
Exercise Prescription for Postprandial Glycemic Management

 ,
,  , and
, and 
Abstract
1. Introduction
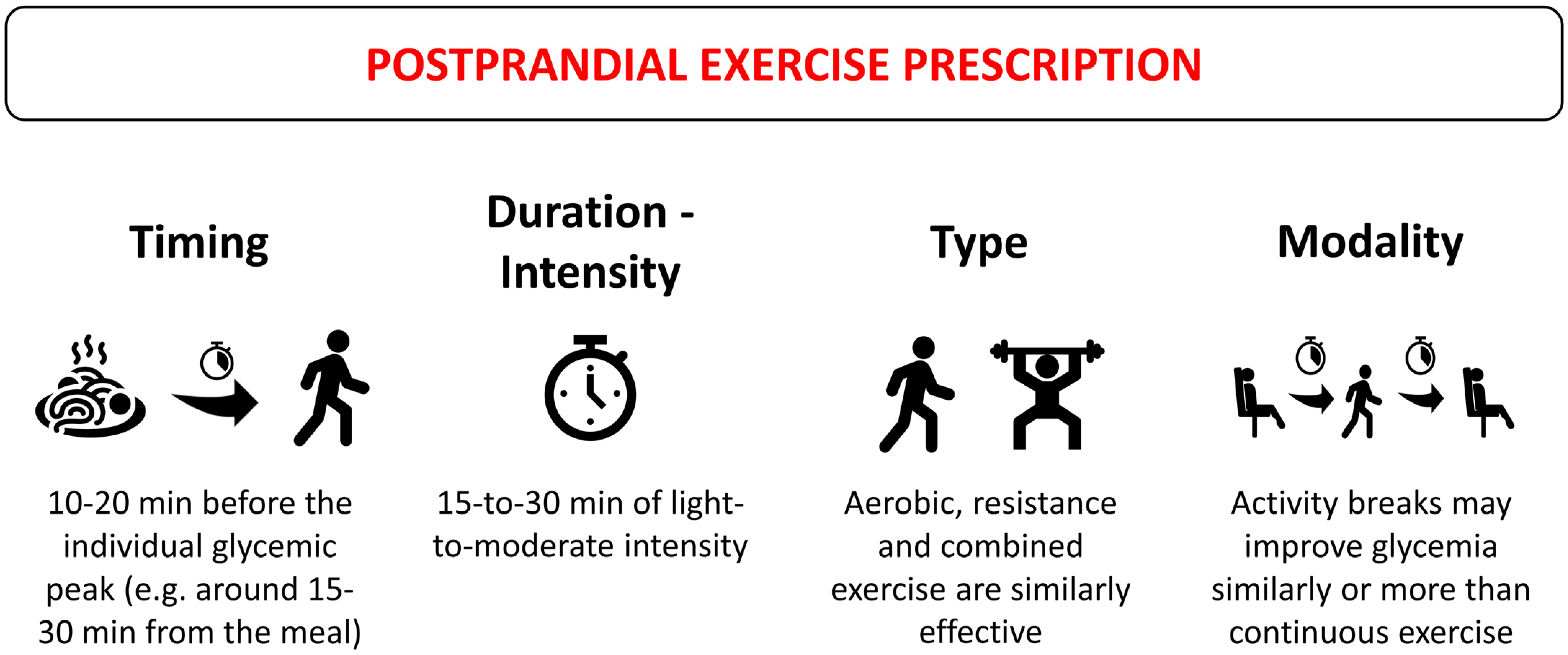
2. Is There an Optimal Time for Exercise Relative to Meals? The Effects of Exercise Timing on Postprandial Glucose Response
3. Which Type of Exercise Is the Most Effective?
4. What Should Be the Exercise Duration and Intensity?
5. Activity Breaks: An Effective Exercise Modality
6. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Ceriello, A.; Ihnat, M.A. ‘Glycaemic Variability’: A New Therapeutic Challenge in Diabetes and the Critical Care Setting. Diabet. Med. 2010, 27, 862–867. [Google Scholar] [CrossRef] [PubMed]
- Færch, K.; Alssema, M.; Mela, D.J.; Borg, R.; Vistisen, D. Relative Contributions of Preprandial and Postprandial Glucose Exposures, Glycemic Variability, and Non-Glycemic Factors to HbA 1c in Individuals with and without Diabetes. Nutr. Diabetes 2018, 8, 38. [Google Scholar] [CrossRef] [PubMed]
- Standl, E.; Schnell, O.; Ceriello, A. Postprandial Hyperglycemia and Glycemic Variability. Diabetes Care 2011, 34, S120–S127. [Google Scholar] [CrossRef] [PubMed]
- Monnier, L.; Colette, C. Contributions of Fasting and Postprandial Glucose to Hemoglobin A1c. Endocr. Pract. 2006, 12, 42–46. [Google Scholar] [CrossRef] [PubMed]
- Monnier, L.; Colette, C.; Owens, D.R. Glycemic Variability: The Third Component of the Dysglycemia in Diabetes. Is It Important? How to Measure It? J. Diabetes Sci. Technol. 2008, 2, 1094–1100. [Google Scholar] [CrossRef] [PubMed]
- Coutinho, M.; Gerstein, H.C.; Wang, Y.; Yusuf, S. The Relationship between Glucose and Incident Cardiovascular Events. A Metaregression Analysis of Published Data from 20 Studies of 95,783 Individuals Followed for 12.4 Years. Diabetes Care 1999, 22, 233–240. [Google Scholar] [CrossRef] [PubMed]
- Giugliano, D.; Ceriello, A.; Esposito, K. Glucose Metabolism and Hyperglycemia. Am. J. Clin. Nutr. 2008, 87, 217S–222S. [Google Scholar] [CrossRef] [PubMed]
- O’Keefe, J.H.; Bell, D.S.H. Postprandial Hyperglycemia/Hyperlipidemia (Postprandial Dysmetabolism) Is a Cardiovascular Risk Factor. Am. J. Cardiol. 2007, 100, 899–904. [Google Scholar] [CrossRef] [PubMed]
- Rendell, M.S.; Jovanovic, L. Targeting Postprandial Hyperglycemia. Metabolism 2006, 55, 1263–1281. [Google Scholar] [CrossRef]
- Teo, S.Y.M.; Kanaley, J.A.; Guelfi, K.J.; Cook, S.B.; Hebert, J.J.; Forrest, M.R.L.; Fairchild, T.J. Exercise Timing in Type 2 Diabetes Mellitus: A Systematic Review. Med. Sci. Sports Exerc. 2018, 50, 2387–2397. [Google Scholar] [CrossRef]
- Haxhi, J.; Scotto di Palumbo, A.; Sacchetti, M. Exercising for Metabolic Control: Is Timing Important? Ann. Nutr. Metab. 2013, 62, 14–25. [Google Scholar] [CrossRef]
- Chacko, E. Exercising Tactically for Taming Postmeal Glucose Surges. Scientifica 2016, 2016, 4045717. [Google Scholar] [CrossRef] [PubMed]
- Engeroff, T.; Groneberg, D.A.; Wilke, J. After Dinner Rest a While, After Supper Walk a Mile? A Systematic Review with Meta-Analysis on the Acute Postprandial Glycemic Response to Exercise Before and After Meal Ingestion in Healthy Subjects and Patients with Impaired Glucose Tolerance. Sports Med. 2023, 53, 849–869. [Google Scholar] [CrossRef]
- Aqeel, M.; Forster, A.; Richards, E.; Hennessy, E.; McGowan, B.; Bhadra, A.; Guo, J.; Gelfand, S.; Delp, E.; Eicher-Miller, H. The Effect of Timing of Exercise and Eating on Postprandial Response in Adults: A Systematic Review. Nutrients 2020, 12, 221. [Google Scholar] [CrossRef] [PubMed]
- Hamilton, M.T.; Healy, G.N.; Dunstan, D.W.; Zderic, T.W.; Owen, N. Too Little Exercise and Too Much Sitting: Inactivity Physiology and the Need for New Recommendations on Sedentary Behavior. Curr. Cardiovasc. Risk Rep. 2008, 2, 292–298. [Google Scholar] [CrossRef]
- Kohl, H.W.; Craig, C.L.; Lambert, E.V.; Inoue, S.; Alkandari, J.R.; Leetongin, G.; Kahlmeier, S. The Pandemic of Physical Inactivity: Global Action for Public Health. Lancet 2012, 380, 294–305. [Google Scholar] [CrossRef]
- Tremblay, M.S.; Colley, R.C.; Saunders, T.J.; Healy, G.N.; Owen, N. Physiological and Health Implications of a Sedentary Lifestyle. Appl. Physiol. Nutr. Metab. 2010, 35, 725–740. [Google Scholar] [CrossRef]
- Healy, G.N.; Wijndaele, K.; Dunstan, D.W.; Shaw, J.E.; Salmon, J.; Zimmet, P.Z.; Owen, N. Objectively Measured Sedentary Time, Physical Activity, and Metabolic Risk. Diabetes Care 2008, 31, 369–371. [Google Scholar] [CrossRef] [PubMed]
- Dempsey, P.C.; Owen, N.; Yates, T.E.; Kingwell, B.A.; Dunstan, D.W. Sitting Less and Moving More: Improved Glycaemic Control for Type 2 Diabetes Prevention and Management. Curr. Diabetes Rep. 2016, 16, 114. [Google Scholar] [CrossRef]
- Kanaley, J.A.; Colberg, S.R.; Corcoran, M.H.; Malin, S.K.; Rodriguez, N.R.; Crespo, C.J.; Kirwan, J.P.; Zierath, J.R. Exercise/Physical Activity in Individuals with Type 2 Diabetes: A Consensus Statement from the American College of Sports Medicine. Med. Sci. Sports Exerc. 2022, 54, 353–368. [Google Scholar] [CrossRef]
- Erickson, M.L.; Jenkins, N.T.; McCully, K.K. Exercise after You Eat: Hitting the Postprandial Glucose Target. Front. Endocrinol. 2017, 8, 228. [Google Scholar] [CrossRef] [PubMed]
- Reid, R.E.R.; Thivel, D.; Mathieu, M.-E. Understanding the Potential Contribution of a Third “T” to FITT Exercise Prescription: The Case of Timing in Exercise for Obesity and Cardiometabolic Management in Children. Appl. Physiol. Nutr. Metab. 2019, 44, 911–914. [Google Scholar] [CrossRef]
- Bellini, A.; Nicolò, A.; Bazzucchi, I.; Sacchetti, M. Effects of Different Exercise Strategies to Improve Postprandial Glycemia in Healthy Individuals. Med. Sci. Sports Exerc. 2021, 53, 1334–1344. [Google Scholar] [CrossRef] [PubMed]
- Bellini, A.; Nicolò, A.; Bulzomì, R.; Bazzucchi, I.; Sacchetti, M. The Effect of Different Postprandial Exercise Types on Glucose Response to Breakfast in Individuals with Type 2 Diabetes. Nutrients 2021, 13, 1440. [Google Scholar] [CrossRef] [PubMed]
- Heden, T.D.; Liu, Y.; Kearney, M.L.; Park, Y.; Dellsperger, K.C.; Thomas, T.R.; Kanaley, J.A. Prior Exercise and Postprandial Incretin Responses in Lean and Obese Individuals. Med. Sci. Sports Exerc. 2013, 45, 1897–1905. [Google Scholar] [CrossRef] [PubMed]
- Rees, J.L.; Chang, C.R.; François, M.E.; Marcotte-Chénard, A.; Fontvieille, A.; Klaprat, N.D.; Dyck, R.A.; Funk, D.R.; Snydmiller, G.; Bastell, K.; et al. Minimal Effect of Walking before Dinner on Glycemic Responses in Type 2 Diabetes: Outcomes from the Multi-Site E-PAraDiGM Study. Acta Diabetol. 2019, 56, 755–765. [Google Scholar] [CrossRef]
- Heden, T.D.; Winn, N.C.; Mari, A.; Booth, F.W.; Rector, R.S.; Thyfault, J.P.; Kanaley, J.A. Postdinner Resistance Exercise Improves Postprandial Risk Factors More Effectively than Predinner Resistance Exercise in Patients with Type 2 Diabetes. J. Appl. Physiol. 2015, 118, 624–634. [Google Scholar] [CrossRef] [PubMed]
- Karstoft, K.; Christensen, C.S.; Pedersen, B.K.; Solomon, T.P.J. The Acute Effects of Interval- Vs Continuous-Walking Exercise on Glycemic Control in Subjects with Type 2 Diabetes: A Crossover, Controlled Study. J. Clin. Endocrinol. Metab. 2014, 99, 3334–3342. [Google Scholar] [CrossRef] [PubMed]
- Francois, M.E.; Baldi, J.C.; Manning, P.J.; Lucas, S.J.E.; Hawley, J.A.; Williams, M.J.A.; Cotter, J.D. ‘Exercise Snacks’ before Meals: A Novel Strategy to Improve Glycaemic Control in Individuals with Insulin Resistance. Diabetologia 2014, 57, 1437–1445. [Google Scholar] [CrossRef]
- Hatamoto, Y.; Goya, R.; Yamada, Y.; Yoshimura, E.; Nishimura, S.; Higaki, Y.; Tanaka, H. Effect of Exercise Timing on Elevated Postprandial Glucose Levels. J. Appl. Physiol. 2017, 123, 278–284. [Google Scholar] [CrossRef]
- Bellini, A.; Nicolò, A.; Bazzucchi, I.; Sacchetti, M. The Effects of Postprandial Walking on the Glucose Response after Meals with Different Characteristics. Nutrients 2022, 14, 1080. [Google Scholar] [CrossRef] [PubMed]
- Bellini, A.; Nicolò, A.; Rocchi, J.E.; Bazzucchi, I.; Sacchetti, M. Walking Attenuates Postprandial Glycemic Response: What Else Can We Do without Leaving Home or the Office? IJERPH 2022, 20, 253. [Google Scholar] [CrossRef] [PubMed]
- Nygaard, H.; Rønnestad, B.R.; Hammarström, D.; Holmboe-Ottesen, G.; Høstmark, A.T. Effects of Exercise in the Fasted and Postprandial State on Interstitial Glucose in Hyperglycemic Individuals. J. Sports Sci. Med. 2017, 16, 254–263. [Google Scholar] [PubMed]
- Solomon, T.P.J.; Tarry, E.; Hudson, C.O.; Fitt, A.I.; Laye, M.J. Immediate Post-Breakfast Physical Activity Improves Interstitial Postprandial Glycemia: A Comparison of Different Activity-Meal Timings. Pflug. Arch. Eur. J. Physiol. 2020, 472, 271–280. [Google Scholar] [CrossRef] [PubMed]
- Colberg, S.R.; Zarrabi, L.; Bennington, L.; Nakave, A.; Thomas Somma, C.; Swain, D.P.; Sechrist, S.R. Postprandial Walking Is Better for Lowering the Glycemic Effect of Dinner than Pre-Dinner Exercise in Type 2 Diabetic Individuals. J. Am. Med. Dir. Assoc. 2009, 10, 394–397. [Google Scholar] [CrossRef] [PubMed]
- Yoko, N.; Hiroshi, Y.; Ying, J. Type and Timing of Exercise during Lunch Breaks for Suppressing Postprandial Increases in Blood Glucose Levels in Workers. J. Occup. Health 2021, 63, e12199. [Google Scholar] [CrossRef] [PubMed]
- Reynolds, A.; Venn, B. The Timing of Activity after Eating Affects the Glycaemic Response of Healthy Adults: A Randomised Controlled Trial. Nutrients 2018, 10, 1743. [Google Scholar] [CrossRef] [PubMed]
- Zhang, X.; Wongpipit, W.; Sun, F.; Sheridan, S.; Huang, W.Y.; Sit, C.H.; Wong, S.H. Walking Initiated 20 Minutes before the Time of Individual Postprandial Glucose Peak Reduces the Glucose Response in Young Men with Overweight or Obesity: A Randomized Crossover Study. J. Nutr. 2021, 151, 866–875. [Google Scholar] [CrossRef]
- Slama, G.; Elgrably, F.; Sola, A.; Mbemba, J.; Larger, E. Postprandial Glycaemia: A Plea for the Frequent Use of Delta Postprandial Glycaemia in the Treatment of Diabetic Patients. Diabetes Metab. 2006, 32, 187–192. [Google Scholar] [CrossRef]
- Huang, T.; Lu, C.; Schumann, M.; Le, S.; Yang, Y.; Zhuang, H.; Lu, Q.; Liu, J.; Wiklund, P.; Cheng, S. Timing of Exercise Affects Glycemic Control in Type 2 Diabetes Patients Treated with Metformin. J. Diabetes Res. 2018, 2018, 2483273. [Google Scholar] [CrossRef]
- Van Dijk, J.-W.; Venema, M.; Van Mechelen, W.; Stehouwer, C.D.A.; Hartgens, F.; Van Loon, L.J.C. Effect of Moderate-Intensity Exercise Versus Activities of Daily Living on 24-Hour Blood Glucose Homeostasis in Male Patients with Type 2 Diabetes. Diabetes Care 2013, 36, 3448–3453. [Google Scholar] [CrossRef] [PubMed]
- Moreno-Cabañas, A.; Gonzalez, J.T. Role of Prior Feeding Status in Mediating the Effects of Exercise on Blood Glucose Kinetics. Am. J. Physiol. Cell Physiol. 2023, 325, C823–C832. [Google Scholar] [CrossRef] [PubMed]
- Kang, J.; Fardman, B.M.; Ratamess, N.A.; Faigenbaum, A.D.; Bush, J.A. Efficacy of Postprandial Exercise in Mitigating Glycemic Responses in Overweight Individuals and Individuals with Obesity and Type 2 Diabetes—A Systematic Review and Meta-Analysis. Nutrients 2023, 15, 4489. [Google Scholar] [CrossRef]
- Holst, J.J.; Albrechtsen, N.J.W.; Rosenkilde, M.M.; Deacon, C.F. Physiology of the Incretin Hormones, GIP and GLP-1—Regulation of Release and Posttranslational Modifications. Compr. Physiol. 2019, 9, 1339–1381. [Google Scholar] [CrossRef] [PubMed]
- Zeevi, D.; Korem, T.; Zmora, N.; Israeli, D.; Rothschild, D.; Weinberger, A.; Ben-Yacov, O.; Lador, D.; Avnit-Sagi, T.; Lotan-Pompan, M.; et al. Personalized Nutrition by Prediction of Glycemic Responses. Cell 2015, 163, 1079–1094. [Google Scholar] [CrossRef] [PubMed]
- Carter, S.; Solomon, T.P.J. Exercise-Induced Improvements in Postprandial Glucose Response Are Blunted by Pre-Exercise Hyperglycemia: A Randomized Crossover Trial in Healthy Individuals. Front. Endocrinol. 2020, 11, 566548. [Google Scholar] [CrossRef] [PubMed]
- Chang, C.R.; Russell, B.M.; Cyriac, T.; Francois, M.E. Using Continuous Glucose Monitoring to Prescribe a Time to Exercise for Individuals with Type 2 Diabetes. JCM 2023, 12, 3237. [Google Scholar] [CrossRef] [PubMed]
- Edinburgh, R.M.; Koumanov, F.; Gonzalez, J.T. Impact of Pre-exercise Feeding Status on Metabolic Adaptations to Endurance-type Exercise Training. J. Physiol. 2022, 600, 1327–1338. [Google Scholar] [CrossRef] [PubMed]
- Haxhi, J.; Leto, G.; Di Palumbo, A.S.; Sbriccoli, P.; Guidetti, L.; Fantini, C.; Buzzetti, R.; Caporossi, D.; Di Luigi, L.; Sacchetti, M. Exercise at Lunchtime: Effect on Glycemic Control and Oxidative Stress in Middle-Aged Men with Type 2 Diabetes. Eur. J. Appl. Physiol. 2016, 116, 573–582. [Google Scholar] [CrossRef]
- Sacchetti, M.; Haxhi, J.; Sgrò, P.; Scotto Di Palumbo, A.; Nicolò, A.; Bellini, A.; Bazzucchi, I.; Di Luigi, L. Effects of Exercise before and/or after a Mixed Lunch on Postprandial Metabolic Responses in Healthy Male Individuals. Eur. J. Nutr. 2021, 60, 3437–3447. [Google Scholar] [CrossRef]
- Johnson-Bonson, D.A.; Narang, B.J.; Davies, R.G.; Hengist, A.; Smith, H.A.; Watkins, J.D.; Taylor, H.; Walhin, J.-P.; Gonzalez, J.T.; Betts, J.A. Interactive Effects of Acute Exercise and Carbohydrate-Energy Replacement on Insulin Sensitivity in Healthy Adults. Appl. Physiol. Nutr. Metab. 2021, 46, 1207–1215. [Google Scholar] [CrossRef] [PubMed]
- Erickson, M.L.; Little, J.P.; Gay, J.L.; McCully, K.K.; Jenkins, N.T. Postmeal Exercise Blunts Postprandial Glucose Excursions in People on Metformin Monotherapy. J. Appl. Physiol. 2017, 123, 444–450. [Google Scholar] [CrossRef] [PubMed]
- Boulé, N.G.; Robert, C.; Bell, G.J.; Johnson, S.T.; Bell, R.C.; Lewanczuk, R.Z.; Gabr, R.Q.; Brocks, D.R. Metformin and Exercise in Type 2 Diabetes. Diabetes Care 2011, 34, 1469–1474. [Google Scholar] [CrossRef] [PubMed]
- Myette-Côté, É.; Terada, T.; Boulé, N.G. The Effect of Exercise with or Without Metformin on Glucose Profiles in Type 2 Diabetes: A Pilot Study. Can. J. Diabetes 2016, 40, 173–177. [Google Scholar] [CrossRef] [PubMed]
- Pilmark, N.S.; Lyngbæk, M.; Oberholzer, L.; Elkjær, I.; Petersen-Bønding, C.; Kofoed, K.; Siebenmann, C.; Kellenberger, K.; Van Hall, G.; Abildgaard, J.; et al. The Interaction between Metformin and Physical Activity on Postprandial Glucose and Glucose Kinetics: A Randomised, Clinical Trial. Diabetologia 2021, 64, 397–409. [Google Scholar] [CrossRef] [PubMed]
- on behalf of the Diabetes Aerobic and Resistance Exercise (DARE) trial investigators; Larose, J.; Sigal, R.J.; Khandwala, F.; Prud’homme, D.; Boulé, N.G.; Kenny, G.P. Associations between Physical Fitness and HbA1c in Type 2 Diabetes Mellitus. Diabetologia 2011, 54, 93–102. [Google Scholar] [CrossRef] [PubMed]
- Sigal, R.J.; Kenny, G.P.; Boulé, N.G.; Wells, G.A.; Prud’homme, D.; Fortier, M.; Reid, R.D.; Tulloch, H.; Coyle, D.; Phillips, P.; et al. Effects of Aerobic Training, Resistance Training, or Both on Glycemic Control in Type 2 Diabetes: A Randomized Trial. Ann. Intern. Med. 2007, 147, 357. [Google Scholar] [CrossRef] [PubMed]
- Munan, M.; Oliveira, C.L.P.; Marcotte-Chénard, A.; Rees, J.L.; Prado, C.M.; Riesco, E.; Boulé, N.G. Acute and Chronic Effects of Exercise on Continuous Glucose Monitoring Outcomes in Type 2 Diabetes: A Meta-Analysis. Front. Endocrinol. 2020, 11, 495. [Google Scholar] [CrossRef] [PubMed]
- Van Dijk, J.-W.; Tummers, K.; Stehouwer, C.D.A.; Hartgens, F.; Van Loon, L.J.C. Exercise Therapy in Type 2 Diabetes. Diabetes Care 2012, 35, 948–954. [Google Scholar] [CrossRef]
- Aadland, E.; Hostmark, A.T. Very Light Physical Activity after a Meal Blunts the Rise in Blood Glucose and Insulin. Open Nutr. J. 2008, 2, 94–99. [Google Scholar] [CrossRef]
- Karstoft, K.; Mortensen, S.P.; Knudsen, S.H.; Solomon, T.P.J. Direct Effect of Incretin Hormones on Glucose and Glycerol Metabolism and Hemodynamics. Am. J. Physiol. Endocrinol. Metab. 2015, 308, E426–E433. [Google Scholar] [CrossRef] [PubMed]
- Shambrook, P.; Kingsley, M.I.; Wundersitz, D.W.; Xanthos, P.D.; Wyckelsma, V.L.; Gordon, B.A. Glucose Response to Exercise in the Post-prandial Period Is Independent of Exercise Intensity. Scand. Med. Sci. Sports 2018, 28, 939–946. [Google Scholar] [CrossRef] [PubMed]
- Bartholomae, E.M.; Moore, J.; Ward, K.; Kressler, J. Sex Differences in Postprandial Glucose Response to Short Bouts of Exercise: A Randomized Controlled Trial. J. Sci. Med. Sport 2019, 22, 181–185. [Google Scholar] [CrossRef] [PubMed]
- Honda, H.; Igaki, M.; Hatanaka, Y.; Komatsu, M.; Tanaka, S.; Miki, T.; Suzuki, T.; Takaishi, T.; Hayashi, T. Stair Climbing/Descending Exercise for a Short Time Decreases Blood Glucose Levels after a Meal in Participants with Type 2 Diabetes. BMJ Open Diabetes Res. Care 2016, 4, e000232. [Google Scholar] [CrossRef] [PubMed]
- Moore, J.; Salmons, H.; Vinoskey, C.; Kressler, J. A Single One-Minute, Comfortable Paced, Stair-Climbing Bout Reduces Postprandial Glucose Following a Mixed Meal. Nutr. Metab. Cardiovasc. Dis. 2020, 30, 1967–1972. [Google Scholar] [CrossRef] [PubMed]
- Takaishi, T.; Hayashi, T. Stair Ascending–Descending Exercise Accelerates the Decrease in Postprandial Hyperglycemia More Efficiently than Bicycle Exercise. BMJ Open Diabetes Res. Care 2017, 5, e000428. [Google Scholar] [CrossRef] [PubMed]
- Andersen, E.; Høstmark, A.T. Effect of a Single Bout of Resistance Exercise on Postprandial Glucose and Insulin Response the Next Day in Healthy, Strength-Trained Men. J. Strength Cond. Res. 2007, 21, 487. [Google Scholar] [CrossRef] [PubMed]
- Bittel, A.J.; Bittel, D.C.; Mittendorfer, B.; Patterson, B.W.; Okunade, A.L.; Abumrad, N.A.; Reeds, D.N.; Cade, W.T. A Single Bout of Premeal Resistance Exercise Improves Postprandial Glucose Metabolism in Obese Men with Prediabetes. Med. Sci. Sports Exerc. 2021, 53, 694–703. [Google Scholar] [CrossRef]
- Moreira, S.R.; Simões, G.C.; Moraes, J.V.N.; Motta, D.F.; Campbell, C.S.G.; Simões, H.G. Blood Glucose Control for Individuals with Type-2 Diabetes: Acute Effects of Resistance Exercise of Lower Cardiovascular-Metabolic Stress. J. Strength Cond. Res. 2012, 26, 2806–2811. [Google Scholar] [CrossRef]
- Miyamoto, T.; Fukuda, K.; Kimura, T.; Matsubara, Y.; Tsuda, K.; Moritani, T. Effect of Percutaneous Electrical Muscle Stimulation on Postprandial Hyperglycemia in Type 2 Diabetes. Diabetes Res. Clin. Pract. 2012, 96, 306–312. [Google Scholar] [CrossRef]
- Jabbour, G.; Belliveau, L.; Probizanski, D.; Newhouse, I.; McAuliffe, J.; Jakobi, J.; Johnson, M. Effect of Low Frequency Neuromuscular Electrical Stimulation on Glucose Profile of Persons with Type 2 Diabetes: A Pilot Study. Diabetes Metab. J. 2015, 39, 264. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Holzer, R.; Schulte-Körne, B.; Seidler, J.; Predel, H.-G.; Brinkmann, C. Effects of Acute Resistance Exercise with and without Whole-Body Electromyostimulation and Endurance Exercise on the Postprandial Glucose Regulation in Patients with Type 2 Diabetes Mellitus: A Randomized Crossover Study. Nutrients 2021, 13, 4322. [Google Scholar] [CrossRef] [PubMed]
- Van Dijk, J.-W.; Manders, R.J.F.; Tummers, K.; Bonomi, A.G.; Stehouwer, C.D.A.; Hartgens, F.; Van Loon, L.J.C. Both Resistance- and Endurance-Type Exercise Reduce the Prevalence of Hyperglycaemia in Individuals with Impaired Glucose Tolerance and in Insulin-Treated and Non-Insulin-Treated Type 2 Diabetic Patients. Diabetologia 2012, 55, 1273–1282. [Google Scholar] [CrossRef] [PubMed]
- Borror, A.; Zieff, G.; Battaglini, C.; Stoner, L. The Effects of Postprandial Exercise on Glucose Control in Individuals with Type 2 Diabetes: A Systematic Review. Sports Med. 2018, 48, 1479–1491. [Google Scholar] [CrossRef] [PubMed]
- Yardley, J.E.; Kenny, G.P.; Perkins, B.A.; Riddell, M.C.; Malcolm, J.; Boulay, P.; Khandwala, F.; Sigal, R.J. Effects of Performing Resistance Exercise Before Versus After Aerobic Exercise on Glycemia in Type 1 Diabetes. Diabetes Care 2012, 35, 669–675. [Google Scholar] [CrossRef] [PubMed]
- Yardley, J.E.; Sigal, R.J.; Riddell, M.C.; Perkins, B.A.; Kenny, G.P. Performing Resistance Exercise before versus after Aerobic Exercise Influences Growth Hormone Secretion in Type 1 Diabetes. Appl. Physiol. Nutr. Metab. 2014, 39, 262–265. [Google Scholar] [CrossRef]
- Pettit-Mee, R.J.; Ready, S.T.; Padilla, J.; Kanaley, J.A. Leg Fidgeting During Prolonged Sitting Improves Postprandial Glycemic Control in People with Obesity. Obesity 2021, 29, 1146–1154. [Google Scholar] [CrossRef]
- Morishima, T.; Restaino, R.M.; Walsh, L.K.; Kanaley, J.A.; Fadel, P.J.; Padilla, J. Prolonged Sitting-Induced Leg Endothelial Dysfunction Is Prevented by Fidgeting. Am. J. Physiol. Heart Circ. Physiol. 2016, 311, H177–H182. [Google Scholar] [CrossRef] [PubMed]
- Hamilton, M.T.; Hamilton, D.G.; Zderic, T.W. A Potent Physiological Method to Magnify and Sustain Soleus Oxidative Metabolism Improves Glucose and Lipid Regulation. iScience 2022, 25, 104869. [Google Scholar] [CrossRef]
- Nakayama, Y.; Ono, K.; Okagawa, J.; Urabe, J.; Yamau, R.; Ishikawa, A. Home-Based High-Intensity Interval Exercise Improves the Postprandial Glucose Response in Young Adults with Postprandial Hyperglycemia. Int. J. Environ. Res. Public Health 2022, 19, 4227. [Google Scholar] [CrossRef]
- Holst, J.J.; Gribble, F.; Horowitz, M.; Rayner, C.K. Roles of the Gut in Glucose Homeostasis. Diabetes Care 2016, 39, 884–892. [Google Scholar] [CrossRef] [PubMed]
- Schiavon, M.; Hinshaw, L.; Mallad, A.; Man, C.D.; Sparacino, G.; Johnson, M.; Carter, R.; Basu, R.; Kudva, Y.; Cobelli, C.; et al. Postprandial Glucose Fluxes and Insulin Sensitivity during Exercise: A Study in Healthy Individuals. Am. J. Physiol. Endocrinol. Metab. 2013, 305, E557–E566. [Google Scholar] [CrossRef] [PubMed]
- Reynolds, A.N.; Mann, J.I.; Williams, S.; Venn, B.J. Advice to Walk after Meals Is More Effective for Lowering Postprandial Glycaemia in Type 2 Diabetes Mellitus than Advice That Does Not Specify Timing: A Randomised Crossover Study. Diabetologia 2016, 59, 2572–2578. [Google Scholar] [CrossRef] [PubMed]
- Iida, Y.; Takeishi, S.; Fushimi, N.; Tanaka, K.; Mori, A.; Sato, Y. Effect of Postprandial Moderate-Intensity Walking for 15-Min on Glucose Homeostasis in Type 2 Diabetes Mellitus Patients. Diabetol. Int. 2020, 11, 383–387. [Google Scholar] [CrossRef] [PubMed]
- Oberlin, D.J.; Mikus, C.R.; Kearney, M.L.; Hinton, P.S.; Manrique, C.; Leidy, H.J.; Kanaley, J.A.; Rector, R.S.; Thyfault, J.P. One Bout of Exercise Alters Free-Living Postprandial Glycemia in Type 2 Diabetes. Med. Sci. Sports Exerc. 2014, 46, 232–238. [Google Scholar] [CrossRef] [PubMed]
- Colberg, S.R.; Grieco, C.R.; Somma, C.T. Exercise Effects on Postprandial Glycemia, Mood, and Sympathovagal Balance in Type 2 Diabetes. J. Am. Med. Dir. Assoc. 2014, 15, 261–266. [Google Scholar] [CrossRef]
- Erickson, M.L.; Little, J.P.; Gay, J.L.; McCully, K.K.; Jenkins, N.T. Effects of Postmeal Exercise on Postprandial Glucose Excursions in People with Type 2 Diabetes Treated with Add-on Hypoglycemic Agents. Diabetes Res. Clin. Pract. 2017, 126, 240–247. [Google Scholar] [CrossRef]
- Høstmark, A.T.; Ekeland, G.S.; Beckstrøm, A.C.; Meen, H.D. Postprandial Light Physical Activity Blunts the Blood Glucose Increase. Prev. Med. 2006, 42, 369–371. [Google Scholar] [CrossRef] [PubMed]
- Lunde, M.S.H.; Hjellset, V.T.; Høstmark, A.T. Slow Post Meal Walking Reduces the Blood Glucose Response: An Exploratory Study in Female Pakistani Immigrants. J. Immigr. Minor. Health 2012, 14, 816–822. [Google Scholar] [CrossRef]
- Nygaard, H.; Tomten, S.E.; Høstmark, A.T. Slow Postmeal Walking Reduces Postprandial Glycemia in Middle-Aged Women. Appl. Physiol. Nutr. Metab. 2009, 34, 1087–1092. [Google Scholar] [CrossRef]
- Francois, M.E.; Little, J.P. The Impact of Acute High-Intensity Interval Exercise on Biomarkers of Cardiovascular Health in Type 2 Diabetes. Eur. J. Appl. Physiol. 2017, 117, 1607–1616. [Google Scholar] [CrossRef] [PubMed]
- Blankenship, J.M.; Chipkin, S.R.; Freedson, P.S.; Staudenmayer, J.; Lyden, K.; Braun, B. Managing Free-Living Hyperglycemia with Exercise or Interrupted Sitting in Type 2 Diabetes. J. Appl. Physiol. 2019, 126, 616–625. [Google Scholar] [CrossRef] [PubMed]
- Jung, M.E.; Bourne, J.E.; Little, J.P. Where Does HIT Fit? An Examination of the Affective Response to High-Intensity Intervals in Comparison to Continuous Moderate- and Continuous Vigorous-Intensity Exercise in the Exercise Intensity-Affect Continuum. PLoS ONE 2014, 9, e114541. [Google Scholar] [CrossRef] [PubMed]
- Gillen, J.B.; Little, J.P.; Punthakee, Z.; Tarnopolsky, M.A.; Riddell, M.C.; Gibala, M.J. Acute High-intensity Interval Exercise Reduces the Postprandial Glucose Response and Prevalence of Hyperglycaemia in Patients with Type 2 Diabetes. Diabetes Obes. Metab. 2012, 14, 575–577. [Google Scholar] [CrossRef] [PubMed]
- Little, J.P.; Jung, M.E.; Wright, A.E.; Wright, W.; Manders, R.J.F. Effects of High-Intensity Interval Exercise versus Continuous Moderate-Intensity Exercise on Postprandial Glycemic Control Assessed by Continuous Glucose Monitoring in Obese Adults. Appl. Physiol. Nutr. Metab. 2014, 39, 835–841. [Google Scholar] [CrossRef] [PubMed]
- Parker, L.; Shaw, C.S.; Banting, L.; Levinger, I.; Hill, K.M.; McAinch, A.J.; Stepto, N.K. Acute Low-Volume High-Intensity Interval Exercise and Continuous Moderate-Intensity Exercise Elicit a Similar Improvement in 24-h Glycemic Control in Overweight and Obese Adults. Front. Physiol. 2017, 7, 661. [Google Scholar] [CrossRef] [PubMed]
- Achten, J.; Jeukendrup, A.E. Effects of Pre-Exercise Ingestion of Carbohydrate on Glycaemic and Insulinaemic Responses during Subsequent Exercise at Differing Intensities. Eur. J. Appl. Physiol. 2003, 88, 466–471. [Google Scholar] [CrossRef] [PubMed]
- DiPietro, L.; Gribok, A.; Stevens, M.S.; Hamm, L.F.; Rumpler, W. Three 15-Min Bouts of Moderate Postmeal Walking Significantly Improves 24-h Glycemic Control in Older People at Risk for Impaired Glucose Tolerance. Diabetes Care 2013, 36, 3262–3268. [Google Scholar] [CrossRef] [PubMed]
- Shambrook, P.; Kingsley, M.I.; Taylor, N.F.; Wundersitz, D.W.; Wundersitz, C.E.; Paton, C.D.; Gordon, B.A. A Comparison of Acute Glycaemic Responses to Accumulated or Single Bout Walking Exercise in Apparently Healthy, Insufficiently Active Adults. J. Sci. Med. Sport 2020, 23, 902–907. [Google Scholar] [CrossRef]
- Wheeler, M.J.; Green, D.J.; Cerin, E.; Ellis, K.A.; Heinonen, I.; Lewis, J.; Naylor, L.H.; Cohen, N.; Larsen, R.; Dempsey, P.C.; et al. Combined Effects of Continuous Exercise and Intermittent Active Interruptions to Prolonged Sitting on Postprandial Glucose, Insulin, and Triglycerides in Adults with Obesity: A Randomized Crossover Trial. Int. J. Behav. Nutr. Phys. Act. 2020, 17, 152. [Google Scholar] [CrossRef]
- Kowalsky, R.J.; Jakicic, J.M.; Hergenroeder, A.; Rogers, R.J.; Gibbs, B.B. Acute Cardiometabolic Effects of Interrupting Sitting with Resistance Exercise Breaks. Appl. Physiol. Nutr. Metab. 2019, 44, 1025–1032. [Google Scholar] [CrossRef] [PubMed]
- Homer, A.R.; Taylor, F.C.; Dempsey, P.C.; Wheeler, M.J.; Sethi, P.; Townsend, M.K.; Grace, M.S.; Green, D.J.; Cohen, N.D.; Larsen, R.N.; et al. Frequency of Interruptions to Sitting Time: Benefits for Postprandial Metabolism in Type 2 Diabetes. Diabetes Care 2021, 44, 1254–1263. [Google Scholar] [CrossRef]
- Climie, R.E.; Grace, M.S.; Larsen, R.L.; Dempsey, P.C.; Oberoi, J.; Cohen, N.D.; Owen, N.; Kingwell, B.A.; Dunstan, D.W. Regular Brief Interruptions to Sitting after a High-Energy Evening Meal Attenuate Glycemic Excursions in Overweight/Obese Adults. Nutr. Metab. Cardiovasc. Dis. 2018, 28, 909–916. [Google Scholar] [CrossRef] [PubMed]
- Dempsey, P.C.; Larsen, R.N.; Sethi, P.; Sacre, J.W.; Straznicky, N.E.; Cohen, N.D.; Cerin, E.; Lambert, G.W.; Owen, N.; Kingwell, B.A.; et al. Benefits for Type 2 Diabetes of Interrupting Prolonged Sitting with Brief Bouts of Light Walking or Simple Resistance Activities. Diabetes Care 2016, 39, 964–972. [Google Scholar] [CrossRef] [PubMed]
- Gillen, J.B.; Estafanos, S.; Williamson, E.; Hodson, N.; Malowany, J.M.; Kumbhare, D.; Moore, D.R. Interrupting Prolonged Sitting with Repeated Chair Stands or Short Walks Reduces Postprandial Insulinemia in Healthy Adults. J. Appl. Physiol. 2021, 130, 104–113. [Google Scholar] [CrossRef] [PubMed]
- Charlett, O.P.; Morari, V.; Bailey, D.P. Impaired Postprandial Glucose and No Improvement in Other Cardiometabolic Responses or Cognitive Function by Breaking up Sitting with Bodyweight Resistance Exercises: A Randomised Crossover Trial. J. Sports Sci. 2021, 39, 792–800. [Google Scholar] [CrossRef] [PubMed]
- Gale, J.T.; Wei, D.L.; Haszard, J.J.; Brown, R.C.; Taylor, R.W.; Peddie, M.C. Breaking Up Evening Sitting with Resistance Activity Improves Postprandial Glycemic Response: A Randomized Crossover Study. Med. Sci. Sports Exerc. 2023, 55, 1471–1480. [Google Scholar] [CrossRef] [PubMed]
- Engeroff, T.; Füzeki, E.; Vogt, L.; Banzer, W. The Acute Effects of Single or Repeated Bouts of Vigorous-Intensity Exercise on Insulin and Glucose Metabolism during Postprandial Sedentary Behavior. Int. J. Environ. Res. Public Health 2022, 19, 4422. [Google Scholar] [CrossRef]
- McCarthy, M.; Edwardson, C.L.; Davies, M.J.; Henson, J.; Rowlands, A.; King, J.A.; Bodicoat, D.H.; Khunti, K.; Yates, T. Breaking up Sedentary Time with Seated Upper Body Activity Can Regulate Metabolic Health in Obese High-risk Adults: A Randomized Crossover Trial. Diabetes Obes. Metab. 2017, 19, 1732–1739. [Google Scholar] [CrossRef]
- Rafiei, H.; Omidian, K.; Myette-Côté, É.; Little, J.P. Metabolic Effect of Breaking Up Prolonged Sitting with Stair Climbing Exercise Snacks. Med. Sci. Sports Exerc. 2021, 53, 150–158. [Google Scholar] [CrossRef]
- Cho, M.J.; Bunsawat, K.; Kim, H.J.; Yoon, E.S.; Jae, S.Y. The Acute Effects of Interrupting Prolonged Sitting with Stair Climbing on Vascular and Metabolic Function after a High-Fat Meal. Eur. J. Appl. Physiol. 2020, 120, 829–839. [Google Scholar] [CrossRef]
- Stork, M.J.; Marcotte-Chénard, A.; Jung, M.E.; Little, J.P. Exercise in the Workplace: Examining the Receptivity of Practical and Time-Efficient Stair-Climbing “Exercise Snacks”. Appl. Physiol. Nutr. Metab. 2024, 49, 30–40. [Google Scholar] [CrossRef]
- Buffey, A.J.; Herring, M.P.; Langley, C.K.; Donnelly, A.E.; Carson, B.P. The Acute Effects of Interrupting Prolonged Sitting Time in Adults with Standing and Light-Intensity Walking on Biomarkers of Cardiometabolic Health in Adults: A Systematic Review and Meta-Analysis. Sports Med. 2022, 52, 1765–1787. [Google Scholar] [CrossRef] [PubMed]
- Bailey, D.P.; Broom, D.R.; Chrismas, B.C.R.; Taylor, L.; Flynn, E.; Hough, J. Breaking up Prolonged Sitting Time with Walking Does Not Affect Appetite or Gut Hormone Concentrations but Does Induce an Energy Deficit and Suppresses Postprandial Glycaemia in Sedentary Adults. Appl. Physiol. Nutr. Metab. 2016, 41, 324–331. [Google Scholar] [CrossRef]
- Dunstan, D.W.; Kingwell, B.A.; Larsen, R.; Healy, G.N.; Cerin, E.; Hamilton, M.T.; Shaw, J.E.; Bertovic, D.A.; Zimmet, P.Z.; Salmon, J.; et al. Breaking Up Prolonged Sitting Reduces Postprandial Glucose and Insulin Responses. Diabetes Care 2012, 35, 976–983. [Google Scholar] [CrossRef]
- Bhammar, D.M.; Sawyer, B.J.; Tucker, W.J.; Gaesser, G.A. Breaks in Sitting Time: Effects on Continuously Monitored Glucose and Blood Pressure. Med. Sci. Sports Exerc. 2017, 49, 2119–2130. [Google Scholar] [CrossRef]
- Hatamoto, Y.; Yoshimura, E.; Takae, R.; Komiyama, T.; Matsumoto, M.; Higaki, Y.; Tanaka, H. The Effects of Breaking Sedentary Time with Different Intensity Exercise Bouts on Energy Metabolism: A Randomized Cross-over Controlled Trial. Nutr. Metab. Cardiovasc. Dis. 2021, 31, 1879–1889. [Google Scholar] [CrossRef] [PubMed]
- Maylor, B.D.; Zakrzewski-Fruer, J.K.; Stensel, D.J.; Orton, C.J.; Bailey, D.P. Effects of Frequency and Duration of Interrupting Sitting on Cardiometabolic Risk Markers. Int. J. Sports Med. 2019, 40, 818–824. [Google Scholar] [CrossRef] [PubMed]
- Mackie, P.; Crowfoot, G.; Gyawali, P.; Janssen, H.; Holliday, E.; Dunstan, D.; English, C. Acute Effects of Frequent Light-Intensity Standing-Based Exercises That Interrupt 8 Hours of Prolonged Sitting on Postprandial Glucose in Stroke Survivors: A Dose-Escalation Trial. J. Phys. Act. Health 2021, 18, 644–652. [Google Scholar] [CrossRef]
- Paing, A.C.; McMillan, K.A.; Kirk, A.F.; Collier, A.; Hewitt, A.; Chastin, S.F.M. Dose-Response between Frequency of Breaks in Sedentary Time and Glucose Control in Type 2 Diabetes: A Proof of Concept Study. J. Sci. Med. Sport 2019, 22, 808–813. [Google Scholar] [CrossRef]
- Duran, A.T.; Friel, C.P.; Serafini, M.A.; Ensari, I.; Cheung, Y.K.; Diaz, K.M. Breaking Up Prolonged Sitting to Improve Cardiometabolic Risk: Dose–Response Analysis of a Randomized Crossover Trial. Med. Sci. Sports Exerc. 2023, 55, 847–855. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.-C.; Walhin, J.-P.; Hengist, A.; Gonzalez, J.T.; Betts, J.A.; Thompson, D. Interrupting Prolonged Sitting with Intermittent Walking Increases Postprandial Gut Hormone Responses. Med. Sci. Sports Exerc. 2022, 54, 1183–1189. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Reference | Population | Meal | Exercise Protocols * | Post-Meal Glucose Response |
|---|---|---|---|---|
| Bellini et al. (2021) [23] a | 27 H in two of six studies (Study 1: 14, 8 M and 6 F, 25 ± 2 years old; Study 4: 13, 8 M and 5 F, 23 ± 1 yrs) | MM: ~75% CHO of total EI (1 g of CHO per kg of BW). | Study 1: Ti: 30 min vs. 60 min vs. 90 min after the meal T: A (walking) D: 60 min I: 120 spm Study 4: Ti: 45 min pre-meal vs. 15 vs. 30 min after the meal T: A (walking) D: 30 min I: 120 spm | Study 1: ↓ with all timings. Study 4: ↓ with 15 and 30 min post-meal, greater effects at 15 min. |
| Heden et al. (2015) [27] a | 13 T2D (5 M and 8 F, 48.5 ± 11.9 years old) | Three MMs: ~50% CHO. | Ti: 20–30 min before vs. 45 min after the meal T: R D: 3 × 10 reps I: 10 RM | ↓ with pre- and post-meal exercise. |
| Hatamoto et al. (2017) [30] a | 11 H (11 M, 23 ± 2 years old) | Three MMs: 113.8 ± 16.6 g (69 ± 3% of EI) CHO for B, 104.5 ± 0.1 g (57 ± 2% of EI) CHO for L and 131.6 ± 11.7 (58 ± 2% of EI) CHO for D. | Ti: 30 min before vs. after each meal T: A (jogging) D: 20 × 1 min with 30 s of rest (60 min in total) I: Individuals’ LT | ↓ with post-meal exercise, more than pre-meal. |
| Nygaard et al. (2017) [33] a | 12 IGT (8 M and 4 F, 65 ± 8 years old) | MM: 1 g of CHO per kg of BW (74 ± 9 g) for B, 52 ± 19 g CHO for L, 51 ± 17 g CHO for D, and 59 ± 33 g CHO for the evening meal. | Ti: 1.5 h before vs. 30 min after B T: A (walking) D: 60 min I: 8% treadmill inclination, individual speed (12 on Borg’s RPE scale) | ↓ with post-meal exercise. |
| Solomon et al. (2020) [34] a | 48 H (Group 1: 16, 11 M and 5 F, 31 ± 11 years old; Group 2: 16, 5 M and 11 F, 24 ± 7 years old; Group 3: 9 M and 7 F, 29 ± 12 years old) | MM: 57% CHO of EI (71 g). | Ti: Immediately before vs. after the end of the meal vs. 30 min after the end of the meal T: Standing (Group 1) vs. walking (Group 2) vs. R (Group 3) D: 30 min (Groups 1 and 2) 3 × 10 repetitions (Group 3) I: Self-selected brisk pace (Group 2) and BW (Group 3) | ↓ with immediate post-meal exercise. |
| Colberg et al. (2009) [35] b | 12 T2D (6 M and 6 F, 61.4 ± 2.7 years old) | MM: 43–54 g CHO. | Ti: Immediately before vs. 15–20 min after the meal T: A (walking) D: 20 min I: Self-selected pace (moderate) | ↓ with post-meal exercise. |
| Yoko et al. (2021) [36] a | 11 H (5 M and 6 F, 42.7 ± 9.4 years old) | MM: 40 g of CHO. | Ti: 20 min before vs. 40 min after the meal. T: A (walking) vs. R D: 20 min I: 4–6 km/h (A) and BW (R) | ↓ with post-meal A. |
| Reynolds and Venn (2018) [37] a | 78 H (Group 1: 38, 6 M and 32 F, 21.4 ± 1.35 years old; Group 2: 40, 10 M and 30 F, 22.3 ± 5.16 years old) | MM: 50 g of CHO. | Ti: 15 min (Group 1) vs. 45 min (Group 2) after the meal T: A (cycling) D: 10 min I: 40 rpm, no resistance | ↓ with timing set at 45 min after the meal. |
| Zhang et al. (2021) [38] a | 20 H (20 M, 23.0 ± 4.26 years old) | MM: 73% CHO of EI (1 g of CHO per kg of BW). | Ti: At the individuals’ glucose peak vs. 20 min before the individuals’ glucose peak T: A (walking) D: 30 min I: 50% VO2max | ↓ with both timings, greater effects before the peak. |
| Huang et al. (2018) [40] a | 26 T2D (12 M and 14 F, 53.8 ± 8.6 years old) | Four MMs: 40–50% CHO of daily EI. B consisted of 30% of TDEI. | Ti: 30 min vs. 60 min vs. 90 min after B T: A (cycling) D: 6 × 1 min + 3 min of recovery (27 min in total) I: 85% Wmax (active phase) and 40% Wmax (recovery) | ↓ with all timings, greater effects at 30 min. |
| Chang et al. (2023) [47] a | 35 T2D (Group 1: 19, 10 M and 9 F, 65.9 ± 6.1 years old; Group 2: 16, 8 M and 8 F, 62.3 ± 7.4 years old) | Normal dietary habits. | Ti: 30 min before (Group 1) vs. 90 min after (Group 2) the individuals’ glucose peak T: A (self-selected) D: 22 min/day for 2 weeks I: Self-selected (moderate) | No changes with both timings. |
| Haxhi et al. (2016) [49] a | 9 T2D (9 M, 58.2 ± 6.6 years old) | MM: 55–60% of CHO of EI. | Ti: 40 min after vs. immediately before (1st bout) and 40 min after (2nd bout) the beginning of the meal T: A (walking) D: 40 min vs. 2 × 20 min I: 50% HRR | ↓ with split (2 × 20 min bouts) exercise. |
| Sacchetti et al. (2021) [50] a | 9 H (9 M, 29 ± 3 years old) | MM: 55–60% of CHO of EI. | Ti: 40 min after vs. 30 min before (1st bout) and 40 min after (2nd bout) the beginning of the meal T: A (cycling) D: 40 min vs. 2 × 20 min I: 65% VO2max | ↓ with both exercise strategies. |
| Reference | Population | Meal | Exercise Protocols * | Main Findings |
|---|---|---|---|---|
| Bellini et al. (2021) [23] a | 20 H in two of six studies (Study 2: 10, 5 M and 5 F, 24 ± 3 years old; Study 3: 10, 4 M and 6 F, 24 ± 6 years old) | MM: ~75% CHO of total EI (1 g of CHO per kg of BW). | Study 2: T: A (walking) vs. R vs. AR Ti: 30 min after the meal D: 30 min I: 120 spm and BW or elastic bands Study 3: T: A (walking vs. cycling vs. elliptical exercise) Ti: 30 min after the meal D: 30 min I: 70% HRmax | ↓ with A, R and AR (Study 2) and different A types (Study 3). |
| Bellini et al. (2021) [24] a | 8 T2D (3 M and 5 F, 62.6 ± 9.4 years old) | MM: 66% CHO of EI. | T: A vs. AR vs. RA vs. R Ti: 30 min after the meal D: 30 min (A, AR and RA) or 15 min (R) I: 100 spm (A bouts) and BW or elastic bands (R bouts) | ↓ with all types, greater effects of A and AR. |
| Bellini et al. (2023) [32] a | 23 H (Study 1: 12, 5 M and 7 F, 24 ± 3 years old; Study 2: 11, 9 M and 2 F, 27 ± 4 years old) | MM with 1 g of CHO per kg of BW (Study 1: 69.56 ± 14.97 g, 79.48 ± 4.00% of EI; Study 2: 69.64 ± 9.80 g, 74.51 ± 5.16% of EI). | Study 1: T: Walking vs. stepping vs. isometric wall squat Ti: 15 min after the meal D: 30 min I: 120 spm (walking and stepping) or BW (isometric wall squat) Study 2: T: Walking vs. passive NMES vs NMES + voluntary contraction Ti: 15 min after the meal D: 30 min I: 120 spm (Walking) or 30 Hz (NMES) | Study 1: ↓ with stepping and walking. Study 2: ↓ with walking and NMES with voluntary contraction. |
| Solomon et al. (2020) [34] a | 48 H (Group 1: 16, 11 M and 5 F, 31 ± 11 years old; Group 2: 16, 5 M and 11 F, 24 ± 7 years old; Group 3: 9 M and 7 F, 29 ± 12 years old) | MM: 57% CHO of EI (71 g). | T: Standing (Group 1) vs. walking (Group 2) vs. R (Group 3) Ti: Immediately before vs. after the end of the meal vs. 30 min after the end of the meal D: 30 min (Groups 1 and 2) 3 × 10 repetitions (Group 3) I: Self-selected brisk pace (Group 2) and BW (Group 3) | ↓ with all exercise types. |
| Yoko et al. (2021) [36] a | 11 H (5 M and 6 F, 42.7 ± 9.4 years old) | MM: 40 g of CHO. | T: A (walking) vs. R Ti: 20 min before vs. 40 min after the meal. D: 20 min I: 4–6 km/h (A) and BW (R) | ↓ with A. |
| Takaishi and Hayashi (2017) [66] a | 7 IGT and 7 T2D (9 M and 5 F, 60.9 ± 11.2 years old) | MM: 106.5 g of CHO. | T: SCD vs. A (cycling) Ti: 90 min after the meal D: 8–10 reps of 21 steps (SCD) and 5–7 min (cycling) I: 60–65% HRR and 12–13 on Borg’s RPE scale | ↓ with both, greater effects with SCD. |
| Holzer et al. (2021) [72] a | 6 T2D (3 M and 3 F, 55.2 ± 7.5 years old) | M: 61.5 g of CHO for B and 77.5 g of CHO for L. | T: R vs. R + NMES vs. A (cycling) Ti: 50 min after the meal D: 20 min (1 × 10–20 reps for 8 exercises for R) I: BW or elastic bands (R), 80 Hz and 4–5 on a 10-points muscle contraction scale (R + NMES) and 50% Wmax | ↓ with all exercise types. |
| Nakayama et al. (2022) [80] a | 12 H (12 M, 24.3 ± 2.3 years old) | MM: 71 g (70.5% of EI) CHO. | T: R HIIE vs. A (running) Ti: 30 min after the meal D: 11 min and 30 min I: BW and 50% VO2max | ↓ with both exercise types. |
| Reference | Population | Meal | Exercise Protocols * | Main Findings |
|---|---|---|---|---|
| Bellini et al. (2021) [23] a | 12 H in Study 5 (6 M and 6 F, 24 ± 2 years old) | MM: ~75% CHO of total EI (1 g of CHO per kg of BW). | D: 30 min vs. 45 min Ti: 15 min after the meal T: A (walking) I: 120 spm | ↓ with all durations. |
| Van Dijk et al. (2012) [59] b | 30 T2D (30 M, 60 ± 1 years old) | Three MMs and three snacks: 55% CHO of TDEI. | D: 60 min vs. 30 min (day 1) + 30 min (day 2) Ti: 1.5 h after B T: A (cycling) I: 50% Wmax | ↓ on day 1 with 60 min. |
| Bartholomae et al. (2019) [63] a | 34 H (20 M and 14 F, 26.8 ± 6.0 years old and 24.8 ± 4.5 years old, respectively) | OGTT (75 g of dextrose). | D: 1 min vs. 3 min vs. 10 min Ti: 18 min, 25 min or 27 min after the OGTT T: SCD I: 90–110 spm | ↓ with 10 min SCD in both sexes. |
| Moore et al. (2020) [65] | 30 H (12 M and 18 F, 23.7 ± 3.0 years old) | MM: 53% CHO of EI | D: 1 min vs. 3 min vs. 10 min Ti: 27 min 25 min and 18 min after the meal T: SCD I: Self-selected pace | ↓ with all durations. Greater effects with 3 min and 10 min bouts. |
| Lunde et al. (2012) [89] a | 11 H (of which 5 with IGT) (11 F, 44 ± 9.3 years old) | MM: 50 g of CHO. | D: 20 min vs. 40 min Ti: 20 min after the meal T: A (walking) I: Individuals’ speed (slow pace) | ↓ with both durations. |
| Nygaard et al. (2009) [90] | 13 H (13 F, >50 years old) | MM: 1 g of CHO per kg of BW. | D: 15 min vs. 40 min Ti: 15 min after the meal T: A (walking) I: 9 on Borg’s RPE scale | ↓ with both durations. |
| Blankenship et al. (2019) [92] a | 30 T2D (14 M and 16 F, 64 ± 8.2 years old) | Three isocaloric MMs: 55.4 ± 6.0% CHO of EI per meal. | D: 20 min vs. 40 min vs. 60 min Ti: 30–60 min after B T: A (walking) I: Individuals’ speed (brisk walking) | ↓ with all durations on post-B glucose response. |
| Reference | Population | Meal | Exercise Protocols * | Main Findings |
|---|---|---|---|---|
| Aadland and Høstmark (2008) [60] a | 9 H (6 M and 3 F, 37.3 ± 12.2 years old) | MM: 1 g of CHO per kg of BW. | I: 9 on Borg’s RPE scale (very light intensity) vs. 11 on Borg’s RPE scale (light intensity) Ti: Immediately after the meal T: A (cycling) D: 30 min | ↓ with both intensities. |
| Shambrook et al. (2018) [62] a | 10 H (10 M, 37.3 ± 7.3 years old) | MM: 51 ± 12% CHO of EI. | I: 35 ± 7% VO2R vs. 48 ± 8% VO2R vs. 10 × 1 min at 80% VO2R with 2 min of active recovery at 31 ± 12% VO2R Ti: 30 min after the meal T: A (cycling) D: 30 min in total | ↓ with all intensities. |
| Moreira et al. (2012) [69] a | 10 H (10 M, 50.8 ± 12.0 years old) and 9 T2D (9 M, 47.2 ± 12.4 years old) | MM: 45 g of CHO. | I: 23% 1 RM vs. 46% 1 RM Ti: 2 h after the meal T: R D: 25 min in total (3 × 30 reps or 3 × 16 reps) | ↓ with R in both populations. |
| Achten and Jeukendrup (2003) [97] b | 8 H (8 M, 26.4 ± 2.9 years old) | OGTT (75 g of glucose). | I: 40% vs. 65% vs. 80% Wmax Ti: 45 min after the OGTT T: A (cycling) D: 20 min | ↓ with all intensities. |
| Reference | Population | Meal | Exercise Protocols * | Main Findings |
|---|---|---|---|---|
| Bellini et al. (2021) [23] a | 14 H in Study 6 (7 M and 7 F, 23 ± 2 years old) | MM: ~75% CHO of total EI (1 g of CHO per kg of BW). | P: 2 × 15 min vs. 6 × 5 min vs. 12 × 2.5 min every 15 min of sitting T: A (walking) I: 120 spm | ↓ with 5 and 2.5 min bouts. |
| Francois et al. (2014) [29] a | 9 IGT and T2D (7 M and 2 F, 48 ± 6 years old) | Three MMs: 78 g CHO for B, 71 g CHO for L and 100 g CHO for D. | P: 6 × 1 min with 1 min of recovery 30 min before each meal vs. 30 min continuous performed 30 min before D T: A (walking) I: 90% of HRmax and 60% HRmax | ↓ with interval walking |
| Hatamoto et al. (2017) [30] a | 11 H (11 M, 23 ± 2 years old) | Three MMs: 113.8 ± 16.6 g (69 ± 3% of EI) CHO for B, 104.5 ± 0.1 g (57 ± 2% of EI) CHO for L and 131.6 ± 11.7 (58 ± 2% of EI) CHO for D. | P:20 × 1 min with 30 s of rest 30 min before or after each meal vs. 3 × 1 min performed every 30 min (20 times in total) T: A (jogging) I: Individuals’ LT | ↓ with brief periodic exercise bouts. |
| Pettit-Mee et al. (2021) [77] b | 20 Ob (5 M and 15 F, 42 ± 3 years old) | OGTT (75 g of glucose) | P: 2.5 min alternated with 2.5 min of resting for 3 h T: Leg fidgeting I: Individual cadence | ↓ with leg fidgeting. |
| Reynolds et al. (2016) [83] a | 41 T2D (26 M and 15 F, 60 ± 9.9 years old) | Habitual diet. | P: 30 min continuous vs. 3 × 10 min within 5 min after each meal T: A (walking) I: Not specified | ↓ with 10 min bouts before each meal. |
| Blankenship et al. (2019) [92] a | 30 T2D (14 M and 16 F, 64 ± 8.2 years old) | Three isocaloric MMs: 55.4 ± 6.0% CHO of EI per meal. | P: 20 min vs. 40 min vs. 60 min or 4 × 1.6 min, 3.3 min or 5 min every 30 min after each meal of the day (12 bouts in total). T: A (walking) I: Individuals’ speed (brisk walking) | ↓ with both continuous and activity breaks after B. |
| Shambrook et al. (2020) [99] a | 10 H (8 M and 2 F, 50 ± 12.6 years old) | Three MMs: 55.2 ± 18.5% CHO of EI. | P: 10 min after each meal vs. 30 min after D T: A (walking) I: 55–70% HRR | No differences in post-D glucose control with both sessions. |
| Wheeler et al. (2020) [100] a | 67 Ov and Ob (32 M and 35 F, 67 ± 7 years old) | Two MMs: 109.1 ± 17.3 g of CHO for B and 97.4 ± 19.7 g of CHO for L. | P: 30 min after B vs. 30 min after B + 3 min of every 30 min of sitting for 6.5 h T: A (walking) I: 65–75% HRmax, 3.2 km/h of speed | ↑ with both conditions. |
| Kowalsky et al. (2019) [101] a | 14 at risk of cardiometabolic diseases (2 M and 12 F, 53.4 ± 9.5 years old) | MM: 55% CHO of EI. | P: 2 × 15 reps every hour of sitting for 4 h T: R I: BW or elastic bands | ↓ with activity breaks. |
| Homer et al. (2021) [102] a | 23 T2D (13 M and 10 F, 62 ± 8 years old) | Three MMs: 55% CHO of total EI. | P: 3 min every 30 min of sitting vs. 6 min every 60 min of sitting for 8 h T: R I: BW | ↓ post-B and -L with 6 min bouts. ↓ post-L with 3 min bouts. |
| Climie et al. (2018) [103] a | 9 Ov and Ob (5 M and 4 F, 32 ± 3 years old) | MM: 53–55% CHO of daily EI. | P: 3 min every 20 min of sitting for 3.5 h T: R I: BW | ↓ with activity breaks. |
| Dempsey et al. (2016) [104] a | 24 T2D (14 M and 10 F, 62 ± 6 years old) | Three MMs: 55–58% CHO of EI. | P: 3 min every 30 min of sitting for 7 h T: A (walking) vs. R I: 3.2 km/h and BW | ↓ with both A and R. |
| Gillen et al. (2021) [105] a | 14 H (7 M and 5 F, 24 ± 5 years old) | Two MMs: 56 ± 12 g (55% of EI) of CHO for B and 84 ± 18 g (55% of EI) of CHO for L. | P: 2 min for A vs. 1 min for chair stands every 30 min of sitting for 7.5 h T: A (walking) vs. chair stands with calf raise I: 3.1 mph and BW | No effects on post-meal glycemia with both protocols. |
| Charlett et al. (2021) [106] a | 12 H (5 M and 7 F, 25 ± 6 years old) | Two MMs: 57% CHO of EI for B and 51% CHO of EI for L. | P: 3 min every 30 min of sitting for 5 h T: R I: BW | ↑ with activity breaks. |
| Gale et al. (2023) [107] a | 10 H-NW (4 M and 6 F, 23.5 ± 4.2 years old), 10 Ov (1 M and 9 F, 25.8 ± 5.8 years old) and 10 Ob (3 M and 7 F, 26.8 ± 5.8 years old) | Two MMs: 114.8 21.3 g (59% of EI) of CHO. | P: 3 min every 30 min of sitting for 4 h T: R I: BW | ↓ with activity breaks in all groups. Greatest reductions in H-NW. |
| Engeroff et al. (2022) [108] a | 18 H (18 F, 25.6 ± 2.6 years old) | Free-portion size MM: 51% CHO of EI. | P: 30 min continuous vs. sitting interrupted by 5 breaks of 6 min for 4 h T: A (cycling) I: 70% VO2max | No effect on post-meal glycemia. |
| McCarthy et al. (2017) [109] a | 13 Ob (6 M and 7 F, 66 ± 6 years old) | Two MMs: 51% CHO of EI. | P: 5 min every 30 min of sitting for 7.5 h T: A (arm ergometer) I: 15-35 W | ↓ with arm exercise. |
| Rafiei et al. (2021) [110] a | 12 H (Study 1: 12 M, 22.8 ± 4.3 years old) and 11 Ov and Ob (Study 2: 3 M and 8 F, 50.2 ± 14.3 years old) | Three MMs: 97 g of CHO. | P: In both studies: 8 × 15–30 s every hour for 9 h T: SCD I: Quickest pace possible | No effects on post-meal glycemia in both H and Ov and Ob. |
| Cho et al. (2020) [111] a | 12 H (7 M and 5 F, 23.5 ± 2.9 years old) | MM: 83 g of CHO. | P: 5 min every hour for 4 h T: SCD I: 66% HRR and 15 on Borg’s RPE scale | ↑ with SCD. |
| Bailey et al. (2016) [114] a | 13 H (6 M and 7 F, 26.6 ± 8.5 years old) | Mixed drink: 75 g of CHO. | P: 2 min every 20 min of sitting for 5 T: A (walking) I: 3.2 km/h vs. 5.8–6.4 km/h | ↓ with both protocols. Greater effects with moderate-intensity. |
| Dunstan et al. (2012) [115] a | 19 Ov and Ob (11 M and 8 F, 53.8 ± 4.9 years old) | Mixed drink: 75 g of CHO. | P: 14 × 2 min every 20 min of sitting for 5 h T: A (walking) I: 3.2 km/h vs. 5.8–7.9 km/h | ↓ with both intensities. |
| Bhammar et al. (2017) [116] a | 10 Ov and Ob (5 M and 5 F, 32 ± 5 years old) | Five MMs: 130 g (77% of EI) of CHO for B, 68 g (53% of EI) of CHO for L, 148 g (58% of EI) of CHO for D and 19 g of CHO for S. | P: 30 min continuous vs. 21 × 2 min every 20 min of sitting vs. 8 × 2 min every hour for 9 h T: A (walking) I: 65–75% HRmax (230 kcal of EE) vs. 3.0 mph (240 kcal of EE) vs. 79 ± 4% HRmax (140 kcal of EE) | ↓ with all protocols. |
| Hatamoto et al. (2021) [117] a | 9 Ov and Ob (9 M, 21.1 ± 0.9 years old) | Two MMs: 99 g (55% of EI) of CHO after B and 141 ± 17 g (55 ± 2% of EI) of CHO after L. | P: 2 min vs. 200 s vs. 75 s every 30 min of sitting for 8 h T: A (running) I: At LT vs. 60% LT vs. OBLA | ↓ with exercise at LT and OBLA intensities. |
| Maylor et al. (2019) [118] a | 14 H (14 F, 33.8 ± 13.4 years old) | Two MMs: 43.1 ± 8.1 g (58% of EI) of CHO for the 1st, 57.6 ± 10.0 g (46% of EI) of CHO for the second. In addition, an ad libitum meal was consumed. | P: 2 min every 30 min of sitting vs. 10 min every 170 min of sitting for 7.5 h T: A (walking) I: 65% VO2peak | No effects for both conditions on post-meal glycemia. |
| Paing et al. (2019) [120] a | 12 T2D (8 M and 4 F, 60 ± 11 years old) | Four MMs: 50–53.7 g of CHO for B, 75 g of CHO for L, 50.1–55.6 g of CHO for D and 10–13.1 g of CHO for S. | P: 3 min every 60 min, 30 min or 15 min of sitting for 7 h T: A (walking) I: 3.2 km/h | ↓ with higher activity breaks frequency (i.e., every 15 min). |
| Duran et al. (2023) [121] a | 9 H (5 M and 4 F, 57 ± 8.6 years old) | Two MMs: 55–58% CHO of EI. | P: 1 min vs. 5 min every 30 vs. 60 min of sitting for 8 h T: A (walking) I: 2 mph and 0% of treadmill slope | ↓ only with 5 min breaks every 30 min. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bellini, A.; Scotto di Palumbo, A.; Nicolò, A.; Bazzucchi, I.; Sacchetti, M. Exercise Prescription for Postprandial Glycemic Management. Nutrients 2024, 16, 1170. https://doi.org/10.3390/nu16081170
Bellini A, Scotto di Palumbo A, Nicolò A, Bazzucchi I, Sacchetti M. Exercise Prescription for Postprandial Glycemic Management. Nutrients. 2024; 16(8):1170. https://doi.org/10.3390/nu16081170
Chicago/Turabian StyleBellini, Alessio, Alessandro Scotto di Palumbo, Andrea Nicolò, Ilenia Bazzucchi, and Massimo Sacchetti. 2024. "Exercise Prescription for Postprandial Glycemic Management" Nutrients 16, no. 8: 1170. https://doi.org/10.3390/nu16081170
APA StyleBellini, A., Scotto di Palumbo, A., Nicolò, A., Bazzucchi, I., & Sacchetti, M. (2024). Exercise Prescription for Postprandial Glycemic Management. Nutrients, 16(8), 1170. https://doi.org/10.3390/nu16081170