
Efficacy of a Low-FODMAP Diet for Coeliac Patients with Persistent IBS-like Symptoms despite a Gluten-Free Diet: A Systematic Review

 , , and
, , and
Abstract
1. Introduction
2. Methods
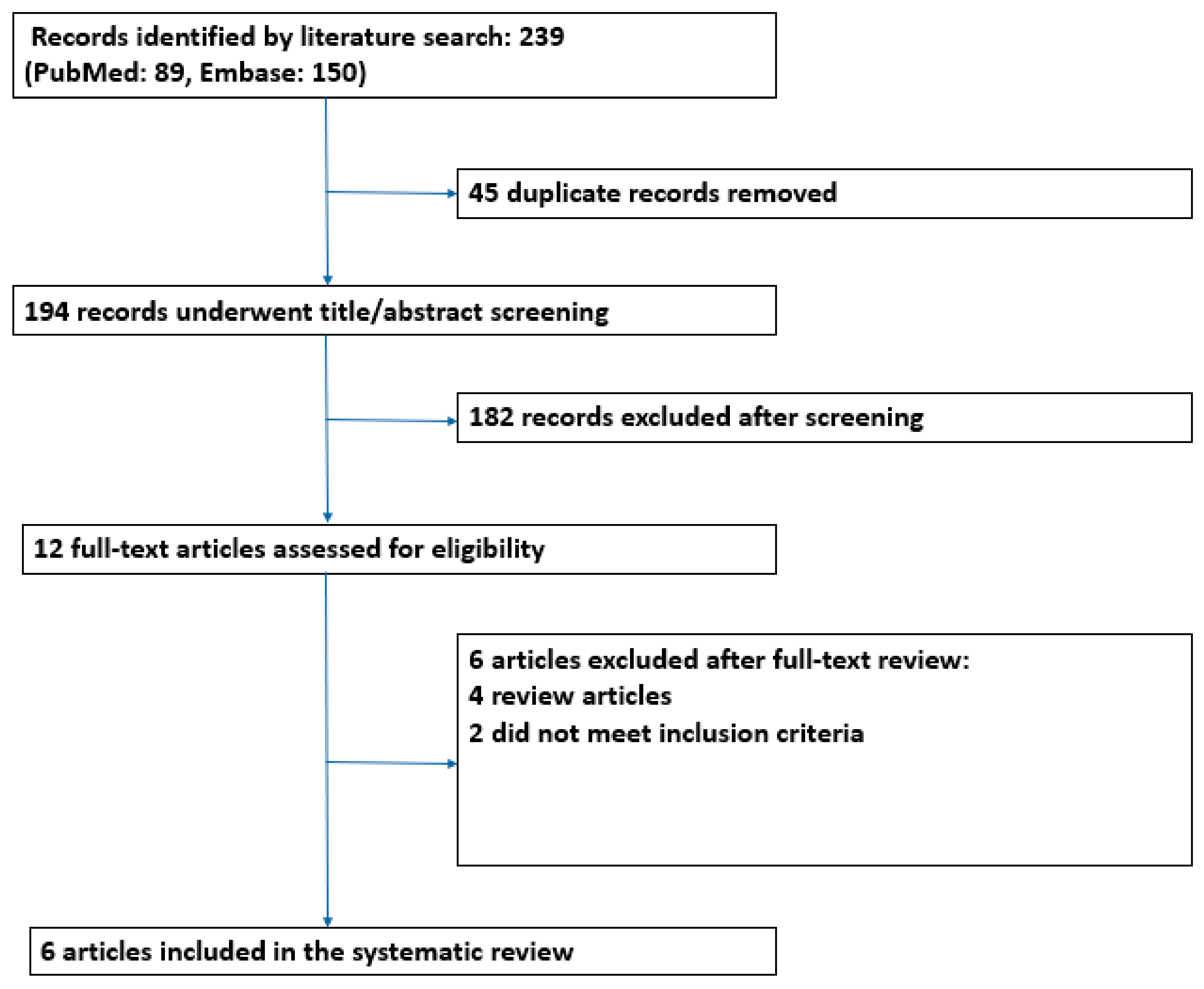
2.1. Literature Search Details
2.2. Eligibility Criteria
2.3. Data Extraction
2.4. Outcomes
2.5. Study Quality and Risk of Bias
3. Results
3.1. Characteristics of Included Studies
3.2. Efficacy of a Low-FODMAP Diet Intervention in Celiac Patients with Persistent Symptoms
3.3. Effect of a Low-FODMAP Diet on Quality of Life and Psychological and General Well-Being
3.4. Relationship of FODMAP Intake with Persistent Symptoms in Coeliac Patients on a Gluten-Free Diet
3.5. Risk of Bias Evaluation
4. Discussion
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Zingone, F.; Maimaris, S.; Auricchio, R.; Caio, G.P.I.; Carroccio, A.; Elli, L.; Galliani, E.; Montagnani, M.; Valiante, F.; Biagi, F. Guidelines of the Italian societies of gastroenterology on the diagnosis and management of coeliac disease and dermatitis herpetiformis. Dig. Liver Dis. 2022, 54, 1304–1319. [Google Scholar] [CrossRef] [PubMed]
- Rubio-Tapia, A.; Hill, I.D.; Semrad, C.; Kelly, C.P.; Greer, K.B.; Limketkai, B.N.; Lebwohl, B. American College of Gastroenterology Guidelines Update: Diagnosis and Management of Celiac Disease. Am. J. Gastroenterol. 2023, 118, 59–76. [Google Scholar] [CrossRef] [PubMed]
- Al-Toma, A.; Volta, U.; Auricchio, R.; Castillejo, G.; Sanders, D.S.; Cellier, C.; Mulder, C.J.; Lundin, K.E.A. European Society for the Study of Coeliac Disease (ESsCD) guideline for coeliac disease and other gluten-related disorders. United Eur. Gastroenterol. J. 2019, 7, 583–613. [Google Scholar] [CrossRef] [PubMed]
- Singh, P.; Arora, A.; Strand, T.A.; Leffler, D.A.; Catassi, C.; Green, P.H.; Kelly, C.P.; Ahuja, V.; Makharia, G.K. Global Prevalence of Celiac Disease: Systematic Review and Meta-analysis. Clin. Gastroenterol. Hepatol. 2018, 16, 823–836. [Google Scholar] [CrossRef] [PubMed]
- Hall, N.J.; Rubin, G.; Charnock, A. Systematic review: Adherence to a gluten-free diet in adult patients with celiac disease. Aliment. Pharmacol. Ther. 2009, 30, 315–330. [Google Scholar] [CrossRef] [PubMed]
- Penny, H.A.; Baggus, E.M.R.; Rej, A.; Snowden, J.A.; Sanders, D.S. Non-Responsive Coeliac Disease: A Comprehensive Review from the NHS England National Centre for Refractory Coeliac Disease. Nutrients 2020, 12, 216. [Google Scholar] [CrossRef] [PubMed]
- Sainsbury, A.; Sanders, D.S.; Ford, A.C. Prevalence of irritable bowel syndrome-type symptoms in patients with celiac disease: A meta-analysis. Clin. Gastroenterol. Hepatol. 2013, 11, 359–365. [Google Scholar] [CrossRef] [PubMed]
- Leffler, D.A.; Dennis, M.; Hyett, B.; Kelly, E.; Schuppan, D.; Kelly, C.P. Etiologies and predictors of diagnosis in nonresponsive celiac disease. Clin. Gastroenterol. Hepatol. 2007, 5, 445–450. [Google Scholar] [CrossRef] [PubMed]
- Stasi, E.; Marafini, I.; Caruso, R.; Soderino, F.; Angelucci, E.; Blanco, G.D.V.; Paoluzi, O.A.; Calabrese, E.; Sedda, S.; Zorzi, F.; et al. Frequency and Cause of Persistent Symptoms in Celiac Disease Patients on a Long-term Gluten-free Diet. J. Clin. Gastroenterol. 2016, 50, 239–243. [Google Scholar] [CrossRef] [PubMed]
- Schiepatti, A.; Maimaris, S.; Lusetti, F.; Scalvini, D.; Minerba, P.; Cincotta, M.; Fazzino, E.; Biagi, F. High Prevalence of Functional Gastrointestinal Disorders in Celiac Patients with Persistent Symptoms on a Gluten-Free Diet: A 20-Year Follow-Up Study. Dig. Dis. Sci. 2023, 68, 3374–3382. [Google Scholar] [CrossRef]
- Parker, S.; Palsson, O.; Sanders, D.S.; Simren, M.; Sperber, A.D.; Törnblom, H.; Urwin, H.; Whitehead, W.; Aziz, I. Functional Gastrointestinal Disorders and Associated Health Impairment in Individuals with Celiac Disease. Clin. Gastroenterol. Hepatol. 2022, 20, 1315–1325. [Google Scholar] [CrossRef] [PubMed]
- Van Megen, F.; Skodje, G.I.; Stendahl, M.; Veierød, M.B.; Lundin, K.E.A.; Henriksen, C. High disease burden in treated celiac patients—A web-based survey. Scand. J. Gastroenterol. 2021, 56, 882–888. [Google Scholar] [CrossRef] [PubMed]
- Zingone, F.; Swift, G.L.; Card, T.R.; Sanders, D.S.; Ludvigsson, J.F.; Bai, J.C. Psychological morbidity of celiac disease: A review of the literature. United Eur. Gastroenterol. J. 2015, 3, 136–145. [Google Scholar] [CrossRef] [PubMed]
- Abdulkarim, A.S.; Burgart, L.J.; See, J.; Murray, J.A. Etiology of nonresponsive celiac disease: Results of a systematic approach. Am. J. Gastroenterol. 2002, 97, 2016–2021. [Google Scholar] [CrossRef] [PubMed]
- Biagi, F.; Marchese, A.; Ferretti, F.; Ciccocioppo, R.; Schiepatti, A.; Volta, U.; Caio, G.; Ciacci, C.; Zingone, F.; D’odorico, A.; et al. A multicentre case control study on complicated coeliac disease: Two different patterns of natural history, two different prognoses. BMC Gastroenterol. 2014, 14, 139. [Google Scholar] [CrossRef] [PubMed]
- Sperber, A.D.; Bangdiwala, S.I.; Drossman, D.A.; Ghoshal, U.C.; Simren, M.; Tack, J.; Whitehead, W.E.; Dumitrascu, D.L.; Fang, X.; Fukudo, S.; et al. Worldwide Prevalence and Burden of Functional Gastrointestinal Disorders, Results of Rome Foundation Global Study. Gastroenterology 2021, 160, 99–114.e3. [Google Scholar] [CrossRef] [PubMed]
- Drossman, D.A.; Hasler, W.L. Rome IV-Functional GI Disorders: Disorders of Gut-Brain Interaction. Gastroenterology 2016, 150, 1257–1261. [Google Scholar] [CrossRef] [PubMed]
- Savarino, E.; Zingone, F.; Barberio, B.; Marasco, G.; Akyuz, F.; Akpinar, H.; Barboi, O.; Bodini, G.; Bor, S.; Chiarioni, G.; et al. Functional bowel disorders with diarrhoea: Clinical guidelines of the United European Gastroenterology and European Society for Neurogastroenterology and Motility. United Eur. Gastroenterol. J. 2022, 10, 556–584. [Google Scholar] [CrossRef] [PubMed]
- Vasant, D.H.; Paine, P.A.; Black, C.J.; Houghton, L.A.; Everitt, H.A.; Corsetti, M.; Agrawal, A.; Aziz, I.; Farmer, A.D.; Eugenicos, M.P.; et al. British Society of Gastroenterology guidelines on the management of irritable bowel syndrome. Gut 2021, 70, 1214–1240. [Google Scholar] [CrossRef] [PubMed]
- Creed, F.; Ratcliffe, J.; Fernandez, L.; Tomenson, B.; Palmer, S.; Rigby, C.; Guthrie, E.; Read, N.; Thompson, D. Health-related quality of life and health care costs in severe, refractory irritable bowel syndrome. Ann. Intern. Med. 2001, 134, 860–868. [Google Scholar] [CrossRef] [PubMed]
- Lacy, B.E.; Pimentel, M.; Brenner, D.M.; Chey, W.D.; Keefer, L.A.; Long, M.D.; Moshiree, B. ACG Clinical Guideline: Management of Irritable Bowel Syndrome. Am. J. Gastroenterol. 2021, 116, 17–44. [Google Scholar] [CrossRef] [PubMed]
- Chey, W.D.; Hashash, J.G.; Manning, L.; Chang, L. AGA Clinical Practice Update on the Role of Diet in Irritable Bowel Syndrome: Expert Review. Gastroenterology 2022, 162, 1737–1745.e5. [Google Scholar] [CrossRef] [PubMed]
- Cardo, A.; Churruca, I.; Lasa, A.; Navarro, V.; Vázquez-Polo, M.; Perez-Junkera, G.; Larretxi, I. Nutritional Imbalances in Adult Celiac Patients Following a Gluten-Free Diet. Nutrients 2021, 13, 2877. [Google Scholar] [CrossRef] [PubMed]
- Page, M.J.; E McKenzie, J.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Moher, D. Updating guidance for reporting systematic reviews: Development of the PRISMA 2020 statement. J. Clin. Epidemiol. 2021, 134, 103–112. [Google Scholar] [CrossRef] [PubMed]
- Van Megen, F.; Skodje, G.I.; Lergenmuller, S.; Zühlke, S.; Aabakken, L.; Veierød, M.B.; Henriksen, C.; Lundin, K.E. A Low FODMAP Diet Reduces Symptoms in Treated Celiac Patients with Ongoing Symptoms-A Randomized Controlled Trial. Clin. Gastroenterol. Hepatol. 2022, 20, 2258–2266. [Google Scholar] [CrossRef] [PubMed]
- Roncoroni, L.; Bascuñán, K.A.; Doneda, L.; Scricciolo, A.; Lombardo, V.; Branchi, F.; Ferretti, F.; Dell’osso, B.; Montanari, V.; Bardella, M.T.; et al. A Low FODMAP Gluten-Free Diet Improves Functional Gastrointestinal Disorders and Overall Mental Health of Celiac Disease Patients: A Randomized Controlled Trial. Nutrients 2018, 10, 1023. [Google Scholar] [CrossRef] [PubMed]
- Testa, A.; Imperatore, N.; Rispo, A.; Rea, M.; Tortora, R.; Nardone, O.M.; Lucci, L.; Accarino, G.; Caporaso, N.; Castiglione, F. Beyond Irritable Bowel Syndrome: The Efficacy of the Low Fodmap Diet for Improving Symptoms in Inflammatory Bowel Diseases and Celiac Disease. Dig. Dis. 2018, 36, 271–280. [Google Scholar] [CrossRef] [PubMed]
- Trott, N.; Rej, A.; Coleman, S.H.; Sanders, D.S. Adult celiac disease with persistent IBS-type symptoms: A pilot study of an adjuvant FODMAP diet. Gastroenterol. Hepatol. Bed Bench 2021, 14, 304–310. [Google Scholar] [PubMed]
- Roncoroni, L.; Elli, L.; Doneda, L.; Bascuñán, K.A.; Vecchi, M.; Morreale, F.; Scricciolo, A.; Lombardo, V.; Pellegrini, N. A Retrospective Study on Dietary FODMAP Intake in Celiac Patients Following a Gluten-Free Diet. Nutrients 2018, 10, 1769. [Google Scholar] [CrossRef] [PubMed]
- Cyrkot, S.; Marcon, M.; Brill, H.; Mileski, H.; Dowhaniuk, J.; Frankish, A.; Carroll, M.W.; Persad, R.; Turner, J.M.; Mager, D.R. FODMAP intake in children with coeliac disease influences diet quality and health-related quality of life and has no impact on gastrointestinal symptoms. Int. J. Food Sci. Nutr. 2021, 72, 956–967. [Google Scholar] [CrossRef] [PubMed]
- Schiepatti, A.; Maimaris, S.; Nicolardi, M.L.; Alimenti, E.; Vernero, M.; Costetti, M.; Costa, S.; Biagi, F. Determinants and Trends of Adherence to a Gluten-Free Diet in Adult Celiac Patients on a Long-term Follow-up (2000–2020). Clin. Gastroenterol. Hepatol. 2022, 20, e741–e749. [Google Scholar] [CrossRef]
- Vernero, M.; Schiepatti, A.; Maimaris, S.; Lusetti, F.; Scalvini, D.; Megang, F.; Nicolardi, M.L.; Gabrielli, G.M.; Sprio, E.; Baiardi, P.; et al. The GLU-10: A validated ten-point score to identify poorly instructed celiac patients in need of dietary interventions. Minerva Gastroenterol. 2022, 68, 91–97. [Google Scholar] [CrossRef] [PubMed]
- Halmos, E.P.; Deng, M.; Knowles, S.R.; Sainsbury, K.; Mullan, B.; Tye-Din, J.A. Food knowledge and psychological state predict adherence to a gluten-free diet in a survey of 5310 Australians and New Zealanders with coeliac disease. Aliment. Pharmacol. Ther. 2018, 48, 78–86. [Google Scholar] [CrossRef] [PubMed]
- Sainsbury, K.; Halmos, E.P.; Knowles, S.; Mullan, B.; Tye-Din, J.A. Maintenance of a gluten free diet in coeliac disease: The roles of self-regulation, habit, psychological resources, motivation, support, and goal priority. Appetite 2018, 125, 356–366. [Google Scholar] [CrossRef] [PubMed]
- Biagi, F.; Schiepatti, A.; Maiorano, G.; Fraternale, G.; Agazzi, S.; Zingone, F.; Ciacci, C.; Volta, U.; Caio, G.; Tortora, R.; et al. Risk of complications in coeliac patients depends on age at diagnosis and type of clinical presentation. Dig. Liver Dis. 2018, 50, 549–552. [Google Scholar] [CrossRef] [PubMed]
- Green, P.H.; Paski, S.; Ko, C.W.; Rubio-Tapia, A. AGA Clinical Practice Update on Management of Refractory Celiac Disease: Expert Review. Gastroenterology 2022, 163, 1461–1469. [Google Scholar] [CrossRef] [PubMed]
- Kurien, M.; Barratt, S.M.; Sanders, D.S. Functional gastrointestinal disorders and coeliac disease in adults—Negative impact on quality of life. Aliment. Pharmacol. Ther. 2011, 34, 1044–1045, author reply 1045–1046. [Google Scholar] [CrossRef]
- Schiepatti, A.; Bellani, V.; Perlato, M.; Maimaris, S.; Klersy, C.; Biagi, F. Inadvertent and minimal gluten intake has a negligible role in the onset of symptoms in patients with coeliac disease on a gluten-free diet. Br. J. Nutr. 2019, 121, 576–581. [Google Scholar] [CrossRef] [PubMed]
- Wolf, R.L.; Lebwohl, B.; Lee, A.R.; Zybert, P.; Reilly, N.R.; Cadenhead, J.; Amengual, C.; Green, P.H. Hypervigilance to a gluten-free diet and decreased quality of life in teenagers and adults with celiac disease. Dig. Dis. Sci. 2018, 63, 1438–1448. [Google Scholar] [CrossRef] [PubMed]
- Ludvigsson, J.F.; Lebwohl, B.; Chen, Q.; Bröms, G.; Wolf, R.L.; Green, P.H.; Emilsson, L. Anxiety after coeliac disease diagnosis predicts mucosal healing: A population-based study. Aliment. Pharmacol. Ther. 2018, 48, 1091–1098. [Google Scholar] [CrossRef] [PubMed]
- Clappison, E.; Hadjivassiliou, M.; Zis, P. Psychiatric manifestations of coeliac disease, a systematic review and meta-analysis. Nutrients 2020, 12, 142. [Google Scholar] [CrossRef] [PubMed]
- Muir, J.G.; Varney, J.E.; Ajamian, M.; Gibson, P. Gluten-free and low-FODMAP sourdoughs for patients with coeliac disease and irritable bowel syndrome: A clinical perspective. Int. J. Food Microbiol. 2019, 290, 237–246. [Google Scholar] [CrossRef] [PubMed]
- Myhrstad, M.C.W.; Slydahl, M.; Hellmann, M.; Garnweidner-Holme, L.; Lundin, K.E.A.; Henriksen, C.; Telle-Hansen, V.H. Nutritional quality and costs of gluten-free products: A case-control study of food products on the Norwegian marked. Food Nutr. Res. 2021, 65. [Google Scholar] [CrossRef] [PubMed]
- Cadenhead, J.W.; Martínez-Steele, E.; Contento, I.; Kushi, L.H.; Lee, A.R.; Nguyen, T.T.T.; Lebwohl, B.; Green, P.H.; Wolf, R.L. Diet quality, ultra-processed food consumption, and quality of life in a cross-sectional cohort of adults and teens with celiac disease. J. Hum. Nutr. Diet. 2023, 36, 1144–1158. [Google Scholar] [CrossRef] [PubMed]
- Mambrini, S.P.; Menichetti, F.; Ravella, S.; Pellizzari, M.; De Amicis, R.; Foppiani, A.; Battezzati, A.; Bertoli, S.; Leone, A. Ultra-Processed Food Consumption and Incidence of Obesity and Cardiometabolic Risk Factors in Adults: A Systematic Review of Prospective Studies. Nutrients 2023, 15, 2583. [Google Scholar] [CrossRef] [PubMed]
- Sugavanam, T.; Crocker, H.; Violato, M.; Peters, M. The financial impact on people with coeliac disease of withdrawing gluten-free food from prescriptions in England: Findings from a cross-sectional survey. BMC Health Serv. Res. 2024, 24, 146. [Google Scholar] [CrossRef] [PubMed]
- Martínez-Rodríguez, A.; Loaiza-Martínez, D.A.; Sánchez-Sánchez, J.; Rubio-Arias, J.Á.; Alacid, F.; Prats-Moya, S.; Martínez-Olcina, M.; Yáñez-Sepúlveda, R.; Marcos-Pardo, P.J. Personalised Nutritional Plan and Resistance Exercise Program to Improve Health Parameters in Celiac Women. Foods 2022, 11, 3238. [Google Scholar] [CrossRef] [PubMed]
- Vereczkei, Z.; Farkas, N.; Hegyi, P.; Imrei, M.; Földi, M.; Szakács, Z.; Kiss, S.; Solymár, M.; Nagy, R.; Bajor, J. It Is High Time for Personalized Dietary Counseling in Celiac Disease: A Systematic Review and Meta-Analysis on Body Composition. Nutrients 2021, 13, 2947. [Google Scholar] [CrossRef]
- Cox, S.R.; Lindsay, J.O.; Fromentin, S.; Stagg, A.J.; McCarthy, N.E.; Galleron, N.; Ibraim, S.B.; Roume, H.; Levenez, F.; Pons, N.; et al. Effects of Low FODMAP Diet on Symptoms, Fecal Microbiome, and Markers of Inflammation in Patients with Quiescent Inflammatory Bowel Disease in a Randomized Trial. Gastroenterology 2020, 158, 176–188.e7. [Google Scholar] [CrossRef] [PubMed]
- Bodini, G.; Zanella, C.; Crespi, M.; Pumo, S.L.; Demarzo, M.G.; Savarino, E.; Savarino, V.; Giannini, E.G. A randomized, 6-wk trial of a low FODMAP diet in patients with inflammatory bowel disease. Nutrition 2019, 67–68, 110542. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Study | Country | Study Design | Enrolment Criteria | Intervention | Patients, N | Primary Outcome | Primary Outcome Results | Secondary Outcomes | Secondary Outcome Results |
|---|---|---|---|---|---|---|---|---|---|
| Roncoroni 2018 [29] | Italy | Retrospective cohort study | Adult patients with CD on a GFD | None | 104 CD 91 healthy controls | Dietary FODMAP intake | FODMAP intake was lower in celiac patients on a GFD (p < 0.001) | Prevalence of IBS and FGIDs | No significant difference in the prevalence of IBS and FGIDs in CD vs. controls (p: NS) |
| Van Megen 2022 [25] | Norway | Open-label parallel-group RCT | Adult celiac patients on a GFD for ≥12 months with serologic and mucosal remission and persistent symptoms (GSRS-IBS ≥ 30) | Low-FODMAP GFD vs. usual GFD for 4 weeks | 70 CD (34 in the intervention group and 36 in the control group) | Improvement of symptoms (reduction in GSRS-IBS ≥ 7) by week 4 | GSRS-IBS was significantly lower at week 4 in the intervention group (MD −10.8, 95% CI −6.8 to −14.8) (p interaction < 0.001) | CSI score, CFQ score, and FODMAP intake at week 4 | All secondary outcome measures were significantly lower in the intervention group (CSI score: p = 0.003; CFQ: p = 0.02; FODMAP intake p < 0.001) |
| Roncoroni 2018 [26] | Italy | RCT | Adult patients with CD on a GFD for ≥12 months with serologic remission and IBS-like symptoms according to the Rome III criteria and a global well-being score assessed by a VAS < 4 | Low-FODMAP GFD vs. usual GFD for 21 days | 50 CD (25 in the intervention group 25 in the control group) | Improvement of gastrointestinal symptoms and general well-being (assessed by a VAS), psychological symptoms (SCL-90), and QOL (SF-36) after 21 days | Reduced global SCL-90 index (p < 0.0003) in the intervention group. Lower VAS for abdominal pain (p < 0.01) and higher VAS for faecal consistency (p < 0.09) in the intervention group. General well-being improved more in the intervention group (p = 0.03) | - | - |
| Testa 2018 [27] | Italy | Dietetic interventional prospective study | Adult patients with CD on a GFD for ≥12 months with serologic remission and IBS-like symptoms according to the Rome III criteria | Low-FODMAP diet (LOW-FODMAP GFD for the CD group) for 3 months | 127 pts: 56 with IBS, 30 with IBD in clinical remission, and 41 with CD | Improvement of gastrointestinal symptoms (IBS-SSS) after 1 and 3 months | Gastrointestinal symptoms improved after 1 and 3 months in all patients, with no significant difference between the groups (p = NS) | Improvement of QOL (SF-36) | No difference between the 3 groups in terms of response to diet (p = NS), but there was a clinical improvement after 3 months for most of the questionnaire’s domains |
| Trott 2021 [28] | UK | Open-label prospective interventional pilot study | Adult patients with CD on a GFD for ≥24 months in mucosal remission and IBS-like symptoms according to the Rome III criteria | Low-FODMAP diet (no comparator) for 4 weeks | 15 CD | Improvement of symptoms (evaluated with GSRS-IBS) after a minimum of 4 weeks of an adjuvant low-FODMAP diet | Global relief of gut symptoms reported by 8/15 patients (53% p = 0.007), with significant reductions in abdominal pain (p < 0.01), distension (p < 0.02), and flatulence (p < 0.01). | - | - |
| Cyrkot 2021 [30] | Canada | Cross-sectional study | Children aged 5–18 years with biopsy-proven CD on GFD | None | 46 CD 46 non-celiac mild chronic gastrointestinal complaints (GIC) 46 healthy controls (HC) | Evaluation of the association between FODMAP consumption and gastrointestinal symptoms (PedsQLTM GI Symptom Scale ([GSS]), diet quality (Canadian Healthy Eating Index (HEI-C)), and health-related quality of life (PedsQLTM 4.0 Generic Core Scales) | CD children consumed fewer foods high in FODMAPs compared to GIC and HC (p < 0.0001). FODMAP intake was not related to GSS in CD children (p > 0.05) but positively associated with child health-related quality of life (p < 0.05). FODMAP intake from fruits and vegetables was positively associated with diet adequacy and total diet quality in CD children (p < 0.05). | - | - |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lusetti, F.; Schiepatti, A.; Scalvini, D.; Maimaris, S.; Biagi, F. Efficacy of a Low-FODMAP Diet for Coeliac Patients with Persistent IBS-like Symptoms despite a Gluten-Free Diet: A Systematic Review. Nutrients 2024, 16, 1094. https://doi.org/10.3390/nu16071094
Lusetti F, Schiepatti A, Scalvini D, Maimaris S, Biagi F. Efficacy of a Low-FODMAP Diet for Coeliac Patients with Persistent IBS-like Symptoms despite a Gluten-Free Diet: A Systematic Review. Nutrients. 2024; 16(7):1094. https://doi.org/10.3390/nu16071094
Chicago/Turabian StyleLusetti, Francesca, Annalisa Schiepatti, Davide Scalvini, Stiliano Maimaris, and Federico Biagi. 2024. "Efficacy of a Low-FODMAP Diet for Coeliac Patients with Persistent IBS-like Symptoms despite a Gluten-Free Diet: A Systematic Review" Nutrients 16, no. 7: 1094. https://doi.org/10.3390/nu16071094
APA StyleLusetti, F., Schiepatti, A., Scalvini, D., Maimaris, S., & Biagi, F. (2024). Efficacy of a Low-FODMAP Diet for Coeliac Patients with Persistent IBS-like Symptoms despite a Gluten-Free Diet: A Systematic Review. Nutrients, 16(7), 1094. https://doi.org/10.3390/nu16071094