
Extracellular Vesicle-Derived Protein File from Peripheral Blood Predicts Immune-Related Adverse Events in Gastric Cancer Patients Receiving Immunotherapy

Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Patient Information
2.2. Specimen Preparation and Plasma EVs Isolation
2.3. EV Expression Array Determination and Identification
2.4. Statistical Methods Database
3. Results
3.1. irAEs May Represent a Better Disease Control Rate of Immunotherapy in GC
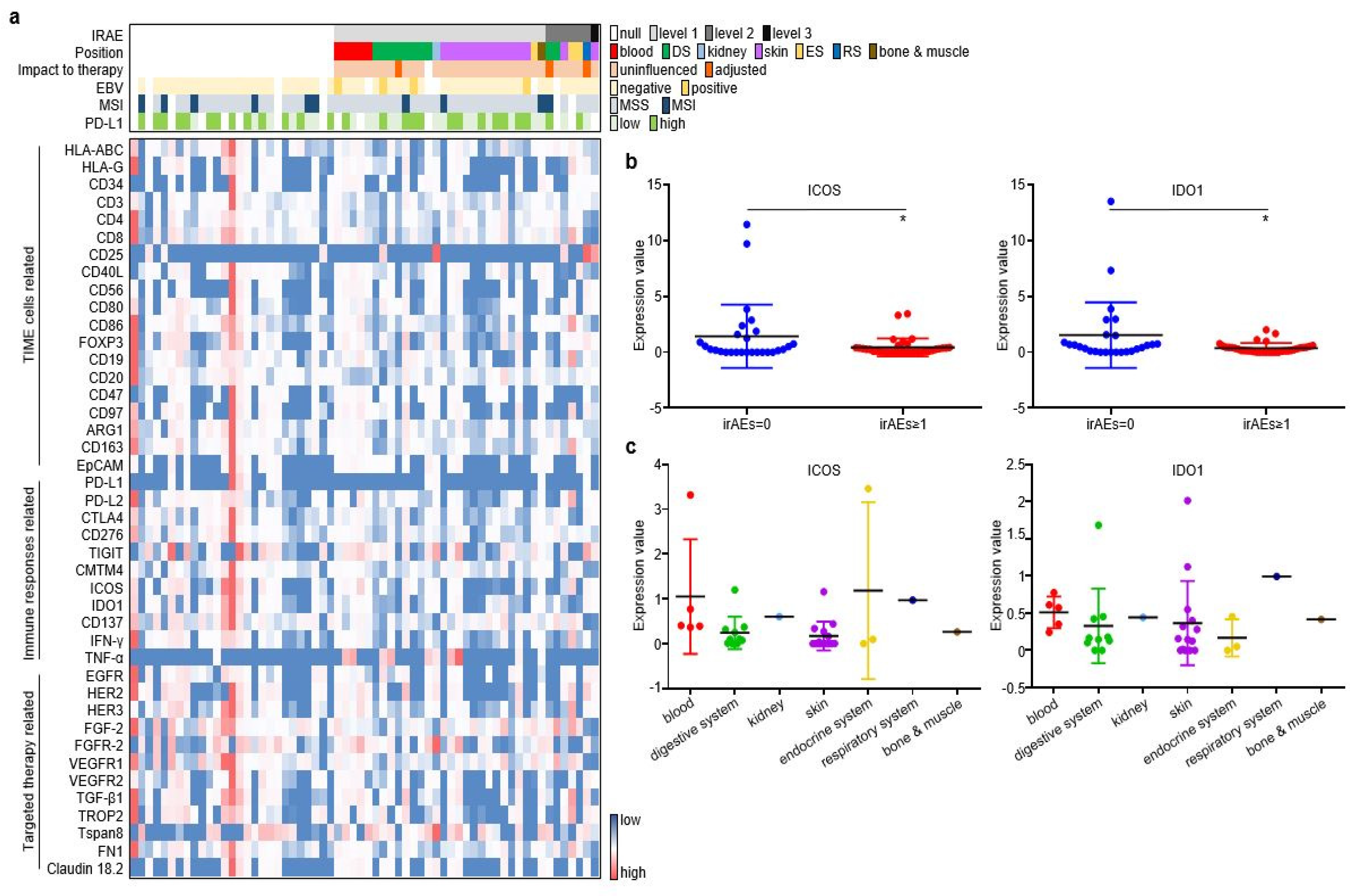
3.2. The Expressional Spectrum of Plasma EV-Proteins Identified ICOS and IDO1 as irAE Predictors
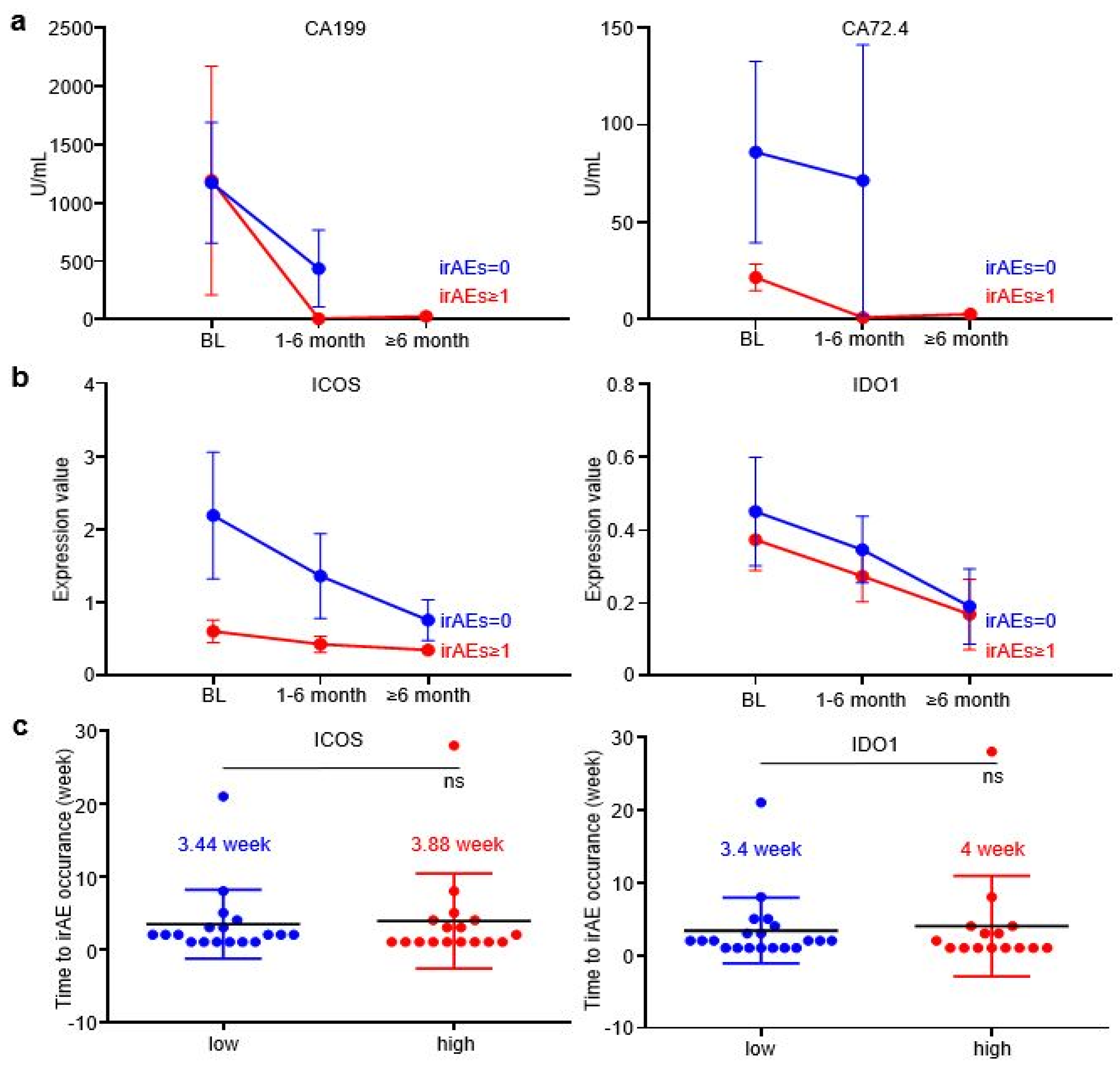
3.3. EV-ICOS and EV-IDO1 Dynamically Predicted irAEs
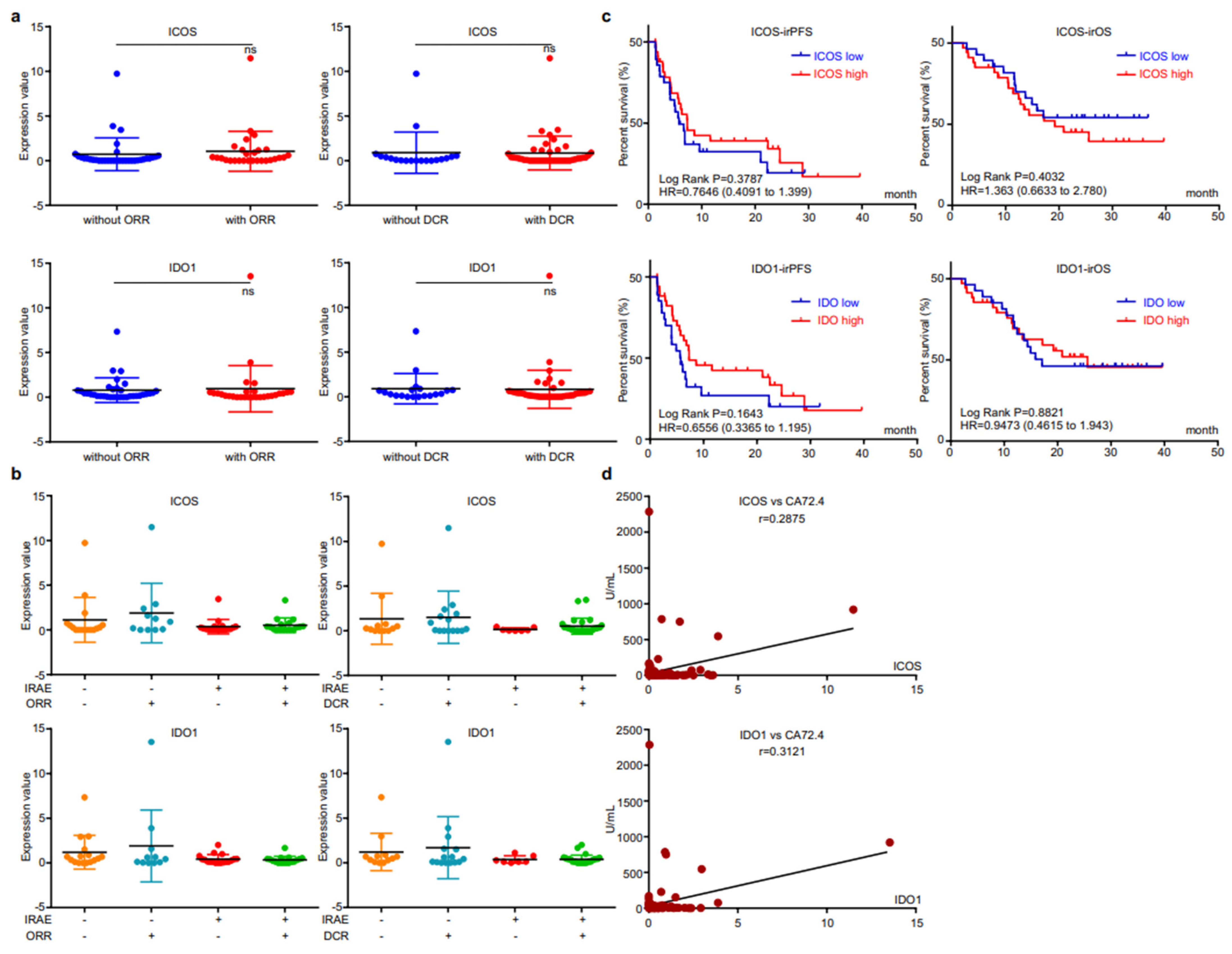
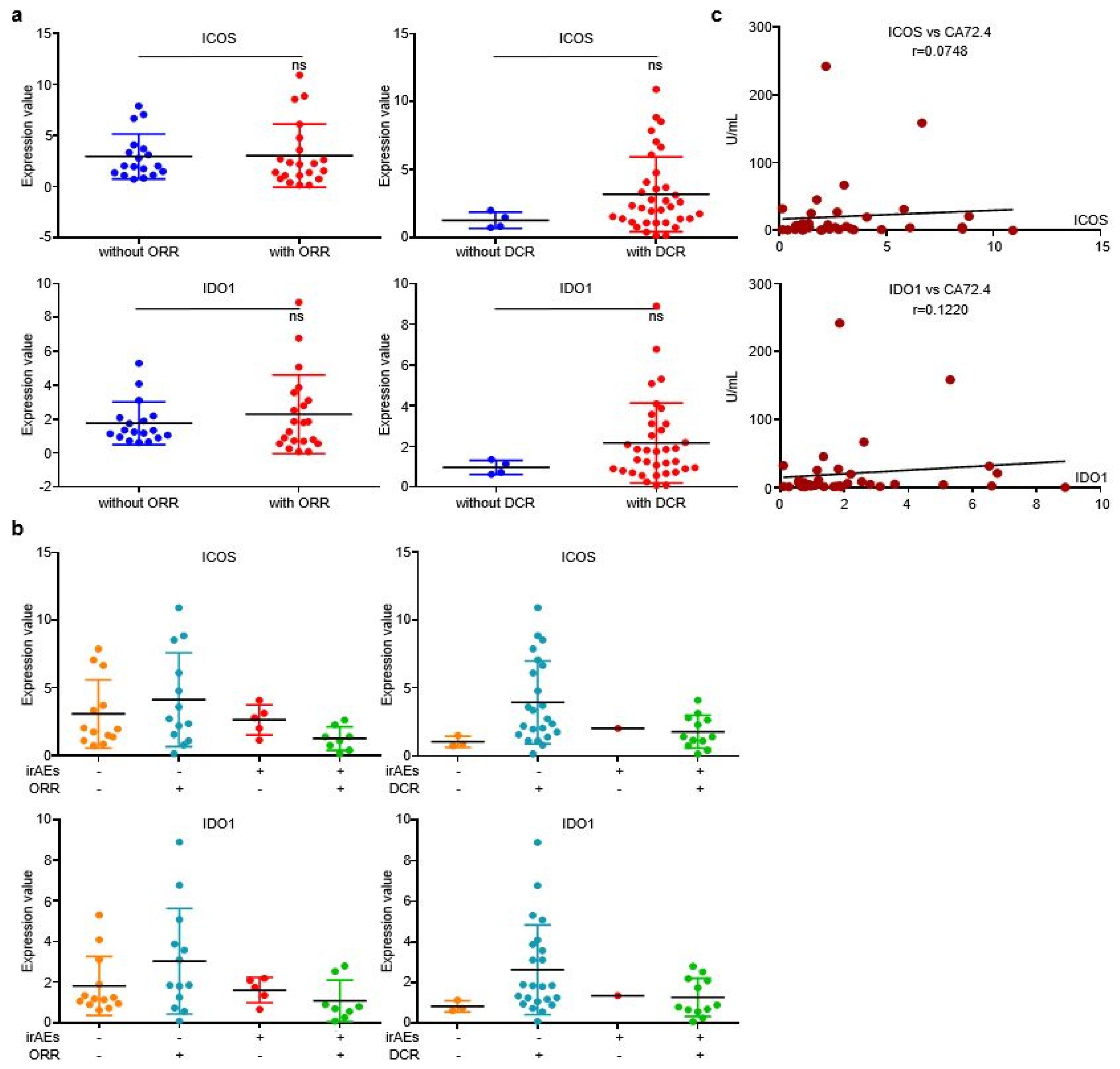
3.4. EV-Derived ICOS/IDO1 Were Irrelevant to Immunotherapeutic Effectiveness, Yet Refected Short-Term Changes of Circulating Tumor Marker CA72.4
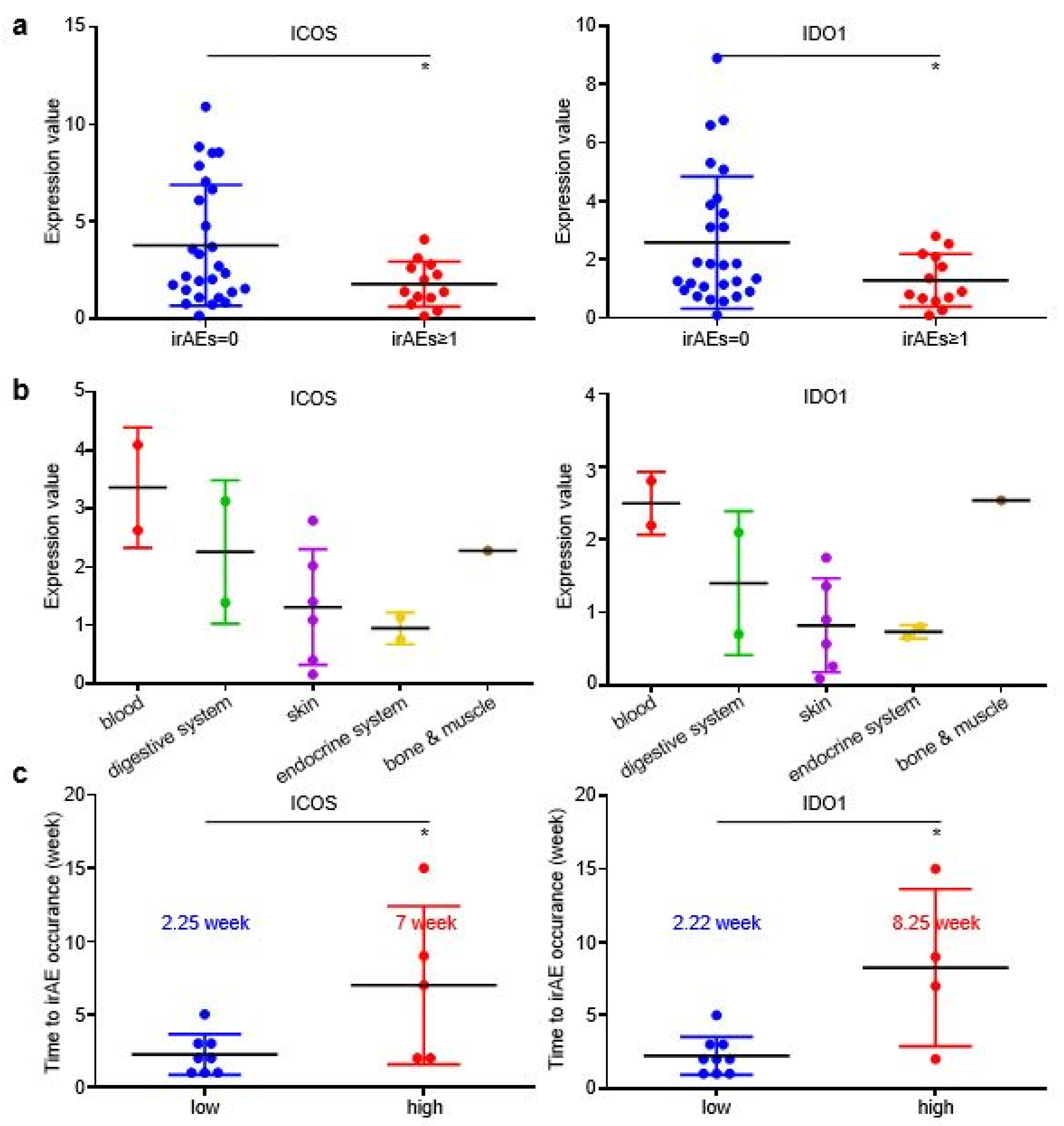
3.5. EV-Derived ICOS/IDO1 Remained as Predictive Biomarkers for irAEs in Prospective Validation
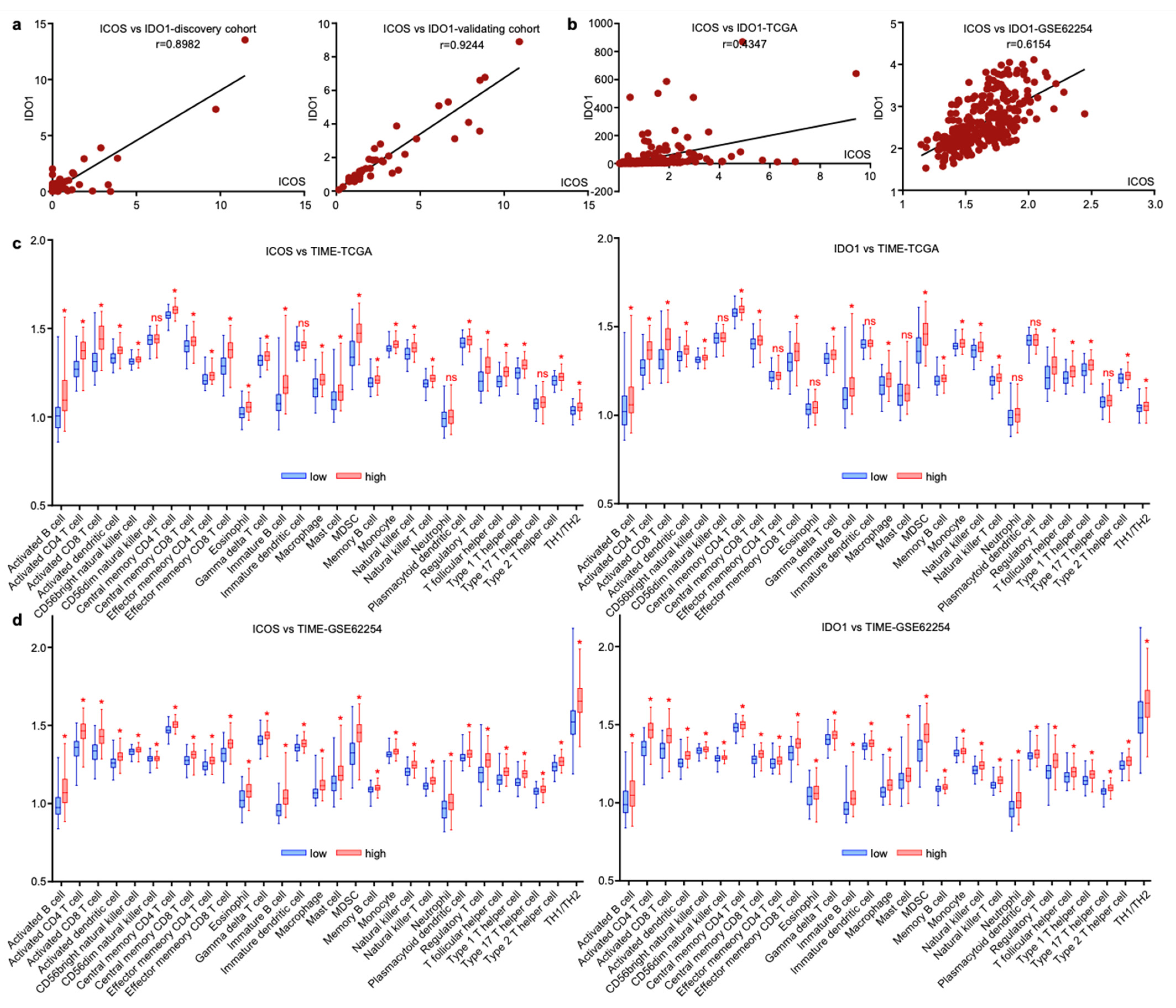
3.6. ICOS and IDO1 Were Related with Unique Tumor-Microenvironmental Features
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Bray, F.; Ferlay, J.; Soerjomataram, I.; Siegel, R.L.; Torre, L.A.; Jemal, A. Global cancer statistics 2018: Globocan estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2018, 68, 394–424. [Google Scholar] [CrossRef] [PubMed]
- Boku, N.; Ryu, M.H.; Kato, K.; Chung, H.C.; Minashi, K.; Lee, K.W.; Cho, H.; Kang, W.K.; Komatsu, Y.; Tsuda, M.; et al. Safety and efficacy of nivolumab in combination with s-1/capecitabine plus oxaliplatin in patients with previously untreated, unresectable, advanced, or recurrent gastric/gastroesophageal junction cancer: Interim results of a randomized, phase ii trial (attraction-4). Ann. Oncol. 2019, 30, 250–258. [Google Scholar] [CrossRef] [PubMed]
- Shitara, K.; Van Cutsem, E.; Bang, Y.J.; Fuchs, C.; Wyrwicz, L.; Lee, K.W.; Kudaba, I.; Garrido, M.; Chung, H.C.; Lee, J.; et al. Efficacy and safety of pembrolizumab or pembrolizumab plus chemotherapy vs chemotherapy alone for patients with first-line, advanced gastric cancer: The keynote-062 phase 3 randomized clinical trial. JAMA Oncol. 2020, 6, 1571–1580. [Google Scholar] [CrossRef] [PubMed]
- Janjigian, Y.Y.; Shitara, K.; Moehler, M.; Garrido, M.; Salman, P.; Shen, L.; Wyrwicz, L.; Yamaguchi, K.; Skoczylas, T.; Campos Bragagnoli, A.; et al. First-line nivolumab plus chemotherapy versus chemotherapy alone for advanced gastric, gastro-oesophageal junction, and oesophageal adenocarcinoma (checkmate 649): A randomised, open-label, phase 3 trial. Lancet 2021, 398, 27–40. [Google Scholar] [CrossRef]
- Kang, Y.K.; Boku, N.; Satoh, T.; Ryu, M.H.; Chao, Y.; Kato, K.; Chung, H.C.; Chen, J.S.; Muro, K.; Kang, W.K.; et al. Nivolumab in patients with advanced gastric or gastro-oesophageal junction cancer refractory to, or intolerant of, at least two previous chemotherapy regimens (ono-4538-12, attraction-2): A randomised, double-blind, placebo-controlled, phase 3 trial. Lancet 2017, 390, 2461–2471. [Google Scholar] [CrossRef]
- Yu, H.Y.; Li, C.P.; Huang, Y.H.; Hsu, S.J.; Wang, Y.P.; Hsieh, Y.C.; Fang, W.L.; Huang, K.H.; Li, A.F.; Lee, R.C.; et al. Microsatellite instability, epstein-barr virus, and programmed cell death ligand 1 as predictive markers for immunotherapy in gastric cancer. Cancers 2022, 14, 218. [Google Scholar] [CrossRef]
- Chao, J.; Fuchs, C.S.; Shitara, K.; Tabernero, J.; Muro, K.; Van Cutsem, E.; Bang, Y.J.; De Vita, F.; Landers, G.; Yen, C.J.; et al. Assessment of pembrolizumab therapy for the treatment of microsatellite instability-high gastric or gastroesophageal junction cancer among patients in the keynote-059, keynote-061, and keynote-062 clinical trials. JAMA Oncol. 2021, 7, 895–902. [Google Scholar] [CrossRef]
- Corallo, S.; Fucà, G.; Morano, F.; Salati, M.; Spallanzani, A.; Gloghini, A.; Volpi, C.C.; Trupia, D.V.; Lobefaro, R.; Guarini, V.; et al. Clinical behavior and treatment response of epstein-barr virus-positive metastatic gastric cancer: Implications for the development of future trials. Oncologist 2020, 25, 780–786. [Google Scholar] [CrossRef]
- Chan, K.K.; Bass, A.R. Autoimmune complications of immunotherapy: Pathophysiology and management. BMJ 2020, 369, m736. [Google Scholar] [CrossRef]
- Jia, X.H.; Geng, L.Y.; Jiang, P.P.; Xu, H.; Nan, K.J.; Yao, Y.; Jiang, L.L.; Sun, H.; Qin, T.J.; Guo, H. The biomarkers related to immune related adverse events caused by immune checkpoint inhibitors. J. Exp. Clin. Cancer Res. 2020, 39, 284. [Google Scholar] [CrossRef]
- Bertrand, A.; Kostine, M.; Barnetche, T.; Truchetet, M.E.; Schaeverbeke, T. mmune related adverse events associated with anti-ctla-4 antibodies: Systematic review and meta-analysis. BMC Med. 2015, 13, 211. [Google Scholar] [CrossRef] [PubMed]
- Zhang, H.; Lu, J.; Liu, J.; Zhang, G.; Lu, A. Advances in the discovery of exosome inhibitors in cancer. J. Enzym. Inhib. Med. Chem. 2020, 35, 1322–1330. [Google Scholar] [CrossRef]
- Xia, Z.; Qing, B.; Wang, W.; Gu, L.; Chen, H.; Yuan, Y. Formation, contents, functions of exosomes and their potential in lung cancer diagnostics and therapeutics. Thorac. Cancer 2021, 12, 3088–3100. [Google Scholar] [CrossRef] [PubMed]
- Jing, Z.; Chen, K.; Gong, L. The significance of exosomes in pathogenesis, diagnosis, and treatment of esophageal cancer. Int. J. Nanomed. 2021, 16, 6115–6127. [Google Scholar] [CrossRef] [PubMed]
- Thompson, J.A.; Schneider, B.J.; Brahmer, J.; Andrews, S.; Armand, P.; Bhatia, S.; Budde, L.E.; Costa, L.; Davies, M.; Dunnington, D.; et al. Nccn guidelines insights: Management of immunotherapy-related toxicities, version 1.2020. J. Natl. Compr. Cancer Netw. 2020, 18, 230–241. [Google Scholar] [CrossRef] [PubMed]
- Eisenhauer, E.A.; Therasse, P.; Bogaerts, J.; Schwartz, L.H.; Sargent, D.; Ford, R.; Dancey, J.; Arbuck, S.; Gwyther, S.; Mooney, M.; et al. New response evaluation criteria in solid tumours: Revised recist guideline (version 1.1). Eur. J. Cancer 2009, 45, 228–247. [Google Scholar] [CrossRef]
- Zhang, C.; Chong, X.; Jiang, F.; Gao, J.; Chen, Y.; Jia, K.; Fan, M.; Liu, X.; An, J.; Li, J.; et al. Plasma extracellular vesicle derived protein profile predicting and monitoring immunotherapeutic outcomes of gastric cancer. J. Extracell. Vesicles. 2022, 11, e12209. [Google Scholar] [CrossRef]
- Wang, J.; Li, Q.; Yuan, J.; Wang, J.; Chen, Z.; Liu, Z.; Li, Z.; Lai, Y.; Gao, J.; Shen, L. Cdk4/6 inhibitor-shr6390 exerts potent antitumor activity in esophageal squamous cell carcinoma by inhibiting phosphorylated rb and inducing g1 cell cycle arrest. J. Transl. Med. 2017, 15, 127. [Google Scholar] [CrossRef]
- Dubin, K.; Callahan, M.K.; Ren, B.; Khanin, R.; Viale, A.; Ling, L.; No, D.; Gobourne, A.; Littmann, E.; Huttenhower, C.; et al. Intestinal microbiome analyses identify melanoma patients at risk for checkpoint-blockade-induced colitis. Nat. Commun. 2016, 7, 10391. [Google Scholar] [CrossRef]
- Chaput, N.; Lepage, P.; Coutzac, C.; Soularue, E.; Le Roux, K.; Monot, C.; Boselli, L.; Routier, E.; Cassard, L.; Collins, M.; et al. Baseline gut microbiota predicts clinical response and colitis in metastatic melanoma patients treated with ipilimumab. Ann. Oncol. 2017, 28, 1368–1379. [Google Scholar] [CrossRef]
- Abolhassani, A.R.; Schuler, G.; Kirchberger, M.C.; Heinzerling, L. C-reactive protein as an early marker of immune-related adverse events. J. Cancer Res. Clin. Oncol. 2019, 145, 2625–2631. [Google Scholar] [CrossRef] [PubMed]
- Hasan Ali, O.; Berner, F.; Bomze, D.; Fässler, M.; Diem, S.; Cozzio, A.; Jörger, M.; Früh, M.; Driessen, C.; Lenz, T.L.; et al. Human leukocyte antigen variation is associated with adverse events of checkpoint inhibitors. Eur. J. Cancer 2019, 107, 8–14. [Google Scholar] [CrossRef] [PubMed]
- Andrews, M.C.; Duong, C.P.M.; Gopalakrishnan, V.; Iebba, V.; Chen, W.S.; Derosa, L.; Khan, M.A.W.; Cogdill, A.P.; White, M.G.; Wong, M.C.; et al. Gut microbiota signatures are associated with toxicity to combined ctla-4 and pd-1 blockade. Nat. Med. 2021, 27, 1432–1441. [Google Scholar] [CrossRef] [PubMed]
- Shahabi, V.; Berman, D.; Chasalow, S.D.; Wang, L.; Tsuchihashi, Z.; Hu, B.; Panting, L.; Jure-Kunkel, M.; Ji, R.R. Gene expression profiling of whole blood in ipilimumab-treated patients for identification of potential biomarkers of immune-related gastrointestinal adverse events. J. Transl. Med. 2013, 11, 75. [Google Scholar] [CrossRef] [PubMed]
- Tarhini, A.A.; Zahoor, H.; Lin, Y.; Malhotra, U.; Sander, C.; Butterfield, L.H.; Kirkwood, J.M. Baseline circulating il-17 predicts toxicity while tgf-β1 and il-10 are prognostic of relapse in ipilimumab neoadjuvant therapy of melanoma. J. Immunother. Cancer 2015, 3, 39. [Google Scholar] [CrossRef]
- Tahir, S.A.; Gao, J.; Miura, Y.; Blando, J.; Tidwell, R.S.S.; Zhao, H.; Subudhi, S.K.; Tawbi, H.; Keung, E.; Wargo, J.; et al. Autoimmune antibodies correlate with immune checkpoint therapy-induced toxicities. Proc. Natl. Acad. Sci. USA 2019, 116, 22246–22251. [Google Scholar] [CrossRef]
- Das, R.; Bar, N.; Ferreira, M.; Newman, A.M.; Zhang, L.; Bailur, J.K.; Bacchiocchi, A.; Kluger, H.; Wei, W.; Halaban, R.; et al. Early b cell changes predict autoimmunity following combination immune checkpoint blockade. J. Clin. Investig. 2018, 128, 715–720. [Google Scholar] [CrossRef]
- Lozano, A.X.; Chaudhuri, A.A.; Nene, A.; Bacchiocchi, A.; Earland, N.; Vesely, M.D.; Usmani, A.; Turner, B.E.; Steen, C.B.; Luca, B.A.; et al. T cell characteristics associated with toxicity to immune checkpoint blockade in patients with melanoma. Nat. Med. 2022, 28, 353–362. [Google Scholar] [CrossRef]
- Heydari, R.; Abdollahpour-Alitappeh, M.; Shekari, F.; Meyfour, A. Emerging role of extracellular vesicles in biomarking the gastrointestinal diseases. Expert Rev. Mol. Diagn. 2021, 21, 939–962. [Google Scholar] [CrossRef]
- Sanborn, R.E.; Hamid, O.; de Vries, E.G.; Ott, P.A.; Garcia-Corbacho, J.; Boni, V.; Bendell, J.; Autio, K.A.; Cho, D.C.; Plummer, R.; et al. Cx-072 (pacmilimab), a probody pd-l1 inhibitor, in combination with ipilimumab in patients with advanced solid tumors (proclaim-cx-072): A first-in-human, dose-finding study. J. Immunother. Cancer 2021, 9, e002446. [Google Scholar] [CrossRef]
- Prendergast, G.C.; Malachowski, W.J.; Mondal, A.; Scherle, P.; Muller, A.J. Indoleamine 2,3-dioxygenase and its therapeutic inhibition in cancer. Int. Rev. Cell Mol. Biol. 2018, 336, 175–203. [Google Scholar] [CrossRef] [PubMed]
- Zhang, X.; Hu, X.; Tian, T.; Pang, W. The role of icos in allergic disease: Positive or negative? Int. Immunopharmacol. 2022, 103, 108394. [Google Scholar] [CrossRef] [PubMed]
- Pang, W.; Jiang, Y.; Li, A.; Zhang, J.; Chen, M.; Hu, L.; Li, Z.; Wang, D. Bacteroides thetaiotaomicron ameliorates experimental allergic airway inflammation via activation of icos(+)tregs and inhibition of th2 response. Front. Immunol. 2021, 12, 620943. [Google Scholar] [CrossRef] [PubMed]
- Uwadiae, F.I.; Pyle, C.J.; Walker, S.A.; Lloyd, C.M.; Harker, J.A. Targeting the icos/icos-l pathway in a mouse model of established allergic asthma disrupts t follicular helper cell responses and ameliorates disease. Allergy 2019, 74, 650–662. [Google Scholar] [CrossRef]
- Ünüvar, S.; Erge, D.; Kılıçarslan, B.; Gözükara Bağ, H.G.; Çatal, F.; Girgin, G.; Baydar, T. Neopterin levels and indoleamine 2,3-dioxygenase activity as biomarkers of immune system activation and childhood allergic diseases. Ann. Lab. Med. 2019, 39, 284–290. [Google Scholar] [CrossRef]
- Esmaeili, S.; Ahajavi, J. The role of indoleamine 2,3-dioxygenase in allergic disorders. Mol. Biol. Rep. 2022, 49, 3297–3306. [Google Scholar] [CrossRef]
- Kraehenbuehl, L.; Weng, C.H.; Eghbali, S.; Wolchok, J.D.; Merghoub, T. Enhancing immunotherapy in cancer by targeting emerging immunomodulatory pathways. Nat. Rev. Clin. Oncol. 2022, 19, 37–50. [Google Scholar] [CrossRef]
- Guo, Y.; Liu, Y.; Wu, W.; Ling, D.; Zhang, Q.; Zhao, P.; Hu, X. Indoleamine 2,3-dioxygenase (ido) inhibitors and their nanomedicines for cancer immunotherapy. Biomaterials 2021, 276, 121018. [Google Scholar] [CrossRef]
- Kjeldsen, J.W.; Lorentzen, C.L.; Martinenaite, E.; Ellebaek, E.; Donia, M.; Holmstroem, R.B.; Klausen, T.W.; Madsen, C.O.; Ahmed, S.M.; Weis-Banke, S.E.; et al. A phase 1/2 trial of an immune-modulatory vaccine against ido/pd-l1 in combination with nivolumab in metastatic melanoma. Nat. Med. 2021, 27, 2212–2223. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Clinicopathological Features | Case Number (%) |
|---|---|
| Age (n = 62) | |
| ≤65 | 39 (62.9) |
| >65 | 23 (37.1) |
| Gender (n = 62) | |
| Male | 46 (74.2) |
| Female | 16 (25.8) |
| Lauren’s classification (n = 62) | |
| intestinal type | 27 (43.5) |
| diffuse type | 13 (21) |
| mixed type | 13 (21) |
| NA | 9 (14.5) |
| TNM stage (n = 62) | |
| III | 9 (14.5) |
| IV | 53 (85.5) |
| Therapeutic line (n = 62) | |
| 1st | 36 (58.1) |
| 2nd | 11 (17.7) |
| ≥3rd | 15 (24.2) |
| Regimen (n = 62) | |
| ICI | 25 (40.3) |
| ICI + chemotherapy | 31 (50) |
| Double-ICI | 6 (9.7) |
| HER2 status (n = 62) | |
| Neg | 54 (87.1) |
| Pos | 3 (4.8) |
| NA | 5 (8.1) |
| MMR status (n = 62) | |
| MSS | 45 (72.6) |
| MSI | 10 (16.1) |
| NA | 7 (11.3) |
| PD-L1 status (n = 62) | |
| Neg | 21 (33.9) |
| Pos | 27 (43.5) |
| NA | 14 (22.6) |
| EBV status (n = 62) | |
| Neg | 49 (79) |
| Pos | 4 (6.5) |
| NA | 9 (14.5) |
| irAE status (n = 62) | |
| 0 | 27 (43.5) |
| 1 | 28 (45.2) |
| 2 | 6 (9.6) |
| 3 | 1 (1.6) |
| irAE organs (n = 35) | |
| skin | 14 (40) |
| digestive system | 10 (28.6) |
| hematopoietic system | 5 (14.3) |
| endocrine system | 3 (8.6) |
| respiratory system | 1 (2.9) |
| kidney | 1 (2.9) |
| bone and muscle | 1 (2.9) |
| Clinicopathological Features | irAE Case Number (%) | p Value | |
|---|---|---|---|
| NO | YES | ||
| total | 27 | 35 | |
| Age | 0.7913 | ||
| ≤65 | 16 (59.3) | 23 (65.7) | |
| >65 | 11 (40.7) | 12 (34.3) | |
| Gender | 1.0000 | ||
| Male | 20 (74.1) | 26 (74.3) | |
| Female | 7 (25.9) | 9 (25.7) | |
| Lauren’s classification | 0.2724 | ||
| intestinal type | 11 (40.7) | 16 (45.7) | |
| diffuse type | 7 (25.9) | 6 (17.1) | |
| mixed type | 3 (11.1) | 10 (28.6) | |
| NA | 6 (22.3) | 3 (8.6) | |
| TNM stage | 0.1604 | ||
| III | 6 (22.2) | 3 (8.6) | |
| IV | 21 (77.8) | 32 (91.4) | |
| Therapeutic line | 0.0608 | ||
| 1st | 15 (55.6) | 21 (60) | |
| 2nd | 8 (29.6) | 3 (8.6) | |
| ≥3rd | 4 (14.8) | 11 (31.4) | |
| Regimen | 0.0676 | ||
| ICI | 13 (48.1) | 12 (34.3) | |
| ICI + chemotherapy | 14 (51.9) | 17 (48.6) | |
| Double-ICI | 0 (0.0) | 6 (17.1) | |
| HER2 status | 0.5590 | ||
| Neg | 21 (77.8) | 33 (94.2) | |
| Pos | 2 (7.4) | 1 (2.9) | |
| NA | 4 (14.8) | 1 (2.9) | |
| MMR status | 0.1747 | ||
| MSS | 16 (59.2) | 29 (82.9) | |
| MSI | 6 (22.3) | 4 (11.4) | |
| NA | 5 (18.5) | 2 (5.7) | |
| PD-L1 status | 0.2369 | ||
| Neg | 6 (22.3) | 15 (42.9) | |
| Pos | 13 (48.1) | 14 (40) | |
| NA | 8 (29.6) | 6 (17.1) | |
| EBV status | 0.1238 | ||
| Neg | 23 (85.2) | 26 (74.3) | |
| Pos | 0 (0) | 4 (11.4) | |
| NA | 4 (14.8) | 5 (14.3) | |
| Clinicopathological Features | Case Number (%) |
|---|---|
| Age (n = 40) | |
| ≤65 | 20 (50) |
| >65 | 20 (50) |
| Gender (n = 40) | |
| Male | 27 (67.5) |
| Female | 13 (32.5) |
| Lauren’s classification (n = 40) | |
| intestinal type | 14 (35) |
| diffuse type | 6 (15) |
| mixed type | 12 (30) |
| NA | 8 (20) |
| Therapeutic line (n = 40) | |
| 1st | 25 (62.5) |
| 2nd | 8 (20) |
| ≥3rd | 7 (17.5) |
| Regimen (n = 40) | |
| ICI | 12 (30) |
| ICI + chemotherapy | 25 (62.5) |
| Double-ICI | 3 (7.5) |
| HER2 status (n = 40) | |
| Neg | 16 (40) |
| Pos | 1 (2.5) |
| NA | 23 (57.5) |
| MMR status (n = 40) | |
| MSS | 31 (77.5) |
| MSI | 8 (20) |
| NA | 1 (2.5) |
| PD-L1 status (n = 40) | |
| Neg | 7 (17.5) |
| Pos | 24 (60) |
| NA | 9 (22.5) |
| EBV status (n = 40) | |
| Neg | 36 (90) |
| Pos | 3 (7.5) |
| NA | 1 (2.5) |
| irAE status (n = 40) | |
| 0 | 27 (67.5) |
| 1 | 8 (20) |
| 2 | 4 (10) |
| 3 | 1 (2.5) |
| irAE organs (n = 13) | |
| skin | 6 (46.1) |
| digestive system | 2 (15.4) |
| hematopoietic system | 2 (15.4) |
| endocrine system | 2 (15.4) |
| respiratory system | 0 (0) |
| kidney | 0 (0) |
| bone and muscle | 1 (7.7) |
| Clinicopathological Features | irAE Case Number (%) | p Value | |
|---|---|---|---|
| NO | YES | ||
| total | 27 | 13 | |
| Age | 1.0000 | ||
| ≤65 | 14 (51.9) | 6 (46.2) | |
| >65 | 13 (48.1) | 7 (53.8) | |
| Gender | 0.1569 | ||
| Male | 16 (59.3) | 11 (84.6) | |
| Female | 11 (40.7) | 2 (15.4) | |
| Lauren’s classification | 0.2033 | ||
| intestinal type | 11 (40.7) | 3 (23.1) | |
| diffuse type | 5 (18.5) | 1 (7.7) | |
| mixed type | 6 (22.3) | 6 (46.1) | |
| NA | 5 (18.5) | 3 (23.1) | |
| Therapeutic line | 0.3415 | ||
| 1st | 15 (55.6) | 10 (76.9) | |
| 2nd | 7 (25.9) | 1 (7.7) | |
| ≥3rd | 5 (18.5) | 2 (15.4) | |
| Regimen | 0.0200 | ||
| ICI | 11 (40.7) | 1 (7.7) | |
| ICI + chemotherapy | 15 (55.6) | 10 (76.9) | |
| Double-ICI | 1 (3.7) | 2 (15.4) | |
| HER2 status | 1.0000 | ||
| Neg | 26 (96.3) | 13 (100) | |
| Pos | 1 (3.7) | 0 (0) | |
| NA | 0 (0) | 0 (0) | |
| MMR status | 0.2286 | ||
| MSS | 19 (70.4) | 12 (92.3) | |
| MSI | 7 (25.9) | 1 (7.7) | |
| NA | 1 (3.7) | 0 (0) | |
| PD-L1 status | 0.0152 | ||
| Neg | 18 (66.7) | 3 (23.1) | |
| Pos | 4 (14.8) | 6 (46.2) | |
| NA | 5 (18.5) | 4 (30.7) | |
| EBV status | 0.2532 | ||
| Neg | 25 (92.6) | 11 (84.6) | |
| Pos | 1 (3.7) | 2 (15.4) | |
| NA | 1 (3.7) | 0 (0) | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jiang, F.; Zhang, Z.; Chong, X.; Shen, L.; Fan, M.; Liu, X.; An, J.; Peng, Z.; Zhang, C. Extracellular Vesicle-Derived Protein File from Peripheral Blood Predicts Immune-Related Adverse Events in Gastric Cancer Patients Receiving Immunotherapy. Cancers 2022, 14, 4167. https://doi.org/10.3390/cancers14174167
Jiang F, Zhang Z, Chong X, Shen L, Fan M, Liu X, An J, Peng Z, Zhang C. Extracellular Vesicle-Derived Protein File from Peripheral Blood Predicts Immune-Related Adverse Events in Gastric Cancer Patients Receiving Immunotherapy. Cancers. 2022; 14(17):4167. https://doi.org/10.3390/cancers14174167
Chicago/Turabian StyleJiang, Fangli, Zhening Zhang, Xiaoyi Chong, Lin Shen, Meng Fan, Xuan Liu, Jin An, Zhi Peng, and Cheng Zhang. 2022. "Extracellular Vesicle-Derived Protein File from Peripheral Blood Predicts Immune-Related Adverse Events in Gastric Cancer Patients Receiving Immunotherapy" Cancers 14, no. 17: 4167. https://doi.org/10.3390/cancers14174167
APA StyleJiang, F., Zhang, Z., Chong, X., Shen, L., Fan, M., Liu, X., An, J., Peng, Z., & Zhang, C. (2022). Extracellular Vesicle-Derived Protein File from Peripheral Blood Predicts Immune-Related Adverse Events in Gastric Cancer Patients Receiving Immunotherapy. Cancers, 14(17), 4167. https://doi.org/10.3390/cancers14174167