
Nurses’ Protests during the COVID-19 Pandemic: A Comparative International Analysis


Abstract
1. Introduction
2. Materials and Methods
2.1. Definitions and Data
2.2. Data Analysis
3. Results
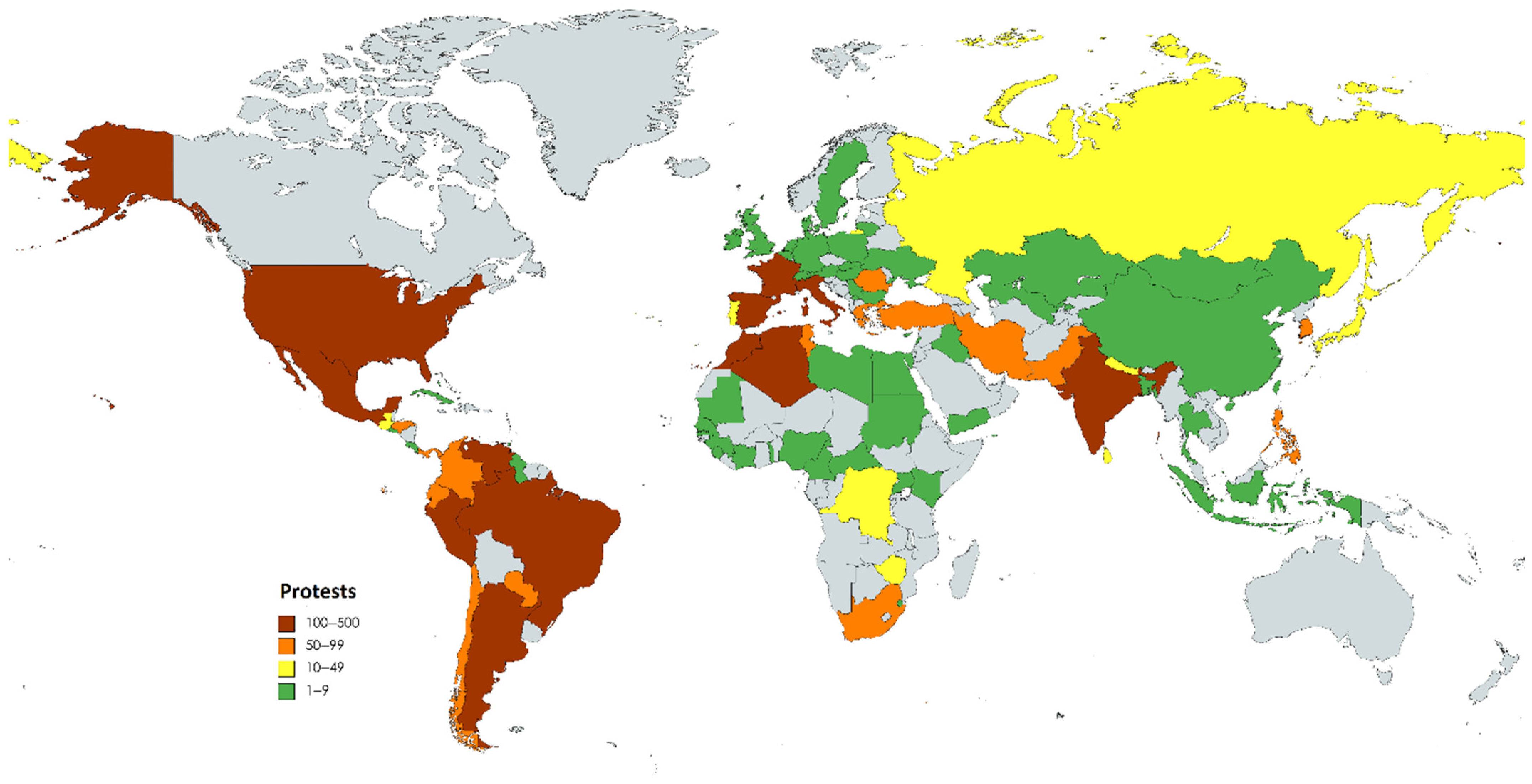
3.1. What Was the Spatial Distribution of Protests, and Which Countries Were Particularly Affected?
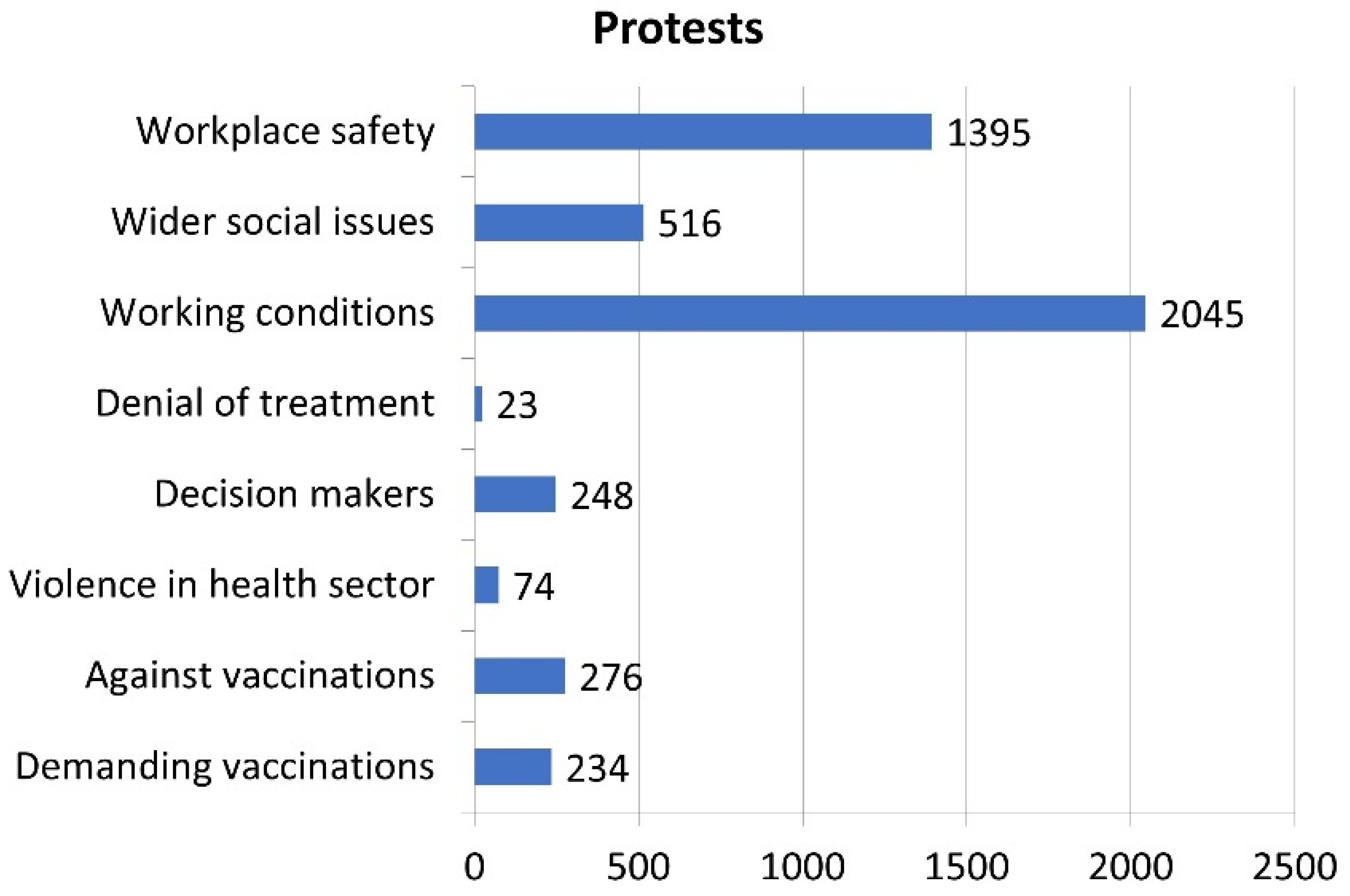
3.2. What Were the Stated Reasons for Protests?
3.3. How Did Protest Patterns Change over Time?
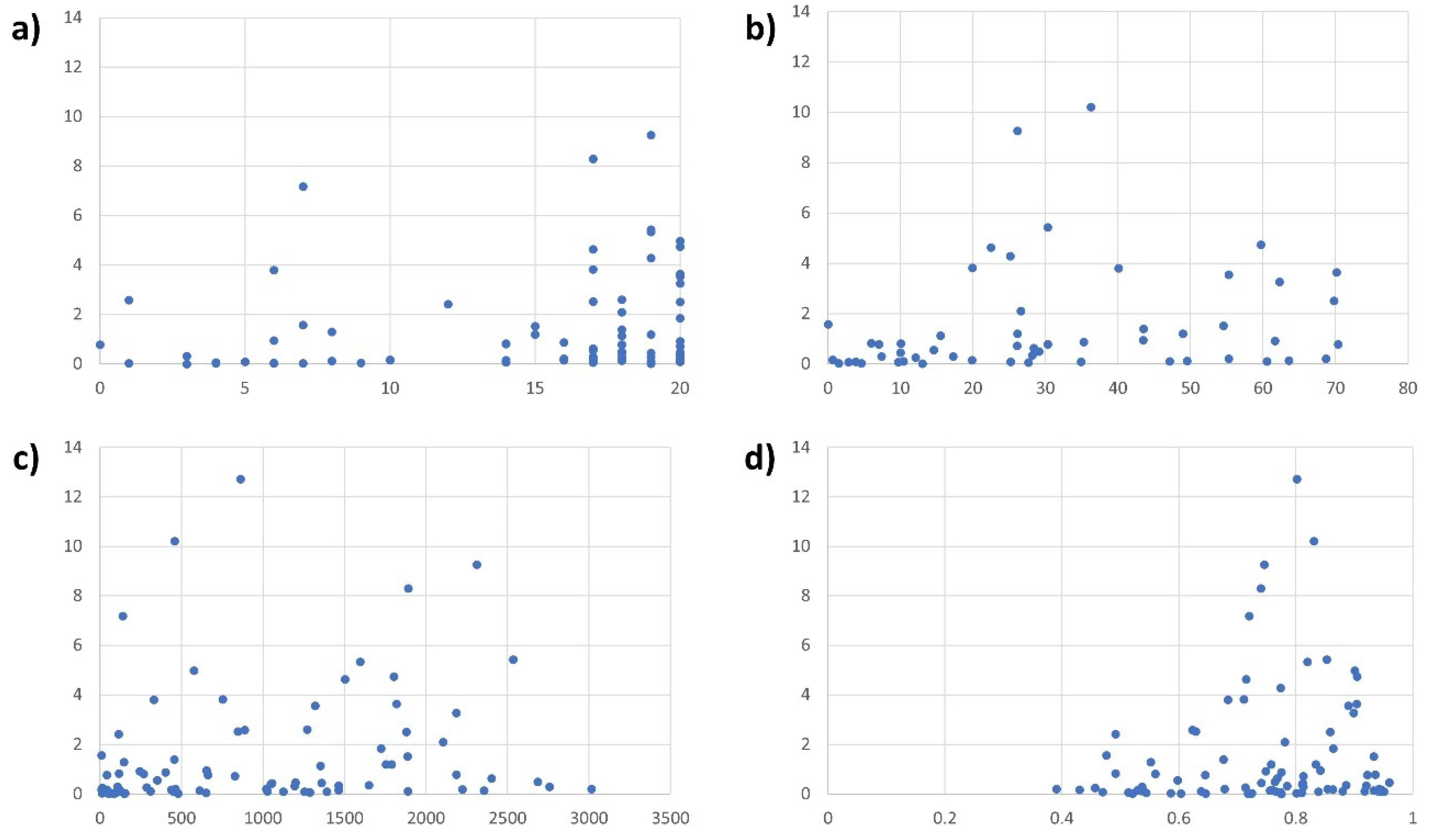
3.4. Which Socio-Economic Conditions Can Explain Higher Protest Occurrence?
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Public Involvement Statement
Guidelines and Standards Statement
Use of Artificial Intelligence
Acknowledgments
Conflicts of Interest
References
- Mathieu, E.; Ritchie, H.; Rodés-Guirao, L.; Appel, C.; Giattino, C.; Hasell, J.; Macdonald, B.; Dattani, S.; Beltekian, D.; Ortiz-Ospina, E.; et al. Coronavirus Pandemic (COVID-19). 2024. Available online: https://ourworldindata.org/coronavirus (accessed on 21 May 2024).
- Woodrow, M.; Carey, C.; Ziauddeen, N.; Thomas, R.; Akrami, A.; Lutje, V.; Greenwood, D.C.; Alwan, N.A. Systematic review of the prevalence of long COVID. Open Forum Infect. Dis. 2023, 10, ofad233. [Google Scholar] [CrossRef] [PubMed]
- UNDP. New Threats to Human Security in the Anthropocene: Demanding Greater Solidarity; UNDP: New York, NY, USA, 2022. [Google Scholar]
- Jacobi, D.; Ide, T. Collective violence against health workers in the context of the COVID-19 pandemic. Nurs. Rep. 2023, 13, 902–912. [Google Scholar] [CrossRef]
- Breslawski, J. Armed groups and public health emergencies: A cross-country look at armed groups’ responses to COVID-19. J. Glob. Secur. Stud. 2022, 7, ogab017. [Google Scholar] [CrossRef]
- Nishikawa, A.; Yamaguchi, T.; Yamada, Y.; Urata, H.; Shinkawa, T.; Matsunari, Y. How do disaster relief nurses in Japan perceive and respond to risks? A cross-sectional study. Nurs. Rep. 2023, 13, 1410–1420. [Google Scholar] [CrossRef] [PubMed]
- Dye, T.D.; Alcantara, L.; Siddiqi, S.; Barbosu, M.; Sharma, S.; Panko, T.; Pressman, E. Risk of COVID-19-related bullying, harassment and stigma among healthcare workers: An analytical cross-sectional global study. BMJ Open 2020, 10, e046620. [Google Scholar] [CrossRef]
- Zhang, S.X.; Chen, J.; Afshar Jahanshahi, A.; Alvarez-Risco, A.; Dai, H.; Li, J.; Patty-Tito, R.M. Succumbing to the COVID-19 pandemic: Healthcare workers not satisfied and intend to leave their jobs. Int. J. Ment. Health Addict. 2022, 20, 956–965. [Google Scholar] [CrossRef]
- Cipriano, P.F.; Boston-Leary, K.; McMillan, K.; Peterson, C. The US COVID-19 crises: Facts, science and solidarity. Int. Nurs. Rev. 2020, 67, 437–444. [Google Scholar] [CrossRef]
- Romero-Martín, M.; Gómez-Salgado, J.; Alcaide-Carrasco, M.; Rodríguez-Jiménez, L.; Ortega-Moreno, M.; López-López, D.; Ruiz-Frutos, C. Impact of the COVID-19 Pandemic on the Work Engagement of UK Active Employees. Healthcare 2022, 10, 1226. [Google Scholar] [CrossRef]
- Gómez-Salgado, J.; Domínguez-Salas, S.; Romero-Martín, M.; Romero, A.; Coronado-Vázquez, V.; Ruiz-Frutos, C. Work engagement and psychological distress of health professionals during the COVID-19 pandemic. J. Nurs. Manag. 2021, 29, 1016–1025. [Google Scholar] [CrossRef]
- Nelson, B. US healthcare workers march against racism despite the risks. BMJ 2020, 369, m2460. [Google Scholar] [CrossRef]
- Morin, K.H.; Baptiste, D. Nurses as heroes, warriors and political activists. J. Clin. Nurs. 2020, 29, 2733. [Google Scholar] [CrossRef] [PubMed]
- Coombs, C.K.; Newman, R.J.; Cebula, R.J.; White, M.L. The bargaining power of health care unions and union wage premiums for registered nurses. J. Labor Res. 2015, 36, 442–461. [Google Scholar] [CrossRef]
- Wichterich, C. Protection and protest by “voluntary” community health workers: COVID-19 authoritarianism in India. Hist. Sozialforschung 2021, 46, 163–188. [Google Scholar]
- Green, D. Voices from the Pandemic Frontlines: Health Worker Protests and Proposals from 84 Countries. 2020. Available online: https://oxfamapps.org/fp2p/voices-from-the-pandemic-frontlines-health-worker-protests-and-proposals-from-84-countries/ (accessed on 7 March 2022).
- Raleigh, C.; Linke, A.; Hegre, H.; Karlsen, J. Introducing ACLED: An armed conflict location and event dataset. J. Peace Res. 2010, 47, 651–660. [Google Scholar] [CrossRef]
- Raleigh, C. Armed Conflict Location & Event Data Project (ACLED): Codebook; University of Sussex: Brighton, UK, 2021. [Google Scholar]
- Tilly, C.; Tarrow, S. Contentious Politics; Oxford University Press: Oxford, UK, 2006. [Google Scholar]
- Bloem, J.R.; Salemi, C. COVID-19 and conflict. World Dev. 2020, 140, 105294. [Google Scholar] [CrossRef] [PubMed]
- Ide, T. COVID-19 and armed conflict. World Dev. 2021, 140, 105355. [Google Scholar] [CrossRef] [PubMed]
- UNDP. Human Development Index (HDI). 2020. Available online: http://hdr.undp.org/en/content/human-development-index-hdi (accessed on 10 May 2021).
- World Bank. World Bank Open Data. 2024. Available online: https://data.worldbank.org/ (accessed on 10 January 2024).
- Marshall, M.G.; Jaggers, K.; Gurr, T.R. Polity V Annual Time-Series, 1800–2019. 2021. Available online: http://www.systemicpeace.org/inscrdata.html (accessed on 24 September 2021).
- Amiel, S. Resist, Resign and Playing for Time: French Health Workers Bid to Avoid Compulsory COVID Vaccination. 2021. Available online: https://www.euronews.com/my-europe/2021/08/11/resist-resign-and-play-for-time-french-health-workers-bid-to-avoid-compulsory-covid-vaccin (accessed on 23 May 2024).
- Böhmelt, T.; Bernauer, T.; Buhaug, H.; Gleditsch, N.P.; Tribaldos, T.; Wischnath, G. Demand, supply, and restraint: Determinants of domestic water conflict and cooperation. Glob. Environ. Change 2014, 29, 337–348. [Google Scholar] [CrossRef]
- Benítez, M.A.; Velasco, C.; Sequeira, A.R.; Henríquez, J.; Menezes, F.M.; Paolucci, F. Responses to COVID-19 in five Latin American countries. Health Policy Technol. 2020, 9, 525–559. [Google Scholar] [CrossRef]
- Kipfer, S. What colour is your vest? Reflections on the yellow vest movement in France. Stud. Political Econ. 2019, 100, 209–231. [Google Scholar] [CrossRef]
- Daou, M. Tunisia and Morocco Quietly ‘uneasy’ with Algeria’s Popular Movement. 2019. Available online: https://www.france24.com/en/20190314-anxious-silence-tunisia-morocco-algeria-political-crisis-bouteflika-protests (accessed on 11 March 2022).
- Navin, M.C.; Attwell, K. America’s New Vaccine Wars: California and the Politics of Mandates; Cambridge University Press: Cambridge, UK, 2023. [Google Scholar]
- Polo, S.M.T. A pandemic of violence? The impact of COVID-19 on conflict. Peace Econ. Peace Sci. Public Policy 2020, 26, 1–13. [Google Scholar] [CrossRef]
- Al Mutair, A.; Al Bazroun, M.I.; Almusalami, E.M.; Aljarameez, F.; Alhasawi, A.I.; Alahmed, F.; Saha, C.; Alharbi, H.F.; Ahmed, G.Y. Quality of nursing work life among nurses in Saudi Arabia: A descriptive cross-sectional study. Nurs. Rep. 2022, 12, 1014–1022. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Reasons for Protest | Example |
|---|---|
| Protests for workplace safety (e.g., insufficient equipment, lack of personnel, improper training) | “On 31 August 2021, members of KCTU Incheon and Incheon Regional Solidarity picketed in front of Incheon Metropolitan City Hall. They urged the government to solve the lack of nursing personnel and provide a better working environment for health workers amid the coronavirus outbreak.” |
| Protests related to wider social issues (these are not job-specific, but concern wider health policies, social security, etc.) | “On 7 March 2020, nearly a dozen nurses, activists and community members protested outside the city hall in Baltimore (Maryland) demanding protection for the most vulnerable to the coronavirus disease. They urged the creation of a distribution food plan, the suspension of evictions, the distribution of school lunches to vulnerable children, the aid for homeless people in shelters and assistance for immigrants.” |
| Protests related to working conditions (predominantly related to payment, compensation, job security, and workload) | “On 3 July 2020, in Lima, a group of health workers of the Arzobispo Loayza National Hospital protested complaining they had not received the coronavirus bonus announced by the Government, as well as the payment for the additional hours they performed.” |
| Protests indicating denial of treatment (health workers refuse to treat COVID patients due to infection risks) | “On 16 April 2020, health workers in the regional hospital of Medenine protested to prevent the transfer of a patient from Djerba allegedly infected with coronavirus.” |
| Protests against decision-makers (directly criticising them, demanding them to take action, or calling for their removal from office) | “On 31 July 2020, in Tonala, Chiapas, health workers demonstrated to demand the release of a doctor arrested for alleged abuse of power and to demand the dismissal of the Chiapas Secretary of Health.” |
| Protests against violence in the health sector (voicing grievances about physical or verbal attacks against health workers) | “On 13 June 2020, health workers held a protest sit-in in Annaba, denouncing the aggression on one of their colleagues by a patient infected with coronavirus.” |
| Protest against vaccinations (opposing vaccination mandates and similar policies) | “On 17 July 2021, between 1000 and 1200 people, including yellow vest demonstrators and health workers, protested in Nancy against coronavirus-related measures such as a mandatory ‘health pass’ to access French cultural venues as well as compulsory vaccination for all health workers.” |
| Protests demanding vaccinations (health workers asking for access to vaccinations) | “On 21 May 2021, in the Palavecino municipality, Lara state, health workers staged a protest to demand the effective provision of the coronavirus vaccine.” |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jacobi, D.; Ide, T. Nurses’ Protests during the COVID-19 Pandemic: A Comparative International Analysis. Nurs. Rep. 2024, 14, 1961-1972. https://doi.org/10.3390/nursrep14030146
Jacobi D, Ide T. Nurses’ Protests during the COVID-19 Pandemic: A Comparative International Analysis. Nursing Reports. 2024; 14(3):1961-1972. https://doi.org/10.3390/nursrep14030146
Chicago/Turabian StyleJacobi, Davina, and Tobias Ide. 2024. "Nurses’ Protests during the COVID-19 Pandemic: A Comparative International Analysis" Nursing Reports 14, no. 3: 1961-1972. https://doi.org/10.3390/nursrep14030146
APA StyleJacobi, D., & Ide, T. (2024). Nurses’ Protests during the COVID-19 Pandemic: A Comparative International Analysis. Nursing Reports, 14(3), 1961-1972. https://doi.org/10.3390/nursrep14030146