
Multidrug Combinations against SARS-CoV-2 Using GS-441524 or Ivermectin with Molnupiravir and/or Nirmatrelvir in Reconstituted Human Nasal Airway Epithelia
 ,
,
Abstract
1. Introduction
2. Materials and Methods
2.1. Cell Culture
2.2. Virus Propagation
2.3. Toxicity of Drug Combinations
2.4. Antiviral Testing
2.5. RNA Extraction and qRT-PCR
2.6. Determination of Infectious Titer
2.7. Statistical Analysis
3. Results
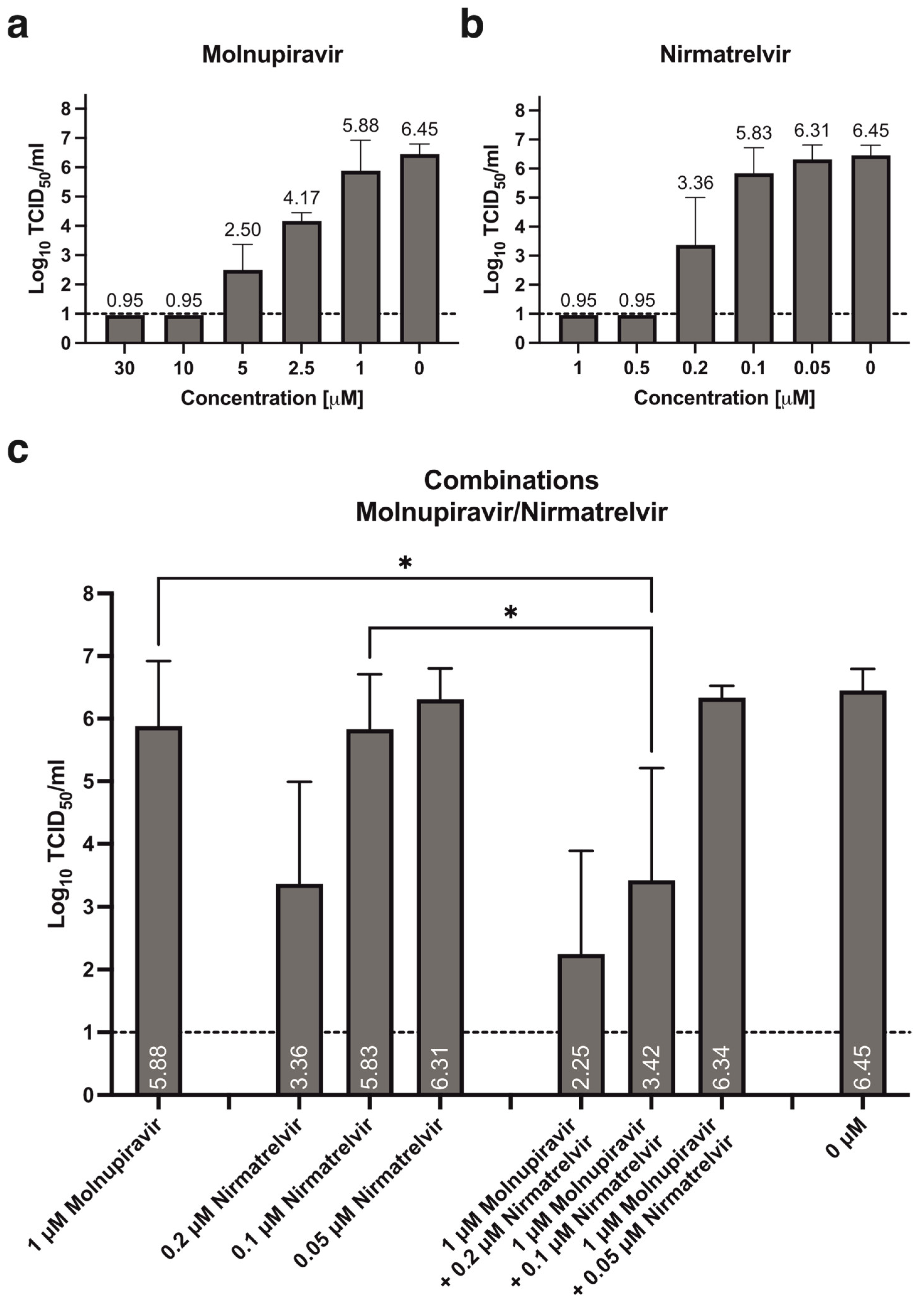
3.1. Antiviral Activity of Molnupiravir and Nirmatrelvir, Alone or in Combination
3.2. Antiviral Activity of GS-441524, Alone or in Combination with Molnupiravir and/or Nirmatrelvir
3.3. Antiviral Activity of Ivermectin, Alone or in Combination with Molnupiravir and/or Nirmatrelvir
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Gordon, D.E.; Jang, G.M.; Bouhaddou, M.; Xu, J.; Obernier, K.; White, K.M.; O’Meara, M.J.; Rezelj, V.V.; Guo, J.Z.; Swaney, D.L.; et al. A SARS-CoV-2 protein interaction map reveals targets for drug repurposing. Nature 2020, 583, 459–468. [Google Scholar] [CrossRef] [PubMed]
- Pan, H.; Richard Peto, F.R.; Karim, Q.A.; Marissa Alejandria, M.D.; Henao-Restrepo, A.M.; García, C.H.; Kieny, M.P.; Reza Malekzadeh, M.D.; Murthy, S.; Srinath Reddy, M.D.; et al. Repurposed Antiviral Drugs for Covid-19—Interim WHO Solidarity Trial Results. N. Engl. J. Med. 2021, 384, 497–511. [Google Scholar] [PubMed]
- Beigel, J.H. Remdesivir for the Treatment of Covid-19—Final Report. N. Engl. J. Med. 2020, 383, 1813–1826. [Google Scholar] [CrossRef]
- Wang, Y.; Zhang, D.; Du, G.; Du, R.; Zhao, J.; Jin, Y.; Fu, S.; Gao, L.; Cheng, Z.; Lu, Q.; et al. Remdesivir in adults with severe COVID-19: A randomised, double-blind, placebo-controlled, multicentre trial. Lancet 2020, 395, 1569–1578. [Google Scholar] [CrossRef] [PubMed]
- Butler, C.C.; Hobbs, F.R.; Gbinigie, O.A.; Rahman, N.M.; Hayward, G.; Richards, D.B.; Dorward, J.; Lowe, D.M.; Standing, J.F.; Breuer, J.; et al. Molnupiravir plus usual care versus usual care alone as early treatment for adults with COVID-19 at increased risk of adverse outcomes (PANORAMIC): An open-label, platform-adaptive randomised controlled trial. Lancet 2023, 401, 281–293. [Google Scholar] [CrossRef]
- Jayk Bernal, A.; Gomes da Silva, M.M.; Musungaie, D.B.; Kovalchuk, E.; Gonzalez, A.; Delos Reyes, V.; Martín-Quirós, A.; Caraco, Y.; Williams-Diaz, A.; Brown, M.L.; et al. Molnupiravir for Oral Treatment of Covid-19 in Nonhospitalized Patients. N. Engl. J. Med. 2022, 386, 509–520. [Google Scholar] [CrossRef]
- Dai, W.; Zhang, B.; Jiang, X.M.; Su, H.; Li, J.; Zhao, Y.; Xie, X.; Jin, Z.; Peng, J.; Liu, F.; et al. Structure-based design of antiviral drug candidates targeting the SARS-CoV-2 main protease. Science 2020, 368, 1331–1335. [Google Scholar] [CrossRef] [PubMed]
- Quan, B.X.; Shuai, H.; Xia, A.J.; Hou, Y.; Zeng, R.; Liu, X.L.; Lin, G.F.; Qiao, J.X.; Li, W.P.; Wang, F.L.; et al. An orally available M(pro) inhibitor is effective against wild-type SARS-CoV-2 and variants including Omicron. Nat. Microbiol. 2022, 7, 716–725. [Google Scholar] [CrossRef] [PubMed]
- Tanimoto, T.; Tada, S.; Fujita, S.; Hirakawa, T.; Matsumura, M.; Isoyama, S.; Ueno, S.; Hamai, K.; Tsuji, N.; Hirosawa, H.; et al. Effect of baricitinib in patients with coronavirus disease 2019 and respiratory failure: A propensity score-matched retrospective cohort study. Respir. Investig. 2022, 60, 418–424. [Google Scholar] [CrossRef]
- Rubin, R. Baricitinib Is First Approved COVID-19 Immunomodulatory Treatment. JAMA 2022, 327, 2281. [Google Scholar] [CrossRef] [PubMed]
- Kodde, C.; Timmen, F.; Hohenstein, S.; Bollmann, A.; Bonsignore, M.; Kuhlen, R.; Nachtigall, I.; Tasci, S. Impact of Dexamethasone on the Pathogen Profile of Critically Ill COVID-19 Patients. Viruses 2023, 15, 1076. [Google Scholar] [CrossRef] [PubMed]
- Arcani, R.; Cauchois, R.; Suchon, P.; Jean, R.; Jarrot, P.A.; Gomes De Pinho, Q.; Dalmas, J.B.; Jean, E.; Andre, B.; Veit, V.; et al. Factors associated with dexamethasone efficacy in COVID-19. A retrospective investigative cohort study. J. Med. Virol. 2022, 94, 3169–3175. [Google Scholar] [CrossRef] [PubMed]
- Tolzali, M.M.R.; Noori, M.; Shokri, P.; Rahmani, S.; Khanzadeh, S.; Nejadghaderi, S.A.; Fazlollahi, A.; Sullman, M.J.M.; Singh, K.; Kolahi, A.; et al. Efficacy of tocilizumab in the treatment of COVID-19: An umbrella review. Rev. Med. Virol. 2022, 32, e2388. [Google Scholar] [CrossRef] [PubMed]
- Oliynyk, O.; Barg, W.; Slifirczyk, A.; Oliynyk, Y.; Gurianov, V.; Rorat, M. Efficacy of Tocilizumab Therapy in Different Subtypes of COVID-19 Cytokine Storm Syndrome. Viruses 2021, 13, 1067. [Google Scholar] [CrossRef] [PubMed]
- Varghese, E.; Samuel, S.M.; Liskova, A.; Kubatka, P.; Büsselberg, D. Diabetes and coronavirus (SARS-CoV-2): Molecular mechanism of Metformin intervention and the scientific basis of drug repurposing. PLoS Pathog. 2021, 17, e1009634. [Google Scholar] [CrossRef]
- Cory, T.J.; Emmons, R.S.; Yarbro, J.R.; Davis, K.L.; Pence, B.D. Metformin Suppresses Monocyte Immunometabolic Activation by SARS-CoV-2 Spike Protein Subunit 1. Front. Immunol. 2021, 12, 733921. [Google Scholar] [CrossRef]
- Chaccour, C.; Casellas, A.; Blanco-Di Matteo, A.; Pineda, I.; Fernandez-Montero, A.; Ruiz-Castillo, P.; Richardson, M.A.; Rodríguez-Mateos, M.; Jordán-Iborra, C.; Brew, J.; et al. The effect of early treatment with ivermectin on viral load, symptoms and humoral response in patients with non-severe COVID-19: A pilot, double-blind, placebo-controlled, randomized clinical trial. EClinicalMedicine 2021, 32, 100720. [Google Scholar] [CrossRef]
- López-Medina, E.; López, P.; Hurtado, I.C.; Dávalos, D.M.; Ramirez, O.; Martínez, E.; Díazgranados, J.A.; Oñate, J.M.; Chavarriaga, H.; Herrera, S.; et al. Effect of Ivermectin on Time to Resolution of Symptoms Among Adults with Mild COVID-19: A Randomized Clinical Trial. JAMA 2021, 325, 1426–1435. [Google Scholar] [CrossRef]
- Hung, I.F.-N.; Lung, K.-C.; Tso, E.Y.-K.; Liu, R.; Chung, T.W.-H.; Chu, M.-Y.; Ng, Y.-Y.; Lo, J.; Chan, J.; Tam, A.R.; et al. Triple combination of interferon beta-1b, lopinavir-ritonavir, and ribavirin in the treatment of patients admitted to hospital with COVID-19: An open-label, randomised, phase 2 trial. Lancet 2020, 395, 1695–1704. [Google Scholar] [CrossRef]
- Cao, B.; Wang, Y.; Wen, D.; Liu, W.; Wang, J.; Fan, G.; Ruan, L.; Song, B.; Cai, Y.; Wei, M.; et al. A Trial of Lopinavir-Ritonavir in Adults Hospitalized with Severe Covid-19. N. Engl. J. Med. 2020, 382, 1787–1799. [Google Scholar] [CrossRef] [PubMed]
- Franco, E.J.; Drusano, G.L.; Hanrahan, K.C.; Warfield, K.L.; Brown, A.N. Combination Therapy with UV-4B and Molnupiravir Enhances SARS-CoV-2 Suppression. Viruses 2023, 15, 1175. [Google Scholar] [CrossRef] [PubMed]
- Orth, H.M.; Flasshove, C.; Berger, M.; Hattenhauer, T.; Biederbick, K.D.; Mispelbaum, R.; Klein, U.; Stemler, J.; Fisahn, M.; Doleschall, A.D.; et al. Early combination therapy of COVID-19 in high-risk patients. Infection 2024, 52, 877–889. [Google Scholar] [CrossRef]
- Günthard, H.F.; Calvez, V.; Paredes, R.; Pillay, D.; Shafer, R.W.; Wensing, A.M.; Jacobsen, D.M.; Richman, D.D. Human Immunodeficiency Virus Drug Resistance: 2018 Recommendations of the International Antiviral Society-USA Panel. Clin. Infect. Dis. 2019, 68, 177–187. [Google Scholar] [CrossRef] [PubMed]
- Su, T.-H.; Liu, C.-J. Combination Therapy for Chronic Hepatitis B: Current Updates and Perspectives. Gut Liver 2017, 11, 590–603. [Google Scholar] [CrossRef] [PubMed]
- Whitley, R.J.; Monto, A.S. Resistance of Influenza Virus to Antiviral Medications. Clin. Infect. Dis. 2020, 71, 1092–1094. [Google Scholar] [CrossRef]
- Rong, L.; Dahari, H.; Ribeiro, R.M.; Perelson, A.S. Rapid emergence of protease inhibitor resistance in hepatitis C virus. Sci. Transl. Med. 2010, 2, 30ra32. [Google Scholar] [CrossRef]
- Jonsdottir, H.R.; Siegrist, D.; Julien, T.; Padey, B.; Bouveret, M.; Terrier, O.; Pizzorno, A.; Huang, S.; Samby, K.; Wells, T.N.; et al. Molnupiravir combined with different repurposed drugs further inhibits SARS-CoV-2 infection in human nasal epithelium in vitro. Biomed. Pharmacother. 2022, 150, 113058. [Google Scholar] [CrossRef] [PubMed]
- Maas, B.M.; Strizki, J.; Miller, R.R.; Kumar, S.; Brown, M.; Johnson, M.G.; Cheng, M.; De Anda, C.; Rizk, M.L.; Stone, J.A. Molnupiravir: Mechanism of action, clinical, and translational science. Clin. Transl. Sci. 2024, 17, e13732. [Google Scholar] [CrossRef]
- Owen, D.R.; Allerton, C.M.; Anderson, A.S.; Aschenbrenner, L.; Avery, M.; Berritt, S.; Boras, B.; Cardin, R.D.; Carlo, A.; Coffman, K.J.; et al. An oral SARS-CoV-2 Mpro inhibitor clinical candidate for the treatment of COVID-19. Science 2021, 374, 1586–1593. [Google Scholar] [CrossRef] [PubMed]
- Li, P.; Wang, Y.; Lavrijsen, M.; Lamers, M.M.; de Vries, A.C.; Rottier, R.J.; Bruno, M.J.; Peppelenbosch, M.P.; Haagmans, B.L.; Pan, Q.; et al. SARS-CoV-2 Omicron variant is highly sensitive to molnupiravir, nirmatrelvir, and the combination. Cell Res. 2022, 32, 322–324. [Google Scholar] [CrossRef]
- Alvarez, J.-C.; Moine, P.; Etting, I.; Annane, D.; Larabi, I.A. Quantification of plasma remdesivir and its metabolite GS-441524 using liquid chromatography coupled to tandem mass spectrometry. Application to a COVID-19 treated patient. Clin. Chem. Lab. Med. 2020, 58, 1461–1468. [Google Scholar] [CrossRef] [PubMed]
- Zaidi, A.K.; Dehgani-Mobaraki, P. The mechanisms of action of ivermectin against SARS-CoV-2—An extensive review. J. Antibiot. 2022, 75, 60–71. [Google Scholar] [CrossRef] [PubMed]
- Matsuyama, S.; Nao, N.; Shirato, K.; Kawase, M.; Saito, S.; Takayama, I.; Nagata, N.; Sekizuka, T.; Katoh, H.; Kato, F.; et al. Enhanced isolation of SARS-CoV-2 by TMPRSS2-expressing cells. Proc. Natl. Acad. Sci. USA 2020, 117, 7001–7003. [Google Scholar] [CrossRef] [PubMed]
- Wiszniewski, L.; Jornot, L.; Dudez, T.; Pagano, A.; Rochat, T.; Lacroix, J.S.; Suter, S.; Chanson, M. Long-term cultures of polarized airway epithelial cells from patients with cystic fibrosis. Am. J. Respir. Cell Mol. Biol. 2006, 34, 39–48. [Google Scholar] [CrossRef]
- Spearman, C. The method of ‘right and wrong cases’ (‘constant stimuli’) without gauss’s formulae. Br. J. Psychol. 1908, 2, 227–242. [Google Scholar] [CrossRef]
- Kärber, G. Beitrag zur kollektiven Behandlung pharmakologischer Reihenversuche. Naunyn Schmiedebergs Arch. Für Exp. Pathol. Und Pharmakol. 1931, 162, 480–483. [Google Scholar] [CrossRef]
- Ramakrishnan, M.A. Determination of 50% endpoint titer using a simple formula. World J. Virol. 2016, 5, 85–86. [Google Scholar] [CrossRef]
- Barber, R.D.; Harmer, D.W.; Coleman, R.A.; Clark, B.J. GAPDH as a housekeeping gene: Analysis of GAPDH mRNA expression in a panel of 72 human tissues. Physiol. Genom. 2005, 21, 389–395. [Google Scholar] [CrossRef] [PubMed]
- Günthard, H.F.; Saag, M.S.; Benson, C.A.; Del Rio, C.; Eron, J.J.; Gallant, J.E.; Hoy, J.F.; Mugavero, M.J.; Sax, P.E.; Thompson, M.A.; et al. Antiretroviral Drugs for Treatment and Prevention of HIV Infection in Adults: 2016 Recommendations of the International Antiviral Society-USA Panel. JAMA 2016, 316, 191–210. [Google Scholar] [CrossRef]
- Naggie, S.; Muir, A.J. Oral Combination Therapies for Hepatitis C Virus Infection: Successes, Challenges, and Unmet Needs. Annu. Rev. Med. 2017, 68, 345–358. [Google Scholar] [CrossRef]
- Chan, J.F.-W.; Yuan, S.; Chu, H.; Sridhar, S.; Yuen, K.-Y. COVID-19 drug discovery and treatment options. Nat. Rev. Microbiol. 2024, 22, 391–407. [Google Scholar] [CrossRef] [PubMed]
- Cannalire, R.; Cerchia, C.; Beccari, A.R.; Di Leva, F.S.; Summa, V. Targeting SARS-CoV-2 Proteases and Polymerase for COVID-19 Treatment: State of the Art and Future Opportunities. J. Med. Chem. 2022, 65, 2716–2746. [Google Scholar] [CrossRef] [PubMed]
- Martonik, D.; Parfieniuk-Kowerda, A.; Starosz, A.; Grubczak, K.; Moniuszko, M.; Flisiak, R. Effect of antiviral and immunomodulatory treatment on a cytokine profile in patients with COVID-19. Front. Immunol. 2023, 14, 1222170. [Google Scholar] [CrossRef] [PubMed]
- Moshawih, S.; Jarrar, Q.; Bahrin, A.A.; Lim, A.F.; Ming, L.; Goh, H.P. Evaluating NSAIDs in SARS-CoV-2: Immunomodulatory mechanisms and future therapeutic strategies. Heliyon 2024, 10, e25734. [Google Scholar] [CrossRef] [PubMed]
- Verma, G.; Dhawan, M.; Saied, A.A.; Kaur, G.; Kumar, R.; Bin Emran, T. Immunomodulatory approaches in managing lung inflammation in COVID-19: A double-edge sword. Immun. Inflamm. Dis. 2023, 11, e1020. [Google Scholar] [CrossRef]
- Rosenke, K.; Lewis, M.C.; Feldmann, F.; Bohrnsen, E.; Schwarz, B.; Okumura, A.; Bohler, W.F.; Callison, J.; Shaia, C.; Bosio, C.M.; et al. Combined molnupiravir-nirmatrelvir treatment improves the inhibitory effect on SARS-CoV-2 in macaques. JCI Insight 2023, 8, e166485. [Google Scholar] [CrossRef]
- Wang, X.; Sacramento, C.Q.; Jockusch, S.; Chaves, O.A.; Tao, C.; Fintelman-Rodrigues, N.; Chien, M.; Temerozo, J.R.; Li, X.; Kumar, S.; et al. Combination of antiviral drugs inhibits SARS-CoV-2 polymerase and exonuclease and demonstrates COVID-19 therapeutic potential in viral cell culture. Commun. Biol. 2022, 5, 154. [Google Scholar] [CrossRef]
- Peña-Silva, R.; Duffull, S.B.; Steer, A.C.; Jaramillo-Rincon, S.X.; Gwee, A.; Zhu, X. Pharmacokinetic considerations on the repurposing of ivermectin for treatment of COVID-19. Br. J. Clin. Pharmacol. 2021, 87, 1589–1590. [Google Scholar] [CrossRef]
- Canga, A.G.; Prieto, A.M.S.; Liébana, M.J.D.; Martínez, N.F.; Vega, M.S.; Vieitez, J.J.G. The pharmacokinetics and interactions of ivermectin in humans—A mini-review. AAPS J. 2008, 10, 42–46. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
| Concentration (µM) | Log10 Fold Change RNA | Infectious Titer | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Molnupiravir | PF-07321332 | GS-441524 | Ivermectin | 48 h | ±SD | 72 h | ±SD | IC | ±SD | Log10 TCID50/mL | ±SD |
| 30 | −3.69 | 0.33 | −3.94 | 0.07 | −4.62 | 0.04 | LOD | n/a | |||
| 10 | −4.13 | 1.23 | −3.20 | 0.43 | −3.43 | 0.34 | LOD | n/a | |||
| 5 | −2.02 | 0.38 | −0.85 | 0.16 | −0.83 | 0.26 | 2.50 | 0.71 | |||
| 2.5 | −0.74 | 0.06 | −0.47 | 0.02 | −0.28 | 0.14 | 4.17 | 0.24 | |||
| 1 | −0.21 | 0.10 | −0.21 | 0.19 | −0.23 | 0.20 | 5.88 | 0.96 | |||
| 0.5 | −0.17 | 0.01 | −0.07 | 0.07 | −0.08 | 0.04 | - | - | |||
| 0.1 | −0.32 | 0.06 | −0.03 | 0.01 | 0.06 | 0.05 | - | - | |||
| 5 | −4.79 | 0.13 | −4.17 | 0.64 | −4.96 | 0.03 | - | - | |||
| 1 | −4.14 | 0.83 | −3.99 | 0.16 | −4.80 | 0.38 | LOD | n/a | |||
| 0.5 | −3.80 | 0.23 | −4.10 | 0.18 | −4.82 | 0.31 | LOD | n/a | |||
| 0.2 | −3.20 | 0.10 | −2.97 | 0.67 | −3.39 | 0.74 | 3.36 | 1.41 | |||
| 0.1 | −2.28 | 0.86 | −0.93 | 0.60 | −0.73 | 0.56 | 5.83 | 0.81 | |||
| 0.05 | −0.44 | 0.21 | −0.19 | 0.12 | 0.00 | 0.16 | 6.31 | 0.46 | |||
| 0.01 | 0.22 | 0.06 | −0.13 | 0.26 | −0.05 | 0.15 | 6.00 | 0.00 | |||
| 10 | −3.89 | 0.12 | −3.85 | 0.74 | −4.79 | 0.21 | LOD | n/a | |||
| 5 | −3.07 | 0.22 | −4.07 | 0.27 | −5.31 | 0.17 | LOD | n/a | |||
| 3 | −3.33 | 0.34 | −3.38 | 0.33 | −4.40 | 0.38 | LOD | n/a | |||
| 1 | −1.12 | 0.11 | −0.88 | 0.10 | −1.67 | 0.15 | 5.72 | 0.84 | |||
| 0.3 | −0.01 | 0.08 | −0.16 | 0.12 | −0.26 | 0.19 | 6.48 | 0.73 | |||
| 10 | −0.83 | 0.08 | −0.55 | 0.17 | −0.69 | 0.19 | 3.89 | 0.97 | |||
| 5 | −0.70 | 0.09 | 0.27 | 0.05 | 0.30 | 0.07 | 6.25 | 0.25 | |||
| 2.5 | −0.78 | 1.07 | 0.06 | 0.24 | 0.45 | 0.14 | 6.17 | 0.24 | |||
| 1 | −0.31 | 0.24 | 0.17 | 0.14 | 0.29 | 0.19 | 6.33 | 0.47 | |||
| 0.5 | −0.08 | 0.08 | 0.02 | 0.12 | 0.26 | 0.19 | 6.33 | 0.47 | |||
| 0.25 | 0.16 | 0.20 | 0.04 | 0.08 | −0.13 | 0.17 | 6.58 | 0.73 | |||
| 0 | 0 | 0 | 0 | 0.16 | 0.20 | 0.01 | 0.06 | −0.01 | 0.06 | 6.45 | 0.32 |
| Concentration (µM) | Log10 Fold Change RNA | Infectious Titer | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Molnupiravir | PF-07321332 | GS-441524 | Ivermectin | 48 h | ±SD | 72 h | ±SD | IC | ±SD | Log10 TCID50/mL | ±SD |
| 1 | −0.21 | 0.10 | −0.21 | 0.19 | −0.23 | 0.20 | 5.88 | 0.96 | |||
| 0.2 | −3.20 | 0.10 | −2.97 | 0.67 | −3.39 | 0.74 | 3.36 | 1.41 | |||
| 0.1 | −2.28 | 0.86 | −0.93 | 0.60 | −0.73 | 0.56 | 5.83 | 0.81 | |||
| 0.05 | −0.44 | 0.21 | −0.19 | 0.12 | 0.00 | 0.16 | 6.31 | 0.46 | |||
| 1 | −1.12 | 0.11 | −0.88 | 0.10 | −1.67 | 0.15 | 5.72 | 0.84 | |||
| 0.3 | −0.01 | 0.08 | −0.16 | 0.12 | −0.26 | 0.19 | 6.48 | 0.73 | |||
| 10 | −0.83 | 0.08 | −0.55 | 0.17 | −0.69 | 0.19 | 3.89 | 0.97 | |||
| 0.25 | 0.16 | 0.20 | 0.04 | 0.08 | −0.13 | 0.17 | 6.58 | 0.73 | |||
| 1 | 0.2 | −2.97 | 0.12 | −3.40 | 0.94 | −3.90 | 0.79 | 2.25 | 1.64 | ||
| 1 | 0.1 | −2.62 | 0.51 | −2.41 | 1.47 | −2.48 | 1.49 | 3.42 | 1.79 | ||
| 1 | 0.05 | −0.98 | 0.13 | −0.50 | 0.11 | −0.18 | 0.29 | 6.33 | 0.19 | ||
| 1 | 1 | −2.25 | 1.49 | −2.09 | 1.26 | −2.81 | 1.87 | 3.33 | 1.91 | ||
| 1 | 0.3 | −1.74 | 0.93 | −0.55 | 0.11 | −0.95 | 0.38 | 5.83 | 0.54 | ||
| 1 | 10 | −1.76 | 0.13 | −2.23 | 0.40 | −2.80 | 0.35 | 3.58 | 0.88 | ||
| 1 | 0.25 | −0.35 | 0.31 | −0.32 | 0.30 | −0.55 | 0.14 | 6.00 | 0.33 | ||
| 0.2 | 1 | −3.11 | 0.19 | −3.84 | 0.51 | −4.58 | 0.18 | 1.86 | 1.12 | ||
| 0.2 | 0.3 | −3.07 | 0.26 | −3.41 | 0.61 | −4.08 | 0.65 | 2.31 | 1.57 | ||
| 0.2 | 10 | −3.03 | 0.24 | −3.73 | 0.51 | −4.67 | 0.41 | 0.98 | 0.14 | ||
| 0.2 | 0.25 | −2.83 | 0.37 | −3.13 | 0.69 | −3.63 | 0.81 | 2.92 | 1.55 | ||
| 0.1 | 1 | −3.09 | 0.26 | −3.43 | 0.64 | −4.42 | 0.29 | 2.00 | 1.37 | ||
| 0.1 | 0.3 | −2.46 | 0.31 | −1.66 | 0.66 | −1.85 | 0.43 | 4.83 | 0.27 | ||
| 0.1 | 10 | −3.06 | 0.18 | −3.60 | 0.65 | −4.13 | 0.75 | LOD | n/a | ||
| 0.1 | 0.25 | −2.73 | 0.40 | −2.43 | 1.12 | −2.29 | 0.77 | 4.42 | 1.34 | ||
| 0.05 | 1 | −2.79 | 0.85 | −2.90 | 0.91 | −3.53 | 1.47 | 2.48 | 1.76 | ||
| 0.05 | 0.3 | −1.95 | 1.25 | −1.10 | 0.63 | −1.59 | 0.74 | 5.83 | 0.27 | ||
| 0.05 | 10 | −2.22 | 0.43 | −2.29 | 1.53 | −2.70 | 1.46 | 3.45 | 2.95 | ||
| 0.05 | 0.25 | −0.65 | 0.09 | −0.57 | 0.23 | −0.44 | 0.20 | 6.50 | 0.27 | ||
| 1 | 0.2 | 1 | −3.27 | 0.29 | −3.70 | 0.48 | −4.38 | 0.27 | 1.78 | 0.83 | |
| 1 | 0.1 | 1 | −3.29 | 0.24 | −3.53 | 0.38 | −4.30 | 0.12 | 1.89 | 1.08 | |
| 1 | 0.05 | 1 | −2.81 | 0.54 | −2.59 | 1.08 | −3.05 | 0.90 | 3.67 | 0.69 | |
| 1 | 0.2 | 0.3 | −2.95 | 0.15 | −3.37 | 0.52 | −3.89 | 0.12 | 1.70 | 1.24 | |
| 1 | 0.1 | 0.3 | −2.72 | 0.47 | −2.55 | 1.11 | −2.50 | 1.22 | 4.00 | 1.93 | |
| 1 | 0.05 | 0.3 | −1.27 | 0.36 | −0.73 | 0.65 | −1.20 | 0.68 | 5.50 | 0.86 | |
| 1 | 0.2 | 10 | −3.16 | 0.17 | −3.71 | 0.49 | −4.43 | 0.19 | LOD | n/a | |
| 1 | 0.1 | 10 | −3.14 | 0.25 | −3.26 | 0.40 | −3.64 | 0.51 | 1.51 | 1.11 | |
| 1 | 0.05 | 10 | −2.52 | 0.22 | −3.07 | 0.45 | −3.70 | 0.76 | 1.92 | 0.88 | |
| 1 | 0.2 | 0.25 | −2.89 | 0.33 | −3.20 | 0.52 | −3.55 | 0.43 | 3.08 | 0.69 | |
| 1 | 0.1 | 0.25 | −2.65 | 0.37 | −2.60 | 1.03 | −2.34 | 0.74 | 4.08 | 1.07 | |
| 1 | 0.05 | 0.25 | −1.15 | 0.22 | −0.80 | 0.40 | −0.87 | 0.19 | 5.42 | 0.57 | |
| 0 | 0 | 0 | 0 | 0.16 | 0.20 | 0.01 | 0.06 | −0.01 | 0.06 | 6.45 | 0.3 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Siegrist, D.; Jonsdottir, H.R.; Bouveret, M.; Boda, B.; Constant, S.; Engler, O.B. Multidrug Combinations against SARS-CoV-2 Using GS-441524 or Ivermectin with Molnupiravir and/or Nirmatrelvir in Reconstituted Human Nasal Airway Epithelia. Pharmaceutics 2024, 16, 1262. https://doi.org/10.3390/pharmaceutics16101262
Siegrist D, Jonsdottir HR, Bouveret M, Boda B, Constant S, Engler OB. Multidrug Combinations against SARS-CoV-2 Using GS-441524 or Ivermectin with Molnupiravir and/or Nirmatrelvir in Reconstituted Human Nasal Airway Epithelia. Pharmaceutics. 2024; 16(10):1262. https://doi.org/10.3390/pharmaceutics16101262
Chicago/Turabian StyleSiegrist, Denise, Hulda R. Jonsdottir, Mendy Bouveret, Bernadett Boda, Samuel Constant, and Olivier B. Engler. 2024. "Multidrug Combinations against SARS-CoV-2 Using GS-441524 or Ivermectin with Molnupiravir and/or Nirmatrelvir in Reconstituted Human Nasal Airway Epithelia" Pharmaceutics 16, no. 10: 1262. https://doi.org/10.3390/pharmaceutics16101262
APA StyleSiegrist, D., Jonsdottir, H. R., Bouveret, M., Boda, B., Constant, S., & Engler, O. B. (2024). Multidrug Combinations against SARS-CoV-2 Using GS-441524 or Ivermectin with Molnupiravir and/or Nirmatrelvir in Reconstituted Human Nasal Airway Epithelia. Pharmaceutics, 16(10), 1262. https://doi.org/10.3390/pharmaceutics16101262