Utility of Comprehensive Serum Glycopeptide Spectra Analysis (CSGSA) for the Detection of Early Stage Epithelial Ovarian Cancer

 ,
,  , , , and
, , , and
Abstract
:1. Introduction
2. Results and Discussion
3. Materials and Methods
3.1. Patient Samples
3.2. Preparation of Quality Control Serum, and Calculation of Inter- and Intra-Assay Coefficients of Variability
3.3. Sample Preparation for Glycoprotein Profiling
3.4. Liquid Chromatography and Mass Spectrometry
3.5. Data Processing
3.6. Pattern Recognition Analysis and Cross-Validation
3.7. Statistical Analysis
3.8. Study Approval
4. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Torre, L.A.; Bray, F.; Siegel, R.L.; Ferlay, J.; Jemal, A.; Lortet-Tieulent, J. Global cancer statistics, 2012. CA Cancer. J. Clin. 2012, 65, 87–108. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mandelbaum, R.S.; Adams, C.L.; Yoshihara, K.; Nusbaum, D.J.; Matsuzaki, S.; Matsushima, K.; Klar, M.; Paulson, R.J.; Roman, L.D.; Wright, J.D.; et al. Carcinoma of the ovaries and fallopian tubes. In Abeloff’s Clinical Oncology, 6th ed.; Elsevier: Philadelphia, PA, USA, 2019; pp. 1525–1543. [Google Scholar]
- Hayashi, M.; Matsuo, K.; Tanabe, K.; Ikeda, M.; Miyazawa, M.; Yasaka, M.; Machida, H.; Shida, M.; Imanishi, T.; Grubbs, B.H.; et al. Comprehensive serum glycopeptide spectra analysis (CSGSA): A potential new tool for early detection of ovarian cancer. Cancers 2019, 11, 591. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ueland, F.R.; DeSimone, C.P.; Seamon, L.G.; Miller, R.A.; Goodrich, S.; Podzielinski, I.; Sokoll, L.; Smith, A.; Van Nagell, J.R.; Zhang, Z. Effectiveness of a multivariate index assay in the preoperative assessment of ovarian tumors. Obstet. Gynecol. 2011, 117, 1289–1297. [Google Scholar] [CrossRef] [PubMed]
- Matsuo, K.; Huang, Y.; Matsuzaki, S.; Klar, M.; Roman, L.D.; Sood, A.K.; Wright, J.D. Minimally Invasive Surgery and Risk of Capsule Rupture for Women with Early-Stage Ovarian Cancer. JAMA Oncol. 2020, 6, 1110. [Google Scholar] [CrossRef] [PubMed]
- Mikami, M.; Tanabe, K.; Matsuo, K.; Miyazaki, Y.; Miyazawa, M.; Hayashi, M.; Asai, S.; Ikeda, M.; Shida, M.; Hirasawa, T.; et al. Fully-sialylated alpha-chain of complement 4-binding protein: Diagnostic utility for ovarian clear cell carcinoma. Gynecol. Oncol. 2015, 139, 520–528. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Matsuo, K.; Tanabe, K.; Ikeda, M.; Shibata, T.; Kajiwara, H.; Miyazawa, M.; Miyazawa, M.; Hayashi, M.; Shida, M.; Hirasawa, T.; et al. Fully sialylated alpha-chain of complement 4-binding protein (A2160): A novel prognostic marker for epithelial ovarian carcinoma. Arch. Gynecol. Obstet. 2018, 297, 749–756. [Google Scholar] [CrossRef] [PubMed]
- Tanabe, K.; Kitagawa, K.; Kojima, N.; Iijima, S. Multifucosylated alpha-1-acid glycoprotein as a novel marker for hepatocellular carcinoma. J. Proteome Res. 2016, 15, 2935–2944. [Google Scholar] [CrossRef] [PubMed]
- Eriksson, L.; Antti, H.; Gottfries, J.; Holmes, E.; Johansson, E.; Lindgren, F.; Long, I.; Trygg, J.; Wold, S. Using chemometrics for navigating in the large data sets of genomics, proteomics, and metabonomics (gpm). Anal. Bioanal. Chem. 2004, 380, 419–429. [Google Scholar] [CrossRef] [PubMed]
- Worley, B.; Powers, R. PCA as a practical indicator of OPLS-DA model reliability. Curr. Metab. 2016, 4, 97–103. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bylesjö, M.; Rantalainen, M.; Cloarec, O.; Nicholson, J.K.; Holmes, E.; Trygg, J. OPLS discriminant analysis: Combining the strengths of PLS-DA and SIMCA classification. J. Chemom. 2006, 20, 341–351. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
| Diagnostic Model | Sensitivity | Specificity | PPV | NPV | Accuracy | AUC (95% CI) |
|---|---|---|---|---|---|---|
| Training set | ||||||
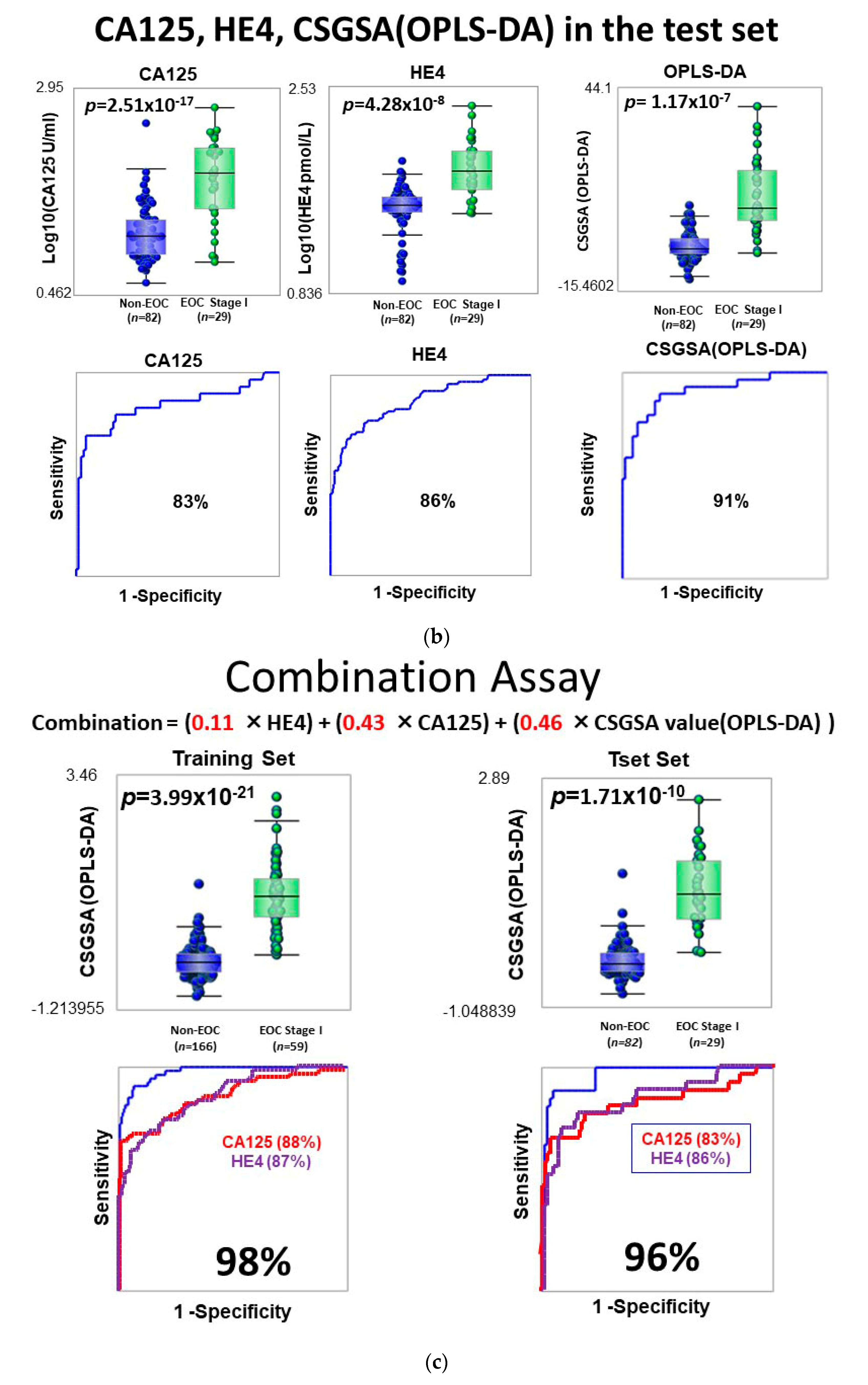
| CA125 | 78% | 81% | 55% | 91% | 78% | 88% (83–94) |
| HE4 | 76% | 80% | 59% | 89% | 80% | 87% (81–92) |
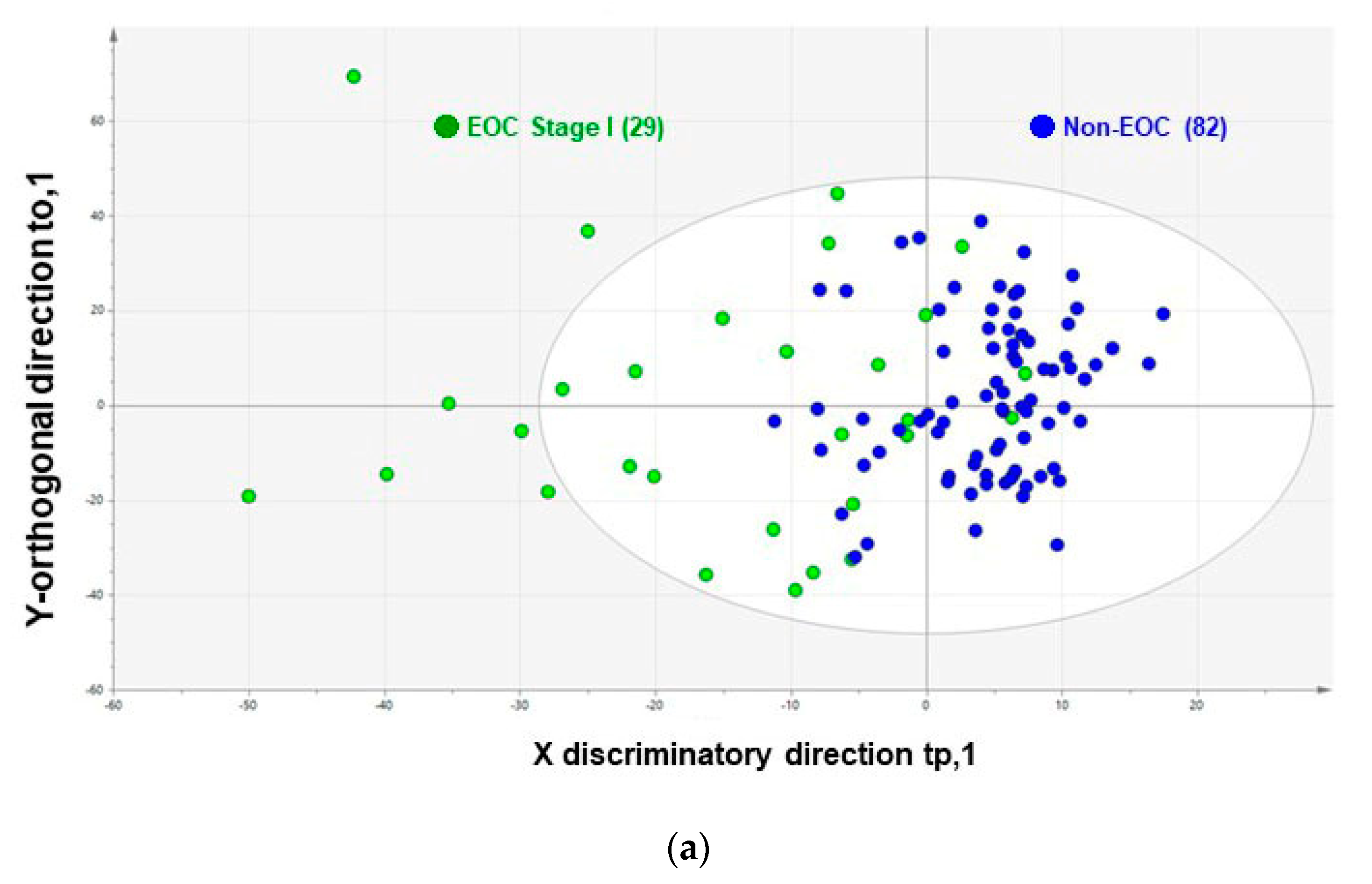
| CSGSA (OPLS-DA) | 90% | 86% | 70% | 96% | 87% | 93% (90–97) |
| Test set | ||||||
| CA125 | 79% | 80% | 59% | 92% | 80% | 83% (73–94) |
| HE4 | 79% | 85% | 66% | 92% | 84% | 86% (78–95) |
| CSGSA (OPLS-DA) | 86% | 84% | 66% | 95% | 85% | 91% (85–98) |
| Combination assay | ||||||
| CA125 + HE4 | 90% | 88% | 71% | 95% | 87% | 90% (82–99) |
| CSGSA (OPLS-DA) + CA125 | 90% | 91% | 78% | 95% | 90% | 95% (91–99) |
| CSGSA (OPLS-DA) + CA125 + HE4 | 90% | 93% | 81% | 96% | 92% | 96% (93–100) |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Matsuo, K.; Tanabe, K.; Hayashi, M.; Ikeda, M.; Yasaka, M.; Machida, H.; Shida, M.; Sato, K.; Yoshida, H.; Hirasawa, T.; et al. Utility of Comprehensive Serum Glycopeptide Spectra Analysis (CSGSA) for the Detection of Early Stage Epithelial Ovarian Cancer. Cancers 2020, 12, 2374. https://doi.org/10.3390/cancers12092374
Matsuo K, Tanabe K, Hayashi M, Ikeda M, Yasaka M, Machida H, Shida M, Sato K, Yoshida H, Hirasawa T, et al. Utility of Comprehensive Serum Glycopeptide Spectra Analysis (CSGSA) for the Detection of Early Stage Epithelial Ovarian Cancer. Cancers. 2020; 12(9):2374. https://doi.org/10.3390/cancers12092374
Chicago/Turabian StyleMatsuo, Koji, Kazuhiro Tanabe, Masaru Hayashi, Masae Ikeda, Miwa Yasaka, Hiroko Machida, Masako Shida, Kenji Sato, Hiroshi Yoshida, Takeshi Hirasawa, and et al. 2020. "Utility of Comprehensive Serum Glycopeptide Spectra Analysis (CSGSA) for the Detection of Early Stage Epithelial Ovarian Cancer" Cancers 12, no. 9: 2374. https://doi.org/10.3390/cancers12092374
APA StyleMatsuo, K., Tanabe, K., Hayashi, M., Ikeda, M., Yasaka, M., Machida, H., Shida, M., Sato, K., Yoshida, H., Hirasawa, T., Imanishi, T., & Mikami, M. (2020). Utility of Comprehensive Serum Glycopeptide Spectra Analysis (CSGSA) for the Detection of Early Stage Epithelial Ovarian Cancer. Cancers, 12(9), 2374. https://doi.org/10.3390/cancers12092374