
Questionnaire Study to Investigate the Preferences of Children, Parents, and Healthcare Professionals for Different Formulations of Oral Medicinal Products

 ,
,
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Objectives
2.2. Study Design
2.3. Inclusion/Exclusion Criteria
2.4. Study Activities, Study Groups, and Formulations
2.5. Sample Size and Statistics
2.6. Questionnaire Design
3. Results
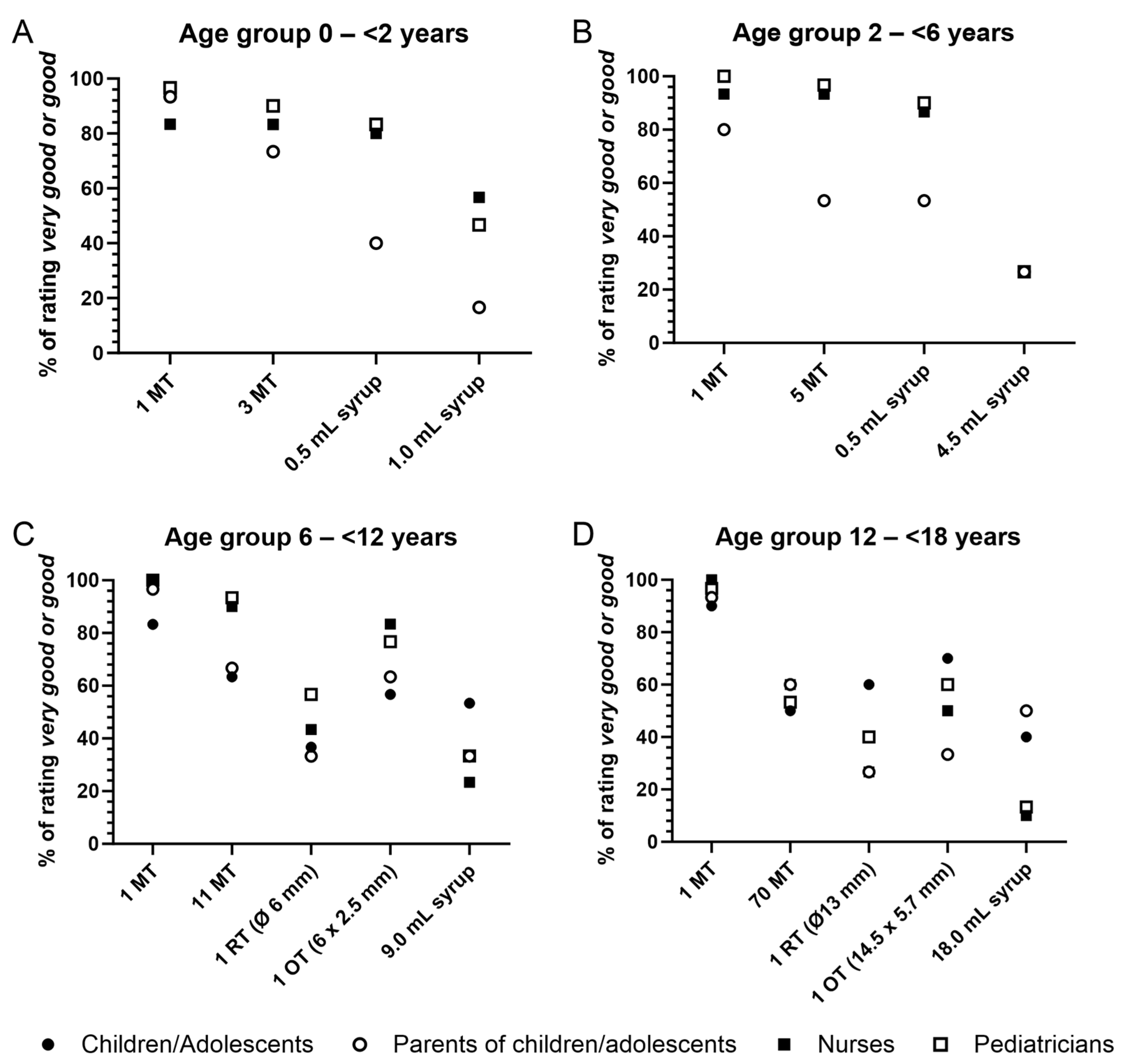
3.1. Age Group 0–<2 y
3.2. Age Group 2–<6 y
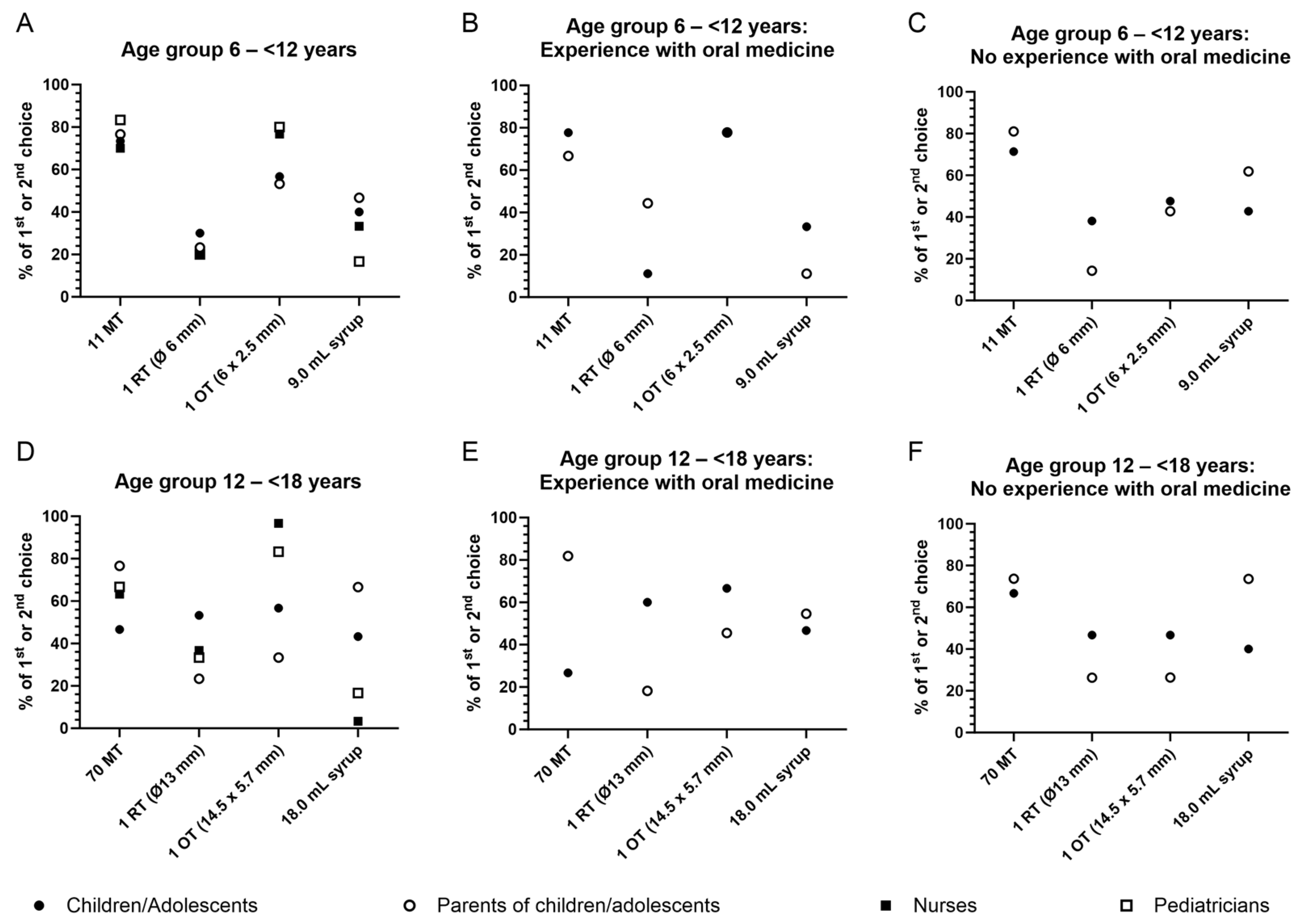
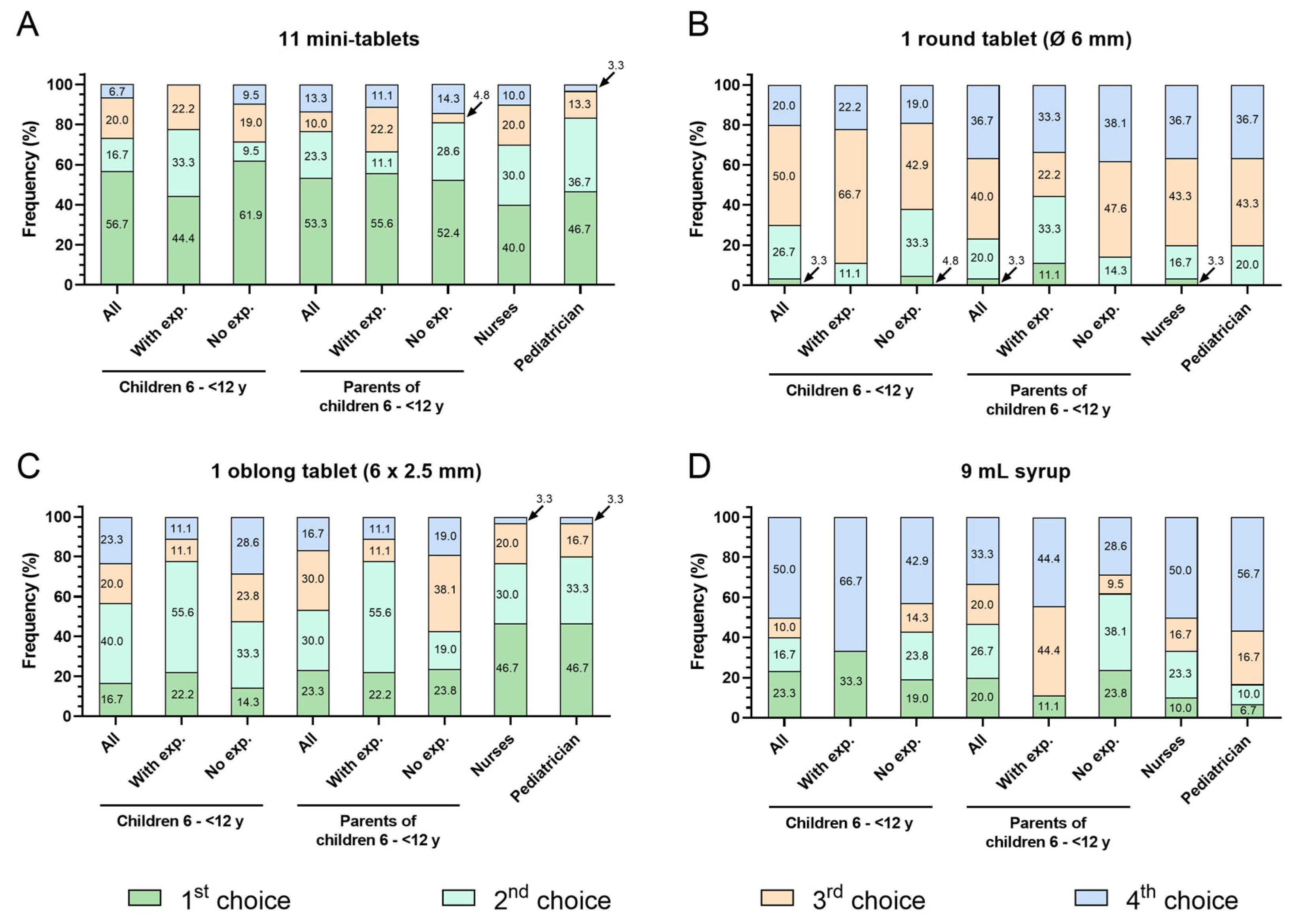
3.3. Age Group 6–<12 y
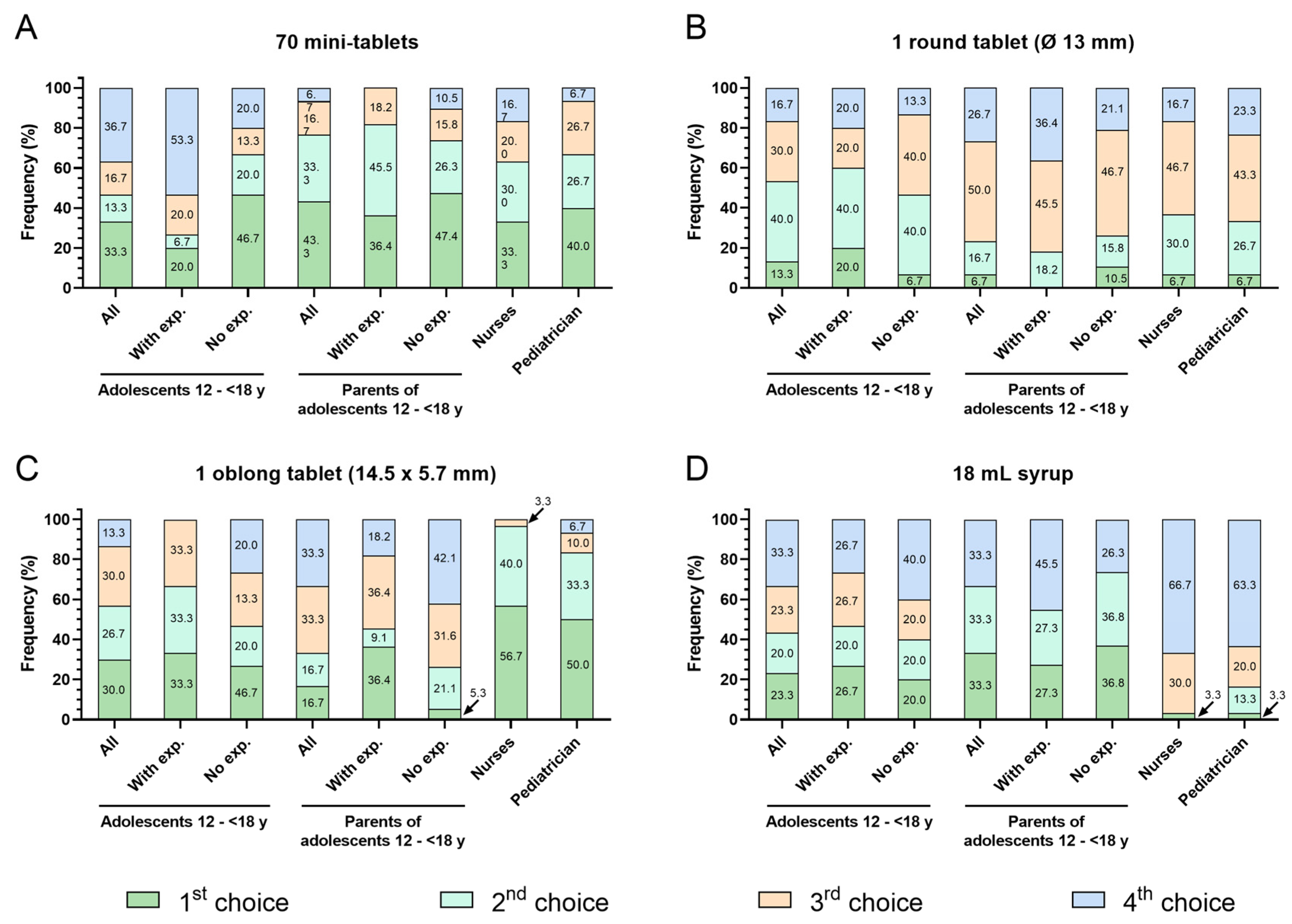
3.4. Age Group 12–<18 y
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Lopalco, A.; Denora, N. Paediatric Formulation: Design and Development. Int. J. Mol. Sci. 2020, 21, 7118. [Google Scholar] [CrossRef] [PubMed]
- Khan, D.; Kirby, D.; Bryson, S.; Shah, M.; Rahman Mohammed, A. Paediatric specific dosage forms: Patient and formulation considerations. Int. J. Pharm. 2022, 616, 121501. [Google Scholar] [CrossRef]
- Vallet, T.; Elhamdaoui, O.; Berraho, A.; Cherkaoui, L.O.; Kriouile, Y.; Mahraoui, C.; Mouane, N.; Pense-Lheritier, A.M.; Ruiz, F.; Bensouda, Y. Medicines Acceptability in Hospitalized Children: An Ongoing Need for Age-Appropriate Formulations. Pharmaceutics 2020, 12, 766. [Google Scholar] [CrossRef]
- European Medicines Agency; Committee for Medicinal Products for Human Use; Paediatric Committee. Guideline on Pharmaceutical Development of Medicines for Paediatric Use. EMA/CHMP/QWP/805880/2012 Rev. 2. European Medicines Agency 2013. Available online: https://www.ema.europa.eu/en/documents/scientific-guideline/guideline-pharmaceutical-development-medicines-paediatric-use_en.pdf (accessed on 8 January 2024).
- Alessandrini, E.; Brako, F.; Scarpa, M.; Lupo, M.; Bonifazi, D.; Pignataro, V.; Cavallo, M.; Cullufe, O.; Enache, C.; Nafria, B.; et al. Children’s Preferences for Oral Dosage Forms and Their Involvement in Formulation Research via EPTRI (European Paediatric Translational Research Infrastructure). Pharmaceutics 2021, 13, 730. [Google Scholar] [CrossRef] [PubMed]
- Liu, F.; Ranmal, S.; Batchelor, H.K.; Orlu-Gul, M.; Ernest, T.B.; Thomas, I.W.; Flanagan, T.; Tuleu, C. Patient-centred pharmaceutical design to improve acceptability of medicines: Similarities and differences in paediatric and geriatric populations. Drugs 2014, 74, 1871–1889. [Google Scholar] [CrossRef] [PubMed]
- Wargenau, W.; Reidemeister, S.; Klingmann, I.; Klingmann, V. A composite endpoint for acceptability evaluation of oral drug formulations in the pediatric population. Ther. Innov. Regul. Sci. 2022, 56, 903–909. [Google Scholar] [CrossRef]
- Spomer, N.; Klingmann, V.; Stoltenberg, I.; Lerch, C.; Meissner, T.; Breitkreutz, J. Acceptance of uncoated mini-tablets in young children: Results from a prospective exploratory cross-over study. Arch. Dis. Child. 2012, 97, 283–286. [Google Scholar] [CrossRef] [PubMed]
- Klingmann, V.; Spomer, N.; Lerch, C.; Stoltenberg, I.; Frömke, C.; Bosse, H.M.; Breitkreutz, J.; Meissner, T. Favorable acceptance of mini-tablets compared with syrup: A randomized controlled trial in infants and preschool children. J. Pediatr. 2013, 163, 1728–1732. [Google Scholar] [CrossRef] [PubMed]
- Klingmann, V.; Seitz, A.; Meissner, T.; Breitkreutz, J.; Möltner, A.; Bosse, H.M. Acceptability of uncoated mini-tablets in neonates—A randomized controlled trial. J. Pediatr. 2015, 167, 893–896. [Google Scholar] [CrossRef] [PubMed]
- Klingmann, V.; Linderskamp, H.; Meissner, T.; Mayatepek, E.; Moeltner, A.; Breitkreutz, J.; Bosse, H.M. Acceptability of multiple uncoated minitablets in infants and toddlers: A randomized controlled trial. J. Pediatr. 2018, 201, 202–207. [Google Scholar] [CrossRef] [PubMed]
- Münch, J.; Meissner, T.; Mayatepek, E.; Wargenau, M.; Breitkreutz, J.; Bosse, H.M.; Klingmann, V. Acceptability of small-sized oblong tablets in comparison to syrup and mini-tablets in infants and toddlers: A randomized controlled trial. J. Pediatr. 2021, 166, 126–134. [Google Scholar] [CrossRef]
- Klingmann, V.; Pohly, C.E.; Meissner, T.; Mayatepek, E.; Moeltner, A.; Flunkert, K.; Breitkreutz, J.; Bosse, H.M. Acceptability of an orodispersible film compared to syrup in neonates and infants: A randomized controlled trial. Eur. J. Pharm. Biopharm. 2020, 151, 239–245. [Google Scholar] [CrossRef] [PubMed]
- Münch, J.; Kloft, C.; Farhan, M.; Fishman, V.; Leng, S.; Bosse, H.M.; Klingmann, V. Acceptability, swallowability, palatability, and safety of multiple film-coated mini-tablets in children aged ≥2–<7 years: Results of an open-label randomised study. Pharmaceutics 2023, 15, 701. [Google Scholar] [CrossRef]
- Klingmann, V.; Hinder, M.; Langenickel, T.H.; Chen, F.; Khder, Y.; Breitkreutz, J.; Bosse, H.M. Acceptability of multiple coated mini-tablets in comparison to syrup in infants and toddlers: A randomised controlled study. Arch. Dis. Child. 2023, 108, 730–735. [Google Scholar] [CrossRef] [PubMed]
- Münch, J.; Sessler, I.; Bosse, H.M.; Wargenau, M.; Dreesen, J.D.; Loforese, G.; Webb, N.J.A.; Sivasubramanian, R.; Reidemeister, S.; Lustenberger, P.; et al. Evaluating the Acceptability, Swallowability, and Palatability of Film-Coated Mini-Tablet Formulation in Young Children: Results from an Open-Label, Single-Dose, Cross-Over Study. Pharmaceutics 2023, 15, 1729. [Google Scholar] [CrossRef] [PubMed]
- Thomson, S.A.; Tuleu, C.; Wong, I.C.; Keady, S.; Pitt, K.G.; Sutcliffe, A.G. Minitablets: New modality to deliver medicines to preschool-aged children. Pediatrics 2009, 123, e235–e238. [Google Scholar] [CrossRef] [PubMed]
- Kluk, A.; Sznitowska, M.; Brandt, A.; Sznurkowska, K.; Plata-Nazar, K.; Mysliwiec, M.; Kaminska, B.; Kotlowska, H. Can preschool-aged children swallow several minitablets at a time? Results from a clinical pilot study. Int. J. Pharm. 2015, 485, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Yin, H.S.; Mendelsohn, A.L.; Wolf, M.S.; Parker, R.M.; Fierman, A.; van Schaick, L.; Bazan, I.S.; Kline, M.D.; Dreyer, B.P. Parents’ medication administration errors: Role of dosing instruments and health literacy. Arch. Pediatr. Adolesc. Med. 2010, 164, 181–186. [Google Scholar] [CrossRef] [PubMed]
- Schirm, E.; Tobi, H.; de Vries, T.W.; Choonara, I.; De Jong-van den Berg, L.T. Lack of appropriate formulations of medicines for children in the community. Acta Paediatr. 2003, 92, 1486–1489. [Google Scholar] [CrossRef] [PubMed]
- Aleksovski, A.; Dreu, R.; Gašperlin, M.; Planinšek, O. Mini-tablets: A contemporary system for oral drug delivery in targeted patient groups. Expert. Opin. Drug Deliv. 2015, 12, 65–84. [Google Scholar] [PubMed]
- Ruiz, F.; Vallet, T.; Dufaÿ Wojcicki, A.; Belissa, É.; Fontan, J.E.; de Pontual, L.; Nathanson, S.; Chevallier, A.; Laribe-Caget, S.; Boudy, V. Dosage form suitability in vulnerable populations: A focus on paracetamol acceptability from infants to centenarians. PLoS ONE 2019, 14, e0221261. [Google Scholar] [CrossRef] [PubMed]
- Mitsui, N.; Hida, N.; Kamiya, T.; Yamazaki, T.; Miyazaki, K.; Saito, K.; Saito, J.; Yamatani, A.; Ishikawa, Y.; Nakamura, H.; et al. Swallowability of Minitablets among Children Aged 6–23 Months: An Exploratory, Randomized Crossover Study. Pharmaceutics 2022, 14, 198. [Google Scholar] [CrossRef] [PubMed]
- Bracken, L.; McDonough, E.; Ashleigh, S.; Wilson, F.; Shakeshaft, J.; Ohia, U.; Mistry, P.; Jones, H.; Kanji, N.; Liu, F.; et al. Can children swallow tablets? Outcome data from a feasibility study to assess the acceptability of different-sized placebo tablets in children (creating acceptable tablets (CAT)). BMJ Open 2020, 10, e036508. [Google Scholar] [CrossRef] [PubMed]
- Ranmal, S.R.; O‘Brien, F.; Lopez, F.; Ruiz, F.; Orlu, M.; Tuleu, C.; Walsh, J.; Liu, F. Methodologies for assessing the acceptability of oral formulations among children and older adults: A systematic review. Drug Discov. Today 2018, 23, 830–847. [Google Scholar] [CrossRef] [PubMed]
- Klingmann, V.; Vallet, T.; Münch, J.; Stegemann, R.; Wolters, L.; Bosse, H.M.; Ruiz, F. Dosage Forms Suitability in Pediatrics: Acceptability of Analgesics and Antipyretics in a German Hospital. Pharmaceutics 2022, 14, 337. [Google Scholar] [CrossRef]
- Turner-Bowker, D.M.; An Haack, K.; Krohe, M.; Yaworsky, A.; Vivas, N.; Kelly, M.; Chatterjee, G.; Chaston, E.; Mann, E.; Reaney, M. Development and content validation of the Pediatric Oral Medicines Acceptability Questionnaires (P-OMAQ): Patient-reported and caregiver-reported outcome measures. J. Patient Rep. Outcomes. 2020, 4, 80. [Google Scholar] [CrossRef] [PubMed]
- Mistry, P.; Batchelor, H.; SPaeDD-UK Project (Smart Paediatric Drug Development—UK). Evidence of acceptability of oral paediatric medicines: A review. J. Pharm. Pharmacol. 2017, 69, 361–376. [Google Scholar] [CrossRef] [PubMed]
- Hall, L.; Hume, C.; Tazzyman, S. Five Degrees of Happiness: Effective Smiley Face Likert Scales for Evaluating with Children. In Proceedings of the 15th International Conference on Interaction Design and Children (IDC ‘16), Manchester, UK, 21–24 June 2016; Association for Computing Machinery: New York, NY, USA, 2016; pp. 311–321. [Google Scholar]
- Borgers, N.; Hox, J.; Sikkel, D. Response Effects in Surveys on Children and Adolescents: The Effect of Number of Response Options, Negative Wording, and Neutral Mid-Point. Qual. Quant. Int. J. Methodol. 2004, 38, 17–33. [Google Scholar]
- Bell, A. Designing and testing questionnaires for children. J. Res. Nurs. 2007, 12, 461–469. [Google Scholar] [CrossRef]
- Borgers, N.; de Leeuw, E.; Hox, J. Children as Respondents in Survey Research: Cognitive Development and Response Quality 1. Bull. Methodol. Sociol. 2000, 66, 60–75. [Google Scholar] [CrossRef]
- van Laerhoven, H.; van der Zaag-Loonen, H.J.; Derkx, B.H. A comparison of Likert scale and visual analogue scales as response options in children’s questionnaires. Acta Paediatr. 2004, 93, 830–835. [Google Scholar] [CrossRef] [PubMed]
- Ruark, J.L.; McCullough, G.H.; Peters, R.L.; Moore, C.A. Bolus consistency and swallowing in children and adults. Dysphagia 2002, 17, 24–33. [Google Scholar] [CrossRef] [PubMed]
- Fabiano, V.; Mameli, C.; Zuccotti, G.V. Paediatric pharmacology: Remember the excipients. Pharmacol. Res. 2011, 63, 362–365. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Age Group | Formulations | |||
|---|---|---|---|---|
| No. of MT | Size of RT | Size of OT | Max. Vol. of Syrup | |
| 0–<2 y | 1 and 3 | n.a. | n.a. | 1.0 mL |
| 2–<6 y | 1 and 5 | n.a. | n.a. | 4.5 mL |
| 6–<12 y | 1 and 11 | Ø 6 mm | 6 × 2.5 mm | 9.0 mL |
| 12–<18 y | 1 and 70 | Ø 13 mm | 14.5 × 5.7 mm | 18.0 mL |
| Manufacturer | NextPharma, Göttingen, Germany | Caesar & Loretz GmbH, Hilden, Germany | ||
| Ingredients | Lactose, cellulose, magnesium stearate, anhydrous colloidal silicon dioxide | Glucose, water | ||
| Type | Group | Questions |
|---|---|---|
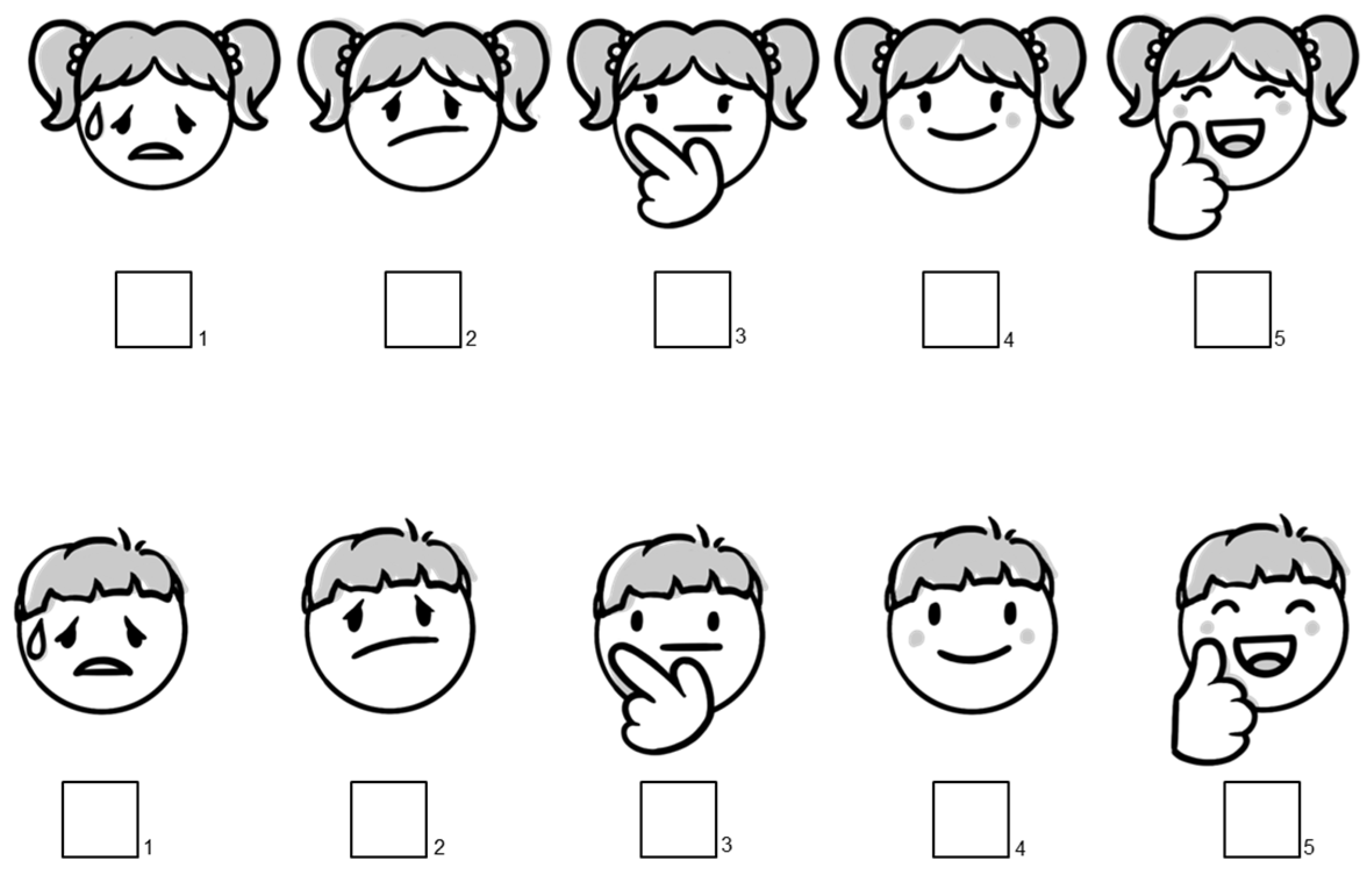
| A | 6–<18 y | (1) Previous experience with the formulations (“Ever taken?”: yes/no); (2) Preference for one formulation in a pairwise comparison with the other formulations (a total of 6 pairs possible); (3) Ranking of the 4 formulations according to their preference (from 1 = best to 4 = worst); (4) Rating of each formulation (“How much would you like to take this formulation 3 times daily for 1 week?’’) according to a 5-point scale presented as sex-specific smileys (Figure 1). |
| B | Parents of 0–<6 y | (1) Previous experience with the formulations (“Ever given to the child?”: yes/no); (2) Pairwise preference when comparing 1 mini-tablet vs. 0.5 mL syrup as well as the age-adapted maximal number of mini-tablets vs. the age-adapted maximal volume of syrup (Table 1); (3) Rating of the 4 age-adapted formulations regimens (“How much would you like to give this formulation to your child 3 times daily for 1 week?”) according to a 5-point scale presented as sex-specific smileys; The formulation regimens presented were 1 mini-tablet, 3 or 5 mini-tablets, 0.5 mL syrup, and 1 mL or 4.5 mL syrup. |
| C | Parents of 6–<18 y | (1) Previous experience with the formulations (“Ever given to the child/adolescent?”: yes/no); (2) Preference for one formulation in a pairwise comparison with the other formulations (a total of 6 pairs possible); (3) Ranking of the 4 formulations according to their preference (from 1 = best to 4 = worst); (4) Rating of each formulation (“How much would you like to take this formulation 3 times daily for 1 week?’’). |
| D | Nurses and Pediatricians | (1) Years of experience in the pediatric area categorized as 0–<5 y, 5–<10 y, and ≥10 y; (2) Previous experience (yes/no) with medicines given as mini-tablets, syrup, round tablet, or oblong tablet for each age group of pediatric patients; (3) Preference for one formulation in a pairwise comparison with the other formulations (a total of 6 pairs possible), specifically for each age group of pediatric patients; (4) Ranking of the 4 formulations according to their preference (from 1 = best to 4 = worst) for pediatric patients aged 6–<12 y and 12–<18 y; (5) Rating of each formulation (“How much would you like to give this formulation to children 3 times daily for 1 week?”) according to a 5-point scale presented as smileys, specifically for each age group of pediatric patients. |
| Participant Group | Formulation | Rating | ||||
|---|---|---|---|---|---|---|
| Very Bad | Bad | Indifferent | Good | Very Good | ||
| Age group 0–<2 years | ||||||
| Parents of children N = 30 (100%) | 1 MT | – | – | 2 (6.7%) | 11 (36.7%) | 17 (56.7%) |
| 3 MT | – | 2 (6.7%) | 6 (20.0%) | 8 (26.7%) | 14 (46.7%) | |
| 0.5 mL syrup | – | 6 (20.0%) | 12 (40.0%) | 7 (23.3%) | 5 (16.7%) | |
| 1.0 mL syrup | 10 (33.3%) | 9 (30.0%) | 6 (20.0%) | 4 (13.3%) | 1 (3.3%) | |
| Nurses N = 30 (100%) | 1 MT | – | 1 (3.3%) | 4 (13.3%) | 5 (16.7%) | 20 (66.7%) |
| 3 MT | 1 (3.3%) | 1 (3.3%) | 3 (10.0%) | 7 (23.3%) | 18 (60.0%) | |
| 0.5 mL syrup | – | 1 (3.3%) | 5 (16.7%) | 14 (46.7%) | 10 (33.3%) | |
| 1.0 mL syrup | – | 3 (10.0% | 10 (33.3%) | 14 (46.7%) | 3 (10.0%) | |
| Pediatricians N = 30 (100%) | 1 MT | 1 (3.3%) | – | – | 7 (23.3%) | 22 (73.3%) |
| 3 MT | 1 (3.3%) | – | 2 (6.7%) | 9 (30.0%) | 18 (60.0%) | |
| 0.5 mL syrup | – | 1 (3.3%) | 4 (13.3%) | 13 (43.3%) | 12 (40.0%) | |
| 1.0 mL syrup | 1 (3.3%) | 1 (3.3%) | 14 (46.7%) | 9 (30.0%) | 5 (16.7%) | |
| Age group 2–<6 years | ||||||
| Parents of children N = 30 (100%) | 1 MT | – | 1 (3.3%) | 5 (16.7%) | 16 (53.3%) | 8 (26.7%) |
| 5 MT | – | 7 (23.3%) | 7 (23.3%) | 11 (36.7%) | 5 (16.7%) | |
| 0.5 mL syrup | – | 7 (23.3%) | 7 (23.3%) | 14 (46.7%) | 2 (6.7%) | |
| 4.5 mL syrup | 6 (20.0%) | 11 (36.7%) | 5 (16.7%) | 6 (20.0%) | 2 (6.7%) | |
| Nurses N = 30 (100%) | 1 MT | – | 1 (3.3%) | 1 (3.3%) | 5 (16.7%) | 23 (76.7%) |
| 5 MT | 1 (3.3%) | – | 1 (3.3%) | 9 (30.0%) | 19 (63.3%) | |
| 0.5 mL syrup | – | 1 (3.3%) | 3 (10.0%) | 13 (43.3%) | 13 (43.3%) | |
| 4.5 mL syrup | 1 (3.3%) | 10 (33.3%) | 11 (36.7%) | 8 (26.7%) | – | |
| Pediatricians N = 30 (100%) | 1 MT | – | – | – | 3 (10.0%) | 27 (90.0%) |
| 5 MT | – | – | 1 (3.3%) | 9 (30.0%) | 20 (66.7%) | |
| 0.5 mL syrup | – | – | 3 (10.0%) | 14 (46.7%) | 13 (43.3%) | |
| 4.5 mL syrup | 1 (3.3%) | 6 (20.0%) | 15 (50.0%) | 6 (20.0%) | 2 (6.7%) | |
| Age group 6–<12 years | ||||||
| Children N = 30 (100%) | 1 MT | 1 (3.3%) | – | 4 (13.3%) | 7 (23.3%) | 18 (60.0%) |
| 11 MT | – | 3 (10.0%) | 8 (26.7%) | 11 (36.7%) | 8 (26.7%) | |
| 1 RT a | 5 (16.7%) | 4 (13.3%) | 10 (33.3%) | 6 (20.0%) | 5 (16.7%) | |
| 1 OT b | 1 (3.3%) | 5 (16.7%) | 7 (23.3%) | 9 (30.0%) | 8 (26.7%) | |
| 9.0 mL syrup | 3 (10.0%) | 5 (16.7%) | 6 (20.0%) | 8 (26.7%) | 8 (26.7%) | |
| Parents of children N = 30 (100%) | 1 MT | – | 1 (3.3%) | – | 10 (33.3%) | 19 (63.3%) |
| 11 MT | – | 4 (13.3%) | 6 (20.0%) | 11 (36.7%) | 9 (30.0%) | |
| 1 RT a | 3 (10.0%) | 6 (20.0%) | 11 (36.7%) | 9 (30.0%) | 1 (3.3%) | |
| 1 OT b | – | 6 (20.0%) | 5 (16.7%) | 11 (36.7%) | 8 (26.7%) | |
| 9.0 mL syrup | 5 (16.7%) | 6 (20.0%) | 9 (30.0%) | 7 (23.3%) | 3 (10.0%) | |
| Nurses N = 30 (100%) | 1 MT | – | – | – | 4 (13.3%) | 26 (86.7%) |
| 11 MT | – | – | 3 (10.0%) | 13 (43.3%) | 14 (46.7%) | |
| 1 RT a | – | 5 (16.7%) | 12 (40.0%) | 10 (33.3%) | 2 (6.7%) | |
| 1 OT b | – | 1 (3.3%) | 4 (13.3%) | 20 (66.7%) | 5 (16.7%) | |
| 9.0 mL syrup | 1 (3.3%) | 9 (30.0%) | 13 (43.3%) | 5 (16.7%) | 2 (6.7%) | |
| Pediatricians N = 30 (100%) | 1 MT | – | – | – | 2 (6.7%) | 28 (93.3%) |
| 11 MT | – | – | 2 (6.7%) | 11 (36.7%) | 17 (56.7%) | |
| 1 RT a | – | 3 (10.0%) | 10 (33.3%) | 14 (46.7%) | 3 (10.0%) | |
| 1 OT b | – | 1 (3.3%) | 6 (20.0%) | 12 (40.0%) | 11 (36.7%) | |
| 9.0 mL syrup | – | 3 (10.0%) | 17 (56.7%) | 8 (26.7%) | 2 (6.7%) | |
| Age group 12–<18 years | ||||||
| Adolescents N=30 (100%) | 1 MT | – | 1 (3.3%) | 2 (6.7%) | 6 (20.0%) | 21 (70.0%) |
| 70 MT | 3 (10.0%) | 1 (3.3%) | 11 (36.7%) | 11 (36.7%) | 4 (13.3%) | |
| 1 RT c | 1 (3.3%) | 4 (13.3%) | 7 (23.3%) | 14 (46.7%) | 4 (13.3%) | |
| 1 OT d | 2 (6.7%) | 2 (6.7%) | 5 (16.7%) | 15 (50.0%) | 6 (20.0%) | |
| 18.0 mL syrup | 3 (10.0%) | 7 (23.3%) | 8 (26.7%) | 8 (26.7%) | 4 (13.3%) | |
| Parents of adolescents N = 30 (100%) | 1 MT | 1 (3.3%) | – | 1 (3.3%) | 6 (20.0%) | 22 (73.3%) |
| 70 MT | – | 2 (6.7%) | 10 (33.3%) | 13 (43.3%) | 5 (16.7%) | |
| 1 RT c | 2 (6.7%) | 12 (40.0%) | 8 (26.7%) | 6 (20.0%) | 2 (6.7%) | |
| 1 OT d | 2 (6.7%) | 11 (36.7%) | 6 (20.0%) | 9 (30.0%) | 2 (6.7%) | |
| 18.0 mL syrup | 4 (13.3%) | 7 (23.3%) | 4 (13.3%) | 8 (26.7%) | 7 (23.3%) | |
| Nurses N = 30 (100%) | 1 MT | – | – | – | 4 (13.3%) | 26 (86.7%) |
| 70 MT | 1 (3.3%) | 2 (6.7%) | 9 (30.0%) | 11 (36.7%) | 7 (23.3%) | |
| 1 RT c | 5 (16.7%) | 8 (26.7%) | 9 (30.0%) | 5 (16.7%) | 3 (10.0%) | |
| 1 OT d | – | 4 (13.3%) | 11 (36.7%) | 11 (36.7%) | 4 (13.3%) | |
| 18.0 mL syrup | 13 (43.3%) | 8 (26.7%) | 6 (20.0%) | 2 (6.7%) | 1 (3.3%) | |
| Pediatricians N = 30 (100%) | 1 MT | – | 1 (3.3%) | – | 2 (6.7%) | 27 (90.0%) |
| 70 MT | 1 (3.3%) | 2 (6.7%) | 11 (36.7%) | 9 (30.0%) | 7 (23.3%) | |
| 1 RT c | 2 (6.7%) | 7 (23.3%) | 9 (30.0%) | 9 (30.0%) | 3 (10.0%) | |
| 1 OT d | 1 (3.3%) | 3 (10.0%) | 8 (26.7%) | 11 (36.7%) | 7 (23.3%) | |
| 18.0 mL syrup | 5 (16.7%) | 11 (36.7%) | 10 (33.3%) | 3 (10.0%) | 1 (3.3%) | |
| Age Group (Years) | Preference Comparison | Children N = 30 (100%) | Parents of Children N = 30 (100%) | Nurses N = 30 (100%) | Pediatricians N = 30 (100%) |
|---|---|---|---|---|---|
| 0–<2 | 1 MT vs. 0.5 mL syrup | – | 23 (76.7%) | 17 (56.7%) | 20 (66.7%) |
| 3 MT vs. 1.0 mL syrup | – | 28 (93.3%) | 19 (63.3%) | 20 (66.7%) | |
| 2–<6 | 1 MT vs. 0.5 mL syrup | – | 21 (70.0%) | 24 (80.0%) | 27 (90.0%) |
| 5 MT vs. 5.0 mL syrup | – | 21 (70.0%) | 27 (90.0%) | 27 (90.0%) | |
| 6–<12 | 11 MT vs. 1 RT a | 19 (63.3%) | 22 (73.3%) | 16 (53.3%) | 18 (60.0%) |
| 11 MT vs. 1 OT b | 17 (56.7%) | 15 (50.0%) | 9 (30.0%) | 10 (33.3%) | |
| 11 MT vs. 9.0 mL syrup | 21 (70.0%) | 23 (76.7%) | 23 (76.7%) | 28 (93.3%) | |
| 1 RT a vs. 1 OT b | 12 (40.0%) | 10 (33.3%) | 5 (16.7%) | 3 (10.0%) | |
| 1 RT a vs. 9.0 mL syrup | 16 (53.3%) | 12 (40.0%) | 17 (56.7%) | 22 (73.3%) | |
| 1 OT b vs. 9.0 mL syrup | 18 (60.0%) | 18 (60.0%) | 24 (80.0%) | 26 (86.7%) | |
| 12–<18 | 70 MT vs. 1 RT c | 13 (43.3%) | 22 (73.3%) | 15 (50.0%) | 18 (60.0%) |
| 70 MT vs. 1 OT d | 11 (36.7%) | 23 (76.7%) | 8 (26.7%) | 12 (40.0%) | |
| 70 MT vs. 18.0 mL syrup | 15 (50.0%) | 18 (60.0%) | 26 (86.7%) | 17 (56.7%) | |
| 1 RT c vs. 1 OT d | 13 (43.3%) | 10 (33.3%) | 1 (3.3%) | 4 (13.3%) | |
| 1 RT c vs. 18.0 mL syrup | 20 (66.7%) | 15 (50.0%) | 25 (83.3%) | 20 (66.7%) | |
| 1 OT d vs. 18.0 mL syrup | 18 (60.0%) | 15 (50.0%) | 28 (93.3%) | 24 (80.0%) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wargenau, M.; Baase, F.; Eckardt, K.; Spitzhorn, L.-S.; Reidemeister, S.; Klingmann, I.; Klingmann, V. Questionnaire Study to Investigate the Preferences of Children, Parents, and Healthcare Professionals for Different Formulations of Oral Medicinal Products. Pharmaceutics 2024, 16, 515. https://doi.org/10.3390/pharmaceutics16040515
Wargenau M, Baase F, Eckardt K, Spitzhorn L-S, Reidemeister S, Klingmann I, Klingmann V. Questionnaire Study to Investigate the Preferences of Children, Parents, and Healthcare Professionals for Different Formulations of Oral Medicinal Products. Pharmaceutics. 2024; 16(4):515. https://doi.org/10.3390/pharmaceutics16040515
Chicago/Turabian StyleWargenau, Manfred, Felicitas Baase, Kristin Eckardt, Lucas-Sebastian Spitzhorn, Sibylle Reidemeister, Ingrid Klingmann, and Viviane Klingmann. 2024. "Questionnaire Study to Investigate the Preferences of Children, Parents, and Healthcare Professionals for Different Formulations of Oral Medicinal Products" Pharmaceutics 16, no. 4: 515. https://doi.org/10.3390/pharmaceutics16040515
APA StyleWargenau, M., Baase, F., Eckardt, K., Spitzhorn, L.-S., Reidemeister, S., Klingmann, I., & Klingmann, V. (2024). Questionnaire Study to Investigate the Preferences of Children, Parents, and Healthcare Professionals for Different Formulations of Oral Medicinal Products. Pharmaceutics, 16(4), 515. https://doi.org/10.3390/pharmaceutics16040515