
Lifestyle Clusters of Diet Quality, Sleep, and Screen Time and Associations with Weight Status in Children from Madrid City: ENPIMAD Study

 ,
,  , , ,
, , ,  ,
,  , ,
, ,  , and
, and
Abstract
1. Introduction
2. Materials and Methods
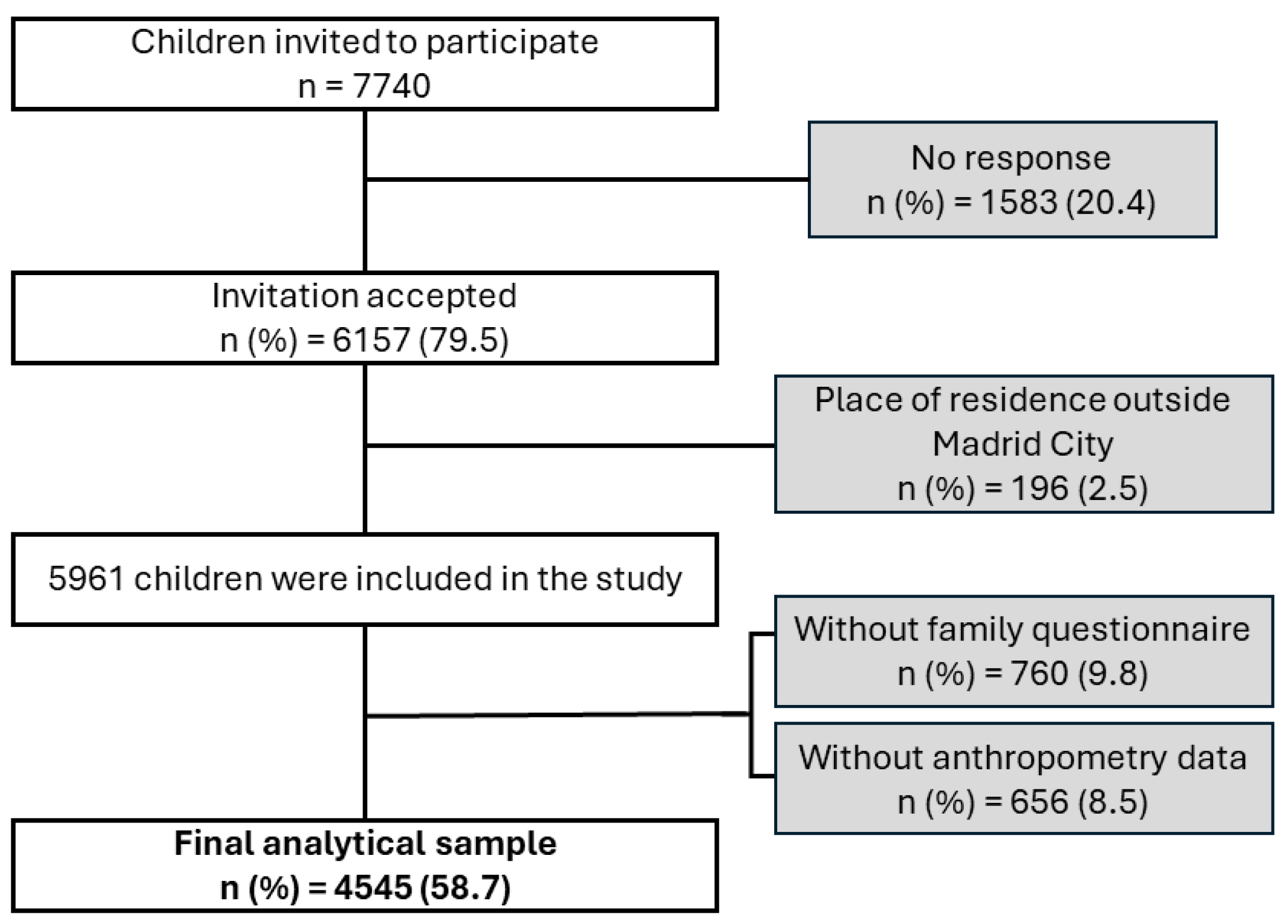
2.1. Study Design and Sample
2.2. Measures
2.2.1. Lifestyle Behaviors: Diet, Sleep, and Screen Time
2.2.2. Socio-Economic Variables
2.2.3. Anthropometric Data
2.3. Statistical Analysis
3. Results
3.1. Sample Characteristics by Sex
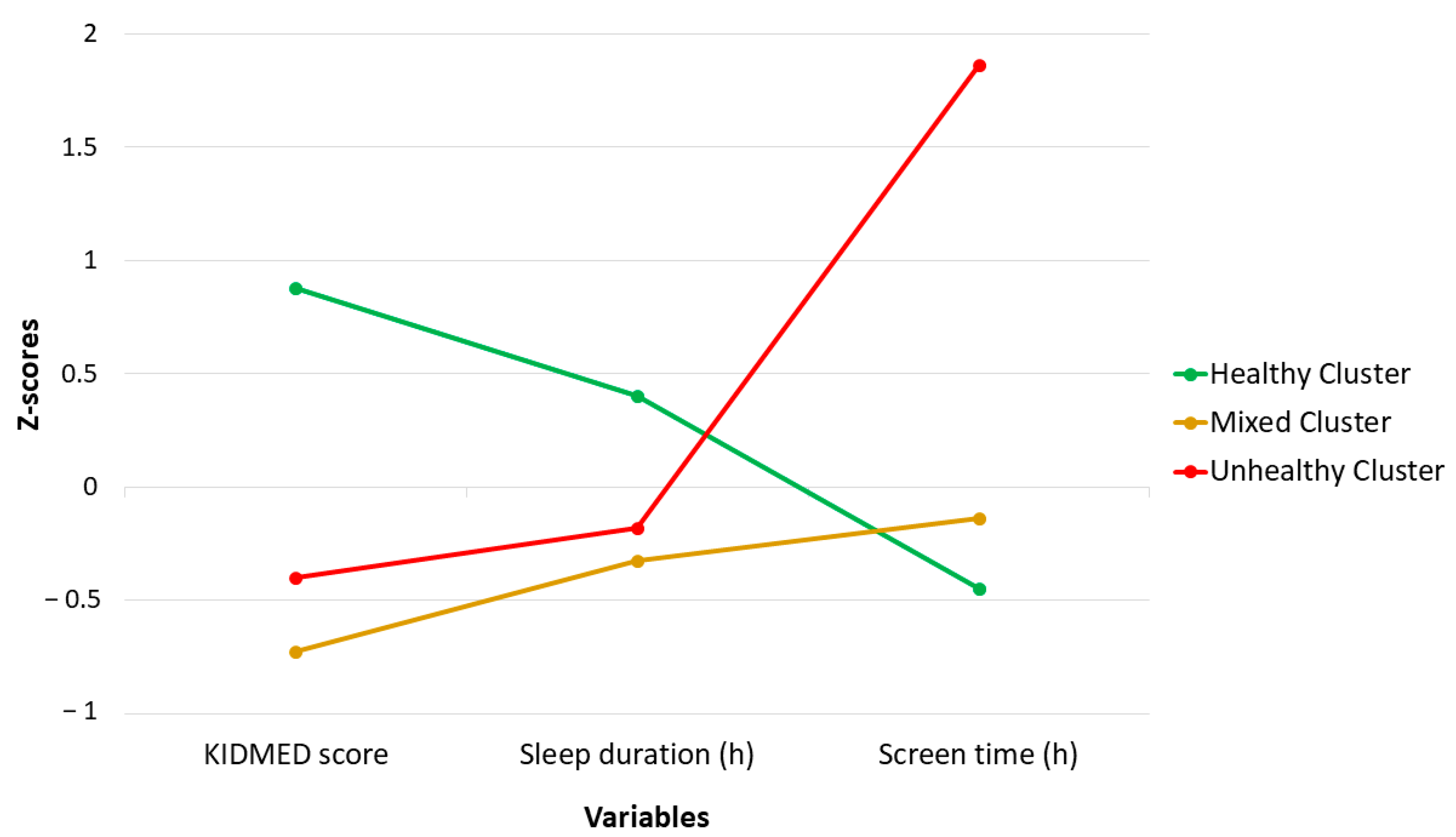
3.2. Characteristics of Lifestyle Clusters
3.3. Socio-Economic Factors Associated with Cluster Membership
3.4. Likelihood of Overweight and Obesity Depending on Cluster Membership
4. Discussion
Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Smith, J.D.; Fu, E.; Kobayashi, M.A. Prevention and Management of Childhood Obesity and Its Psychological and Health Comorbidities. Annu. Rev. Clin. Psychol. 2020, 16, 351–378. [Google Scholar] [CrossRef] [PubMed]
- Morales Camacho, W.J.; Molina Díaz, J.M.; Plata Ortiz, S.; Plata Ortiz, J.E.; Morales Camacho, M.A.; Calderón, B.P. Childhood Obesity: Aetiology, Comorbidities, and Treatment. Diabetes Metab. Res. Rev. 2019, 35, e3203. [Google Scholar] [CrossRef] [PubMed]
- Yan, Y.; Liu, J.; Zhao, X.; Cheng, H.; Huang, G.; Mi, J. Abdominal Visceral and Subcutaneous Adipose Tissues in Association with Cardiometabolic Risk in Children and Adolescents: The China Child and Adolescent Cardiovascular Health (CCACH) Study. BMJ Open Diabetes Res. Care 2019, 7, e000824. [Google Scholar] [CrossRef] [PubMed]
- Viitasalo, A.; Schnurr, T.M.; Pitkänen, N.; Hollensted, M.; Nielsen, T.R.H.; Pahkala, K.; Atalay, M.; Lind, M.V.; Heikkinen, S.; Frithioff-Bøjsøe, C.; et al. Abdominal Adiposity and Cardiometabolic Risk Factors in Children and Adolescents: A Mendelian Randomization Analysis. Am. J. Clin. Nutr. 2019, 110, 1079–1087. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization (WHO). Obesity and Overweight. Available online: https://www.who.int/news-room/fact-sheets/detail/obesity-and-overweight (accessed on 21 June 2023).
- Bravo-Saquicela, D.M.; Sabag, A.; Rezende, L.F.M.; Rey-Lopez, J.P. Has the Prevalence of Childhood Obesity in Spain Plateaued? A Systematic Review and Meta-Analysis. Int. J. Environ. Res. Public Health 2022, 19, 5240. [Google Scholar] [CrossRef] [PubMed]
- Bertomeu-Gonzalez, V.; Sanchez-Ferrer, F.; Quesada, J.A.; Nso-Roca, A.P.; Lopez-Pineda, A.; Ruiz-Nodar, J.M. Prevalence of Childhood Obesity in Spain and Its Relation with Socioeconomic Status and Health Behaviors: Population-Based Cross-Sectional Study. Med. Clin. 2024. [Google Scholar] [CrossRef]
- Gutiérrez-González, E.; García-Solano, M.; Pastor-Barriuso, R.; Fernández de Larrea-Baz, N.; Rollán-Gordo, A.; Peñalver-Argüeso, B.; Peña-Rey, I.; Pollán, M.; Pérez-Gómez, B. A Nation-wide Analysis of Socioeconomic and Geographical Disparities in the Prevalence of Obesity and Excess Weight in Children and Adolescents in Spain: Results from the ENE-COVID Study. Pediatr. Obes. 2024, 19, e13085. [Google Scholar] [CrossRef]
- Poorolajal, J.; Sahraei, F.; Mohamdadi, Y.; Doosti-Irani, A.; Moradi, L. Behavioral Factors Influencing Childhood Obesity: A Systematic Review and Meta-Analysis. Obes. Res. Clin. Pract. 2020, 14, 109–118. [Google Scholar] [CrossRef]
- Liberali, R.; Del Castanhel, F.; Kupek, E.; Assis, M.A.A.D. Latent Class Analysis of Lifestyle Risk Factors and Association with Overweight and/or Obesity in Children and Adolescents: Systematic Review. Child. Obes. 2021, 17, 2–15. [Google Scholar] [CrossRef]
- Alosaimi, N.; Sherar, L.B.; Griffiths, P.; Pearson, N. Clustering of Diet, Physical Activity and Sedentary Behaviour and Related Physical and Mental Health Outcomes: A Systematic Review. BMC Public Health 2023, 23, 1572. [Google Scholar] [CrossRef]
- Seo, S.H.; Shim, Y.S. Association of Sleep Duration with Obesity and Cardiometabolic Risk Factors in Children and Adolescents: A Population-Based Study. Sci. Rep. 2019, 9, 9463. [Google Scholar] [CrossRef] [PubMed]
- Han, S.-H.; Yee, J.-Y.; Pyo, J.-S. Impact of Short Sleep Duration on the Incidence of Obesity and Overweight among Children and Adolescents. Medicina 2022, 58, 1037. [Google Scholar] [CrossRef] [PubMed]
- Nugent, R.; Althouse, A.; Yaqub, Y.; Nugent, K.; Raj, R. Modeling the Relation between Obesity and Sleep Parameters in Children Referred for Dietary Weight Reduction Intervention. South. Med. J. 2014, 107, 473–480. [Google Scholar] [CrossRef] [PubMed]
- D’Souza, N.J.; Kuswara, K.; Zheng, M.; Leech, R.; Downing, K.L.; Lioret, S.; Campbell, K.J.; Hesketh, K.D. A Systematic Review of Lifestyle Patterns and Their Association with Adiposity in Children Aged 5–12 Years. Obes. Rev. 2020, 21, e13029. [Google Scholar] [CrossRef] [PubMed]
- Parker, K.E.; Salmon, J.; Costigan, S.A.; Villanueva, K.; Brown, H.L.; Timperio, A. Activity-Related Behavior Typologies in Youth: A Systematic Review. Int. J. Behav. Nutr. Phys. Act. 2019, 16, 44. [Google Scholar] [CrossRef] [PubMed]
- Lee, A.M.; Scharf, R.J.; Filipp, S.L.; Gurka, M.J.; DeBoer, M.D. Food Insecurity Is Associated with Prediabetes Risk among U.S. Adolescents, NHANES 2003–2014. Metab. Syndr. Relat. Disord. 2019, 17, 347–354. [Google Scholar] [CrossRef] [PubMed]
- Au, L.E.; Zhu, S.M.; Nhan, L.A.; Plank, K.R.; Frongillo, E.A.; Laraia, B.A.; Gurzo, K.; Ritchie, L.D. Household Food Insecurity Is Associated with Higher Adiposity among US Schoolchildren Ages 10–15 Years: The Healthy Communities Study. J. Nutr. 2019, 149, 1642–1650. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.; Kubik, M.Y.; Fulkerson, J.A. Diet Quality and Fruit, Vegetable, and Sugar-Sweetened Beverage Consumption by Household Food Insecurity among 8- to 12-Year-Old Children during Summer Months. J. Acad. Nutr. Diet. 2019, 119, 1695–1702. [Google Scholar] [CrossRef]
- Na, M.; Eagleton, S.G.; Jomaa, L.; Lawton, K.; Savage, J.S. Food Insecurity Is Associated with Suboptimal Sleep Quality, but Not Sleep Duration, among Low-Income Head Start Children of Pre-School Age. Public Health Nutr. 2020, 23, 701–710. [Google Scholar] [CrossRef]
- Serra-Majem, L.; García-Closas, R.; Ribas, L.; Pérez-Rodrigo, C.; Aranceta, J. Food Patterns of Spanish Schoolchildren and Adolescents: The EnKid Study. Public Health Nutr. 2001, 4, 1433–1438. [Google Scholar] [CrossRef]
- Coates, J.; Swindale, A.; Bilinsky, P. Household Food Insecurity Access Scale (HFIAS) for Measurement of Food Access: Indicator Guide: Version 3; USAID: Washington, DC, USA, 2007. [Google Scholar]
- Torsheim, T.; Cavallo, F.; Levin, K.A.; Schnohr, C.; Mazur, J.; Niclasen, B.; Currie, C. Psychometric Validation of the Revised Family Affluence Scale: A Latent Variable Approach. Child Indic. Res. 2016, 9, 771–784. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization (WHO). Expert Committee Physical Status: The Use and Interpretation of Anthropometry; World Health Organization (WHO): Geneva, Switzerland, 1995. [Google Scholar]
- World Health Organization. BMI-for-Age (5–19 Years). Available online: https://www.who.int/tools/growth-reference-data-for-5to19-years/indicators/bmi-for-age (accessed on 7 May 2024).
- World Health Organization. Body Mass Index-for-Age (BMI-for-Age). Available online: https://www.who.int/toolkits/child-growth-standards/standards/body-mass-index-for-age-bmi-for-age (accessed on 7 May 2024).
- Nagy, P.; Intemann, T.; Buck, C.; Pigeot, I.; Ahrens, W.; Molnar, D. Erratum: Percentile Reference Values for Anthropometric Body Composition Indices in European Children from the IDEFICS Study. Int. J. Obes. 2016, 40, 1604–1605. [Google Scholar] [CrossRef] [PubMed]
- Browning, L.M.; Hsieh, S.D.; Ashwell, M. A Systematic Review of Waist-to-Height Ratio as a Screening Tool for the Prediction of Cardiovascular Disease and Diabetes: 0·5 Could Be a Suitable Global Boundary Value. Nutr. Res. Rev. 2010, 23, 247–269. [Google Scholar] [CrossRef] [PubMed]
- Zapico, A.G.; Aparicio-Ugarriza, R.; Quesada-González, C.; Gómez, S.F.; Wärnberg, J.; Medrano, M.; Gusi, N.; Aznar, S.; Marín-Cascales, E.; González-Valeiro, M.A.; et al. Lifestyle Behaviors Clusters in a Nationwide Sample of Spanish Children and Adolescents: PASOS Study. Pediatr. Res. 2023, 94, 2077–2084. [Google Scholar] [CrossRef] [PubMed]
- Gebremariam, M.K.; Totland, T.H.; Andersen, L.F.; Bergh, I.H.; Bjelland, M.; Grydeland, M.; Ommundsen, Y.; Lien, N. Stability and Change in Screen-Based Sedentary Behaviours and Associated Factors among Norwegian Children in the Transition between Childhood and Adolescence. BMC Public Health 2012, 12, 104. [Google Scholar] [CrossRef]
- Janssen, X.; Mann, K.D.; Basterfield, L.; Parkinson, K.N.; Pearce, M.S.; Reilly, J.K.; Adamson, A.J.; Reilly, J.J. Development of Sedentary Behavior across Childhood and Adolescence: Longitudinal Analysis of the Gateshead Millennium Study. Int. J. Behav. Nutr. Phys. Act. 2016, 13, 88. [Google Scholar] [CrossRef] [PubMed]
- Pearson, N.; Haycraft, E.; Johnston, J.P.; Atkin, A.J. Sedentary Behaviour across the Primary-Secondary School Transition: A Systematic Review. Prev. Med. 2017, 94, 40–47. [Google Scholar] [CrossRef] [PubMed]
- Gebremariam, M.K.; Bergh, I.H.; Andersen, L.F.; Ommundsen, Y.; Totland, T.H.; Bjelland, M.; Grydeland, M.; Lien, N. Are Screen-Based Sedentary Behaviors Longitudinally Associated with Dietary Behaviors and Leisure-Time Physical Activity in the Transition into Adolescence? Int. J. Behav. Nutr. Phys. Act. 2013, 10, 9. [Google Scholar] [CrossRef] [PubMed]
- Shqair, A.Q.; Pauli, L.A.; Costa, V.P.P.; Cenci, M.; Goettems, M.L. Screen Time, Dietary Patterns and Intake of Potentially Cariogenic Food in Children: A Systematic Review. J. Dent. 2019, 86, 17–26. [Google Scholar] [CrossRef]
- Rubín, L.; Gába, A.; Pelclová, J.; Štefelová, N.; Jakubec, L.; Dygrýn, J.; Hron, K. Changes in Sedentary Behavior Patterns during the Transition from Childhood to Adolescence and Their Association with Adiposity: A Prospective Study Based on Compositional Data Analysis. Arch. Public Health 2022, 80, 1. [Google Scholar] [CrossRef]
- Neufeld, L.M.; Andrade, E.B.; Ballonoff Suleiman, A.; Barker, M.; Beal, T.; Blum, L.S.; Demmler, K.M.; Dogra, S.; Hardy-Johnson, P.; Lahiri, A.; et al. Food Choice in Transition: Adolescent Autonomy, Agency, and the Food Environment. Lancet 2022, 399, 185–197. [Google Scholar] [CrossRef] [PubMed]
- Kemp, B.J.; Parrish, A.-M.; Cliff, D.P. ‘Social Screens’ and ‘the Mainstream’: Longitudinal Competitors of Non-Organized Physical Activity in the Transition from Childhood to Adolescence. Int. J. Behav. Nutr. Phys. Act. 2020, 17, 5. [Google Scholar] [CrossRef] [PubMed]
- Pérez-Rodrigo, C.; Gil, Á.; González-Gross, M.; Ortega, R.; Serra-Majem, L.; Varela-Moreiras, G.; Aranceta-Bartrina, J. Clustering of Dietary Patterns, Lifestyles, and Overweight among Spanish Children and Adolescents in the ANIBES Study. Nutrients 2015, 8, 11. [Google Scholar] [CrossRef] [PubMed]
- de Mello, G.T.; Minatto, G.; Costa, R.M.; Leech, R.M.; Cao, Y.; Lee, R.E.; Silva, K.S. Clusters of 24-Hour Movement Behavior and Diet and Their Relationship with Health Indicators among Youth: A Systematic Review. BMC Public Health 2024, 24, 1080. [Google Scholar] [CrossRef] [PubMed]
- Kivimäki, M.; Vahtera, J.; Tabák, A.G.; Halonen, J.I.; Vineis, P.; Pentti, J.; Pahkala, K.; Rovio, S.; Viikari, J.; Kähönen, M.; et al. Neighbourhood Socioeconomic Disadvantage, Risk Factors, and Diabetes from Childhood to Middle Age in the Young Finns Study: A Cohort Study. Lancet Public Health 2018, 3, e365–e373. [Google Scholar] [CrossRef]
- Sanders, T.; Feng, X.; Fahey, P.P.; Lonsdale, C.; Astell-Burt, T. The Influence of Neighbourhood Green Space on Children’s Physical Activity and Screen Time: Findings from the Longitudinal Study of Australian Children. Int. J. Behav. Nutr. Phys. Act. 2015, 12, 126. [Google Scholar] [CrossRef] [PubMed]
- Seabra, A.; Mendonça, D.; Maia, J.; Welk, G.; Brustad, R.; Fonseca, A.M.; Seabra, A.F. Gender, Weight Status and Socioeconomic Differences in Psychosocial Correlates of Physical Activity in Schoolchildren. J. Sci. Med. Sport 2013, 16, 320–326. [Google Scholar] [CrossRef] [PubMed]
- Kral, T.V.E.; Chittams, J.; Moore, R.H. Relationship between Food Insecurity, Child Weight Status, and Parent-reported Child Eating and Snacking Behaviors. J. Spec. Pediatr. Nurs. 2017, 22, e12177. [Google Scholar] [CrossRef] [PubMed]
- Ortiz-Marrón, H.; Ortiz-Pinto, M.A.; Urtasun Lanza, M.; Cabañas Pujadas, G.; Valero Del Pino, V.; Belmonte Cortés, S.; Gómez Gascón, T.; Ordobás Gavín, M. Household Food Insecurity and Its Association with Overweight and Obesity in Children Aged 2 to 14 Years. BMC Public Health 2022, 22, 1930. [Google Scholar] [CrossRef]
- Yannakoulia, M.; Lykou, A.; Kastorini, C.M.; Saranti Papasaranti, E.; Petralias, A.; Veloudaki, A.; Linos, A. Socio-Economic and Lifestyle Parameters Associated with Diet Quality of Children and Adolescents Using Classification and Regression Tree Analysis: The DIATROFI Study. Public Health Nutr. 2016, 19, 339–347. [Google Scholar] [CrossRef]
- Borraccino, A.; Lemma, P.; Iannotti, R.J.; Zambon, A.; Dalmasso, P.; Lazzeri, G.; Giacchi, M.; Cavallo, F. Socioeconomic Effects on Meeting Physical Activity Guidelines. Med. Sci. Sports Exerc. 2009, 41, 749–756. [Google Scholar] [CrossRef] [PubMed]
- Yang-Huang, J.; van Grieken, A.; Wang, L.; Jansen, W.; Raat, H. Clustering of Sedentary Behaviours, Physical Activity, and Energy-Dense Food Intake in Six-Year-Old Children: Associations with Family Socioeconomic Status. Nutrients 2020, 12, 1722. [Google Scholar] [CrossRef] [PubMed]
- Leech, R.M.; McNaughton, S.A.; Timperio, A. Clustering of Children’s Obesity-Related Behaviours: Associations with Sociodemographic Indicators. Eur. J. Clin. Nutr. 2014, 68, 623–628. [Google Scholar] [CrossRef] [PubMed]
- Schröder, H.; Bawaked, R.A.; Ribas-Barba, L.; Izquierdo-Pulido, M.; Roman-Viñas, B.; Fíto, M.; Serra-Majem, L. Cumulative Effect of Obesogenic Behaviours on Adiposity in Spanish Children and Adolescents. Obes. Facts 2017, 10, 584–596. [Google Scholar] [CrossRef] [PubMed]
- Sánchez-Oliva, D.; Grao-Cruces, A.; Carbonell-Baeza, A.; Cabanas-Sánchez, V.; Veiga, O.L.; Castro-Piñero, J. Lifestyle Clusters in School-Aged Youth and Longitudinal Associations with Fatness: The UP&DOWN Study. J. Pediatr. 2018, 203, 317–324.e1. [Google Scholar] [CrossRef] [PubMed]
- Miguel-Berges, M.L.; Mouratidou, T.; Santaliestra-Pasias, A.; Androutsos, O.; Iotova, V.; Galcheva, S.; De Craemer, M.; Cardon, G.; Koletzko, B.; Kulaga, Z.; et al. Longitudinal Associations between Diet Quality, Sedentary Behaviours and Physical Activity and Risk of Overweight and Obesity in Preschool Children: The ToyBox-study. Pediatr. Obes. 2023, 18, e13068. [Google Scholar] [CrossRef] [PubMed]
- Bae, J.-H.; Choi, J.-H. Gender Disparities in Childhood Obesity and Household Food Insecurity. Nutrition 2021, 87–88, 111190. [Google Scholar] [CrossRef] [PubMed]
- Reilly, J.J. Physical Activity, Sedentary Behaviour and Energy Balance in the Preschool Child: Opportunities for Early Obesity Prevention. Proc. Nutr. Soc. 2008, 67, 317–325. [Google Scholar] [CrossRef] [PubMed]
- Wang, X.; Cheng, Z. Cross-Sectional Studies. Chest 2020, 158, S65–S71. [Google Scholar] [CrossRef]
- Quinlan, C.; Rattray, B.; Pryor, D.; Northey, J.M.; Anstey, K.J.; Butterworth, P.; Cherbuin, N. The Accuracy of Self-Reported Physical Activity Questionnaires Varies with Sex and Body Mass Index. PLoS ONE 2021, 16, e0256008. [Google Scholar] [CrossRef]
- Ravelli, M.N.; Schoeller, D.A. Traditional Self-Reported Dietary Instruments Are Prone to Inaccuracies and New Approaches Are Needed. Front. Nutr. 2020, 7, 90. [Google Scholar] [CrossRef] [PubMed]
- Svedberg, P.; Nygren, J.M.; Staland-Nyman, C.; Nyholm, M. The Validity of Socioeconomic Status Measures among Adolescents Based on Self-Reported Information about Parents Occupations, FAS and Perceived SES; Implication for Health Related Quality of Life Studies. BMC Med. Res. Methodol. 2016, 16, 48. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
| Total | Boys | Girls | p | ||
|---|---|---|---|---|---|
| n | n (%) | 4545 | 2331 (51.3) | 2214 (48.7) | |
| Age (years) | median (IQR) | 7.0 (5.0–10.0) | 7.0 (5.0–10.0) | 7.0 (5.0–10.0) | 0.718 |
| School district | 0.876 | ||||
| Low | n (%) | 1203 (26.5) | 619 (26.5) | 584 (26.4) | |
| Mid-low | n (%) | 1562 (34.4) | 793 (34.0) | 769 (34.8) | |
| Mid-high | n (%) | 1090 (24.0) | 571 (24.5) | 519 (23.4) | |
| High | n (%) | 690 (15.2) | 349 (15.0) | 342 (15.4) | |
| Food insecurity ¥ | 0.076 | ||||
| With food insecurity | n (%) | 812 (18.1) | 414 (17.9) | 398 (18.2) | |
| Without food insecurity | n (%) | 3683 (81.9) | 1897 (82.1) | 1785 (81.8) | |
| Socio-economic status ¥ | 0.922 | ||||
| Low class | n (%) | 2085 (45.9) | 1062 (45.6) | 1023 (46.2) | |
| Mid class | n (%) | 1852 (40.8) | 952 (40.8) | 901 (40.7) | |
| High class | n (%) | 568 (12.5) | 296 (12.7) | 272 (12.3) | |
| Undetermined | n (%) | 40 (0.9) | 22 (0.9) | 18 (0.8) | |
| Weight status | <0.001 | ||||
| Underweight | n (%) | 44 (1.0) | 24 (1.0) | 19 (0.9) | |
| Normal weight | n (%) | 2636 (58.1) | 1277 (54.8) | 1359 (61.5) | |
| Overweight | n (%) | 1150 (25.3) | 588 (25.3) | 561 (25.4) | |
| Obesity | n (%) | 710 (15.6) | 439 (18.9) | 271 (12.3) | |
| Abdominal obesity | n (%) | 1411 (31.1) | 724 (31.2) | 687 (31.1) | 0.962 |
| Adherence to MD | 0.005 | ||||
| Low adherence | n (%) | 385 (8.5) | 225 (9.6) | 161 (7.3) | |
| Medium adherence | n (%) | 3199 (70.4) | 1640 (70.4) | 1559 (70.4) | |
| High adherence | n (%) | 960 (21.1) | 466 (20.0) | 494 (22.3) | |
| Sleep duration (h/day) | median (IQR) | 9.8 (9.5–10.5) | 9.8 (9.5–10.5) | 9.8 (9.5–10.5) | 0.777 |
| Screen time (h/day) | median (IQR) | 2.1 (1.4–3.1) | 2.3 (1.6–3.3) | 2.0 (1.3–2.9) | <0.001 |
| Healthy Cluster (HC) | Mixed Cluster (MC) | Unhealthy Cluster (UC) | p | ||
|---|---|---|---|---|---|
| Sex | <0.001 | ||||
| Boys | n (%) | 952 (49.6) | 996 (51.3) | 383 (56.1) | |
| Girls | n (%) | 967 (50.4) | 948 (48.7) | 300 (43.9) | |
| Age (years) | Median (IQR) | 7.0 (5.0–9.0) a | 7.0 (5.0–10.0) b | 8.0 (6.0–10.0) c | <0.001 |
| School district | <0.001 | ||||
| Low | n (%) | 412 (21.5) | 555 (28.6) | 236 (34.5) | |
| Mid-low | n (%) | 623 (32.5) | 646 (33.2) | 293 (43.0) | |
| Mid-high | n (%) | 546 (28.5) | 454 (23.3) | 90 (13.2) | |
| High | n (%) | 337 (17.6) | 289 (14.9) | 64 (9.3) | |
| Food insecurity ¥ | <0.001 | ||||
| With food insecurity | n (%) | 229 (12.0) | 373 (19.5) | 210 (31.3) | |
| Without food insecurity | n (%) | 1677 (88.0) | 1545 (80.5) | 461 (68.7) | |
| Socio-economic status ¥ | <0.001 | ||||
| Low class | n (%) | 656 (34.2) | 963 (49.5) | 466 (68.2) | |
| Mid class | n (%) | 908 (47.3) | 771 (39.6) | 174 (25.5) | |
| High class | n (%) | 341 (17.8) | 193 (10.0) | 34 (4.9) | |
| Undetermined | n (%) | 14 (0.7) | 17 (0.9) | 9 (1.3) | |
| Weight status | <0.001 | ||||
| Underweight | n (%) | 16 (0.8) | 14 (0.7) | 14 (2.1) | |
| Normal weight | n (%) | 1224 (63.8) | 1086 (55.9) | 327 (48.0) | |
| Overweight | n (%) | 434 (22.7) | 535 (27.6) | 180 (26.5) | |
| Obesity | n (%) | 243 (12.7) | 307 (15.8) | 160 (23.5) | |
| Abdominal obesity | n (%) | 542 (28.3) | 603 (31.1) | 266 (39.2) | <0.001 |
| KIDMED score | Median (IQR) | 7.0 (7.0–8.0) a | 5.0 (4.0–5.0) b | 5.0 (4.0–6.0) c | <0.001 |
| Adherence to MD | <0.001 | ||||
| Low adherence | n (%) | 0 (0.0) | 298 (15.3) | 88 (12.8) | |
| Medium adherence | n (%) | 999 (52.0) | 1646 (84.7) | 555 (81.3) | |
| High adherence | n (%) | 920 (48.0) | 0 (0.0) | 40 (5.9) | |
| Sleep duration (h/day) | Median (IQR) | 10.2 (9.8–10.7) a | 9.6 (9.1–10.1) b | 9.5 (8.8–10.8) b | <0.001 |
| Screen time (h/day) | Median (IQR) | 1.6 (1.1–2.3) a | 2.2 (1.6–2.9) b | 4.9 (4.3–5.7) c | <0.001 |
| Boys | Girls | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Mixed Cluster | Unhealthy Cluster | Mixed Cluster | Unhealthy Cluster | |||||||
| OR (95% CI) | p | OR (95% CI) | p | OR (95% CI) | p | OR (95% CI) | p | |||
| Model 1: Unadjusted | School district development | Low | 1.66 (1.25, 2.20) | <0.001 | 4.43 (2.80, 6.99) | <0.001 | 1.50 (1.13, 2.00) | 0.006 | 2.04 (1.33, 3.15) | 0.001 |
| Mid-low | 1.16 (0.89, 1.52) | 0.275 | 3.42 (2.19, 5.32) | <0.001 | 1.26 (0.96, 1.66) | 0.095 | 1.80 (1.19, 2.73) | 0.005 | ||
| Mid-high | 1.01 (0.76, 1.33) | 0.949 | 1.00 (0.60, 1.67) | 0.993 | 0.93 (0.69, 1.24) | 0.605 | 0.77 (0.48, 1.24) | 0.288 | ||
| Food insecurity (HFIAS scale) | With insecurity | 1.63 (1.26, 2.10) | <0.001 | 3.60 (2.70, 4.81) | <0.001 | 1.92 (1.50, 2.47) | <0.001 | 3.03 (2.20, 4.16) | <0.001 | |
| SES (FAS scale) | Low class | 2.26 (1.71, 2.99) | <0.001 | 7.10 (4.32, 11.65) | <0.001 | 3.02 (2.25, 4.06) | <0.001 | 7.30 (4.13, 12.90) | <0.001 | |
| Mid class | 1.29 (0.98, 1.70) | 0.067 | 1.73 (1.03, 2.90) | 0.039 | 1.76 (1.31, 2.37) | <0.001 | 2.22 (1.23, 4.00) | 0.008 | ||
| Model 2: Adjusted | School district development | Low | 1.30 (0.97, 1.75) | 0.092 | 2.65 (1.65, 4.25) | <0.001 | 1.18 (0.87, 1.59) | 0.280 | 1.23 (0.78, 1.94) | 0.366 |
| Mid-low | 0.98 (0.75, 1.30) | 0.910 | 2.33 (1.48, 3.69) | <0.001 | 1.08 (0.81, 1.43) | 0.607 | 1.35 (0.88, 2.08) | 0.172 | ||
| Mid-high | 0.99 (0.75, 1.32) | 0.967 | 0.94 (0.56, 1.59) | 0.827 | 0.92 (0.69, 1.24) | 0.605 | 0.62 (0.37, 1.02) | 0.060 | ||
| Food insecurity (HFIAS scale) | With insecurity | 1.17 (0.88, 1.55) | 0.278 | 1.71 (1.24, 2.35) | <0.001 | 1.41 (1.01, 1.88) | 0.007 | 1.81 (1.29, 2.54) | <0.001 | |
| SES (FAS scale) | Low class | 1.99 (1.47, 2.69) | <0.001 | 3.95 (2.34, 6.68) | <0.001 | 2.57 (1.87, 3.51) | <0.001 | 5.05 (2.80, 9.10) | <0.001 | |
| Mid class | 1.23 (0.93, 1.63) | 0.146 | 1.40 (0.82, 2.36) | 0.214 | 1.68 (1.24, 2.27) | <0.001 | 1.95 (1.07, 3.54) | 0.028 | ||
| Overweight | Obesity | Abdominal Obesity | ||||||
|---|---|---|---|---|---|---|---|---|
| OR (95% CI) | p | OR (95% CI) | p | OR (95% CI) | p | |||
| Boys | Model 1: Unadjusted | Mixed | 1.53 (1.24, 1.90) | <0.001 | 1.50 (1.18, 1.92) | 0.001 | 1.27 (1.04, 1.54) | 0.017 |
| Unhealthy | 1.60 (1.19, 2.14) | 0.002 | 2.42 (1.79,3.27) | <0.001 | 1.93 (1.51, 2.48) | <0.001 | ||
| Model 2: Adjusted | Mixed | 1.40 (1.13, 1.74) | 0.002 | 1.21 (0.94, 1.56) | 0.144 | 1.19 (0.97, 1.45) | 0.092 | |
| Unhealthy | 1.31 (0.97, 1.78) | 0.077 | 1.49 (1.08, 2.05) | 0.016 | 1.65 (1.27, 2.14) | <0.001 | ||
| Model 3: Adjusted | Mixed | 1.45 (1.17, 1.80) | <0.001 | 1.39 (1.08, 1.79) | 0.011 | 1.30 (1.06, 1.58) | 0.011 | |
| Unhealthy | 1.37 (1.01, 1.85) | 0.042 | 1.93 (1.41, 2.64) | <0.001 | 1.93 (1.49, 2.50) | <0.001 | ||
| Model 4: Adjusted | Mixed | 1.40 (1.12, 1.74) | 0.003 | 1.22 (0.94, 1.58) | 0.128 | 1.21 (0.98, 1.48) | 0.069 | |
| Unhealthy | 1.25 (0.92, 1.70) | 0.149 | 1.46 (1.06, 2.02) | 0.021 | 1.67 (1.29, 2.18) | <0.001 | ||
| Girls | Model 1: Unadjusted | Mixed | 1.26 (1.02, 1.56) | 0.033 | 1.32 (0.99, 1.77) | 0.059 | 1.032 (0.85, 1.25) | 0.755 |
| Unhealthy | 1.41 (1.04, 1.92) | 0.027 | 2.24 (1.54, 3.24) | <0.001 | 1.35 (1.03, 1.77) | 0.032 | ||
| Model 2: Adjusted | Mixed | 1.19 (0.96, 1.48) | 0.104 | 1.15 (0.85, 1.54) | 0.362 | 0.95 (0.77, 1.17) | 0.650 | |
| Unhealthy | 1.25 (0.94, 1.75) | 0.122 | 1.71 (1.17, 2.51) | 0.006 | 1.36 (1.01, 1.83) | 0.039 | ||
| Model 3: Adjusted | Mixed | 1.31 (0.95, 1.78) | 0.094 | 1.17 (0.87, 1.58) | 0.300 | 0.99 (0.81, 1.23) | 0.968 | |
| Unhealthy | 1.24 (1.00, 1.54) | 0.049 | 1.66 (1.12, 2.46) | 0.012 | 1.42 (1.06, 1.91) | 0.019 | ||
| Model 4: Adjusted | Mixed | 1.20 (0.97, 1.49) | 0.094 | 1.08 (0.80, 1.47) | 0.602 | 0.94 (0.76, 1.16) | 0.562 | |
| Unhealthy | 1.25 (0.91, 1.71) | 0.173 | 1.47 (0.99, 2.19) | 0.056 | 1.28 (0.95, 1.73) | 0.106 | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Peral-Suárez, Á.; Bermejo, L.M.; Salas-González, M.D.; Cuadrado-Soto, E.; Lozano-Estevan, M.D.C.; Loria-Kohen, V.; González-Rodríguez, L.G.; Aparicio, A.; Díaz-Olalla, J.M.; López-Sobaler, A.M. Lifestyle Clusters of Diet Quality, Sleep, and Screen Time and Associations with Weight Status in Children from Madrid City: ENPIMAD Study. Nutrients 2024, 16, 2096. https://doi.org/10.3390/nu16132096
Peral-Suárez Á, Bermejo LM, Salas-González MD, Cuadrado-Soto E, Lozano-Estevan MDC, Loria-Kohen V, González-Rodríguez LG, Aparicio A, Díaz-Olalla JM, López-Sobaler AM. Lifestyle Clusters of Diet Quality, Sleep, and Screen Time and Associations with Weight Status in Children from Madrid City: ENPIMAD Study. Nutrients. 2024; 16(13):2096. https://doi.org/10.3390/nu16132096
Chicago/Turabian StylePeral-Suárez, África, Laura M. Bermejo, María Dolores Salas-González, Esther Cuadrado-Soto, María Del Carmen Lozano-Estevan, Viviana Loria-Kohen, Liliana G. González-Rodríguez, Aránzazu Aparicio, José Manuel Díaz-Olalla, and Ana M. López-Sobaler. 2024. "Lifestyle Clusters of Diet Quality, Sleep, and Screen Time and Associations with Weight Status in Children from Madrid City: ENPIMAD Study" Nutrients 16, no. 13: 2096. https://doi.org/10.3390/nu16132096
APA StylePeral-Suárez, Á., Bermejo, L. M., Salas-González, M. D., Cuadrado-Soto, E., Lozano-Estevan, M. D. C., Loria-Kohen, V., González-Rodríguez, L. G., Aparicio, A., Díaz-Olalla, J. M., & López-Sobaler, A. M. (2024). Lifestyle Clusters of Diet Quality, Sleep, and Screen Time and Associations with Weight Status in Children from Madrid City: ENPIMAD Study. Nutrients, 16(13), 2096. https://doi.org/10.3390/nu16132096