, V.; Langham, E.; Rockloff, M. Breaking Bad: Comparing Gambling Harms among Gamblers and Affected Others. J. Gambl. Stud. 2017, 33, 223–248. [Google Scholar] [CrossRef]
- Sanscartier, M.D.; Shen, J.; Edgerton, J.D. Gambling among Emerging Adults: How Gender and Risk Level Influence Associated Problem Behaviours. J. Gambl. Issues 2019, 41, 101–123. [Google Scholar] [CrossRef]
- Afifi, T.O.; Nicholson, R.; Martins, S.S.; Sareen, J. A Longitudinal Study of the Temporal Relation between Problem Gambling and Mental and Substance Use Disorders among Young Adults. Can. J. Psychiatry 2016, 61, 102–111. [Google Scholar] [CrossRef] [PubMed]
- Feigelman, W.; Gorman, B.S.; Lesieur, H. Examining the Relationship between At-risk Gambling and Suicidality in a National Representative Sample of Young Adults. Suicide Life-Threat. Behav. 2006, 36, 396–408. [Google Scholar] [CrossRef] [PubMed]
- Wardle, H.; Kesaite, V.; Tipping, S.; McManus, S. Changes in Severity of Problem Gambling and Subsequent Suicide Attempts: A Longitudinal Survey of Young Adults in Great Britain, 2018–2020. Lancet Public Health 2023, 8, e217–e225. [Google Scholar] [CrossRef] [PubMed]
- Blank, L.; Baxter, S.; Woods, H.B.; Goyder, E. Should Screening for Risk of Gambling-Related Harm Be Undertaken in Health, Care and Support Settings? A Systematic Review of the International Evidence. Addict. Sci. Clin. Pract. 2021, 16, 35. [Google Scholar] [CrossRef] [PubMed]
- Bickl, A.M.; Kraus, L.; Loy, J.K.; Kriwy, P.; Sleczka, P.; Schwarzkopf, L. Development of Gambling Behaviour and Its Relationship with Perceived Social Support: A Longitudinal Study of Young Adult Male Gamblers. J. Gambl. Stud. 2024, 40, 307–332. [Google Scholar] [CrossRef]
- Marchica, L.; Zhao, Y.; Richard, J.; Derevensky, J.; Shaffer, H.J. A Comparative Analysis of Canadian University Policies toward Alcohol, Drugs, and Gambling Use. Can. J. Addict. 2018, 9, 18–25. [Google Scholar] [CrossRef]
- Zhao, Y.; Marchica, L.; Derevensky, J.L.; Shaffer, H.J. The Scope, Focus and Types of Gambling Policies among Canadian Colleges and Universities. Can. Psychol. 2017, 58, 187–193. [Google Scholar] [CrossRef]
- Council of Europe International Co-Operation Group on Drugs and Addictions. Strategies and Regulatory Options Aimed at Minimising Risks and Harms Related to Online Gaming and Online Gambling; Council of Europe: Strasbourg Cedex, France, 2024. [Google Scholar]


{kind=link}
{kind=link}
| Variable | Emerging Adults | Adults Aged 30+ |
|---|---|---|
| Women | 447 (60.4%) | 1388 (55.4%) |
| Men | 293 (39.6%) | 1116 (44.6%) |
| In a Relationship | 287 (38.8%) | 1953 (78.0%) |
| Not in a Relationship | 453 (61.2%) | 551 (22.0%) |
| High School Diploma | 316 (42.7%) | 544 (21.7%) |
| No Formal Education | 37 (5.0%) | 167 (6.7%) |
| Partial Academic Degree | 113 (15.3%) | 177 (7.1%) |
| Full Bachelor’s Degree | 179 (24.2%) | 727 (29.0%) |
| Master’s Degree or Higher | 45 (6.1%) | 692 (27.6%) |
| Non-Academic Technical Diploma | 50 (6.8%) | 197 (7.9%) |
| Emerging Adults (n = 740) | Adults Aged 30+ (n = 2504) | |||
|---|---|---|---|---|
| M | SD | M | SD | |
| Problem gambling severity | 0.4740 | 0.78068 | 0.3797 | 0.69707 |
| Gambling-related harms | 0.8092 | 1.69005 | 0.6297 | 1.39822 |
| Depression and anxiety | 3.8446 | 2.68790 | 3.2025 | 2.61578 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gavriel-Fried, B.; Malka, I.; Levin, Y. The Dual Burden of Emerging Adulthood: Assessing Gambling Severity, Gambling-Related Harm, and Mental Health Challenges. Int. J. Environ. Res. Public Health 2024, 21, 702. https://doi.org/10.3390/ijerph21060702
Gavriel-Fried B, Malka I, Levin Y. The Dual Burden of Emerging Adulthood: Assessing Gambling Severity, Gambling-Related Harm, and Mental Health Challenges. International Journal of Environmental Research and Public Health. 2024; 21(6):702. https://doi.org/10.3390/ijerph21060702
Chicago/Turabian StyleGavriel-Fried, Belle, Inbar Malka, and Yafit Levin. 2024. "The Dual Burden of Emerging Adulthood: Assessing Gambling Severity, Gambling-Related Harm, and Mental Health Challenges" International Journal of Environmental Research and Public Health 21, no. 6: 702. https://doi.org/10.3390/ijerph21060702
APA StyleGavriel-Fried, B., Malka, I., & Levin, Y. (2024). The Dual Burden of Emerging Adulthood: Assessing Gambling Severity, Gambling-Related Harm, and Mental Health Challenges. International Journal of Environmental Research and Public Health, 21(6), 702. https://doi.org/10.3390/ijerph21060702