Simple Summary
Primary liver transplantation (PLT) for HCC represents the ideal treatment. However, since organ shortage increases the risk of drop-out from the waiting list for tumor progression, a new surgical strategy has been developed: Salvage Liver Transplantation (SLT) can be offered as an additional curative strategy for HCC recurrence after liver resection. The aim of this updated meta-analysis is to compare surgical and long-term outcomes of SLT versus PLT for HCC. The findings of our analysis reveal that SLT offers comparable surgical outcomes but slightly poorer oncological long-term outcomes with respect to PLT.
Abstract
(1) Background: Primary liver transplantation (PLT) for HCC represents the ideal treatment. However, since organ shortage increases the risk of drop-out from the waiting list for tumor progression, a new surgical strategy has been developed: Salvage Liver Transplantation (SLT) can be offered as an additional curative strategy for HCC recurrence after liver resection. The aim of this updated meta-analysis is to compare surgical and long-term outcomes of SLT versus PLT for HCC. (2) Materials and Methods: A systematic review and meta-analysis was conducted using the published papers comparing SLT and PLT up to January 2022. (3) Results: 25 studies describing 11,275 patients met the inclusion criteria. The meta-analysis revealed no statistical difference in intraoperative blood loss, overall vascular complications, retransplantation rate, and hospital stay in the SLT group compared with the PLT group. However, the SLT group showed a slightly significant lower 5-year OS rate and 5-year disease-free survival rate. (4) Conclusion: meta-analysis advocates the relative safety and feasibility of both Salvage LT and Primary LT strategies. Specifically, SLT seems to have comparable surgical outcomes but slightly poorer long-term survival than PLT.
1. Introduction
Hepatocellular carcinoma (HCC) is a major contributor to the world’s cancer burden and is currently the third leading cause of cancer-related death, with incidences increasing continuously in recent years [1]. Locoregional treatments (mainly radiofrequency ablation and transarterial chemoembolization), liver resection (LR), and liver transplantation (LT) are well-defined and widely accepted treatments for hepatocellular carcinoma [2,3,4]. However, the best therapy for HCC is still an open and controversial oncological challenge. LT is considered the gold standard therapy for early HCC within liver cirrhosis since it radically removes the cancer and any dysplastic foci and it treats liver disease-related complications (e.g., portal hypertension) [5,6,7]. The oncological benefits of LT for HCC in terms of 5-year overall survival (OS) and 5-year disease-free survival (DFS) are well-documented: 75% and 90%, respectively [8]. However, organ shortage and the risk of drop-out from the waiting list for tumor progression and deterioration of liver function represent the main limitations for LT [9]. Nowadays, liver surgery for HCC has been demonstrated to be feasible and safe with very low postoperative morbidity and almost zero perioperative mortality [10,11]. Studies on minimally invasive liver surgery have also strongly confirmed these findings [12]. Therefore, primary LR for early HCC with preserved liver function and mild portal hypertension is considered the first-choice treatment [13,14]. Nevertheless, most published data showed a 5-year survival rate and a 5-year DSF after LR for HCC due to cancer relapses of 60% and 30%, respectively [15]. Salvage Liver Transplantation (SLT) is an alternative and promising curative strategy for HCC recurrence or deterioration of liver function after primary liver resection [16]. Moreover, some authors recently described “de principe” Salvage LT (pre-emptive transplantation before tumor recurrence) for a subgroup of patients who present poor histological features and aggressive biological tumor behavior on the final pathology of the resected specimen [17]. Previous studies comparing SLT with primary liver transplantation (PLT) have reported conflicting results in terms of surgical complication and risk of HCC recurrence [18,19,20,21]. However, with the advancement of surgical techniques, recent papers have shown SLT to be an effective and feasible treatment for patients with HCC recurrence after primary liver resection with a good long-term survival rate [22]. The purpose of this meta-analysis is to investigate the technical, postoperative, oncological and survival outcomes of PLT compared with SLT.
2. Materials and Methods
2.1. Study Design
Our meta-analysis was designed according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement [23], while the authors predetermined the eligibility criteria for the study. Two investigators (E.G. and G.G.P.) independently searched the literature. All retrospective clinical studies that compared Salvage LT with Primary LT for HCC were included in the present systematic review. No prospective studies have been published so far. Case reports, reviews, letters, and animal studies were excluded. All discrepancies during the data collection, synthesis, and analysis were resolved by the consensus of two authors (E.G. and G.G.).
2.2. Literature Search and Data Collection
We systematically searched the literature using the PubMed, MEDLINE, and Cochrane library databases for articles published up to January 2022; querying three databases maximizes the probability of capturing articles, as recently demonstrated by Goossen et al. [24]. Our search included the words “HCC”, “salvage liver transplantation”, “rescue liver transplantation”, and “salvage liver transplantation or liver transplantation and liver resection”. The search strategy was confined to English language papers and is described in Supplementary File S1 [23] and Supplementary File S2.
2.3. Quality Assessment
The quality of the included articles was estimated using the Methodological Index for Non-Randomized Studies (MINORS) [25].
2.4. Statistical Analysis
Meta-analysis was realized using the software Review Manager (RevMan) [Version 5.1. Copenhagen: The Nordic Cochrane Centre, The Cochrane Collaboration, 2011). Dichotomous outcomes are displayed as odds ratios (OR) with a 95% confidence interval (CI) by using the Mantel–Haenszel method and continuous variables are displayed as Mean difference (MD) with a 95% CI by utilizing the generic inverse variance method. Mean and standard deviation (SD) for continuous data, if not reported, were estimated using the method illustrated by Hozo et al. [26]. However, for continuous data provided as median and interquartile range (IQR), mean and SD were estimated by employing the method described by Luo et al. [27] and Wan et al. [28], respectively. The cut-off for statistical significance was set at p ≤ 0.05. Heterogeneities between the studies were evaluated using Q statistics and total variation was computed by I2. A random-effects model (REM) was always adopted due to the conceptual heterogeneity of clinical studies. Publication bias of the included papers is illustrated in Supplementary File S3.
3. Results
3.1. Studies and Patient Characteristics
Our search strategy disclosed 857 publications concerning Salvage LT. Twenty-nine full papers were examined; however, five studies were not included in the analysis because they did not meet the inclusion criteria. Finally, 25 articles and a total of 11,275 patients were included in the meta-analysis; 9645 patients were offered a Primary LT for HCC, whereas 1630 underwent Salvage LT for HCC recurrence or impaired liver function after primary liver resection. No randomized trials have been published so far. The flow diagram in Figure 1 shows the search process. The baseline characteristics of the two groups are presented in Table 1 and Table 2. Technical and postoperative outcomes and oncological and survival features are tabulated in Table 3. The two groups were similar as regards etiology, HBV, and/or HCV infection rates and maximum tumor diameter pre-LT and on post-LT pathology. The number of patients in each study ranged from a minimum of 42 to up to 6975. The MINORS scale assessed a low-quality heterogeneity between studies, providing a mean score of 21.8 (SD: 0.85) and a median score of 22 (range 20–23) (Table 1).
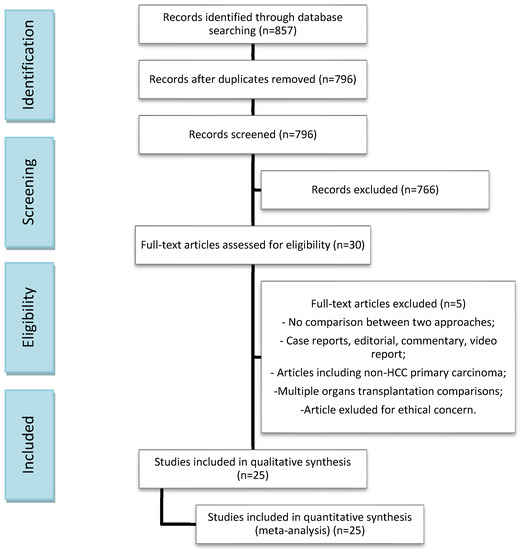
Figure 1.
Search flow diagram.

Table 1.
Summary of studies included in the Meta-analysis.
Table 2.
General and Patients characteristics.
Table 3.
Technical and postoperative outcomes; Oncological and survival outcomes.
3.2. Technical Outcomes
3.2.1. Duration of Surgery
The mean operating time was 600.44 min in the SLT group and 547.12 min in the PLT group; sixteen articles reported this item. Operating time was shorter in the Primary LT group, and the meta-analysis showed a statistically significant difference (MD 33.30, (95% CI 17.60, 49.00) p < 0.0001), as shown in Figure 2.
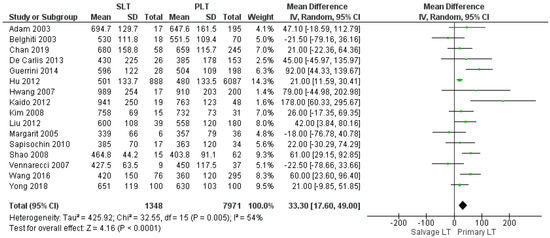
Figure 2.
Operating time.
3.2.2. Intraoperative Blood Loss, Intraoperative Red Blood Cell (RBC), and Fresh Frozen Plasma (FFP) Transfusion
The meta-analysis showed no statistically significant increased intraoperative blood loss in the Salvage LT group when compared with the Primary one (MD 290.35, (95% CI −82.63, 663.32) p = 0.13), as shown in Figure 3. The mean intraoperative blood loss in the SLT and PLT groups was 3174.55 cc and 2342.02 cc, respectively. The mean of intraoperative RBC and FFP transfusion was 7.8 RBC units and 9 FFP units in the Salvage LT group, and 6.5 RBC units and 8 FFP units in the Primary LT group. However, our analysis revealed no statistically significant differences between the two approaches: (MD 0.92, (95% CI −0.48, 2.32) p = 0.07) and (MD 0.34, (95% CI −0.69, 1.36) p = 0.52), respectively, as shown in Figure 4 and Figure 5.
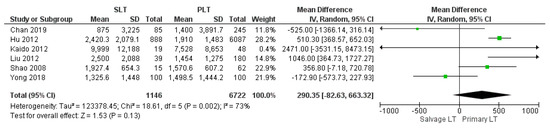
Figure 3.
Intraoperative blood loss.
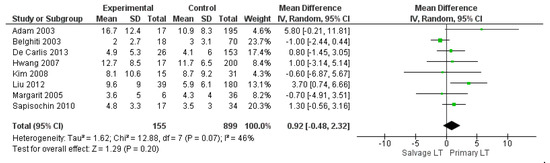
Figure 4.
Intraoperative Red Blood Cell (RBC) transfusion.
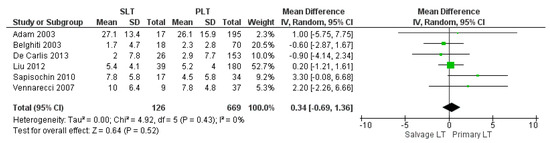
Figure 5.
Fresh frozen plasma (FFP) transfusion.
3.2.3. Reoperation Rate
Reoperation rate was 16.96% (48/283) in the SLT group and 9.45% (103/1090) in the PLT group. The meta-analysis showed a statistically significant difference in the rate of reoperation between the two groups, higher in the SLT than in the PLT group (OR 2.34, (95% CI 1.53, 3.59) p < 0.0001), as shown in Figure 6.
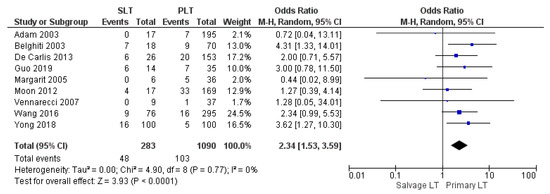
Figure 6.
Reoperation rate.
3.2.4. Perioperative Mortality Rate
Perioperative mortality rate was 6.31% (32/507) in the SLT group and 4.47% (100/2235) in the PLT group; slightly higher in the former group. The meta-analysis of the 18 trials showed a statistically significant difference in the rate of perioperative mortality between the two groups (OR 1.83, (95% CI 1.18, 2.84) p = 0.007), as shown in Figure 7.
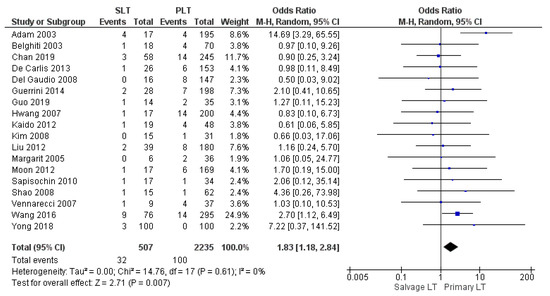
Figure 7.
Perioperative mortality rate.
3.2.5. Retransplantation Rate
Seven studies reported the retransplantation rate. The retransplantation rate was 6.11% (8/131) in the Salvage LT group and 7.22% (70/969) in the PLT sample. However, the different rates were not statistically significant between the two treatment strategies (OR 1.07, (95% CI 0.51, 2.24) p = 0.86), as shown in Figure 8.
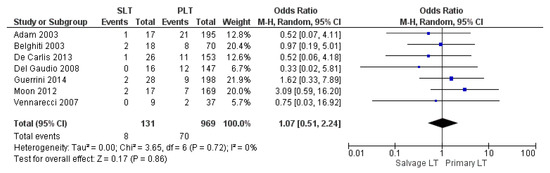
Figure 8.
Retransplantation rate.
3.3. Postoperative Outcomes
3.3.1. Postoperative Bleeding
Ten studies reported the postoperative bleeding rate. The Salvage LT group’s postoperative bleeding rate was considerably higher than the Primary LT group: 8.25% (88/1066) and 5.73% (411/7165), respectively. The difference in bleeding rates was statistically significant (OR 2.19, (95% CI 1.25, 3.81) p = 0.006), as shown in Figure 9.
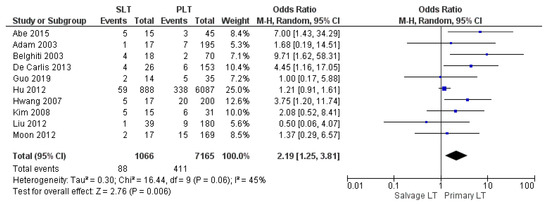
Figure 9.
Postoperative bleeding.
3.3.2. Intensive Care Unit Stay
The mean Intensive Care Unit (ICU) stay was 8.34 days in the SLT group and 5.44 days in the PLT group. No statistically significant mean difference was recorded (MD −0.12, (95% CI −0.88, 0.63) p = 0.75), although a higher mean ICU stay was displayed in the SLT group, as shown in Figure 10.
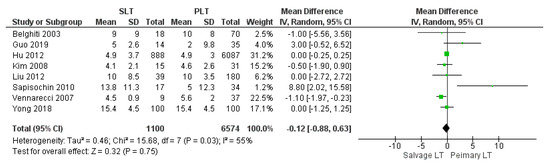
Figure 10.
Intensive care unit stay.
3.3.3. Length of Hospitalization
The mean hospital stay was 33.01 days in the SLT group and 26.44 in the PLT group; nine articles described this variable. The meta-analysis reported that the mean hospitalization was shorter in the PLT group than in the Salvage LT group, although this imbalance was not significant (MD 0.49, (95% CI −2.13, 3.11) p = 0.71), as shown in Figure 11.
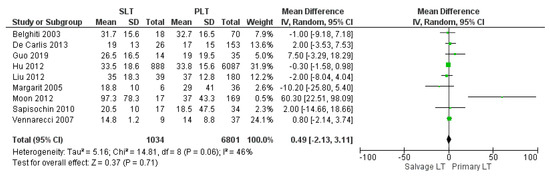
Figure 11.
Length of hospital stay.
3.3.4. Overall Vascular Complication
The rate of vascular complications was evaluated by 12 studies. The vascular complications rate was similar between SLT and PLT: 4.68% (55/1176) and 3.48% (258/7404), respectively. The meta-analysis revealed a statistically significant difference (OR 1.37, (95% CI 1.01, 1.86) p = 0.04), as shown in Figure 12.
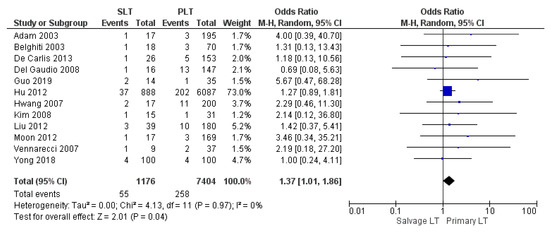
Figure 12.
Overall vascular complication.
3.3.5. Arterial Thrombosis
A total of 34 patients developed arterial thrombosis in twelve studies. The arterial thrombosis rate in the SLT group was higher than within the PLT group: 5.56% (12/216) and 2.78% (22/790), respectively. However, a statistically significant difference in these rates was not recognized between the two approaches (OR 1.87, (95% CI 0.87, 4.03) p = 0.11), as shown in Figure 13.
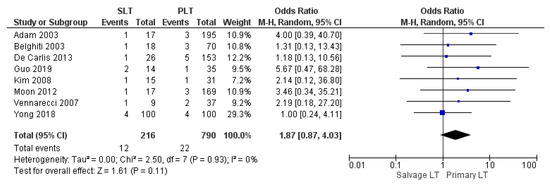
Figure 13.
Arterial thrombosis.
3.3.6. Biliary Complications
Thirteen papers analyzed the frequency of biliary complications (stenosis, leakage, and fistula). The biliary complication rate was significantly higher in the SLT group than the PLT group: 13.6% (162/1191) and 11.2% (838/7449), (OR 1.22, (95% CI 1.01, 1.47) p = 0.04), as shown in Figure 14.
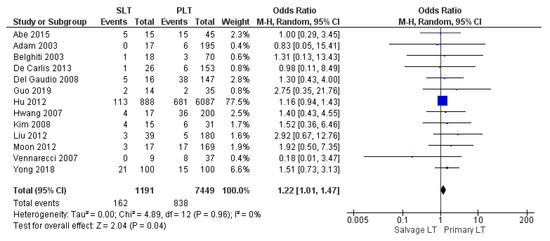
Figure 14.
Biliary complication.
3.3.7. Infection and Sepsis
Ten studies retrospectively assessed overall infection and sepsis rate. Infection rate of the SLT group was slightly higher than the PLT group: 28.2% (299/1059) and 25.5% (1826/7149), respectively. Nevertheless, the meta-analysis stated that the result was not significant (OR 1.14, (95% CI 0.98, 1.32) p = 0.08), as shown in Figure 15.
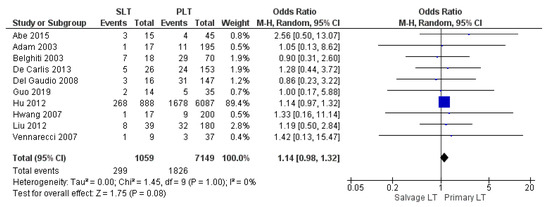
Figure 15.
Infection and sepsis.
3.4. Oncological and Survival Outcomes
3.4.1. Overall Survival Rates
Thirteen, fifteen, and twenty studies reported the 1-year, 3-year, and 5-year overall survival (OS) rate, respectively. Our meta-analysis revealed a similar 1-year OS rate of 77.9% (1072/1375) in the SLT group and 78.5% (6801/8666) in the PLT group, although this evidence was not statistically significant (OR 0.80, (95% CI 0.62, 1.03) p = 0.08), as shown in Figure 16. On the other hand, the meta-analysis showed a statistically significant difference in the 3-year and 5-year OS rates between the two groups with a slightly lower OS rate in the SLT group: SLT 59.3% (837/1410) and PLT 61.9% (5508/8905) (OR 0.72, (95% CI 0.60, 0.86) p = 0.0002), as shown in Figure 17; and SLT 53.9% (810/1503) and PLT 56.5% (5327/9424) (OR 0.68, (95% CI 0.56, 0.82) p < 0.0001), as shown in Figure 18, respectively.
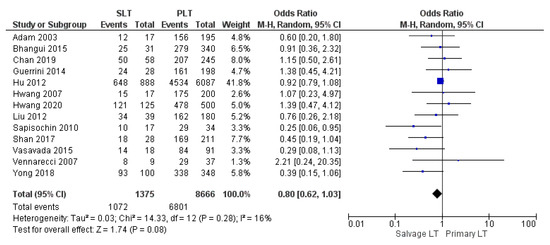
Figure 16.
1-year overall survival rates.
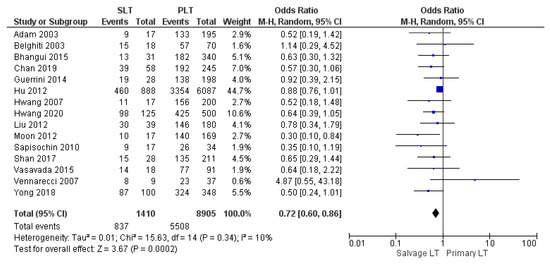
Figure 17.
3-year overall survival rates.
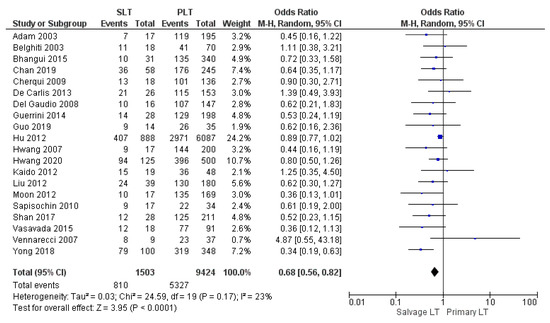
Figure 18.
5-year overall survival rates.
3.4.2. HCC Recurrence Rate
Types of HCC recurrence after LT were locoregional and/or systemic. Ten studies assessed tumor recurrence rate. Disease recurrence rate was 15.4% (37/240) in the SLT group and 10.9% (98/896) in the Primary LT group. The meta-analysis showed a statistically significant difference in the rate of disease recurrence between the two groups with a lower rate in the PLT group (OR 1.93, (95% CI 1.23, 3.04) p = 0.004), as shown in Figure 19.
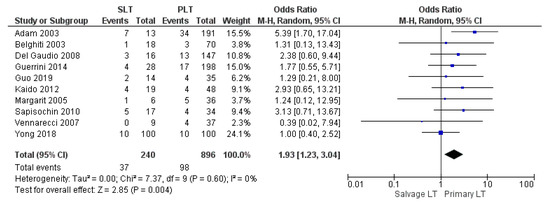
Figure 19.
HCC recurrence rate.
3.4.3. Disease-Free Survival Rates
Twelve, fourteen, and eighteen papers retrospectively assessed the 1-year, 3-year, and 5-year disease-free survival (DFS) rates, respectively. The meta-analysis showed statistically significant differences in the DFS rate of HCC between the two groups with the same 1-year DFS rate in the SLT group and PLT group, with 71.2% (967/1358) and 71.2% (5855/8218), respectively (OR 0.66, (95% CI 0.47, 0.92) p = 0.01), as shown in Figure 20. However, the 3-year and 5-year DFS rates were lower in the SLT group than the PLT group: SLT 54.8% (763/1393) and PLT 57% (4821/8457) (OR 0.59, (95% CI 0.44, 0.88) p = 0.007), as shown in Figure 21; and SLT 49.1% (721/1468) and PLT 51.3% (4538/8840), (OR 0.65, (95% CI 0.52, 0.82) p = 0.0002), as shown in Figure 22, respectively.
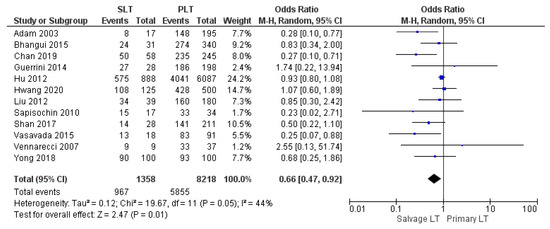
Figure 20.
1-year disease free survival rates.
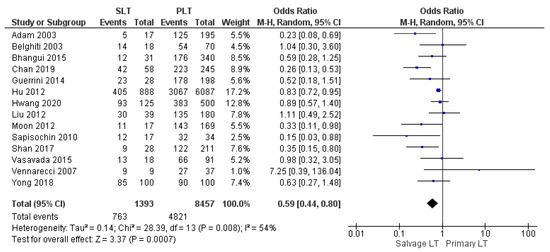
Figure 21.
3-year disease free survival rates.
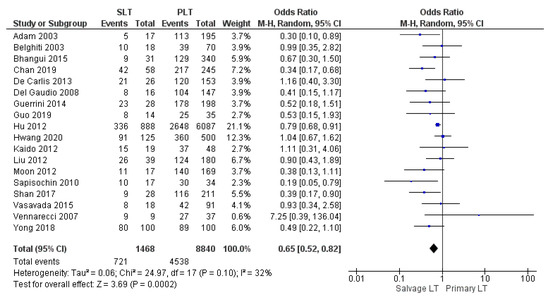
Figure 22.
5-year disease free survival rates.
4. Discussion
Liver transplantation (LT) represents the ideal treatment option for patients with HCC since it achieves radical tumor clearance and eradicates the underlying liver diseases. However, several patients on the waiting list for LT are faced with tumor progression, the loss of chance for transplantation, or even death due to severe organ shortage and long waiting list times [54]. Thus, in order to overcome the gap between the numbers of donors and recipients, salvage liver transplantation has been proposed in the last decade as an attractive and feasible strategy that combines liver resection and subsequent LT in the case of HCC recurrence [55,56,57,58,59].
This meta-analysis includes the highest number of articles comparing the findings of primary and salvage liver transplantation for HCC and also demonstrates completely new results compared to other studies on the same topic, bringing different and innovative concepts to the strategy of salvage transplantation for recurrence of HCC after liver resection [19].
Operating time and intraoperative blood loss are some of the surgical variables in terms of safety and feasibility most taken into consideration when Salvage LT is compared with Primary LT. Several studies reported a longer mean operating time for SLT than PLT. Although considerable differences exist in terms of duration of surgery and blood loss among the included articles, the duration of the operation and the extent of bleeding are necessarily affected by some technical and anatomical issues. SLT increases the difficulty of surgery due to severe adhesion in the abdominal operation area and due to abnormal anatomical structures as a consequence of previous hepatic resection [22,60]. Our meta-analysis revealed a significantly longer duration of surgery for SLT than Primary LT and also disclosed that intraoperative bleeding was slightly higher in the Salvage LT strategy, but this finding was not statistically significant. Moreover, differences between the two surgical approaches in terms of the mean need for intraoperative RBC and FFP transfusion were not statistically significant. Several papers showed that innovations in surgical techniques and accumulation of surgical experience have gradually decreased the risk of perioperative bleeding for SLT. It has been shown that reducing intraoperative bleeding and blood transfusions rate leads to a better postoperative recovery.
Our study showed that the reoperation rate was significantly higher in the SLT group than in the PLT group, and the perioperative mortality was slightly higher for the Salvage LT approach. Multiple preoperative bridging and downstaging treatments and the liver resection before salvage LT led to the formation of dense adhesions, portal collateral circulations due to hypertension, and coagulopathy [61,62,63]. Therefore, these factors increase bleeding after SLT, likely accounting for the higher re-exploration rate. Surgery for salvage liver transplantation is technically demanding, and this could explain the slightly higher perioperative mortality in patients undergoing Salvage rather than Primary LT.
In terms of intensive care unit stay and length of hospital stay, our data showed a longer recovery in the SLT group, although these findings were not statistically significant. On the other hand, overall vascular complication rate, overall infection, and sepsis rate were statistically similar between the two groups.
Several studies have found that the outcome of patients with HCC was similar between liver resection and liver transplantation [15,64,65,66]. Therefore, liver resection and LT are not opposing alternatives, but, rather, represent the components of a combined strategy for the management of HCC: liver resection can potentially improve the survival of patients listed for LT by decreasing the risk of dropout [67]. Moreover, minimally invasive liver resection (MILR) has a minor technical impact on a subsequent liver transplantation and seems to be associated with shorter operation time, reduced blood loss, and transfusion requirement during Salvage LT [68,69]. Therefore, MILR (laparoscopic or robotic) may become the gold standard for “early” HCC in patient cirrhosis and mild portal hypertension. In 2008, Felli et al. [70] introduced the concept of liver resection as a selection tool for LT. In fact, some pathological characteristics of the resected specimen can identify a subgroup of patients with favorable histological factors (small and well-differentiated HCC, without satellite nodules or microvascular invasion) who could avoid upfront LT because the risk of recurrence appears to be relatively low and if it should occur, then transplantation remains a salvage option at a later date [42,71,72,73]. On the other hand, patients showing negative prognostic histological features on the resected specimen (e.g., microvascular infiltration, high grade of differentiation) could undergo liver transplantation prior to tumor recurrence: so-called “de principe” SLT [17,74]. Indeed, the French allocation system recently integrated the SLT strategy within its algorithm, although no priority is given to patients at a high risk of HCC recurrence. These results and future research would clarify the role of the molecular and biological pattern of HCC in order to stratify patients with a high risk of recurrence and then arrive at defining the best personalized treatment [75].
A clear definition of “transplantability criteria in SLT”, that is, criteria that identify the group of patients who benefit most from transplantation for HCC recurrence after liver resection, has not yet been established [46,76]. Most authors agree that the criteria of patients with a limited recurrence within the Milan criteria is acceptable in order to achieve a good survival post-SLT [77]. Recently, Liu et al. observed the efficacy of SLT for patients with recurrent HCC after liver resection within the University of California San Francisco (UCSF) criteria, since in that study there was no significant difference in OS and DFS rates between the SLT and PLT groups [41].
Recurrence of HCC after transplantation is still a devastating event as no surgical or pharmacological therapy has shown significant prolongation of these patients’ survival [78,79,80,81]. Some authors have observed that the strategy of the salvage liver transplantation may increase the risk of recurrence of post-transplant patients, thus limiting their survival [51].
In our meta-analysis, the HCC recurrence rate was 15.4% in the SLT group and 10.9% in the PLT group. However, between the different studies taken into account by our meta-analysis, contrasting results can be observed with regard to tumor recurrence. Adam et al. [29]. reported that SLT had an increased risk of recurrence and poorer survival compared with primary transplantation. By contrast, in the same period, Belghiti et al. [30] showed that recurrence rate, operative mortality, and long-term survival were comparable between the two groups.
Important end points of this meta-analysis were overall survival (OS) rate and disease free-survival rate between SLT and PLT. Our meta-analysis showed statistically significant lower 1-, 3-, and 5-year DFS rates for SLT compared to PLT. However, DFS as a long-term outcome indicator could be misleading because it is a composite end point influenced by two events: death and tumor recurrence. However, to better determine long-term outcomes, future studies should match patients based on histological features (tumor size and nodule number) at explant pathology which clearly influence tumor recurrence and mortality [72].
The 1-year OS rate presented no significant difference between SLT and PLT, whereas 3- and 5-year overall survival rates were significantly slightly lower in SLT than after PLT. However, previous studies disclosed that the 5-year survival rates did not differ significantly for patients with SLT and for those with PLT (69% vs 73%; p = 0.34) [39].
Our results on survival post-SLT appear to be in contrast to the recent meta-analyses published on the subject [19,20,21]. However, this is not surprising because most of the studies included in the meta-analysis show a lower survival in the SLT group than in the PLT groups [39]. On the other hand, while survival differences often do not reach a statistically significant difference within an individual study, this difference in survival becomes statistically significant in the meta-analysis, which represents a statistical tool of great relevance and precision (since it “weights” the result in individual studies according to its precision) [82].
Despite the relatively high quality of the included articles, there are several limitations concerning this meta-analysis. The included studies were retrospective and not randomized, so the variables analyzed exhibited heterogeneity. However, the heterogeneity within the studies was treated and resolved by applying the random effect model on all the variables in the study [83]. Moreover, some studies included heterogeneous patient populations with transplantation for HCC recurrence and those who underwent SLT due to liver failure, although this latter indication represents less than 5% of the SLT. Therefore, because of the inherent risk of bias in the considered articles, it is desirable that further well-designed studies are conducted.
Nevertheless, our systematic review summarizes most of the available evidence in comparing outcomes of SLT and PLT. To our knowledge, it is the largest and most recent meta-analysis that makes these comparisons. It introduces completely new results that can form the scientific basis on which to develop further studies on the topic of liver transplantation as an integrated therapy in the treatment of HCC.
5. Conclusions
Our meta-analysis advocates the relative safety and feasibility of SLT over the PLT approach for patients with HCC. Specifically, the results of our study confirm that SLT offers comparable technical outcomes but slightly lower survival outcomes with respect to PLT.
Supplementary Materials
The following supporting information can be downloaded at: https://www.mdpi.com/article/10.3390/cancers14143465/s1, Files S1 and S2: Search strategy, and File S3: Publication bias.
Author Contributions
Study conception and design: G.P.G., G.E. and P.M.; acquisition of data: G.E., R.B. and T.O.; analysis and interpretation of data: G.P.G., G.E. and P.M.; drafting of manuscript: G.P.G., S.D.S. and R.B.; critical revision: G.P.G., S.D.S. and F.D.B. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding. The authors of this study declare no financial support.
Institutional Review Board Statement
The study did not require institutional review board as is a review of published studies.
Informed Consent Statement
Not applicable.
Data Availability Statement
Not applicable.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef] [PubMed]
- Guerrini, G.P.; Pleguezuelo, M.; Maimone, S.; Calvaruso, V.; Xirouchakis, E.; Patch, D.; Rolando, N.; Davidson, B.; Rolles, K.; Burroughs, A. Impact of tips preliver transplantation for the outcome posttransplantation. Am. J. Transplant. 2009, 9, 192–200. [Google Scholar] [CrossRef] [PubMed]
- DuBray, B.J., Jr.; Chapman, W.C.; Anderson, C.D. Hepatocellular carcinoma: A review of the surgical approaches to management. Mo. Med. 2011, 108, 195–198. [Google Scholar]
- Abrams, P.; Marsh, J.W. Current approach to hepatocellular carcinoma. Surg. Clin. North Am. 2010, 90, 803–816. [Google Scholar] [CrossRef]
- Di Benedetto, F.; Tarantino, G.; De Ruvo, N.; Cautero, N.; Montalti, R.; Guerrini, G.P.; Ballarin, R.; Spaggiari, M.; Smerieri, N.; Serra, V.; et al. University of Modena Experience in HIV-Positive Patients Undergoing Liver Transplantation. Transplant. Proc. 2011, 43, 1114–1118. [Google Scholar] [CrossRef]
- Lewin, S.M.; Mehta, N.; Kelley, R.K.; Roberts, J.P.; Yao, F.Y.; Brandman, D. Liver Transplant (LT) recipients with Nonalcoholic Steatohepatitis (NASH) Have Lower Risk Hepatocellular Carcinoma (HCC). Liver Transpl. 2017, 23, 1015–1022. [Google Scholar] [CrossRef] [PubMed]
- Mazzaferro, V. Squaring the circle of selection and allocation in liver transplantation for HCC: An adaptive approach. Hepatology 2016, 63, 1707–1717. [Google Scholar] [CrossRef]
- Mazzaferro, V.; Lencioni, R.; Majno, P. Early hepatocellular carcinoma on the procrustean bed of ablation, resection, and transplantation. Semin. Liver Dis. 2014, 34, 415–426. [Google Scholar]
- Alver, S.K.; Lorenz, D.J.; Washburn, K.; Marvin, M.R.; Brock, G.N. Comparison of two equivalent MELD scores for hepatocellular carcinoma patients using data from the United Network for Organ Sharing liver transplant waiting list registry. Transpl. Int. Off. J. Eur. Soc. Organ Transplant. 2017, 30, 1098. [Google Scholar]
- Akamatsu, N.; Cillo, U.; Cucchetti, A.; Donadon, M.; Pinna, A.D.; Torzilli, G.; Kokudo, N. Surgery and Hepatocellular Carcinoma. Liver Cancer 2016, 6, 44–50. [Google Scholar] [CrossRef]
- Bruix, J.; Fuster, J. A Snapshot of the Effective Indications and Results of Surgery for Hepatocellular Carcinoma in Tertiary Referral Centers: Is It Adherent to the EASL/AASLD Recommendations? An Observational Study of the HCC East-West Study Group. Ann. Surg. 2015, 262, e30. [Google Scholar] [CrossRef]
- Laurent, A.; Tayar, C.; Andréoletti, M.; Lauzet, J.Y.; Merle, J.C.; Cherqui, D. Laparoscopic liver resection facilitates salvage liver transplantation for hepatocellular carcinoma. J. Hepatobiliary Pancreat. Surg. 2009, 16, 310–314. [Google Scholar] [CrossRef] [PubMed]
- Aube, C.; Oberti, F.; Lonjon, J.; Pageaux, G.; Seror, O.; N’Kontchou, G.; Rode, A.; Radenne, S.; Cassinotto, C.; Vergniol, J.; et al. EASL and AASLD recommendations for the diagnosis of HCC to the test of daily practice. Liver Int. 2017, 37, 1515–1525. [Google Scholar] [CrossRef] [PubMed]
- Scatton, O.; Goumard, C.; Cauchy, F.; Fartoux, L.; Perdigao, F.; Conti, F.; Calmus, Y.; Boelle, P.Y.; Belghiti, J.; Rosmorduc, O.; et al. Early and resectable HCC: Definition and validation of a subgroup of patients who could avoid liver transplantation. J. Surg. Oncol. 2015, 111, 1007–1015. [Google Scholar] [CrossRef] [PubMed]
- Facciuto, M.E.; Rochon, C.; Pandey, M.; Rodriguez-Davalos, M.; Samaniego, S.; Wolf, D.C.; Kim-Schluger, L.; Rozenblit, G.; Sheiner, P.A. Surgical dilemma: Liver resection or liver transplantation for hepatocellular carcinoma and cirrhosis. Intention-to-treat analysis in patients within and outwith Milan criteria. HPB 2009, 11, 398–404. [Google Scholar] [CrossRef] [PubMed]
- Majno, P.E.; Sarasin, F.P.; Mentha, G.; Hadengue, A. Primary liver resection and salvage transplantation or primary liver transplantation in patients with single, small hepatocellular carcinoma and preserved liver function: An outcome-oriented decision analysis. Hepatology 2000, 31, 899–906. [Google Scholar] [CrossRef]
- Goumard, C.; Scatton, O. Resectable HCC: Should salvage liver transplantation for HCC be discussed de principe? Clin. Res. Hepatol. Gastroenterol. 2020, 44, 117–118. [Google Scholar] [CrossRef]
- Muaddi, H.; Al-Adra, D.P.; Beecroft, R.; Ghanekar, A.; Moulton, C.A.; Doyle, A.; Selzner, M.; Wei, A.; McGilvary, I.D.; Gallinger, S.; et al. Liver Transplantation is Equally Effective as a Salvage Therapy for Patients with Hepatocellular Carcinoma Recurrence Following Radiofrequency Ablation or Liver Resection with Curative Intent. Ann. Surg. Oncol. 2018, 25, 991–999. [Google Scholar] [CrossRef]
- Zhu, Y.; Dong, J.; Wang, W.L.; Li, M.X.; Lu, Y. Short- and long-term outcomes after salvage liver transplantation versus primary liver transplantation for hepatocellular carcinoma: A meta-analysis. Transplant. Proc. 2013, 45, 3329–3342. [Google Scholar] [CrossRef] [PubMed]
- Yadav, D.K.; Chen, W.; Bai, X.; Singh, A.; Li, G.; Ma, T.; Yu, X.; Xiao, Z.; Huang, B.; Liang, T. Salvage Liver Transplant versus Primary Liver Transplant for Patients with Hepatocellular Carcinoma. Ann. Transplant. 2018, 23, 524–545. [Google Scholar] [CrossRef]
- Xiong, Q.; Geng, T.T.; He, L.; Gao, H. Harm and Benefits of Salvage Transplantation for Hepatocellular Carcinoma: An Updated Meta-analysis. Transplant. Proc. 2016, 48, 3336–3347. [Google Scholar] [CrossRef] [PubMed]
- Zheng, S.; Xie, Q.; Cheng, J. Salvage liver transplant for hepatocellular carcinoma: Rescues and benefits. Transl. Gastroenterol. Hepatol. 2018, 3, 65. [Google Scholar] [CrossRef] [PubMed]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 88, 105906. [Google Scholar] [CrossRef]
- Goossen, K.; Tenckhoff, S.; Probst, P.; Grummich, K.; Mihaljevic, A.L.; Büchler, M.W.; Diener, M.K. Optimal literature search for systematic reviews in surgery. Langenbecks Arch. Surg. 2018, 403, 119–129. [Google Scholar] [CrossRef] [PubMed]
- Slim, K.; Nini, E.; Forestier, D.; Kwiatkowski, F.; Panis, Y.; Chipponi, J. Methodological index for non-randomized studies (minors): Development and validation of a new instrument. ANZ J. Surg. 2003, 73, 712–716. [Google Scholar] [CrossRef]
- Hozo, S.P.; Djulbegovic, B.; Hozo, I. Estimating the mean and variance from the median, range, and the size of a sample. BMC Med. Res. Methodol. 2005, 5, 13. [Google Scholar] [CrossRef]
- Luo, D.; Wan, X.; Liu, J.; Tong, T. Optimally estimating the sample mean from the sample size, median, mid-range, and/or mid-quartile range. Stat. Methods Med. Res. 2018, 27, 1785–1805. [Google Scholar] [CrossRef]
- Wan, X.; Wang, W.; Liu, J.; Tong, T. Estimating the sample mean and standard deviation from the sample size, median, range and/or interquartile range. BMC Med. Res. Methodol. 2014, 14, 135. [Google Scholar] [CrossRef]
- Adam, R.; Azoulay, D.; Castaing, D.; Eshkenazy, R.; Pascal, G.; Hashizume, K.; Samuel, D.; Bismuth, H. Liver resection as a bridge to transplantation for hepatocellular carcinoma on cirrhosis: A reasonable strategy? Ann. Surg. 2003, 238, 508–518; discussion 18–19. [Google Scholar] [CrossRef]
- Belghiti, J.; Cortes, A.; Abdalla, E.K.; Régimbeau, J.M.; Prakash, K.; Durand, F.; Sommacale, D.; Dondero, F.; Lesurtel, M.; Sauvanet, A.; et al. Resection prior to liver transplantation for hepatocellular carcinoma. Ann. Surg. 2003, 238, 885–893; discussion 92–93. [Google Scholar] [CrossRef]
- Margarit, C.; Escartín, A.; Castells, L.; Vargas, V.; Allende, E.; Bilbao, I. Resection for hepatocellular carcinoma is a good option in Child-Turcotte-Pugh class A patients with cirrhosis who are eligible for liver transplantation. Liver Transplant. 2005, 11, 1242–1251. [Google Scholar] [CrossRef] [PubMed]
- Hwang, S.; Lee, S.-G.; Moon, D.-B.; Ahn, C.-S.; Kim, K.-H.; Lee, Y.-J.; Ha, T.-Y.; Song, G.-W. Salvage living donor liver transplantation after prior liver resection for hepatocellular carcinoma. Liver Transplant. 2007, 13, 741–746. [Google Scholar] [CrossRef] [PubMed]
- Vennarecci, G.; Ettorre, G.M.; Antonini, M.; Santoro, R.; Maritti, M.; Tacconi, G.; Spoletini, D.; Tessitore, L.; Perracchio, L.; Visco, G.; et al. First-line liver resection and salvage liver transplantation are increasing therapeutic strategies for patients with hepatocellular carcinoma and child a cirrhosis. Transplant. Proc. 2007, 39, 1857–1860. [Google Scholar] [CrossRef] [PubMed]
- Del Gaudio, M.; Ercolani, G.; Ravaioli, M.; Cescon, M.; Lauro, A.; Vivarelli, M.; Zanello, M.; Cuccheti, A.; Vetrone, G.; Tuci, F.; et al. Liver transplantation for recurrent hepatocellular carcinoma on cirrhosis after liver resection: University of Bologna experience. Am. J. Transplant. 2008, 8, 1177–1185. [Google Scholar] [CrossRef]
- Kim, B.W.; Park, Y.K.; Kim, Y.B.; Wang, H.J.; Kim, M.W. Salvage liver transplantation for recurrent hepatocellular carcinoma after liver resection: Feasibility of the Milan criteria and operative risk. Transplant. Proc. 2008, 40, 3558–3561. [Google Scholar] [CrossRef]
- Shao, Z.; Lopez, R.; Shen, B.; Yang, G.S. Orthotopic liver transplantation as a rescue operation for recurrent hepatocellular carcinoma after partial hepatectomy. World J. Gastroenterol. 2008, 14, 4370–4376. [Google Scholar] [CrossRef][Green Version]
- Cherqui, D.; Laurent, A.; Mocellin, N.; Tayar, C.; Luciani, A.; Van Nhieu, J.T.; Decaens, T.; Hurtova, M.; Memeo, R.; Mallat, A.; et al. Liver resection for transplantable hepatocellular carcinoma: Long-term survival and role of secondary liver transplantation. Ann. Surg. 2009, 250, 738–746. [Google Scholar] [CrossRef]
- Sapisochin, G.; Bilbao, I.; Balsells, J.; Dopazo, C.; Caralt, M.; Lázaro, J.L.; Castells, L.; Allende, H.; Charco, R. Optimization of liver transplantation as a treatment of intrahepatic hepatocellular carcinoma recurrence after partial liver resection: Experience of a single European series. World J. Surg. 2010, 34, 2146–2154. [Google Scholar] [CrossRef]
- Hu, Z.; Zhou, J.; Xu, X.; Li, Z.; Zhou, L.; Wu, J.; Zhang, M.; Zheng, S. Salvage liver transplantation is a reasonable option for selected patients who have recurrent hepatocellular carcinoma after liver resection. PLoS ONE 2012, 7, e36587. [Google Scholar] [CrossRef]
- Kaido, T.; Mori, A.; Ogura, Y.; Hata, K.; Yoshizawa, A.; Iida, T.; Yagi, S.; Uemoto, S. Living donor liver transplantation for recurrent hepatocellular carcinoma after liver resection. Surgery 2012, 151, 55–60. [Google Scholar] [CrossRef]
- Liu, F.; Wei, Y.; Wang, W.; Chen, K.; Yan, L.; Wen, T.; Zhao, J.; Xu, M.; Li, B. Salvage liver transplantation for recurrent hepatocellular carcinoma within UCSF criteria after liver resection. PLoS ONE 2012, 7, e48932. [Google Scholar] [CrossRef]
- Moon, J.I.; Kwon, C.H.; Joh, J.W.; Choi, G.S.; Jung, G.O.; Kim, J.M.; Shin, M.; Choi, S.; Kim, S.; Lee, S.-K. Primary versus salvage living donor liver transplantation for patients with hepatocellular carcinoma: Impact of microvascular invasion on survival. Transplant. Proc. 2012, 44, 487–493. [Google Scholar] [CrossRef] [PubMed]
- De Carlis, L.; Di Sandro, S.; Giacomoni, A.; Mangoni, I.; Lauterio, A.; Mihaylov, P.; Cusumano, C.; Rampoldi, A. Liver transplantation for hepatocellular carcinoma recurrence after liver resection: Why deny this chance of cure? J. Clin. Gastroenterol. 2013, 47, 352–358. [Google Scholar] [CrossRef] [PubMed]
- Guerrini, G.P.; Gerunda, G.E.; Montalti, R.; Ballarin, R.; Cautero, N.; De Ruvo, N.; Spaggiari, M.; Di Benedetto, F. Results of salvage liver transplantation. Liver Int. 2014, 34, e96–e104. [Google Scholar] [CrossRef]
- Abe, T.; Tashiro, H.; Teraoka, Y.; Hattori, M.; Tanimine, N.; Kuroda, S.; Tahara, H.; Ohira, M.; Tanaka, Y.; Kobayashi, T.; et al. Efficacy and Feasibility of Salvage Living Donor Liver Transplantation after Initial Liver Resection in Patients with Hepatocellular Carcinoma. Dig. Surg. 2015, 33, 8–14. [Google Scholar] [CrossRef]
- Bhangui, P.; Allard, M.A.; Vibert, E.; Cherqui, D.; Pelletier, G.; Cunha, A.S.; Guettier, C.; Valle, J.-C.D.; Saliba, F.; Bismuth, H.; et al. Salvage Versus Primary Liver Transplantation for Early Hepatocellular Carcinoma: Do Both Strategies Yield Similar Outcomes? Ann. Surg. 2016, 264, 155–163. [Google Scholar] [CrossRef]
- Bhavin Bhupendra Vasavada C-LC. Salvage transplantation for post-resection recurrence in hepatocellular carcinoma associated with hepatitis C virus. etiology: A feasible strategy? Hepatoma Res. 2015, 1, 36–40. [Google Scholar] [CrossRef][Green Version]
- Wang, P.; Pu, Y.; Li, H.; Shi, B.; Zheng, S.; Zhong, L. Prognosis for recipients with hepatocellular carcinoma of salvage liver transplantation versus those of primary liver transplantation: A retrospective single-center study. Springer Plus 2016, 5, 1809. [Google Scholar] [CrossRef]
- Shan, Y.; Huang, L.; Xia, Q. Salvage Liver Transplantation Leads to Poorer Outcome in Hepatocellular Carcinoma Compared with Primary Liver Transplantation. Sci. Rep. 2017, 7, 44652. [Google Scholar] [CrossRef]
- Yong, C.C.; Elsarawy, A.M.; Wang, S.H.; Lin, T.S.; Wang, C.C.; Li, W.F.; Lin, T.-L.; Kuo, F.-Y.; Cheng, Y.-F.; Chen, C.-L.; et al. The surgical challenges of salvage living donor liver transplantation for Hepatocellular carcinoma; The cumulative experience of 100 cases-A retrospective cohort study and a propensity score analysis. Int. J. Surg. 2018, 54, 187–192. [Google Scholar] [CrossRef]
- Chan, K.M.; Cheng, C.H.; Wu, T.H.; Lee, C.F.; Wu, T.J.; Chou, H.S.; Lee, W.-C. Salvage living donor liver transplantation for posthepatectomy recurrence: A higher incidence of recurrence but promising strategy for long-term survival. Cancer Manag. Res. 2019, 11, 7295–7305. [Google Scholar] [CrossRef] [PubMed]
- Guo, Y.; Tan, E.K.; Krishnamoorthy, T.L.; Tan, C.K.; Tan, B.H.; Tan, T.T.; Lee, S.-Y.; Chan, C.-Y.; Cheow, P.-C.; Chung, A.Y.F.; et al. Outcomes of salvage liver transplant for recurrent hepatocellular carcinoma: A comparison with primary liver transplant. Ann. Hepatobiliary Pancreat. Surg. 2019, 23, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Hwang, S.; Song, G.W.; Ahn, C.S.; Kim, K.H.; Moon, D.B.; Ha, T.Y.; Jung, D.; Park, G.; Yoon, Y.; Lee, S. Salvage living donor liver transplantation for hepatocellular carcinoma recurrence after hepatectomy: Quantitative prediction using ADV score. J. Hepatobiliary Pancreat. Sci. 2021, 28, 1000–1013. [Google Scholar] [CrossRef] [PubMed]
- Toniutto, P.; Zanetto, A.; Ferrarese, A.; Burra, P. Current challenges and future directions for liver transplantation. Liver Int. 2016, 37, 317–327. [Google Scholar] [CrossRef]
- Lee, S.; Ahn, C.; Ha, T.; Moon, D.; Choi, K.; Song, G.; Chung, D.; Park, G.; Yu, Y.; Choi, N.; et al. Liver transplantation for hepatocellular carcinoma: Korean experience. J. Hepatobiliary Pancreat. Sci. 2010, 17, 539–547. [Google Scholar] [CrossRef] [PubMed]
- Azzam, A.Z. Liver transplantation as a management of hepatocellular carcinoma. World J. Hepatol. 2015, 7, 1347–1354. [Google Scholar] [CrossRef]
- Cucchetti, A.; Cescon, M.; Bertuzzo, V.; Bigonzi, E.; Ercolani, G.; Morelli, M.C.; Ravaioli, M.; Pinna, A.D. Can the dropout risk of candidates with hepatocellular carcinoma predict survival after liver transplantation? Am. J. Transplant. 2011, 11, 1696–1704. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Di Benedetto, F.; Tarantino, G.; De Ruvo, N.; Cautero, N.; Montalti, R.; Guerrini, G.P.; Ballarin, R.; Spaggiari, M.; Serra, V.; Guaraldi, G.; et al. Liver Transplantation for Hepatocellular Carcinoma in HIV Co-Infected Patients: A Single Centre Experience. Liver Transplant. 2011, 17, S273–S274. [Google Scholar]
- Guerrini, G.P.; Berretta, M.; Guaraldi, G.; Magistri, P.; Esposito, G.; Ballarin, R.; Serra, V.; Di Sandro, S.; Di Benedetto, F. Liver Transplantation for HCC in HIV-Infected Patients: Long-Term Single-Center Experience. Cancers 2021, 13, 4727. [Google Scholar] [CrossRef]
- Xu, D.W.; Wan, P.; Xia, Q. Liver transplantation for hepatocellular carcinoma beyond the Milan criteria: A review. World J. Gastroenterol. 2016, 22, 3325–3334. [Google Scholar] [CrossRef]
- Di Benedetto, F.; Mimmo, A.; De Ruvo, N.; Montalti, R.; Cautero, N.; Guerrini, G.P.; Gerunda, G.E. Liver Transplantation Due to TIPS Complications. Liver Transplant. 2010, 16, S161. [Google Scholar]
- Parikh, N.D.; Waljee, A.K.; Singal, A.G. Downstaging hepatocellular carcinoma: A systematic review and pooled analysis. Liver Transplant. 2015, 21, 1142–1152. [Google Scholar] [CrossRef] [PubMed]
- Jarnagin, W.R. Management of small hepatocellular carcinoma: A review of transplantation, resection, and ablation. Ann. Surg. Oncol. 2010, 17, 1226–1233. [Google Scholar] [CrossRef][Green Version]
- Morise, Z.; Kawabe, N.; Tomishige, H.; Nagata, H.; Kawase, J.; Arakawa, S.; Yoshida, R.; Isetani, M. Recent advances in liver resection for hepatocellular carcinoma. Front. Surg. 2014, 1, 21. [Google Scholar] [CrossRef]
- Hanish, S.I.; Knechtle, S.J. Liver transplantation for the treatment of hepatocellular carcinoma. Oncology 2011, 25, 752–757. [Google Scholar]
- Llovet, J.M.; Fuster, J.; Bruix, J. Intention-to-treat analysis of surgical treatment for early hepatocellular carcinoma: Resection versus transplantation. Hepatology 1999, 30, 1434–1440. [Google Scholar] [CrossRef]
- Colombo, M.; Sangiovanni, A. Treatment of hepatocellular carcinoma: Beyond international guidelines. Liver Int. 2015, 35 (Suppl. S1), 129–138. [Google Scholar] [CrossRef]
- Magistri, P.; Olivieri, T.; Assirati, G.; Guerrini, G.P.; Ballarin, R.; Tarantino, G.; Di Benedetto, F. Robotic Liver Resection Expands the Opportunities of Bridging Before Liver Transplantation. Liver Transpl. 2019, 25, 1110–1112. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.H.; Kim, K.H.; Ha, T.Y.; Jung, D.H.; Park, G.C.; Lee, S.G. Salvage living donor liver transplantation for recurrent hepatocellular carcinoma after prior laparoscopic hepatectomy. Hepatobiliary Pancreat Dis Int. 2018, 17, 473–476. [Google Scholar] [CrossRef] [PubMed]
- Felli, E.; Baumert, T.; Pessaux, P. Is minimally invasive true anatomical HCC resection a future way to improve results in bridge or salvage liver transplantation? Clin. Res. Hepatol. Gastroenterol. 2021, 45, 101396. [Google Scholar] [CrossRef]
- Qu, W.; Zhu, Z.J.; Sun, L.Y.; Wei, L.; Liu, Y.; Zeng, Z.G. Salvage liver transplantation for hepatocellular carcinoma recurrence after primary liver resection. Clin. Res. Hepatol. Gastroenterol. 2015, 39, 93–97. [Google Scholar] [CrossRef] [PubMed]
- Pawlik, T.M.; Delman, K.A.; Vauthey, J.N.; Nagorney, D.M.; Ng, I.O.; Ikai, I.; Yamaoka, Y.; Belghiti, J.; Lauwers, G.Y.; Poon, R.T.; et al. Tumor size predicts vascular invasion and histologic grade: Implications for selection of surgical treatment for hepatocellular carcinoma. Liver Transplant. 2005, 11, 1086–1092. [Google Scholar] [CrossRef] [PubMed]
- Guerrini, G.P.; Pinelli, D.; Di Benedetto, F.; Marini, E.; Corno, V.; Guizzetti, M.; Aluffi, A.; Zambelli, M.; Fagiuoli, S.; Lucà, M.G.; et al. Predictive value of nodule size and differentiation in HCC recurrence after liver transplantation. Surg. Oncol. 2015, 25, 419–428. [Google Scholar] [CrossRef] [PubMed]
- Ferrer-Fàbrega, J.; Forner, A.; Liccioni, A.; Miquel, R.; Molina, V.; Navasa, M.; Fondevila, C.; García-Valdecasas, J.C.; Bruix, J.; Fuster, J. Prospective validation of ab initio liver transplantation in hepatocellular carcinoma upon detection of risk factors for recurrence after resection. Hepatology 2016, 63, 839–849. [Google Scholar] [CrossRef]
- Sala, M.; Fuster, J.; Llovet, J.M.; Navasa, M.; Solé, M.; Varela, M.; Pons, F.; Rimola, A.; García-Valdecasas, J.C.; Brú, C.; et al. High pathological risk of recurrence after surgical resection for hepatocellular carcinoma: An indication for salvage liver transplantation. Liver Transplant. 2004, 10, 1294–1300. [Google Scholar] [CrossRef]
- Lee, S.G. Salvage living-donor liver transplantation to previously hepatectomized hepatocellular carcinoma patients: Is it a reasonable strategy? Hepatobiliary Pancreat. Dis. Int. 2013, 12, 10–11. [Google Scholar] [CrossRef]
- Fuks, D.; Dokmak, S.; Paradis, V.; Diouf, M.; Durand, F.; Belghiti, J. Benefit of initial resection of hepatocellular carcinoma followed by transplantation in case of recurrence: An intention-to-treat analysis. Hepatology 2012, 55, 132–140. [Google Scholar] [CrossRef]
- Chok, K. Management of recurrent hepatocellular carcinoma after liver transplant. World J. Hepatol. 2015, 7, 1142–1148. [Google Scholar] [CrossRef]
- Tarantino, G.; Magistri, P.; Ballarin, R.; Di Francia, R.; Berretta, M.; Di Benedetto, F. Oncological Impact of M-Tor Inhibitor Immunosuppressive Therapy after Liver Transplantation for Hepatocellular Carcinoma: Review of the Literature. Front. Pharmacol. 2016, 7, 387. [Google Scholar] [CrossRef]
- Duvoux, C.; Toso, C. mTOR inhibitor therapy: Does it prevent HCC recurrence after liver transplantation? Transplant. Rev. 2015, 29, 168–174. [Google Scholar] [CrossRef]
- Perricone, G.; Mancuso, A.; Belli, L.S.; Mazzarelli, C.; Zavaglia, C. Sorafenib for the treatment of recurrent hepatocellular carcinoma after liver transplantation: Does mTOR inhibitors association augment toxicity? Eur. J. Gastroenterol. Hepatol. 2014, 26, 577–578. [Google Scholar] [CrossRef] [PubMed]
- Jackson, D.; Turner, R. Power analysis for random-effects meta-analysis. Res. Synth. Methods 2017, 8, 290–302. [Google Scholar] [CrossRef] [PubMed]
- Higgins, J.; Thompson, S.; Deeks, J.; Altman, D. Statistical heterogeneity in systematic reviews of clinical trials: A critical appraisal of guidelines and practice. J. Health Serv. Res. Policy 2002, 7, 51–61. [Google Scholar] [CrossRef] [PubMed]






















Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).