Simple Summary
This is a scoping review of published literature on the usefulness of acupuncture-related therapies and herbal medicine in alleviating the side effects associated with breast cancer treatments. It is an important study given that the various treatment interventions for breast cancer, such as surgery, chemotherapy, radiotherapy, and hormone therapy, have unpleasant side effects that compromise the patient’s quality of life. The study revealed positive impact of some acupuncture-related therapies and herbal medicines in improving the symptoms and quality of life of patients with breast cancer. These findings will inform further studies on the economic impact of acupuncture and herbal medicines in the management of adverse events in patients on breast cancer treatment.
Abstract
The side effects associated with breast cancer treatments often reduce the patients’ quality of life. The effectiveness of acupuncture-related therapies and herbal medicine in managing the side effect is not fully understood. The study included clinical studies published in the 10 years since 2011 and analyzed the effectiveness of the therapies for managing side effects of anticancer treatment. The databases of MEDLINE via PubMed, CENTRAL, EMBASE, OASIS, and NSDL were searched. Thirty studies, including 13 (43.3%) randomized controlled trials (RCTs), 12 (40.0%) before-and-after studies, three (10.0%) case series, one (3.3%) case report, and one (3.3%) non-RCT, were included in this review. The main symptoms identified were aromatase inhibitors-induced arthralgia (AIA), lymphedema, and chemotherapy-induced peripheral neuropathy (CIPN). The types of acupuncture-related therapies applied included manual acupuncture, electro-acupuncture, moxibustion, and electro-moxibustion. In ten studies, eight herbal medications were administered. The Brief Pain Inventory-Short Form (BPI-SF) and Functional Assessment of Cancer Therapy-General (FACT-G) and -Breast (FACT-B) were frequently used to evaluate pain and QoL, respectively. Most studies suggested beneficial effects of acupuncture and herbal medicine on managing pain, daily function, and quality of life in patients going through AIA, CIPN, and/or lymphedema, with mild side effects. The scoping review implies the potential of CAM therapies as promising interventions for managing symptoms which otherwise lack alternative management options, and for improving the quality of life of breast cancer patients.
1. Introduction
Breast cancer is the most prevalent type of cancer and the leading cause of death among women, representing 13.8% of all cancer cases worldwide [1]. In 2018, 23,647 women were diagnosed with breast cancer in Korea, accounting for approximately 20.5% of all cancer incidence among Korean women [2]. Furthermore, in contrast with other types of cancer, such as cancer in the stomach, colon, and rectum, breast cancer incidence in Korea is constantly increasing, and the average annual percentage change is 5.4% [2]. One of the characteristics of breast cancer patients in Korea is the relatively younger age of the patients with an average of 50 years, which is approximately 10 years younger compared to the average age worldwide; in 2018, 13% of breast cancer patients in Korea were still in their 40s [3]. Moreover, the 5-year survival rate of Korean breast cancer patients was 93.3% in 2014–2018 [3,4]. Thus, breast cancer patients in Korea tend to be younger, with more than a 90% chance of 5-year survival, implying a higher rate of return to work (RTW) after or even during cancer treatments [5].
Nevertheless, the side effects of breast cancer treatments, such as surgery, chemotherapy, radiotherapy, and hormone therapy, are exceedingly common and have profound effects on the patients’ quality of life [6]. The symptoms due to cancer treatments include pain, fatigue, sleep disturbances, nausea, vomiting, and depression [7], and some symptoms specifically prevalent in breast cancer patients undergoing treatments include aromatase inhibitor-induced arthralgia (AIA); diarrhea, cough, neutropenia, and myalgia induced by monoclonal antibody therapy (e.g., trastuzumab) [8]; post-surgery symptoms, such as lymphedema [9] and post-mastectomy pain syndrome [10]; and menopausal symptoms such as hot flashes [11]. Recent studies indicate that the consistent use of aromatase inhibitors (AIs) increases the risk of osteoporosis. Many of these symptoms are not fully addressed in Western Medicine, which often leads to unmet needs in breast cancer patients, especially in relation to their health-related quality of life (HRQoL) [12]. Furthermore, the patients’ unmet needs may account for the high usage of complementary and alternative medicine (CAM) therapies, such as acupuncture-related therapies and herbal medicine, by breast cancer patients. Studies reported that approximately half of the patients diagnosed with cancer have experiences with CAM therapies, [13,14] with high levels of satisfaction reported [14].
Several studies have been conducted to examine the effectiveness of CAM therapies in the symptom management of breast cancer patients. Acupuncture and acupressure are suggested for reducing nausea and vomiting [15,16], vasomotor symptoms, such as hot flashes [17,18,19], and cancer-related fatigue [20,21,22]; mind–body therapies, such as meditation and yoga, are suggested for stress reduction and mood disorders [23,24,25]. Based on these findings, several clinical practice guidelines on the use of CAM therapies have been published and updated. A recently updated clinical practice guideline from the Society for Integrative Oncology discusses a variety of adjuvant CAM therapies available to breast cancer patients [25]. In this guideline, acupuncture for nausea and vomiting, hot flashes, and fatigue, and mind–body therapies for stress, anxiety, and depression were recommended; in contrast, ingested dietary supplements were not suggested. Acupuncture to relieve hot flashes was also recommended by the Breast Cancer Clinical Guidelines published by the Northern Cancer Alliance in the United Kingdom to complement the National Institute for Health and Care Excellence and Association of Breast Surgery guidelines [26]. However, many CAM therapies were graded C or D in existing guidelines due to the lack of sufficient evidence [25].
The question that remains to be answered upon examining previous studies is the effectiveness of CAM therapies in symptom management not yet reported in the clinical practice guidelines but still prevalent in breast cancer patients due to anticancer treatments. Although the management of these symptoms is not yet fully elucidated by clinical guidelines and previous studies, they have a strong impact on the patients’ quality of life, as well as on societal costs. A noteworthy update in recent studies is the investigation of the effectiveness of CAM therapies in post-surgery symptoms, such as lymphedema [27,28]; chemotherapy-induced neuropathic pain [29]; and muscle and joint pain due to endocrine therapy, such as AI-related arthralgia [30]. In this regard, the goal of this study is to collect all relevant data on the management of these symptoms using acupuncture-related therapies and herbal medicine and assess the effectiveness of these therapies.
This scoping review aims to provide an update on the efficacy of CAM therapies in symptoms commonly experienced by breast cancer patients associated with surgery and anticancer treatments with no sufficient management options. In this review, our focus is to identify how acupuncture-related therapies and herbal medicine are being used in relieving muscle and joint pain and lymphedema and assess their effectiveness in terms of symptom relief and improvement in HRQoL. The outcome measures used to measure pain and HRQoL, as well as the related results, were collected. Due to the paucity of related publications in the field of the research topic, this scoping review aims to cover two main interventions in CAM, namely acupuncture-related therapies and herbal medicine, at different levels of evidence collected from various types of clinical study designs.
2. Materials and Methods
A scoping review design was used to review the current status of studies on acupuncture-related treatments for symptom management and quality of life improvement of breast cancer patients. A scoping review is a method of knowledge synthesis that deals with exploratory research questions aiming to map major concepts, types of evidence, and gaps in research related to a defined area or field by systematically searching, collecting, and synthesizing existing knowledge [31]. This type of review helps researchers, clinical practitioners, and policymakers understand the current status of a particular research area and decide the direction for future research [32].
This study followed the method based on the Arksey and O’Malley framework [32], as well as the Preferred Reporting Items for Systematic Reviews and Meta-Analyses extension for scoping reviews (PRISMA-ScR) [33]. The following five steps were used to conduct this scoping review: (1) identification of the research question; (2) identification of relevant studies; (3) study selection; (4) charting of data; and (5) collecting, summarizing, and reporting the results.
2.1. Identifying the Research Questions
Prior to the initiation of this study, the broad research question was ‘how are acupuncture-related therapies and herbal medicine being used in relieving muscle and joint pain and lymphedema in breast cancer patients who underwent anticancer treatments?’
The more detailed research questions used after starting the study were as follows:
- What kind of research has been conducted?
- Which acupuncture-related therapies and herbal medicine types are mainly used?
- What were the main outcomes related to pain and quality of life?
- What were the results of the treatments?
- What is the level of evidence regarding the effectiveness of acupuncture-related therapies and herbal medicines?
2.2. Identifying the Relevant Studies
The following electronic databases were searched: MEDLINE via PubMed, the Cochrane Central Register of Controlled Trials (CENTRAL), Excerpta Medical dataBASE (EMBASE), Oriental Medicine Advanced Searching Integrated System (OASIS), and National Science Digital Library (NSDL). An example of the specific search strategy is listed in Table 1. Modifications to the search terms and search strategies may be adopted in reference to the database being searched. The initial search was limited to the time period between January 2011 and April 2021, as this scoping review aimed to provide an update on the use of adjuvant CAM therapies. However, the search period in scoping reviews may be subject to change if the collected studies are too few and the authors feel there is a lack of information from the retrieved results.

Table 1.
Search Strategy for PubMed.
2.3. Study Selection
Inclusion/Exclusion Criteria
Human studies including randomized controlled trials (RCTs), controlled clinical trials, case series, case reports, pilot clinical studies, and retrospective observational studies investigating the efficacy and safety of adjuvant acupuncture-related or herbal medicine-related therapies in breast cancer patients were reviewed. To reflect the purpose of this study, this review focused on studies published in the last 10 years, written in English. Existing guidelines, expert consensus papers, and existing qualitative studies focusing on the experience of breast cancer patients in using CAM therapies for the purpose of aforementioned symptom relief were not included in this scoping review; however, they were considered in analyzing the results of this scoping review as complementary information. In vivo and in vitro experiments, reviews, duplicate articles, ongoing studies, and studies that failed to provide detailed results or with incomplete data were also excluded. Table 2 presents elaborate selection criteria for this scoping review.
Table 2.
The selection criteria of studies for this scoping review.
The eligible participants were defined as breast cancer patients (1) over 18 years of age, (2) who were, or had been, going through anti-cancer therapy, such as breast cancer surgery (either mastectomy or lumpectomy), chemotherapy, immunotherapy, and/or endocrine therapy, and (3) who were experiencing post-surgery pain, neuropathic pain, joint pain, or lymphedema due to anti-cancer therapy. Patients experiencing other types of side effects, such as nausea, vomiting, and hot flashes, were excluded from this scoping review. In addition, clinical studies focusing on the antitumor abilities of acupuncture-related therapies and herbal medicine were not within the scope of this review and were excluded. No restriction was applied on sex, ethnicity, symptom severity, cancer stage, disease duration, clinical setting, and country of study.
Although the definition of CAM therapy may somewhat vary depending on the health care system of each country or the perspective of CAM, this scoping review focused on the interventional role of acupuncture-related therapies and herbal medicine-related therapies utilized by patients as adjuvant therapy to conventional treatments. These CAM therapies included: Traditional East Asian Medicine therapies, such as acupuncture, acupressure, electro-acupuncture, laser acupuncture, massage, and herbal medicine, as described in individual studies. CAM treatments, such as vitamin supplements; mindfulness therapies, such as meditation; and yoga were excluded after thorough discussions among the authors regarding the aim and scope of this review. No limitations were applied to the frequency, dosage, and duration of treatments.
Some examples of the outcomes within the scope of this review include self-reported pain severity; cancer-specific inventory, such as Functional Assessment of Cancer Therapy-Breast (FACT-B), scores; length of hospital stay; patient satisfaction; depression assessment instrument, such as Beck’s Depression Inventory (BDI), scores; absolute circumference or relative volume change of the arm, range of motion (ROM); dosage of painkillers; costs and health-related quality of life assessment tool, such as Short Form (SF)-12, SF-36, and EQ5D, scores. All the outcomes reported in the included studies were listed and mapped during the review process. For example, adjuvant CAM therapies may not be helpful in reducing the absolute circumference of the arm in breast cancer patients suffering from lymphedema, but they might show beneficial effects on HRQoL. Such conflicting results might indicate no benefit from the practitioner’s perspective but imply some benefit from the perspective of the patient facing RTW.
Another dimension that requires attention is the paucity of sufficient measures to address the needs of breast cancer patients. While the anti-cancer treatment regimen of breast cancer is well-designed and presented in the forms of guidelines and clinical pathways, management of side effects of these anticancer therapies is often dealt with limited options. CAM interventions may confer therapeutic effects that are different from those of conventional anti-cancer treatments or usual care. This scoping review assessed the types of outcome indicators to analyze the effects of CAM interventions in the management of side effects. This may also account for the limitations faced by many clinical studies on breast cancer patients using CAM therapies, and the lack of sufficient or proper controls. As this scoping review aims to assess adjuvant CAM therapies, the controls used in clinical studies to compare the effectiveness were assessed with particular interest.
2.4. Screening and Agreement
Two authors (G.H. and H.J.J.), who were reviewers trained in the process and purpose of the study, independently searched the electronic databases using the search strategies described above and screened the retrieved studies for eligibility. Upon initial search, all citations were uploaded to EndNote X20 (Clarivate Analytics, Philadelphia, PA, USA). After removing the duplicates, full texts were reviewed in detail against the inclusion criteria. The number of results for each database search was noted and presented in a PRISMA flow diagram. The reasons for excluding studies were recorded for individual studies. All disagreements were resolved by consulting an independent reviewer (Y.-S.L.).
2.5. Charting the Data
Study information assessed for this review are as follows: the first author, corresponding author, publication year, country, language, study type, study aim, study population and sample size, patient characteristics (e.g., age, sex, breast cancer stage), surgery history, anti-cancer therapy history, type and cycle of current anti-cancer therapy, randomization method (if applicable), blinding method (if applicable), interventions (type of treatment, number and dosage of administration), type, number and dosage of comparison (if applicable), treatment period, outcome measures, primary outcome, secondary outcome, and statistical analysis method. The third author ((Y.-S.L.) reviewed and confirmed the data extraction process. Any disagreements during the data extraction process were reconciled through discussion or through consulting a fourth author (S.-Y.K.). The data charting table was modified as necessary during the process of data extraction.
2.6. Collecting, Summarising, and Reporting the Results
After coding the included studies, the contents of the studies were analyzed. The extracted data were presented in tabular form in line with the objective of this scoping review. The distribution of the studies by the aforementioned extracted information was analyzed. A qualitative analysis was conducted to illustrate an overview of each study. The tabulated results were supported by narrative summaries to describe the results in relation to the objective of this scoping review.
3. Results
3.1. Literature Search and Selection Process
A total of 1491 studies published between January 2011 and April 2021 were identified. Through the literature selection process, 30 studies were finally selected [29,34,35,36,37,38,39,40,41,42,43,44,45,46,47,48,49,50,51,52,53,54,55,56,57,58,59,60,61,62] (Figure 1). Table 3 summarizes the general characteristics of the included studies. Sixty-four duplicate articles were excluded. Additionally, 1397 studies were excluded based on their titles and abstracts, as they were not related to acupuncture-related therapies for breast cancer, they were not conducted in vivo or in vitro, or they focused on other diseases in patients with breast cancer. Studies without complete results, such as RCT protocols, letters, correspondence, conference abstracts, or RCT protocols, were also excluded. The PRISMA flow chart was used to track the number of articles at each stage of the review. Table 4 elaborates the studies included in this review.
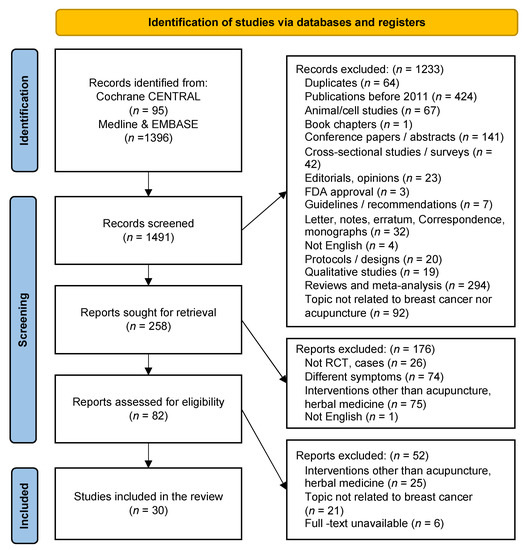
Figure 1.
Study Flow Chart.
Table 3.
General characteristics of the final included studies (n = 30).
Table 4.
Summary of included studies.
3.2. General Characteristics of the Identified Literature
3.2.1. Publication Year
Except for the year 2012, research has been carried out steadily since 2011. The largest number of studies (seven articles) was published in 2018.
3.2.2. Study Design Types
The 30 studies included experimental studies and observational studies. Among the experimental studies, there were 12 before-and-after studies, 13 RCTs, and one non-RCT. Among the observational studies, there were three case reports and one case series (Table 3).
3.2.3. Research Regions
Most studies were conducted in the USA (n = 13), followed by China (n = 7), Korea (n = 4), Japan (n = 1), Taiwan (n = 1), Switzerland (n = 1), Israel (n= 1), Brazil (n = 1), and Armenia (n = 1) (Table 4).
3.3. Characteristics of Study Participants
3.3.1. Participants
A total of 2005 participants were enrolled in the included studies (Table 5). The number of participants in RCTs/non-RCTs or before-and-after studies was 2000. Five patients were the subjects of a case report and three case series. All patients included in this review were female, and no male patients were enrolled in any of the included studies. The age range of patients varied, and only six studies mentioned the duration of breast cancer.
Table 5.
Demographic and clinical characteristics of patients.
The number of articles focusing on patients with AI-induced side effects was the highest. In addition, there were studies focusing on lymphedema, post-mastectomy syndrome, and chemotherapy-induced peripheral neuropathy (CIPN) (Table 5).
3.3.2. Type of Anti-Cancer Treatments Received by the Patients
Among the articles dealing with the AI-induced side effects, the patients received adjuvant hormonal therapy, such as tamoxifen, anastrozole, letrozole, and exemestane. The patients underwent surgery, chemotherapy, and/or radiotherapy prior to hormonal treatments.
In the studies focusing on patients experiencing breast-surgery-related pain, the patients received total mastectomy, modified radical mastectomy, quadrantectomy, and/or breast-conserving surgery. In addition, the patients in the other studies underwent chemotherapy, such as taxane, oxaliplatin, docetaxel, and paclitaxel administration.
3.3.3. Main Symptoms of Patients
The main clinical symptoms presented in the included articles identified musculoskeletal symptoms (arthralgia and/or stiffness and/or swelling in one or more joints, bone pain, myalgia, carpal tunnel syndrome, trigger finger), lymphedema, neuropathy, post-mastectomy pain syndrome (shoulder and chest wall), fatigue, psychological distress (anxiety, depression), insomnia, vasomotor symptoms (hot flushes and sweating), atypical genital bleeding from vaginal mucosa, sexual dysfunction (vaginal dryness, dyspareunia), mucosal dryness, nausea, vomiting, coping, pruritus, dizziness, and headache (Table 5).
3.4. Treatment Details
3.4.1. Acupuncture-Related Treatments
Among the included studies, the number of acupuncture-related articles was 20 (67%). The type of acupuncture-related therapies, such as manual acupuncture (MA), electro-acupuncture (EA), moxibustion, electro-moxibustion, transcutaneous electrical acupoint stimulation (TEAS), contact needle therapy, and auricular acupuncture (AA), varied. There were 10 studies using only MA [43,44,45,49,50,51,52,54,57,59], four studies using only EA [36,37,52,55], one study using MA and EA [29,42], one study using herbal medicine and MA [59], and one study using MA, EA, and AA together [42]. In the study by Lin [60], AA, MA, TENS, and Silver Spike Point therapy were used together. In addition, moxibustion [47], electro-moxibustion [48], and bloodletting puncture and cupping [46] were used in one study each.
All studies except two [52,59] reported the selection of acupoints. Acupoints are specifically chosen sites for acupuncture manipulation according to theories of traditional medicine. A total of 114 acupoints were reported, and the acupoint mostly used was ST36. The acupoints used more than thrice were LI11, LI4, LR3, LI15, SP6, SP9, GV20, KI7, BL60, CV12, CV3, GB21, GB34, LR8, LU5, PC6, SP10, and Baxie. In addition, Ah shi points were also used. Details of acupoints used for each symptom are shown in Table 6.
Table 6.
Summary of the intervention (acupuncture-related therapies) in the included studies.
3.4.2. Herbal Medicine
In 10 of the C, including Sipjeondaebo-tang [34] (Juzentaihoto in Japanese, Shi Quan Da Bu decoction in Chinese), aconitine root [34], oral medication containing Lens culinaris lectin [35], tiger bone powder [39], Ikshingungol granules (Ekijingenkotsu in Japanese, Yi Shen Jian Gu in Chinese) [40,41], black cohosh (Cimicifuga racemosa) extracts [58], Ikkiyangeumheadok-tang (Ekkiyouingedokuto in Japanese, Yiqi Yangyin Jiedu decoction in Chinese) [59], and curcumin [62]. The type of herbal medicine used included decoction, powder, and granules. Sipjeondaebo-tang was composed of Astragali radix, Cinnamomi cortex, Angelicae radix, Paeoniae radix, Cnidii rhizoma, Rehmanniae radix, Ginseng radix, Atractylodis lanceae rhizome, Poria, and Glycyrrhizae radix. Ikshingungolhwan (Yi Shen Jian Gu granules) was used both in an RCT [40] and a before-and-after study [41] and was composed of Radix rehmanniae Preparata, Fructus Corni, Semen cuscutae, Radix Achyranthis Bidentatae, Cyperi rhizoma, Angelicae Sinensis radix, Poria, Paeoniae Alba radix, Chuanxiong rhizoma, Corydalis rhizoma, and Phryma leptostachya. Ikkiyangeumheadok-tang is composed of Astragali radix, Codonopsis pilosula, Poria cocos, Glehnia littoralis, Curcuma phaeocaulis, Pelodiscus sinensis, Tulipa edulis, Corydalis remota, Dendrobium moniliforme, Ponciri Fructus Immaturus, Trichosanthes kirilowii, and Polygonum multiflorum [59]. A total of 31 herbal ingredients were used for the prescriptions stated above, and the most used ingredient was Poria cocos (three times).
3.5. Control
A control group was included in 13 controlled studies and the types of control used were placebo, sham acupuncture, waitlist, usual care, exercise, and kinesiotherapy. Three studies used sham needle as control, two studies used both waitlist and sham controls, two studies used only waitlist control, and three studies used placebo medications as the control.
3.6. Evaluation Tools
The main focus of this study was to evaluate the improvement in pain and HRQoL. To evaluate the pain, the Brief Pain Inventory Short Form (BPI-SF) [29,36,40,41,55], Western Ontario and McMaster Universities Osteoarthritis Index [36,40,41], BPI [38], Visual Analog Scale (VAS) [39,46,47,49,50,53], modified BPI (M-BPI) [39], modified Score for the Assessment of Chronic Rheumatoid Affections of the Hands (M-SACRAH) [41], Numerical rating scale (NRS) [42,52,54], shoulder ROM tool [42,48], Neuropathic Pain Scale (NPS) [55], Disabilities of the Arm, Shoulder, and Hand (DASH) questionnaire [51] were used.
FACT-General (FACT-G) [36], M-SACRAH [40,41], FACT-B [39,40,41], European Organization for Research and Treatment of Cancer Breast Cancer-Specific Quality of Life Questionnaire (EORCT QLQ-BR23) [42,48], Measure Yourself Medical Outcome Profile 2 [42], ‘Was it Worth it?’ questionnaire [42,50], FACT-Taxane [55], 36-Item SF (SF-36) health survey [57], Edmonton Symptom Assessment Scale (ESAS) [59], SF-12 health survey [60], EORTC quality of life questionnaire (QLQ) [62], and EORTC Cancer Quality of Life Questionnaire Core (QLQ-C30 version 1.0) [62] were used to evaluate the quality of life.
In addition, the Common Terminology Criteria for Adverse Events (CTCAE) [54,56], Functional Assessment of Cancer Therapy/Gynecologic Oncology Group-Neurotoxicity (FACT/GOG-NTX) scale [54,56], FACT-Neurotoxicity scale [29,55], Neuropathic Pain Symptom Inventory (NPSI) [57], Nerve Conduction Study [57] test results, and Patient Neurotoxicity Questionnaire (PNQ) [29] were used to assess the degree of CIPN.
As for assessing fatigue, the Brief Fatigue Inventory [37], Functional Assessment of Chronic Illness Therapy-Fatigue [42], and revised Piper Fatigue Scale [47] were utilized. In the studies treating lymphedema [33,34,35,36,38,44,45,48], the arm circumference and VAS for swelling were used to measure the improvement in lymphedema. To evaluate the vasomotor symptoms after anti-estrogen therapy, a hot flush symptom diary (severity and frequency) and the Menopause Rating Scale were used [42,58]. In addition, the Pittsburgh Sleep Quality Index [39,42] and the Women’s Health Initiative Insomnia Rating Scale [42] were used for evaluating insomnia. The Hospital Anxiety and Depression Scale [37], VAS [50], and NRS [52] were used to evaluate anxiety. Another study assessed depression by using BDI [51]. In the study [42] by Kim et al., Female Sexual Function Index, Female Sexual Distress Scale, and Arizona Sexual Experiences Scale were used to evaluate sexual dysfunction [42]. In the article by Quinlan-Woodward et al., the NRS was used to evaluate nausea and the ability to cope [52].
Studies also examined changes in serum estradiol and follicle-stimulating hormone levels [39]; bone mineral density [40,41]; blood indices, such as calcium, phosphate, and alkaline phosphatase [41]; cytokine assays (interleukin [IL]-2, IL-4, interferon gamma) [53]; and brain-derived neurotrophic factor, carcinoembryonic antigen, and cancer antigen 15-3 levels. Additionally, the Measure Yourself Concerns and Wellbeing questionnaire (MYCaW) [59], Response Evaluation Criteria in Solid Tumors [62], Eastern Cooperative Oncology Group performance status [62], biothesiometer assessment [55], grooved pegboard test [55], and vibration sensation test [56] were used.
3.7. Treatment Effects
- Acupuncture-related therapies
The pain analyzed in this review was divided into two types: post-mastectomy pain and AI-induced pain. The post-surgical pain was evaluated in one case report, two before-and-after studies focusing on acupuncture [49,50,52], and one RCT focusing on TEAS [53]. Three studies used VAS for assessing postoperative pain [49,50,53], and one study used the NRS for assessing post-mastectomy pain [52]. All four studies reported that postoperative pain improved after acupuncture or TEAS. BPI was utilized for the measurement of AI-induced pain in two RCTs [36,38] and one before-and-after study [42]. There were improvements reported in two of the studies [38,42], whereas no significant difference was demonstrated in the before-and-after study [36].
In contrast, various tools, such as FACT-G [36], EORTC-QLQ [42], SF-36 [57], SF-12 [60], and FACT/GOG-NTX [56], were used in five studies to measure the QoL of patients treated with acupuncture. There were improvements in the aspect of QoL in three studies [42,57,60], whereas there was no significant improvement in one RCT [42] and one before-and-after study [56].
Seven studies compared the arm circumference of patients presenting with lymphedema including three before-and-after studies [41,43,48], one non-RCT [46], and three RCTs [45,47,51]. All studies utilized acupuncture-related therapies for the treatment of lymphedema. In the three before-and-after studies, there was an improvement in the arm circumference after acupuncture [43,44] and electro-moxibustion treatment relatively [48]. In the RCT [45] conducted by Bao et al., acupuncture treatment did not significantly reduce breast cancer treatment-related lymphedema in pre-treated patients receiving concurrent lymphedema treatment, as there was no significant difference between the acupuncture and waitlist group regarding arm circumference or bioimpedance. The remaining RCTs reported that moxibustion [47] and acupuncture with kinesiotherapy [51] significantly decreased arm circumference relatively. In the study [46] by Wang et al., bloodletting puncture and cupping significantly reduced the circumference of the affected arm, and the reduction of arm circumference mainly occurred in the region extending from the wrist crease to 10 cm distal to the wrist crease.
Five studies focused on CIPN, including three before-and-after studies and two RCTs [29,54,55,56,57]. Among these five studies, neuropathic pain was evaluated using the BPI, National Cancer Institute-CTCAE, NPS, NPSI, and PNQ. Except for one before-and-after study [55], the symptoms of CIPN improved after receiving acupuncture-related therapies as reported in one RCT and three before-and-after studies [29,54,56,57].
In terms of CIPN-related QoL evaluation, FACT/GOG-NTX was used in one study by Ogawa et al.; they reported that all patients showed improvement in the FACT/GOG-NTX score after contact needle therapy [54].
- 2.
- Herbal medicine
Three studies, including two RCTs [39,40] and one before-and-after study [41], using herbal medicine as intervention compared BPI scores to measure the AIA of patients. These studies presented data showing an improvement in average pain levels, including the degree of worst pain and pain interference.
FACT-B scores were calculated in three studies, including two RCTs [39,40] and one before-and-after study [41], to evaluate the QoL of patients. There were improvements in the aspect of physical well-being and functional well-being in all these studies. However, no significant differences were observed in the FACT-B social/family, emotional, and additional concern subscales in one before-and-after study [41]. In the RCT conducted by Saghatelyan et al., there was no significant difference between the groups in terms of EORTC-QLQ scores [62].
In the case report by Chino et al., a patient with AI-induced atypical genital bleeding and arthralgia was treated with Sipjeondaebo-tang (Juzentaihoto in Japanese, Shi Quan Da Bu decoction in Chinese) and aconitine root [34]. The atypical bleeding and arthralgia disappeared after taking herbal medicines for 5 weeks and 5 months, respectively. However, when the patient discontinued taking herbal medicine, atypical bleeding recurred. Therefore, the patient continued taking the herbal medicine for 2 years without any signs of side effects. In another case report by Zhu, the patient experienced relief from bone pain with improved appetite and gained 11 kg in weight after 8 years of Yiqi Yangyin Jiedu decoction treatments [61]. Another before-and-after study reported that herbal medicine (Lens culinaris lectin) improved arthralgia and mucosal dryness [35].
- 3.
- Acupuncture combined with herbal medicine
In the case report by Ben-Arye et al., there were improvements in clinical symptoms, such as fatigue, nausea, anxiety, drowsiness, dyspnea, appetite, sleep, well-being, headache, and hot flashes, measured using ESAS and MYCaW [59].
- 4.
- Safety
Adverse events (AEs) were reported in thirteen studies. In the before-and-after study by Beuth et al., adverse reactions, such as nausea and bloating, were documented [35]. In the RCT conducted by Mao et al., despite needle placement in the same arm as breast cancer surgery, there were no cases of infection or worsening of lymphedema in the EA or SA groups. However, 18 related AEs were reported by eight participants in both groups. Most AEs reported in the EA group, such as tingling and numbness, were related to the “De Qi” sensation experienced during the acupuncture process [38]. In the study by Li et al., six participants reported stomach discomfort, but the symptoms were tolerable [39]. In the study by Peng et al., 14 participants among those receiving Yi Shen Jian Gu granules reported AEs and 16 participants among those receiving placebo granules [40] reported AEs. In the study by Zhang et al., six out of 30 participants reported AEs, such as mild epigastric discomfort, heartburn, hiccup, and mild diarrhoea [41]. In the study by Kim et al., there were six minor self-limiting AEs, such as subcutaneous bleeding and needle pain [42]. In the before-and-after study by Cassileth et al., 12 out of 33 patients reported mild bruising or minor pain/tingling in the arm, shoulder, or acupuncture site at least once. However, there was a transient increase in lymphedema in the axilla of the lymphedematous arm in one patient [43]. In the study by Bao et al., treatment-related AEs, such as bruising, hematoma, and pain, were reported in participants who received acupuncture [45]. In the study by Han et al., one serious AE and six AEs were reported during the trial, but most AEs were irrelevant to the intervention [48]. In the study by Bauml, acupuncture needle site reaction with discomfort, minor swelling, and bruising after acupuncture needle withdrawal was reported [49]. In the study by Bao et al., there were four AEs among 27 patients, concerning mild bruising [56]. In the study by Lu et al., two participants reported mild AEs, such as pruritis in the feet and joint pain [29]. In the study by Rostock, only one AE (nausea) possibly related to the study medication was reported [58].
In contrast, no AEs were reported in seven studies, while the remaining 10 studies did not mention adverse reactions.
4. Discussion
This study was conducted to explore the current status of research related to acupuncture-related treatment and herbal medicine treatment in patients with breast cancer through a scoping review. The ultimate aim of this scoping review was to gather information on the use of adjuvant acupuncture-related therapies and herbal medicine to relieve symptoms, particularly pain and lymphedema, caused by ongoing or completed anticancer treatments and assess the effectiveness of acupuncture-related therapies and herbal medicine. The analysis was conducted based on the following five criteria: (1) Types of research conducted; (2) Types of acupuncture-related therapies and herbal medicine applied; (3) Reported outcomes related to pain and quality of life of breast cancer patients; (4) Effectiveness of the CAM treatments employed; (5) The level of evidence regarding the effectiveness of acupuncture-related therapies and herbal medicines.
4.1. Main Findings
A total of 30 studies focusing on acupuncture-related therapies and herbal medicine were identified. Studies have been carried out steadily since 2011, culminating in 13 (43.3%) RCTs, 12 (40.0%) before-and-after studies, three (10.0%) case series, one (3.3%) case report, and one (3.3%) non-RCT, with the RCT being the main type of the studies included. The studies analyzed included a total of 2005 female patients presenting with 44 symptoms, such as post-operative chest and/or shoulder pain, arthralgia, lymphedema, neuropathy, vasomotor symptoms, insomnia, anxiety, depression, and sexual dysfunction.
The type of anti-cancer treatments the patients received varied. First, in the studies focusing on postoperative pain, the patients underwent total mastectomy, modified radical mastectomy, quadrantectomy, and/or breast-conserving surgery. The patients received adjuvant hormonal therapy, such as tamoxifen, anastrozole, letrozole, and exemestane, in the studies about AI-induced side effects. The patients in the remaining studies also underwent chemotherapy, such as taxane, oxaliplatin, docetaxel, and paclitaxel.
The treatments analyzed in this scoping review were divided into two main categories: acupuncture-related therapies and herbal medicine. The proportion of acupuncture-related articles was 67%. The type of acupuncture-related therapies included MA, EA, moxibustion, electro-moxibustion, TEAS, contact needle therapy, and AA. A total of 114 acupoints were utilized, and the most frequently used acupoint was ST36. On the other hand, there were 10 studies on herbal medicine among the 30 studies. Eight herbal medicines were administered, including Sipjeondaebo-tang (Juzentaihoto in Japanese, Shi Quan Da Bu Wan in Chinese), aconitine root, oral medication containing Lens culinaris lectin, tiger bone powder, Ikshingungol granules (Ekijingenkotsu in Japanese, Yi Shen Jian Gu in Chinese), black cohosh (Cimicifuga racemosa) extracts, Ikkiyangeumheadok-tang (Ekkiyouingedokuto in Japanese, Yiqi Yangyin Jiedu tang in Chinese), and curcumin. The types of herbal medicine included decoction, powder, and granules. The aforementioned treatments were administered to breast cancer patients to manage adverse effects from cancer treatments and were not directly involved in anticancer treatments.
Thirteen of the studies included in the review reported adverse events. Seven studies reported no harmful effects, while the remaining 10 studies made no mention of adverse effects. Acupuncture was associated with needle pain, tingling and numbness, subcutaneous hemorrhage, bruising, and mild swelling. Despite the fact that acupuncture treatment for lymphedema was declared safe even in the arm where axillary dissection was performed, one adverse event (AE) warrants caution, since a transient increase in lymphedema was noted, though it resolved quickly. AEs due to herbal medicine were nausea, stomach discomfort, heartburn, hiccup, and mild diarrhoea, most of which were tolerable. In summary, the AEs from complementary therapies of acupuncture and herbal medicine were associated with mild side effects, and in general, safe.
Thirteen RCTs presented a range of control groups, including placebo medications, sham acupuncture, waitlist, usual care, exercise, and kinesiotherapy. There were three studies that used a sham needle as the control, two studies that used both a waitlist and a sham needle as the control, two studies that used only a waitlist as the control, and three studies that used placebo medications as the control. Due to the lack of therapy alternatives for cancer treatment side effects, physicians and patients seeking further support in symptom management may take into account the efficacy of CAM therapies compared to standard care and waitlist. However, verum acupuncture treatment failed to demonstrate superior efficacy compared to active controls such as sham acupuncture in many studies; additional research is still necessary to determine the efficacy of CAM therapies in comparison to sham controls.
Various methods were available for the measurement of the effectiveness of adjuvant therapies to manage AIA, lymphedema, HRQoL, and CIPN. The nature of the outcomes that these methods measure may depend on what the patient or practitioner considers important. Among the patient-reported outcomes (PROs), unidimensional measures such as VAS and NRS, as well as BPI-SF help perceive pain severity intuitively; other PROs such as FACT-G and FACT-B help understand the patient’s functional abilities, and SF-12 helps assess the patient’s quality of life. Outcomes other than PROs include arm circumference, which is an outcome commonly used for lymphedema, and which interestingly was reduced in a number of studies by CAM therapies. On the other hand, levels of E2 and FSH, as well as BMD were not altered by herbal medicine, while symptoms such as arthralgia and AI-induced pain were significantly reduced in the same studies.
4.2. Limitations of This Analysis
Our study has two main limitations. First, the definition of intervention is somewhat ambiguous. During the searching stage, we used the search term ‘CAM’. However, we limited the search regarding interventions to acupuncture-related therapies and herbal medicine according to our inclusion criteria in the screening stage. Further reviews with broader scope of CAM therapies may be necessary (ex. Vitamin supplements) to include therapies often used by cancer patients. Second, we did not include the Chinese database, CNKI, which may have led to us missing some studies suitable for this scoping review. Additional studies focusing on the studies in the Chinese database would enable a deeper understanding on the interventions used in mainland China as well as their effectiveness.
5. Conclusions
5.1. Implications for Research
The results of this study indicate the potential efficacy of acupuncture-related therapies and herbal products for the symptom management of breast cancer patients. Although the level of effectiveness varied between trials, pain management and lymphedema management were demonstrated to be effective across a range of outcome measures. Side effects were generally mild and often not related to the treatments. Further studies are warranted to explore the efficacy of the aforementioned treatments in a larger sample.
The case reports and case series identified in this review provides a summary of data on the effect of acupuncture-related therapies and herbal medicine on symptom management in breast cancer patients. In addition, existing pilot before-and-after studies and RCTs included in the current scoping review indicate that this research area is continuing to develop. Unfortunately, economic data were not included in this scoping review. Studies that focus on the economic data of acupuncture-related therapies and herbal medicine should be conducted in the future.
5.2. Implications for Practice
The most important aspect of breast cancer treatment in a Korean Medicine hospital is the management of adverse effects from standard therapies such as chemotherapy, surgery, and radiation. In actual clinical settings, patients’ satisfaction with Korean medicine treatment has been observed to be high. In this review, we demonstrated that acupuncture-related therapies and herbal medicines had promising effects on the symptoms and QoL of breast cancer patients. As stated previously, this outcome is congruent with clinical practice.
In clinical practice, however, patients with lymphedema following breast cancer surgery frequently fear needle insertion in the arm on the side of the surgery site. In this context, the research included in this review demonstrates that acupuncture is a safe and effective treatment option for lymphedema.
Author Contributions
Conceptualization, G.H., H.J.J., S.-Y.K. and Y.-S.L.; Data curation, Y.J.L. and Y.-S.L.; Formal analysis, G.H., H.J.J., S.-Y.K. and Y.-S.L.; Writing—original draft, G.H., H.J.J. and Y.-S.L.; Writing—review and editing, Y.J.L., I.-H.H., S.-Y.K. and Y.-S.L.; Funding acquisition, Y.-S.L.; Study administration, Y.-S.L.; All authors have read and agreed to the published version of the manuscript.
Funding
This research was s supported by a grant of the Korea Health Technology R&D Project through the Korea Health Industry Development Institute (KHIDI), funded by the Ministry of Health & Welfare, Republic of Korea (grant number: HF20C0222, Recipient: Y.-S.L.).
Conflicts of Interest
The authors declare no conflict of interest.
References
- Azamjah, N.; Soltan-Zadeh, Y.; Zayeri, F. Global Trend of Breast Cancer Mortality Rate: A 25-Year Study. Asian Pac. J. Cancer Prev. 2019, 20, 2015–2020. [Google Scholar] [CrossRef] [PubMed]
- Korea Central Cancer Registry, N.C.C. Annual Report of Cancer Statistics in Korea in 2018; Ministry of Health and Welfare: Seoul, Korea, 2020.
- Hyang-Ha, C.; Hwa-Jeong, S. The Risk of Breast Cancer in Women in Their 40s by Economic Activity. J. Radiol. Sci. Technol. 2020, 43, 23–27. [Google Scholar]
- Kang, S.Y.; Kim, Y.S.; Kim, Z.; Kim, H.Y.; Kim, H.J.; Park, S.; Bae, S.Y.; Yoon, K.H.; Lee, S.B.; Lee, S.K.; et al. Breast Cancer Statistics in Korea in 2017: Data from a Breast Cancer Registry. J. Breast Cancer 2020, 23, 115–128. [Google Scholar] [CrossRef]
- Campagna, M.; Loscerbo, R.; Pilia, I.; Meloni, F. Return to Work of Breast Cancer Survivors: Perspectives and Challenges for Occupational Physicians. Cancers 2020, 12, 355. [Google Scholar] [CrossRef] [PubMed]
- Rosenberg, S.M.; Stanton, A.L.; Petrie, K.J.; Partridge, A.H. Symptoms and Symptom Attribution Among Women on Endocrine Therapy for Breast Cancer. Oncologist 2015, 20, 598–604. [Google Scholar] [CrossRef]
- Kwekkeboom, K.L. Cancer Symptom Cluster Management. Semin. Oncol. Nurs. 2016, 32, 373–382. [Google Scholar] [CrossRef]
- Cameron, D.; Piccart-Gebhart, M.J.; Gelber, R.D.; Procter, M.; Goldhirsch, A.; de Azambuja, E.; Castro, G., Jr.; Untch, M.; Smith, I.; Gianni, L.; et al. 11 years’ follow-up of trastuzumab after adjuvant chemotherapy in HER2-positive early breast cancer: Final analysis of the HERceptin Adjuvant (HERA) trial. Lancet 2017, 389, 1195–1205. [Google Scholar] [CrossRef]
- Zhang, X.; Oliveri, J.M.; Paskett, E.D. Features, Predictors, and Treatment of Breast Cancer-related Lymphedema. Curr. Breast Cancer Rep. 2020, 12, 244–254. [Google Scholar] [CrossRef]
- Chappell, A.G.; Bai, J.; Yuksel, S.; Ellis, M.F. Post-Mastectomy Pain Syndrome: Defining Perioperative Etiologies to Guide New Methods of Prevention for Plastic Surgeons. World J. Plast. Surg. 2020, 9, 247–253. [Google Scholar] [CrossRef]
- Santen, R.J.; Stuenkel, C.A.; Davis, S.R.; Pinkerton, J.V.; Gompel, A.; Lumsden, M.A. Managing Menopausal Symptoms and Associated Clinical Issues in Breast Cancer Survivors. J. Clin. Endocrinol. Metab. 2017, 102, 3647–3661. [Google Scholar] [CrossRef]
- Ho, P.J.; Gernaat, S.A.M.; Hartman, M.; Verkooijen, H.M. Health-related quality of life in Asian patients with breast cancer: A systematic review. BMJ Open 2018, 8, e020512. [Google Scholar] [CrossRef] [PubMed]
- Buckner, C.A.; Lafrenie, R.M.; Denommee, J.A.; Caswell, J.M.; Want, D.A. Complementary and alternative medicine use in patients before and after a cancer diagnosis. Curr. Oncol. 2018, 25, e275–e281. [Google Scholar] [CrossRef] [PubMed]
- Molassiotis, A.; Scott, J.A.; Kearney, N.; Pud, D.; Magri, M.; Selvekerova, S.; Bruyns, I.; Fernadez-Ortega, P.; Panteli, V.; Margulies, A.; et al. Complementary and alternative medicine use in breast cancer patients in Europe. Support Care Cancer 2006, 14, 260–267. [Google Scholar] [CrossRef] [PubMed]
- Collins, K.B.; Thomas, D.J. Acupuncture and acupressure for the management of chemotherapy-induced nausea and vomiting. J. Am. Acad. Nurse Pract. 2004, 16, 76–80. [Google Scholar] [CrossRef] [PubMed]
- Yang, Y.; Zhang, Y.; Jing, N.C.; Lu, Y.; Xiao, H.Y.; Xu, G.L.; Wang, X.G.; Wang, L.M.; Zhang, Y.M.; Zhang, D.J.; et al. Electroacupuncture at Zusanli (ST 36) for treatment of nausea and vomiting caused by the chemotherapy of the malignant tumor: A multicentral randomized controlled trial. Zhongguo Zhen Jiu 2009, 29, 955–958. [Google Scholar]
- Deng, G.; Vickers, A.; Yeung, S.; D’Andrea, G.M.; Xiao, H.; Heerdt, A.S.; Sugarman, S.; Troso-Sandoval, T.; Seidman, A.D.; Hudis, C.A.; et al. Randomized, controlled trial of acupuncture for the treatment of hot flashes in breast cancer patients. J. Clin. Oncol. 2007, 25, 5584–5590. [Google Scholar] [CrossRef]
- Frisk, J.; Carlhall, S.; Kallstrom, A.C.; Lindh-Astrand, L.; Malmstrom, A.; Hammar, M. Long-term follow-up of acupuncture and hormone therapy on hot flushes in women with breast cancer: A prospective, randomized, controlled multicenter trial. Climacteric 2008, 11, 166–174. [Google Scholar] [CrossRef]
- Hervik, J.; Mjaland, O. Acupuncture for the treatment of hot flashes in breast cancer patients, a randomized, controlled trial. Breast Cancer Res. Treat. 2009, 116, 311–316. [Google Scholar] [CrossRef]
- Deng, G.; Chan, Y.; Sjoberg, D.; Vickers, A.; Yeung, K.S.; Kris, M.; Straus, D.; Cassileth, B. Acupuncture for the treatment of post-chemotherapy chronic fatigue: A randomized, blinded, sham-controlled trial. Support Care Cancer 2013, 21, 1735–1741. [Google Scholar] [CrossRef]
- Molassiotis, A.; Bardy, J.; Finnegan-John, J.; Mackereth, P.; Ryder, D.W.; Filshie, J.; Ream, E.; Richardson, A. Acupuncture for cancer-related fatigue in patients with breast cancer: A pragmatic randomized controlled trial. J. Clin. Oncol. 2012, 30, 4470–4476. [Google Scholar] [CrossRef]
- Molassiotis, A.; Bardy, J.; Finnegan-John, J.; Mackereth, P.; Ryder, W.D.; Filshie, J.; Ream, E.; Eaton, D.; Richardson, A. A randomized, controlled trial of acupuncture self-needling as maintenance therapy for cancer-related fatigue after therapist-delivered acupuncture. Ann. Oncol. 2013, 24, 1645–1652. [Google Scholar] [CrossRef] [PubMed]
- Kiecolt-Glaser, J.K.; Bennett, J.M.; Andridge, R.; Peng, J.; Shapiro, C.L.; Malarkey, W.B.; Emery, C.F.; Layman, R.; Mrozek, E.E.; Glaser, R. Yoga’s impact on inflammation, mood, and fatigue in breast cancer survivors: A randomized controlled trial. J. Clin. Oncol. 2014, 32, 1040–1049. [Google Scholar] [CrossRef] [PubMed]
- Taso, C.J.; Lin, H.S.; Lin, W.L.; Chen, S.M.; Huang, W.T.; Chen, S.W. The effect of yoga exercise on improving depression, anxiety, and fatigue in women with breast cancer: A randomized controlled trial. J. Nurs. Res. 2014, 22, 155–164. [Google Scholar] [CrossRef] [PubMed]
- Greenlee, H.; DuPont-Reyes, M.J.; Balneaves, L.G.; Carlson, L.E.; Cohen, M.R.; Deng, G.; Johnson, J.A.; Mumber, M.; Seely, D.; Zick, S.M.; et al. Clinical practice guidelines on the evidence-based use of integrative therapies during and after breast cancer treatment. CA Cancer J. Clin. 2017, 67, 194–232. [Google Scholar] [CrossRef] [PubMed]
- Northern Cancer Alliance, National Health Service. Breast Cancer Clinical Guidelines; Northern Cancer Alliance, National Health Service: Newcastle Upon Tyne, UK, 2020. [Google Scholar]
- Abbasi, B.; Mirzakhany, N.; Angooti Oshnari, L.; Irani, A.; Hosseinzadeh, S.; Tabatabaei, S.M.; Haghighat, S. The effect of relaxation techniques on edema, anxiety and depression in post-mastectomy lymphedema patients undergoing comprehensive decongestive therapy: A clinical trial. PLoS ONE 2018, 13, e0190231. [Google Scholar] [CrossRef]
- De Groef, A.; Van Kampen, M.; Vervloesem, N.; De Geyter, S.; Christiaens, M.R.; Neven, P.; Vos, L.; De Vrieze, T.; Geraerts, I.; Devoogdt, N. Myofascial techniques have no additional beneficial effects to a standard physical therapy programme for upper limb pain after breast cancer surgery: A randomized controlled trial. Clin. Rehabil. 2017, 31, 1625–1635. [Google Scholar] [CrossRef]
- Lu, W.; Giobbie-Hurder, A.; Freedman, R.A.; Shin, I.H.; Lin, N.U.; Partridge, A.H.; Rosenthal, D.S.; Ligibel, J.A. Acupuncture for Chemotherapy-Induced Peripheral Neuropathy in Breast Cancer Survivors: A Randomized Controlled Pilot Trial. Oncologist 2020, 25, 310–318. [Google Scholar] [CrossRef]
- Liu, X.; Lu, J.; Wang, G.; Chen, X.; Xv, H.; Huang, J.; Xue, M.; Tang, J. Acupuncture for Arthralgia Induced by Aromatase Inhibitors in Patients with Breast Cancer: A Systematic Review and Meta-analysis. Integr. Cancer Ther. 2021, 20, 1534735420980811. [Google Scholar] [CrossRef]
- Colquhoun, H.L.; Levac, D.; O’Brien, K.K.; Straus, S.; Tricco, A.C.; Perrier, L.; Kastner, M.; Moher, D. Scoping reviews: Time for clarity in definition, methods, and reporting. J. Clin. Epidemiol. 2014, 67, 1291–1294. [Google Scholar] [CrossRef]
- Arksey, H.; O’Malley, L. Scoping studies: Towards a methodological framework. Int. J. Soc. Res. Methodol. 2005, 8, 19–32. [Google Scholar] [CrossRef]
- Tricco, A.C.; Lillie, E.; Zarin, W.; O’Brien, K.K.; Colquhoun, H.; Levac, D.; Moher, D.; Peters, M.D.J.; Horsley, T.; Weeks, L.; et al. PRISMA Extension for Scoping Reviews (PRISMA-ScR): Checklist and Explanation. Ann. Intern. Med. 2018, 169, 467–473. [Google Scholar] [CrossRef] [PubMed]
- Chino, A.; Okamoto, H.; Hirasaki, Y.; Ueda, K.; Ogawa, K.; Namiki, T. A case of aromatase inhibitor (anastrozole)-induced side-effects successfully treated with Kampo medicines. J. Altern. Complement. Med. 2011, 17, 1075–1077. [Google Scholar] [CrossRef] [PubMed]
- Beuth, J.; van Leendert, R.; Schneider, B.; Uhlenbruck, G. Complementary medicine on side-effects of adjuvant hormone therapy in patients with breast cancer. In Vivo 2013, 27, 781–869. [Google Scholar] [PubMed]
- Oh, B.; Kimble, B.; Costa, D.S.J.; Davis, E.; McLean, A.; Orme, K.; Beith, J. Acupuncture for treatment of arthralgia secondary to aromatase inhibitor therapy in women with early breast cancer: Pilot study. Acupunct. Med. 2013, 31, 264–271. [Google Scholar] [CrossRef]
- Mao, J.J.; Farrar, J.T.; Bruner, D.; Zee, J.; Bowman, M.; Seluzicki, C.; DeMichele, A.; Xie, S.X. Electroacupuncture for fatigue, sleep, and psychological distress in breast cancer patients with aromatase inhibitor-related arthralgia: A randomized trial. Cancer 2014, 120, 3744–3751. [Google Scholar] [CrossRef]
- Mao, J.J.; Xie, S.X.; Farrar, J.T.; Stricker, C.T.; Bowman, M.A.; Bruner, D.; DeMichele, A. A randomised trial of electro-acupuncture for arthralgia related to aromatase inhibitor use. Eur. J. Cancer. 2014, 50, 267–276. [Google Scholar] [CrossRef]
- Li, Y.; Zhang, Z.; Cui, F.; Liu, J.; Wang, Y.; Jiang, J.; Ma, W.; Lu, W. Traditional Chinese medicine bionic tiger bone powder for the treatment of ai-Associated musculoskeletal symptoms. Evid. Based Complement. Alternat. Med. 2017, 2017, 2478565. [Google Scholar] [CrossRef]
- Peng, N.; Yu, M.; Yang, G.; Fu, Q.; Xu, Y.; Yu, J.; Liu, Q.; Li, C.; Xu, W.; Zhang, Y.; et al. Effects of the Chinese medicine Yi Shen Jian Gu granules on aromatase inhibitor-associated musculoskeletal symptoms: A randomized, controlled clinical trial. Breast 2018, 37, 18–27. [Google Scholar] [CrossRef]
- Zhang, X.; Peng, N.; Yu, M.-W.; Zhang, G.-L.; Sun, X.; Yang, G.-W.; Li, C.; Yang, L.; Wang, X.-M. Chinese Medicine Yishen Jiangu Granules () on Aromatase Inhibitor-Associated Musculoskeletal Symptoms. Chin. J. Integr. Med. 2018, 24, 867–872. [Google Scholar] [CrossRef]
- Kim, T.H.; Kang, J.W. Acupuncture for symptoms management in Korean breast cancer survivors: A prospective pilot study. Acupunct. Med. 2019, 37, 164–174. [Google Scholar] [CrossRef]
- Ms, B.R.C.; Van Zee, K.; Yeung, K.; Ma, M.I.C.; Cohen, S.; Chan, Y.H.; Vickers, A.; Ma, D.D.S.; Hudis, C.A. Acupuncture in the treatment of upper-limb lymphedema: Results of a pilot study. Cancer 2013, 119, 2455–24561. [Google Scholar] [CrossRef]
- Jeong, Y.J.; Kwon, H.J.; Park, Y.S.; Kwon, O.C.; Shin, I.H.; Park, S.H. Treatment of Lymphedema with Saam Acupuncture in Patients with Breast Cancer: A Pilot Study. Med. Acupunct. 2015, 27, 206–215. [Google Scholar] [CrossRef] [PubMed]
- Bao, T.; Zhi, W.I.; Vertosick, E.A.; Li, Q.S.; DeRito, J.; Vickers, A.; Cassileth, B.R.; Mao, J.J.; Van Zee, K.J. Acupuncture for breast cancer-related lymphedema: A randomized controlled trial. Breast Cancer Res. Treat. 2018, 170, 77–87. [Google Scholar] [CrossRef] [PubMed]
- Wang, C.; Zhang, Y.; Yang, M.; Liu, Y.; Zhu, Y.; Fan, Y.; Li, Q.; Pei, X. Bloodletting puncture and cupping as an adjuvant therapy for breast cancer-related lymphedema in female adults: A non-randomized controlled pragmatic trial. J. Tradit. Chin. Med. Sci. 2018, 5, 255–263. [Google Scholar] [CrossRef]
- Wang, C.; Yang, M.; Fan, Y.; Pei, X. Moxibustion as a Therapy for Breast Cancer-Related Lymphedema in Female Adults: A Preliminary Randomized Controlled Trial. Integr. Cancer Ther. 2019, 18, 1534735419866919. [Google Scholar] [CrossRef]
- Han, K.; Kwon, O.; Park, H.-J.; Kim, A.-R.; Lee, B.; Kim, M.; Kim, J.-H.; Yang, C.-S.; Yoo, H.-S. Electronic Moxibustion for Breast Cancer-Related Lymphedema: A Pilot Clinical Trial. Integr. Cancer Ther. 2020, 19, 1534735420962854. [Google Scholar] [CrossRef]
- Bauml, J.; Basal, C.; Mao, J.J. Treatment of post-mastectomy pain syndrome with acupuncture: A case report. Acupunct. Med. 2014, 32, 183–185. [Google Scholar] [CrossRef]
- Mallory, M.J.; Croghan, K.A.; Sandhu, N.P.; Lemaine, V.; Degnim, A.C.; Bauer, B.A.; Cha, S.S.; Croghan, I.T. Acupuncture in the postoperative setting for breast cancer patients: A feasibility study. Am. J. Chin. Med. 2015, 43, 45–56. [Google Scholar] [CrossRef]
- Giron, P.S.; Haddad, C.A.S.; Rizzi, S.K.; Nazário, A.C.P.; Facina, G. Effectiveness of acupuncture in rehabilitation of physical and functional disorders of women undergoing breast cancer surgery. Support Care Cancer 2016, 24, 2491–2496. [Google Scholar] [CrossRef]
- Quinlan-Woodward, J.; Gode, A.; Dusek, J.; Reinstein, A.; Johnson, J.; Sendelbach, S. Assessing the Impact of Acupuncture on Pain, Nausea, Anxiety, and Coping in Women Undergoing a Mastectomy. Oncol. Nurs. Forum. 2016, 43, 725–732. [Google Scholar] [CrossRef]
- Ao, L.; Shi, J.; Bai, Y.; Zhang, S.; Gan, J. Effects of transcutaneous electrical acupoint stimulation on perioperative immune function and postoperative analgesia in patients undergoing radical mastectomy: A randomized controlled trial. Exp. Ther. Med. 2021, 21, 184. [Google Scholar] [CrossRef] [PubMed]
- Ogawa, K.; Ogawa, M.; Nishijima, K.; Tsuda, M.; Nishimura, G. Efficacy of contact needle therapy for chemotherapy-induced peripheral neuropathy. Evid. Based Complement. Alternat. Med. 2013, 2013, 928129. [Google Scholar] [CrossRef] [PubMed]
- Greenlee, H.; Crew, K.D.; Capodice, J.; Awad, D.; Buono, D.; Shi, Z.; Jeffres, A.; Wyse, S.; Whitman, W.; Trivedi, M.S.; et al. Randomized sham-controlled pilot trial of weekly electro-acupuncture for the prevention of taxane-induced peripheral neuropathy in women with early stage breast cancer. Breast Cancer Res. Treat. 2016, 156, 453–464. [Google Scholar] [CrossRef] [PubMed]
- Bao, T.; Seidman, A.D.; Piulson, L.; Vertosick, E.; Chen, X.; Vickers, A.J.; Blinder, V.S.; Zhi, W.I.; Li, Q.; Vahdat, L.T.; et al. A phase IIA trial of acupuncture to reduce chemotherapy-induced peripheral neuropathy severity during neoadjuvant or adjuvant weekly paclitaxel chemotherapy in breast cancer patients. Eur. J. Cancer 2018, 101, 12–19. [Google Scholar] [CrossRef]
- Jeong, Y.J.; Kwak, M.A.; Seo, J.C.; Park, S.H.; Bong, J.G.; Shin, I.H.; Park, S.H. Acupuncture for the treatment of taxane-induced peripheral neuropathy in breast cancer patients: A pilot trial. Evid. Based Complement. Alternat. Med. 2018, 2018, 5367014. [Google Scholar] [CrossRef]
- Rostock, M.; Fischer, J.; Mumm, A.; Stammwitz, U.; Saller, R.; Bartsch, H.H. Black cohosh (Cimicifuga racemosa) in tamoxifen-treated breast cancer patients with climacteric complaints a prospective observational study. Gynecol. Endocrinol. 2011, 27, 844–848. [Google Scholar] [CrossRef]
- Ben-Arye, E.; Israely, P.; Baruch, E.; Dagash, J. Integrating family medicine and complementary medicine in cancer care: A cross-cultural perspective. Patient Educ. Couns. 2014, 97, 135–139. [Google Scholar] [CrossRef]
- Zhu, L.M. One case report of postoperative bone metastases after treatment of Yiqi Yangyin Jiedu Decoction to breast cancer. J. Shanghai Jiao Tong Univ. 2014, 34, 126–128. [Google Scholar] [CrossRef]
- Lin, Y.-H.; Shiu, J.-H.; Chen, F.-P.; Chiu, J.-H. Building an Integrative Outpatient Care Program for Breast Cancer Patients in Taiwan. Integr Cancer Ther. 2016, 15, 343–348. [Google Scholar] [CrossRef]
- Saghatelyan, T.; Tananyan, A.; Janoyan, N.; Tadevosyan, A.; Petrosyan, H.; Hovhannisyan, A.; Hayrapetyan, L.; Arustamyan, M.; Arnhold, J.; Rotmann, A.-R.; et al. Efficacy and safety of curcumin in combination with paclitaxel in patients with advanced, metastatic breast cancer: A comparative, randomized, double-blind, placebo-controlled clinical trial. Phytomedicine 2020, 70, 153218. [Google Scholar] [CrossRef]

Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).