

Optimization of Sodium Iodide-Based Root Filling Material for Clinical Applications: Enhancing Physicochemical Properties
 , , , , , , , and
, , , , , , , and 
Abstract
1. Introduction
2. Material and Methods
2.1. Preparation for Sample
2.2. Physicochemical Characteristics of Samples
2.3. Solubility
2.3.1. Flow
2.3.2. Film Thickness
2.3.3. Optical Images
2.3.4. Radiopacity
2.3.5. Injectability
2.3.6. Viscosity
2.3.7. Extraction Test
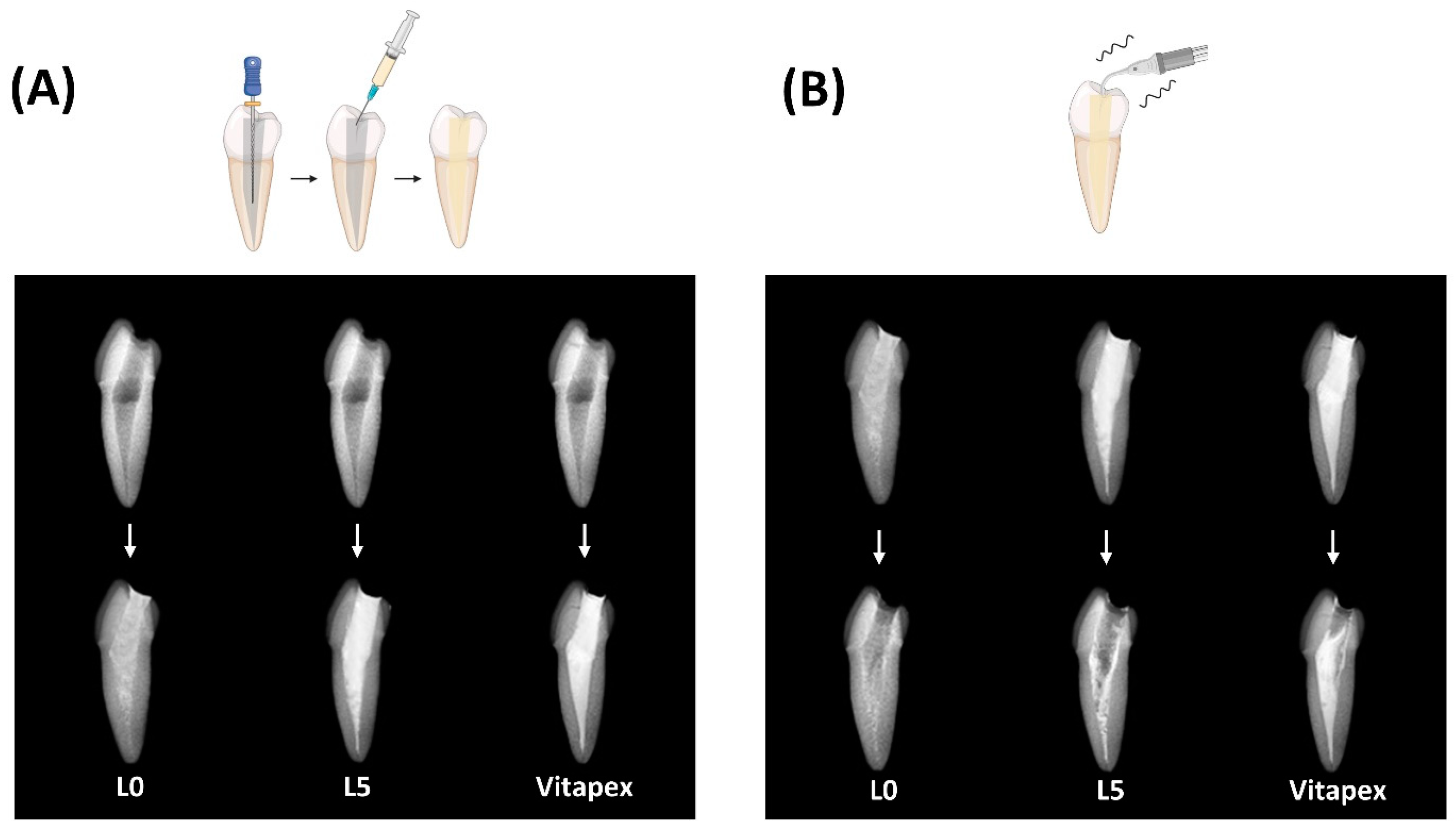
2.3.8. Endodontic Treatment for Resin Tooth
- (1)
- Root-filling ability evaluation
- (2)
- Removability of Pastes
2.4. Antibacterial Test
2.5. Statistical Analysis
3. Results
3.1. Physicochemical Properties
3.1.1. Solubility
3.1.2. Flow
3.1.3. Film Thickness
3.1.4. Optical Images
3.1.5. Radiopacity
3.1.6. Injectability
3.1.7. Viscosity
3.1.8. Extraction Test
3.1.9. Endodontic Treatment for Resin Tooth
- (1)
- Root-filling ability evaluation
- (2)
- Removability of paste
3.2. Antibacterial Test for Paste
4. Discussion
5. Conclusions
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
References
- Takiguchi, M.; Fujiwara, T.; Sobue, S.; Ooshima, T. Radicular cyst associated with a primary molar following pulp therapy: A case report. Int. J. Paediatr. Dent. 2001, 11, 452–455. [Google Scholar] [CrossRef] [PubMed]
- Mass, E.; Kaplan, I.; Hirshberg, A. A clinical and histopathological study of radicular cysts associated with primary molars. J. Oral Pathol. Med. 1995, 24, 458–461. [Google Scholar] [CrossRef] [PubMed]
- Savage, N.; Adkins, K.; Weir, A.; Grundy, G. An histological study of cystic lesions following pulp therapy in deciduous molars. J. Oral Pathol. Med. 1986, 15, 209–212. [Google Scholar] [CrossRef] [PubMed]
- Bhat, S.S.; Vidhya, M.; Sargod, S. Radicular cyst associated with endodontically treated deciduous tooth: A case report. J. Indian Soc. Pedod. Prev. Dent. 2003, 21, 139–141. [Google Scholar] [PubMed]
- Rifkin, A. The root canal treatment of abscessed primary teeth—A three to four year follow-up. ASDC J. Dent. Child. 1982, 49, 428–431. [Google Scholar] [PubMed]
- Petel, R.; Moskovitz, M.; Tickotsky, N.; Halabi, A.; Goldstein, J.; Houri-Haddad, Y. Cytotoxicity and proliferative effects of Iodoform-containing root canal-filling material on RAW 264.7 macrophage and RKO epithelial cell lines. Arch. Oral Biol. 2013, 58, 75–81. [Google Scholar] [CrossRef] [PubMed]
- Moskovitz, M.; Tickotsky, N.; Ashkar, H.; Holan, G. Degree of root resorption after root canal treatment with iodoform-containing filling material in primary molars. Quintessence Int. 2012, 43, 361–368. [Google Scholar] [PubMed]
- Nakornchai, S.; Banditsing, P.; Visetratana, N. Clinical evaluation of 3Mix and Vitapex® as treatment options for pulpally involved primary molars. Int. J. Paediatr. Dent. 2010, 20, 214–221. [Google Scholar] [CrossRef] [PubMed]
- Nurko, C.; Garcia-Godoy, F. Evaluation of a calcium hydroxide/iodoform paste (Vitapex) in root canal therapy for primary teeth. J. Clin. Pediatr. Dent. 1999, 23, 289–294. [Google Scholar]
- Estrela, C.; Estrela, C.R.d.A.; Hollanda, A.C.B.; Decurcio, D.d.A.; Pécora, J.D. Influence of iodoform on antimicrobial potential of calcium hydroxide. J. Appl. Oral Sci. 2006, 14, 33–37. [Google Scholar] [CrossRef]
- Smith, V.E.; Read, M.L.; Turnell, A.S.; Watkins, R.J.; Watkinson, J.C.; Lewy, G.D.; Fong, J.C.; James, S.R.; Eggo, M.C.; Boelaert, K. A novel mechanism of sodium iodide symporter repression in differentiated thyroid cancer. J. Cell Sci. 2009, 122, 3393–3402. [Google Scholar] [CrossRef] [PubMed]
- Choi, J.-M.; Vu, H.T.; Shin, S.-J.; Ahn, J.-Y.; Kim, Y.-J.; Song, S.; Han, M.-R.; Lee, J.-H.; Kim, J.-S.; Knowles, J.C. Improvement of Biological Effects of Root-Filling Materials for Primary Teeth by Incorporating Sodium Iodide. Molecules 2022, 27, 2927. [Google Scholar] [CrossRef]
- Jacenko, O. c-Fos and bone loss: A proto-oncogene regulates osteoclast lineage determination. BioEssays 1995, 17, 277–281. [Google Scholar] [CrossRef]
- Fujisaki, K.; Tanabe, N.; Suzuki, N.; Kawato, T.; Takeichi, O.; Tsuzukibashi, O.; Makimura, M.; Ito, K.; Maeno, M. Receptor activator of NF-κB ligand induces the expression of carbonic anhydrase II, cathepsin K, and matrix metalloproteinase-9 in osteoclast precursor RAW264. 7 cells. Life Sci. 2007, 80, 1311–1318. [Google Scholar] [CrossRef]
- Chang, S.J.; Kim, Y.; Lee, J.; Kim, J.; Lee, J.; Han, M.R.; Shin, J.; Kim, J. Effectiveness of Sodium Iodide Root Canal Filling Pastes in Primary Teeth. J. Korean Acad. Pediatr. Dent. 2023, 50, 168–178. [Google Scholar] [CrossRef]
- ISO 6876:2012; Dentistry—Root Canal Sealing Materials. ISO: Geneva, Switzerland, 2012.
- Faria-Júnior, N.; Tanomaru-Filho, M.; Berbert, F.L.C.V.; Guerreiro-Tanomaru, J. Antibiofilm activity, pH and solubility of endodontic sealers. Int. Endod. J. 2013, 46, 755–762. [Google Scholar] [CrossRef] [PubMed]
- Kuga, M.C.; Faria, G.; So, M.V.; Keine, K.C.; Santos, A.D.d.; Duarte, M.A.H.; Kopper, P.M.P. The impact of the addition of iodoform on the physicochemical properties of an epoxy-based endodontic sealer. J. Appl. Oral Sci. 2014, 22, 125–130. [Google Scholar] [CrossRef]
- Marques, R.P.d.S.; Moura-Netto, C.; Oliveira, N.M.d.; Bresolin, C.R.; Mello-Moura, A.C.V.; Mendes, F.M.; Novaes, T.F. Physicochemical properties and filling capacity of an experimental iodoform-based paste in primary teeth. Braz. Oral Res. 2020, 34, e089. [Google Scholar] [CrossRef]
- Kumar, V.; Sharma, V.K.; Kalonia, D.S. Effect of polyols on polyethylene glycol (PEG)-induced precipitation of proteins: Impact on solubility, stability and conformation. Int. J. Pharm. 2009, 366, 38–43. [Google Scholar] [CrossRef]
- Xie, Y.; Hettiarachchy, N. Xanthan gum effects on solubility and emulsification properties of soy protein isolate. J. Food Sci. 1997, 62, 1101–1104. [Google Scholar] [CrossRef]
- Osborne, D.W. Phase behavior characterization of ointments containing lanolin or a lanolin substitute. Drug Dev. Ind. Pharm. 1993, 19, 1283–1302. [Google Scholar] [CrossRef]
- Húngaro Duarte, M.A.; D’arc de Oliveira El, G.; Vivan, R.R.; Tanomaru, J.M.G.; Tanomaru Filho, M.; de Moraes, I.G. Radiopacity of portland cement associated with different radiopacifying agents. J. Endod. 2009, 35, 737–740. [Google Scholar] [CrossRef] [PubMed]
- Robinson, T.E.; Hughes, E.A.; Bose, A.; Cornish, E.A.; Teo, J.Y.; Eisenstein, N.M.; Grover, L.M.; Cox, S.C. Filling the gap: A correlation between objective and subjective measures of injectability. Adv. Healthc. Mater. 2020, 9, 1901521. [Google Scholar] [CrossRef] [PubMed]
- Bang, S.-J.; Jun, S.-K.; Kim, Y.-J.; Ahn, J.-Y.; Vu, H.T.; Mandakhbayar, N.; Han, M.-R.; Lee, J.-H.; Kim, J.-B.; Kim, J.-S. Characterization of physical and biological properties of a caries-arresting liquid containing copper doped bioglass nanoparticles. Pharmaceutics 2022, 14, 1137. [Google Scholar] [CrossRef] [PubMed]
- Kang, T.-Y.; Choi, J.-W.; Seo, K.-J.; Kim, K.-M.; Kwon, J.-S. Physical, chemical, mechanical, and biological properties of four different commercial root-end filling materials: A comparative study. Materials 2021, 14, 1693. [Google Scholar] [CrossRef] [PubMed]
- Chawla, H.; Setia, S.; Gupta, N.; Gauba, K.; Goyal, A. Evaluation of a mixture of zinc oxide, calcium hydroxide, and sodium fluoride as a new root canal filling material for primary teeth. J. Indian Soc. Pedod. Prev. Dent. 2008, 26, 53–58. [Google Scholar] [CrossRef] [PubMed]
- Jung, C.; Kim, S.; Sun, T.; Cho, Y.-B.; Song, M. Pulp-dentin regeneration: Current approaches and challenges. J. Tissue Eng. 2019, 10, 2041731418819263. [Google Scholar] [CrossRef] [PubMed]
- Fuks, A.; Eidelman, E.; Pauker, N. Root fillings with Endoflas in primary teeth: A retrospective study. J. Clin. Pediatr. Dent. 2003, 27, 41–45. [Google Scholar] [CrossRef] [PubMed]
- Chang, S.-J.; Kim, Y.-J.; Vu, H.T.; Choi, J.-M.; Park, J.-H.; Shin, S.-J.; Dashnyam, K.; Knowles, J.C.; Lee, H.-H.; Jun, S.-K. Physicochemical, Pre-Clinical, and Biological Evaluation of Viscosity Optimized Sodium Iodide-Incorporated Paste. Pharmaceutics 2023, 15, 1072. [Google Scholar] [CrossRef]
- Amorim, L.d.F.G.d.; Toledo, O.A.d.; Estrela, C.R.d.A.; Decurcio, D.d.A.; Estrela, C. Antimicrobial analysis of different root canal filling pastes used in pediatric dentistry by two experimental methods. Braz. Dent. J. 2006, 17, 317–322. [Google Scholar] [CrossRef]
- Bawazir, O.A.; Salama, F.S. Clinical evaluation of root canal obturation methods in primary teeth. Pediatr. Dent. 2006, 28, 39–47. [Google Scholar]
- Barcelos, R.; Santos, M.; Primo, L.; Luiz, R.; Maia, L. ZOE paste pulpectomies outcome in primary teeth: A systematic review. J. Clin. Pediatr. Dent. 2011, 35, 241–248. [Google Scholar] [CrossRef] [PubMed]
- Coll, J.; Sadrian, R. Predicting pulpectomy success and its relationship to exfoliation and succedaneous dentition. Pediatr. Dent. 1996, 18, 57–63. [Google Scholar] [PubMed]
- Moskovitz, M.; Sammara, E.; Holan, G. Success rate of root canal treatment in primary molars. J. Dent. 2005, 33, 41–47. [Google Scholar] [CrossRef]
- Rifkin, A. A simple, effective, safe technique for the root canal treatment of abscessed primary teeth. ASDC J. Dent. Child. 1980, 47, 435–441. [Google Scholar]
- Najjar, R.S.; Alamoudi, N.M.; El-Housseiny, A.A.; Al Tuwirqi, A.A.; Sabbagh, H.J. A comparison of calcium hydroxide/iodoform paste and zinc oxide eugenol as root filling materials for pulpectomy in primary teeth: A systematic review and meta-analysis. Clin. Exp. Dent. Res. 2019, 5, 294–310. [Google Scholar] [CrossRef]
- Erausquin, J.; Muruzábal, M. Root canal fillings with zinc oxide-eugenol cement in the rat molar. Oral Surg. Oral Med. Oral Pathol. 1967, 24, 547–558. [Google Scholar] [CrossRef]
- Spedding, R. Incomplete resorption of resorbable zinc oxide root canal fillings in primary teeth: Report of two cases. ASDC J. Dent. Child. 1985, 52, 214–216. [Google Scholar] [PubMed]
- Hendry, J.A.; Jeansonne, B.G.; Dummett, C.O., Jr.; Burrell, W. Comparison of calcium hydroxide and zinc oxide and eugenol pulpectomies in primary teeth of dogs. Oral Surg. Oral Med. Oral Pathol. 1982, 54, 445–451. [Google Scholar] [CrossRef]
- Nurko, C.; Ranly, D.; García-Godoy, F.; Lakshmyya, K. Resorption of a calcium hydroxide/iodoform paste (Vitapex) in root canal therapy for primary teeth: A case report. Pediatr. Dent. 2000, 22, 517–520. [Google Scholar]
- Reddy, G.K.; Enwemeka, C.S. A simplified method for the analysis of hydroxyproline in biological tissues. Clin. Biochem. 1996, 29, 225–229. [Google Scholar] [CrossRef] [PubMed]
- Fava, L.; Saunders, W. Calcium hydroxide pastes: Classification and clinical indications. Int. Endod. J. 1999, 32, 257–282. [Google Scholar] [CrossRef] [PubMed]
- Carvalho-Junior, J.R.; Correr-Sobrinho, L.; Correr, A.B.; Sinhoreti, M.A.; Consani, S.; Sousa-Neto, M.D. Solubility and dimensional change after setting of root canal sealers: A proposal for smaller dimensions of test samples. J. Endod. 2007, 33, 1110–1116. [Google Scholar] [CrossRef] [PubMed]
- Pilownic, K.J.; Gomes, A.P.N.; Wang, Z.J.; Almeida, L.H.S.; Romano, A.R.; Shen, Y.; Felix, A.d.O.C.; Haapasalo, M.; Pappen, F.G. Physicochemical and biological evaluation of endodontic filling materials for primary teeth. Braz. Dent. J. 2017, 28, 578–586. [Google Scholar] [CrossRef] [PubMed]
- Pramila, R.; Muthu, M.; Deepa, G.; Farzan, J.; Rodrigues, S. Pulpectomies in primary mandibular molars: A comparison of outcomes using three root filling materials. Int. Endod. J. 2016, 49, 413–421. [Google Scholar] [CrossRef] [PubMed]
- Dahake, P.T.; Joshi, S.S.; Kale, Y.J.; Dadpe, M.V.; Kendre, S.B. Biocompatibility of Ajwain Oil Combined with Eugenol and Zinc Oxide as a Deciduous Root Canal Obturating Material: An In Vivo Study. Int. J. Clin. Pediatr. Dent. 2023, 16, 431. [Google Scholar] [PubMed]
- Setty, J.V.; Srinivasan, I.; Sathiesh, R.T. Comparative Evaluation of Myristica fragrans Essential Oil-Zinc Oxide Mixture with Zinc Oxide Eugenol in Root Canal Filling of Primary Teeth: An In Vivo Study. Int. J. Clin. Pediatr. Dent. 2023, 16, 237–243. [Google Scholar]
- Estrela, C.; Bammann, L.; Pimenta, F.; Pécora, J. Control of microorganisms in vitro by calcium hydroxide pastes. Int. Endod. J. 2001, 34, 341–345. [Google Scholar] [CrossRef]
- Estrela, C.; Mamede Neto, I.; Estrela, C.R.; Pécora, J.D. Evaluation of density of calcium hydroxide pastes in dog’s mandible. Braz. Endod. J. 1998, 3, 24–30. [Google Scholar]
- Estrela, C.; Sydney, G.B.; Bammann, L.L.; Felippe Junior, O. Mechanism of the action of calcium and hydroxy ions of calcium hydroxide on tissue and bacteria. Braz. Dent. J. 1995, 6, 85–90. [Google Scholar]
- Ordinola-Zapata, R.; Bramante, C.M.; GarcÍa-godoy, F.; Moldauer, B.I.; Minotti, P.G.; TercíLIA Grizzo, L.; Duarte, M.A.H. The effect of radiopacifiers agents on p H, calcium release, radiopacity, and antimicrobial properties of different calcium hydroxide dressings. Microsc. Res. Tech. 2015, 78, 620–625. [Google Scholar] [CrossRef]
- Reddy, V. Clinical and radiological evaluation of zinc oxide-eugenol and Maisto’s paste as obturating materials in infected primary teeth--nine months study. J. Indian Soc. Pedod. Prev. Dent. 1996, 14, 39–44. [Google Scholar] [PubMed]
- Chen, J.W.; Jorden, M. Materials for primary tooth pulp treatment: The present and the future. Endod. Top. 2010, 23, 41–49. [Google Scholar] [CrossRef]
- Zargar, N.; Rezvani, Y.; Eftekhar, L. Characteristics of Root Canal Filling Materials for Primary Teeth: A Review of Literature. J. Dent. Sch. Shahid Beheshti Univ. Med. Sci. 2021, 39, 110–114. [Google Scholar]
- Zacharczuk, G.A.; Toscano, M.A.; López, G.E.; Ortolani, A.M. Evaluación de 3Mix-MP y pulpectomías en molares primarios no vitales. Acta Odontol. Latinoam. 2019, 32, 22–28. [Google Scholar] [PubMed]
- James, A.R. Radiographic Evaluation of Three Obturation Techniques in Primary Molars an In-Vivo Study. Master’s Thesis, Rajiv Gandhi University of Health Sciences, Bengaluru, India, 2009. [Google Scholar]
- Murata, S.S.; Holland, R.; Souza, V.d.; Dezan Junior, E.; Grossi, J.A.d.; Percinoto, C. Histological analysis of the periapical tissues of dog deciduous teeth after root canal filling with diferent materials. J. Appl. Oral Sci. 2005, 13, 318–324. [Google Scholar] [CrossRef]
- Liebreich, O. Observations on the Practical Uses of Lanolin. Br. Med. J. 1886, 1, 282. [Google Scholar] [CrossRef] [PubMed]
- Neto, C.M.; de Albuquerque, R.S.; de Souza, S.C.; Giesta, R.O.; Fernandes, A.P.S.; Mondin, B. Comparative study of the use of hpa lanolin and breast milk for treating pain associated with nipple trauma. Rev. Bras. Ginecol. Obstet./RBGO Gynecol. Obstet. 2018, 40, 664–672. [Google Scholar]
- Alonso, C.; Collini, I.; Carrer, V.; Barba, C.; Martí, M.; Coderch, L. Permeation kinetics of active drugs through lanolin-based artificial membranes. Colloids Surf. B Biointerfaces 2020, 192, 111024. [Google Scholar] [CrossRef]
- Kleckner, M.S., Jr.; Allen, E.V.; Wakim, K.G. The effect of local application of glyceryl trinitrate (nitroglycerine) on Raynaud’s disease and Raynaud’s phenomenon: Studies on blood flow and clinical manifestations. Circulation 1951, 3, 681–689. [Google Scholar] [CrossRef]
- Özdemir, O.; Kopac, T. Cytotoxicity and biocompatibility of root canal sealers: A review on recent studies. J. Appl. Biomater. Funct. Mater. 2022, 20, 22808000221076325. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Ca(OH)2 | NaI (Iodoform) | Silicone Oil | PEG | Xantangum | Lanolin | Others | Sum | ||
|---|---|---|---|---|---|---|---|---|---|
| A | D30 | 1 | 1 | 1 | 3 | ||||
| 33.33 | 33.33 | 33.33 | 100 | ||||||
| Oil up-1 | 1 | 1 | 1 | 3.5 | |||||
| 28.57 | 28.57 | 42.86 | 100 | ||||||
| Oil up-2 | 1 | 1 | 2 | 4 | |||||
| 25 | 25 | 50 | 100 | ||||||
| Low Ca(OH)2 | 0.5 | 1.5 | 1 | 3 | |||||
| 16.67 | 50 | 33.33 | 100 | ||||||
| Low NaI | 1.5 | 0.5 | 1 | 3 | |||||
| 50 | 16.67 | 33.33 | 100 | ||||||
| B | PEG | 0.95 | 0.95 | 1.9 | 0.2 | 4 | |||
| 23.75 | 23.75 | 47.5 | 5 | 100 | |||||
| Xantangum | 0.95 | 0.95 | 1.9 | 0.2 | 4 | ||||
| 23.75 | 23.75 | 47.5 | 5 | 100 | |||||
| Lanolin | 0.95 | 0.95 | 1.9 | 0.2 | 4 | ||||
| 23.75 | 23.75 | 47.5 | 5 | 100 | |||||
| C | Lanolin | 0.95 | 0.95 | 1.9 | 0.2 | 4 | |||
| 23.75 | 23.75 | 47.5 | 5 | 100 | |||||
| Oil down-1 | 1.05 | 1.05 | 1.7 | 0.2 | 4 | ||||
| 26.25 | 26.25 | 42.5 | 5 | 100 | |||||
| Oil down-2 | 1.15 | 1.15 | 1.5 | 0.2 | 4 | ||||
| 28.75 | 28.75 | 37.5 | 5 | 100 | |||||
| Oil down-3 | 1.25 | 1.25 | 1.3 | 0.2 | 4 | ||||
| 31.25 | 31.25 | 32.5 | 5 | 100 | |||||
| D | L 0 | 1.15 | 1.15 | 1.7 | 4 | ||||
| 28.75 | 28.75 | 42.5 | 100 | ||||||
| L 2.5 | 1.15 | 1.15 | 1.6 | 0.1 | 4 | ||||
| 28.75 | 28.75 | 40 | 2.5 | 100 | |||||
| L 5 | 1.15 | 1.15 | 1.5 | 0.2 | 4 | ||||
| 28.75 | 28.75 | 37.5 | 5 | 100 | |||||
| L 7.5 | 1.15 | 1.15 | 1.4 | 0.3 | 4 | ||||
| 28.75 | 28.75 | 35 | 7.5 | 100 | |||||
| Vitapex | 30.3 | 40.4 | 22.4 | 6.9 | 100 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Park, H.-S.; Kim, Y.-J.; Chang, S.-J.; Lee, H.-H.; Han, M.-R.; Lee, J.-H.; Kim, J.-S.; Kim, J.-B.; Shin, J.-S.; Lee, J.-H. Optimization of Sodium Iodide-Based Root Filling Material for Clinical Applications: Enhancing Physicochemical Properties. Pharmaceutics 2024, 16, 1031. https://doi.org/10.3390/pharmaceutics16081031
Park H-S, Kim Y-J, Chang S-J, Lee H-H, Han M-R, Lee J-H, Kim J-S, Kim J-B, Shin J-S, Lee J-H. Optimization of Sodium Iodide-Based Root Filling Material for Clinical Applications: Enhancing Physicochemical Properties. Pharmaceutics. 2024; 16(8):1031. https://doi.org/10.3390/pharmaceutics16081031
Chicago/Turabian StylePark, Hye-Shin, Yu-Jin Kim, Soo-Jin Chang, Hae-Hyoung Lee, Mi-Ran Han, Joon-Haeng Lee, Jong-Soo Kim, Jong-Bin Kim, Ji-Sun Shin, and Jung-Hwan Lee. 2024. "Optimization of Sodium Iodide-Based Root Filling Material for Clinical Applications: Enhancing Physicochemical Properties" Pharmaceutics 16, no. 8: 1031. https://doi.org/10.3390/pharmaceutics16081031
APA StylePark, H.-S., Kim, Y.-J., Chang, S.-J., Lee, H.-H., Han, M.-R., Lee, J.-H., Kim, J.-S., Kim, J.-B., Shin, J.-S., & Lee, J.-H. (2024). Optimization of Sodium Iodide-Based Root Filling Material for Clinical Applications: Enhancing Physicochemical Properties. Pharmaceutics, 16(8), 1031. https://doi.org/10.3390/pharmaceutics16081031