
The Prognostic Value of Eight Comorbidity Indices in Older Patients with Cancer: The ELCAPA Cohort Study

 , ,
, ,  ,
,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
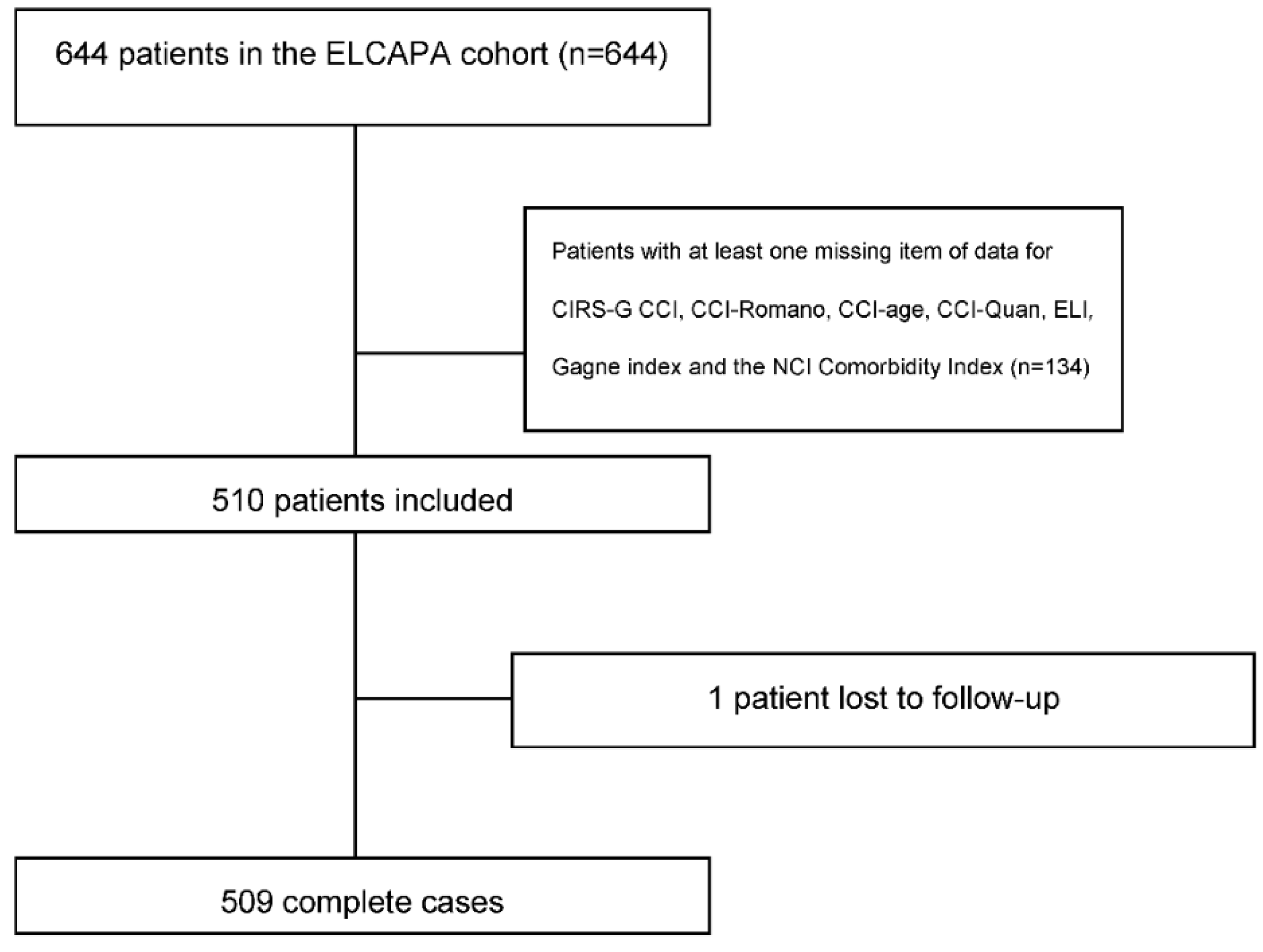
2.1. Design and Setting
2.2. Data Collection
2.3. Main Outcome Measure
2.4. Statistical Analysis
2.5. Sensitivity Analysis
3. Results
3.1. Main Analysis
3.2. Tumor Site Analysis
3.3. Sensitivity Analyses
4. Discussion
Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Dyba, T.; Randi, G.; Bray, F.; Martos, C.; Giusti, F.; Nicholson, N.; Gavin, A.; Flego, M.; Neamtiu, L.; Dimitrova, N.; et al. The European cancer burden in 2020: Incidence and mortality estimates for 40 countries and 25 major cancers. Eur. J. Cancer 2021, 157, 308–347. [Google Scholar] [CrossRef] [PubMed]
- Edwards, B.K.; Noone, A.M.; Mariotto, A.B.; Simard, E.P.; Boscoe, F.P.; Henley, S.J.; Jemal, A.; Cho, H.; Anderson, R.N.; Kohler, B.A.; et al. Annual Report to the Nation on the status of cancer, 1975–2010, featuring prevalence of comorbidity and impact on survival among persons with lung, colorectal, breast, or prostate cancer. Cancer 2014, 120, 1290–1314. [Google Scholar] [CrossRef] [PubMed]
- Terret, C.; Castel-Kremer, E.; Albrand, G.; Droz, J.P. Effects of comorbidity on screening and early diagnosis of cancer in elderly people. Lancet Oncol. 2009, 10, 80–87. [Google Scholar] [CrossRef]
- Corkum, M.; Urquhart, R.; Kendell, C.; Burge, F.; Porter, G.; Johnston, G. Impact of comorbidity and healthcare utilization on colorectal cancer stage at diagnosis: Literature review. Cancer Causes Control 2012, 23, 213–220. [Google Scholar] [CrossRef] [Green Version]
- Lee, L.; Cheung, W.Y.; Atkinson, E.; Krzyzanowska, M.K. Impact of comorbidity on chemotherapy use and outcomes in solid tumors: A systematic review. J. Clin. Oncol. 2011, 29, 106–117. [Google Scholar] [CrossRef] [PubMed]
- Dehal, A.; Abbas, A.; Johna, S. Comorbidity and outcomes after surgery among women with breast cancer: Analysis of nationwide in-patient sample database. Breast Cancer Res. Treat. 2013, 139, 469–476. [Google Scholar] [CrossRef] [PubMed]
- Van Gestel, Y.R.; Lemmens, V.E.; de Hingh, I.H.; Steevens, J.; Rutten, H.J.; Nieuwenhuijzen, G.A.; van Dam, R.M.; Siersema, P.D. Influence of comorbidity and age on 1-, 2-, and 3-month postoperative mortality rates in gastrointestinal cancer patients. Ann. Surg. Oncol. 2013, 20, 371–380. [Google Scholar] [CrossRef] [PubMed]
- Tomaszewski, J.J.; Uzzo, R.G.; Kutikov, A.; Hrebinko, K.; Mehrazin, R.; Corcoran, A.; Ginzburg, S.; Viterbo, R.; Chen, D.Y.; Greenberg, R.E.; et al. Assessing the burden of complications after surgery for clinically localized kidney cancer by age and comorbidity status. Urology 2014, 83, 843–849. [Google Scholar] [CrossRef] [Green Version]
- Cazzaniga, M.E.; Cordani, N.; Capici, S.; Cogliati, V.; Riva, F.; Cerrito, M.G. Metronomic Chemotherapy. Cancers 2021, 13, 2236. [Google Scholar] [CrossRef] [PubMed]
- Charlson, M.E.; Pompei, P.; Ales, K.L.; MacKenzie, C.R. A new method of classifying prognostic comorbidity in longitudinal studies: Development and validation. J. Chronic. Dis. 1987, 40, 373–383. [Google Scholar] [CrossRef]
- Gagne, J.J.; Glynn, R.J.; Avorn, J.; Levin, R.; Schneeweiss, S. A combined comorbidity score predicted mortality in elderly patients better than existing scores. J. Clin. Epidemiol. 2011, 64, 749–759. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Klabunde, C.N.; Legler, J.M.; Warren, J.L.; Baldwin, L.-M.; Schrag, D. A refined comorbidity measurement algorithm for claims-based studies of breast, prostate, colorectal, and lung cancer patients. Ann. Epidemiol. 2007, 17, 584–590. [Google Scholar] [CrossRef]
- Romano, P.S.; Roos, L.L.; Jollis, J.G. Adapting a clinical comorbidity index for use with ICD-9-CM administrative data: Differing perspectives. J. Clin. Epidemiol. 1993, 46, 1075–1079, discussion 1081–1090. [Google Scholar] [CrossRef]
- Quan, H.; Li, B.; Couris, C.M.; Fushimi, K.; Graham, P.; Hider, P.; Januel, J.M.; Sundararajan, V. Updating and validating the Charlson comorbidity index and score for risk adjustment in hospital discharge abstracts using data from 6 countries. Am. J. Epidemiol. 2011, 173, 676–682. [Google Scholar] [CrossRef] [Green Version]
- Sarfati, D. Review of methods used to measure comorbidity in cancer populations: No gold standard exists. J. Clin. Epidemiol. 2012, 65, 924–933. [Google Scholar] [CrossRef] [PubMed]
- Puts, M.T.E.; Hardt, J.; Monette, J.; Girre, V.; Springall, E.; Alibhai, S.M.H. Use of geriatric assessment for older adults in the oncology setting: A systematic review. J. Natl. Cancer Inst. 2012, 104, 1133–1163. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wildiers, H.; Heeren, P.; Puts, M.; Topinkova, E.; Janssen-Heijnen, M.L.; Extermann, M.; Falandry, C.; Artz, A.; Brain, E.; Colloca, G.; et al. International Society of Geriatric Oncology consensus on geriatric assessment in older patients with cancer. J. Clin. Oncol. 2014, 32, 2595–2603. [Google Scholar] [CrossRef] [Green Version]
- Van Walraven, C.; Austin, P.C.; Jennings, A.; Quan, H.; Forster, A.J. A modification of the Elixhauser comorbidity measures into a point system for hospital death using administrative data. Med. Care 2009, 47, 626–633. [Google Scholar] [CrossRef]
- Parmelee, P.A.; Thuras, P.D.; Katz, I.R.; Lawton, M.P. Validation of the Cumulative Illness Rating Scale in a geriatric residential population. J. Am. Geriatr. Soc. 1995, 43, 130–137. [Google Scholar] [CrossRef]
- Jørgensen, T.L.; Hallas, J.; Friis, S.; Herrstedt, J. Comorbidity in elderly cancer patients in relation to overall and cancer-specific mortality. Br. J. Cancer 2012, 106, 1353–1360. [Google Scholar] [CrossRef] [Green Version]
- Land, L.H.; Dalton, S.O.; Jensen, M.-B.; Ewertz, M. Impact of comorbidity on mortality: A cohort study of 62,591 Danish women diagnosed with early breast cancer, 1990–2008. Breast Cancer Res. Treat. 2012, 131, 1013–1020. [Google Scholar] [CrossRef] [PubMed]
- Von Elm, E.; Altman, D.G.; Egger, M.; Pocock, S.J.; Gøtzsche, P.C.; Vandenbroucke, J.P. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: Guidelines for reporting observational studies. Lancet 2007, 370, 1453–1457. [Google Scholar] [CrossRef]
- Caillet, P.; Canoui-Poitrine, F.; Vouriot, J.; Berle, M.; Reinald, N.; Krypciak, S.; Bastuji-Garin, S.; Culine, S.; Paillaud, E. Comprehensive geriatric assessment in the decision-making process in elderly patients with cancer: ELCAPA study. J. Clin. Oncol. 2011, 29, 3636–3642. [Google Scholar] [CrossRef] [PubMed]
- Quan, H.; Sundararajan, V.; Halfon, P.; Fong, A.; Burnand, B.; Luthi, J.C.; Saunders, L.D.; Beck, C.A.; Feasby, T.E.; Ghali, W.A. Coding algorithms for defining comorbidities in ICD-9-CM and ICD-10 administrative data. Med. Care 2005, 43, 1130–1139. [Google Scholar] [CrossRef] [PubMed]
- Charlson, M.; Szatrowski, T.P.; Peterson, J.; Gold, J. Validation of a combined comorbidity index. J. Clin. Epidemiol. 1994, 47, 1245–1251. [Google Scholar] [CrossRef]
- Elixhauser, A.; Steiner, C.; Harris, D.R.; Coffey, R.M. Comorbidity measures for use with administrative data. Med. Care 1998, 36, 8–27. [Google Scholar] [CrossRef]
- Royston, P.; Sauerbrei, W. A new measure of prognostic separation in survival data. Stat. Med. 2004, 23, 723–748. [Google Scholar] [CrossRef]
- Swets, J.A. Measuring the accuracy of diagnostic systems. Science 1988, 240, 1285–1293. [Google Scholar] [CrossRef] [Green Version]
- Katz, S.; Ford, A.B.; Moskowitz, R.W.; Jackson, B.A.; Jaffe, M.W. studies of illness in the aged. the index of adl: A standardized measure of biological and psychosocial function. JAMA 1963, 185, 914–919. [Google Scholar] [CrossRef]
- Linn, B.S.; Linn, M.W.; Gurel, L. Cumulative illness rating scale. J. Am. Geriatr. Soc. 1968, 16, 622–626. [Google Scholar] [CrossRef]
- Miller, M.D.; Paradis, C.F.; Houck, P.R.; Mazumdar, S.; Stack, J.A.; Rifai, A.H.; Mulsant, B.; Reynolds, C.F., III. Rating chronic medical illness burden in geropsychiatric practice and research: Application of the Cumulative Illness Rating Scale. Psychiatry Res. 1992, 41, 237–248. [Google Scholar] [CrossRef]
- Sarfati, D.; Koczwara, B.; Jackson, C. The impact of comorbidity on cancer and its treatment. CA Cancer J. Clin. 2016, 66, 337–350. [Google Scholar] [CrossRef] [PubMed]
- Boorjian, S.A.; Kim, S.P.; Tollefson, M.K.; Carrasco, A.; Cheville, J.C.; Thompson, R.H.; Thapa, P.; Frank, I. Comparative performance of comorbidity indices for estimating perioperative and 5-year all cause mortality following radical cystectomy for bladder cancer. J. Urol. 2013, 190, 55–60. [Google Scholar] [CrossRef] [PubMed]
- Lieffers, J.R.; Baracos, V.E.; Winget, M.; Fassbender, K. A comparison of Charlson and Elixhauser comorbidity measures to predict colorectal cancer survival using administrative health data. Cancer 2011, 117, 1957–1965. [Google Scholar] [CrossRef]
- Boulos, D.L.; Groome, P.A.; Brundage, M.D.; Siemens, D.R.; Mackillop, W.J.; Heaton, J.P.; Schulze, K.M.; Rohland, S.L. Predictive validity of five comorbidity indices in prostate carcinoma patients treated with curative intent. Cancer 2006, 106, 1804–1814. [Google Scholar] [CrossRef]
- Steyerberg, E.W. Clinical Prediction Models. In Statistics for Biology and Health; Springer: New York, NY, USA, 2009; Available online: http://link.springer.com/10.1007/978-0-387-77244-8 (accessed on 24 April 2022).


{kind=link}
{kind=link}
| Patients (n = 510) | ||
|---|---|---|
| No. | % | |
| Age, median (IQR) | 80 (76–84) | |
| Male sex | 233 | 45.7 |
| ECOG PS ≥ 2 | 235 | 50.4 |
| Solid cancer | 466 | 91.6 |
| Metastatic cancer | 215 | 47.3 |
| Haematologic malignancies | 43 | 8.4 |
| Cancer site (n = 463) | ||
| -Colorectal | 130 | 25.7 |
| -Breast | 107 | 21.1 |
| -Urinary tract | 55 | 10.9 |
| -Prostate | 46 | 9.1 |
| -Upper digestive tract and liver | 45 | 8.9 |
| -Pancreas | 40 | 7.9 |
| -Others * | 40 | 7.9 |
| Indices | ||
| Charlson Comorbidity Index (CCI), median (IQR) | 7 (4–12.5) | |
| Romano CCI version, median (IQR) | 8 (5–13) | |
| Quan CCI, median (IQR) | 5 (3–10) | |
| Age-adjusted CCI version, median (IQR) | 10.5 (8–14) | |
| Elishauser, median (IQR) | 21 (12–32) | |
| Gagne, median (IQR) | 7 (4–10) | |
| CIRS-G, median (IQR) | 12 (8–16) | |
| Whole Population | Metastatic Cancer | Nonmetastatic Cancer | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| n = 510 | n = 215 | n = 240 | ||||||||||
| Models | Hazard Ratio * 95% CI | Calibration | C Harrel | D.Sauerbrei/R2 | Hazard Ratio * 95% CI | Calibration | C Harrel | D.Sauerbrei/R2 | Hazard Ratio * 95% CI | Calibration | C Harrel | D.Sauerbrei/R2 |
| Initial (Adjusted for age, ECOG-PS and sex) | - | 0.85 | 0.7897 (0.77–0.81) | 1.89/0.46 | - | 0.56 | 0.7242 (0.71–0.77) | 1.35/0.30 | - | 0.49 | 0.8051 (0.74–0.84) | 1.74/0.42 |
| +CCI | 1.06 (0.86–1.29) | 0.71 | 0.7893 (0.75–0.81) | 1.90/0.46 | 0.82 (0.64–1.04) | 0.31 | 0.7282 (0.72–0.77) | 1.30/0.29 | 1.93 (1.34–2.77) | 0.004 | 0.8194 (0.76–085) | 2.34/0.57 |
| +Romano CCI version | 1.13 (0.94–1.36) | 0.73 | 0.7898 (0.76–0.81) | 1.92/0.47 | 0.88 (0.70–1.12) | 0.46 | 0.7257 (0.70–0.78) | 1.29/0.28 | 2.06 (1.44–2.96) | 0.001 | 0.8211 (0.75–0.85) | 2.38/0.57 |
| +Quan CCI version | 1.06 (0.86–1.31) | 0.71 | 0.7897 (0.76–0.81) | 1.91/0.47 | 0.81 (0.64–1.04) | 0.28 | 0.7281 (0.71–0.76) | 1.30/0.29 | 2.13 (1.48–3.07) | 0.002 | 0.8212 (0.74–0.86) | 2.44/0.59 |
| +Age-adjusted CCI | 1.08 (0.88–1.33) | 0.73 | 0.7887 (0.75–0.81) | 1.93/0.47 | 0.83 (0.64–1.06) | 0.37 | 0.7287 (0.71–0.79) | 1.29/0.28 | 1.98 (1.37–2.86) | 0.002 | 0.8203 (0.76–0.85) | 2.36/0.57 |
| +Elixhauser | 1.28 (1.08–1.52) | 0.81 | 0.7938 (0.76–0.81) | 2.01/0.49 | 1.02 (0.80–1.29) | 0.80 | 0.725 (0.70–0.77) | 1.38/0.31 | 2.40 (1.75–3.28) | 0.006 | 0.8377 (0.76–0.87) | 2.78/0.65 |
| +Gagne | 1.41 (1.19–1.69) | 0.74 | 0.7982 (0.76–0.82) | 2.09/0.51 | 1.12 (0.88–1.41) | 0.96 | 0.7246 (0.70–0.77) | 1.37/0.31 | 2.51 (1.80–3.50) | 0.001 | 0.8419 (0.78–0.88) | 2.81/0.65 |
| +CIRS-G | 1.29 (1.13–1.48) | 0.94 | 0.8029 (0.76–0.82) | 2.01/0.49 | 1.26 (1.06–1.50) | 0.62 | 0.7402 (0.72–0.80) | 1.43/0.33 | 1.44 (1.02–2.04) | 0.18 | 0.8109 (0.74–0.85) | 1.93/0.47 |
| Breast | Colorectal | Prostate | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| n = 106 | n = 130 | n = 46 | ||||||||||
| Models | Hazard Ratio * 95% CI | Calibration | C Harrel | D.Sauerbrei/R2 | Hazard Ratio * 95% CI | Calibration | C Harrel | D.Sauerbrei/R2 | Hazard Ratio * 95% CI | Calibration | C Harrel | D.Sauerbrei/R2 |
| Initial (Adjusted for age, ECOG-PS and sex) | - | 0.85 | 0.8683 (0.79–0.91) | 2.57/0.61 | - | 0.71 | 0.7505 (0.66–0.81) | 1.52/0.36 | - | <0.001 | 0.8950 (0.77–0.93) | 2.82/0.66 |
| +CCI | 0.83 (0.33–2.09) | 0.93 | 0.8683 (0.78–0.90) | 2.74/0.64 | 0.78 (0.56–1.10) | 0.96 | 0.7425 (0.65–0.80) | 1.72/0.41 | 1.16 (0.43–3.13) | <0.001 | 0.9037 (0.87–0.94) | 3.03/0.69 |
| +Romano CCI version | 1.26 (0.58–2.76) | 0.49 | 0.8672 (0.78–0.90) | 2.50/0.60 | 0.84 (0.59–1.20) | 0.89 | 0.7456 (0.67–0.81) | 1.77/0.43 | 0.91 (0.34–2.45) | <0.001 | 0.9081 (0.82–0.94) | 3.07/0.69 |
| +Quan CCI version | 1.13 (0.45–2.83) | 0.74 | 0.8680 (0.79–0.90) | 2.52/0.60 | 0.83 (0.58–1.21) | 0.85 | 0.7461 (0.67–0.81) | 1.73/0.42 | 0.52 (0.11–2.45) | <0.001 | 0.9212 (0.82–0.95) | 3.78/0.77 |
| +Age-adjusted CCI | 0.86 (0.33–2.21) | 0.92 | 0.8705 (0.79–0.91) | 2.74/0.64 | 0.78 (0.55–1.12) | 0.96 | 0.7436 (0.66–0.80) | 1.74/0.42 | 1.26 (0.45–3.49) | <0.001 | 0.9037 (0.79–0.93) | 3.16/0.70 |
| +Elixhauser | 1.58 (0.83–2.98) | 0.01 | 0.8718 (0.80–0.91) | 2.50/0.60 | 1.07 (0.73–1.56) | 0.86 | 0.7522 (0.67–0.81) | 1.46/0.34 | 0.72 (0.30–1.74) | <0.001 | 0.9125 (0.82–0.95) | 3.68/0.76 |
| +Gagne | 1.41 (0.70–2.83) | 0.24 | 0.8675 (0.80–0.90) | 2.47/0.59 | 1.06 (0.74–1.54) | 0.82 | 0.7547 (0.67–0.81) | 4.52/0.36 | 0.88 (0.38–2.06) | <0.001 | 0.8993 (0.81–0.93) | 2.91/0.67 |
| +CIRS-G | 1.38 (0.79–2.41) | 0.002 | 0.8772 (0.78–0.92) | 2.84/0.66 | 0.98 (0.73–1.33) | 0.58 | 0.7510 (0.66–0.81) | 1.54/0.36 | 2.80 (1.05–7.49) | <0.001 | 0.9365 (0.88–0.98) | 4.55/0.83 |
| +NCI breast | 1.02 (1.00–1.04) | 0.36 | 0.8691 (0.76–0.91) | 2.49/0.60 | ||||||||
| +NCI Colorectal | 1.04 (0.97–1.11) | 0.99 | 0.7569(0.68–0.82) | 1.39/0.32 | ||||||||
| +NCI prostate | 1.06 (0.88–1.27) | <0.001 | 0.8993 (0.81–0.93) | 3.09/0.70 | ||||||||
| Start Population | Metastatic Cancer | Nonmetastatic Cancer | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| n = 618 | n = 269 | n = 292 | ||||||||||
| Models | Hazard Ratio * 95% CI | Calibra tion | C Harrel | D.Sauerbrei/R2 | Hazard Ratio * 95% CI | Calibra tion | C Harrel | D.Sauerbrei/R2 | Hazard Ratio * 95% CI | Calibration | C Harrel | D.Sauerbrei/R2 |
| Initial (Adjusted for age, ECOG-PS and sex) | - | - | - | |||||||||
| +CCI | 1.27(1.05–1.52) | 1.05(0.86–1.29) | 1.91(1.29–2.81) | |||||||||
| +Romano CCI version | 1.35(1.13–1.60) | 1.12(0.92–1.37) | 2.06(1.42–3.00) | |||||||||
| +Quan CCI version | 1.33(1.11–1.61) | 1.09(0.89–1.34) | 2.16(1.47–3.18) | |||||||||
| +Age-adjusted CCI | 1.29(1.07–1.55) | 1.07(0.86–1.32) | 1.96(1.32–2.91) | |||||||||
| +Elixhauser | 1.49(1.27–1.76) | 1.23(1.01–1.50) | 2.40(1.75–3.28) | |||||||||
| +Gagne | 1.69(1.43–2.00) | 1.41(1.15–1.72) | 2.55(1.82–3.58) | |||||||||
| +CIRS-G | 1.52(1.37–1.70) | 1.56(1.36–1.79) | 1.57(1.21–2.04) | |||||||||
| Breast | Colorectal | Prostate | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| n = 115 | n = 130 | n = 54 | ||||||||||
| Models | Hazard Ratio * 95% CI | Calibra tion | C Harrel | D.Sauerbrei/R2 | Hazard Ratio * 95% CI | Calibra tion | C Harrel | D.Sauerbrei/R2 | Hazard Ratio * 95% CI | Calibra tion | C Harrel | D.Sauerbrei/R2 |
| Initial (Adjusted for age, ECOG-PS and sex) | - | - | - | |||||||||
| +CCI | 1.63(0.82–3.25) | 1.06(0.76–1.49) | 1.40(0.67–2.89) | |||||||||
| +Romano CCI version | 1.99(1.04–3.82) | 1.19(0.85–1.66) | 1.55(0.73–3.33) | |||||||||
| +Quan CCI version | 2.00(0.91–4.40) | 1.25(0.87–1.79) | 1.28(0.51–3.24) | |||||||||
| +Age-adjusted CCI | 1.71(0.85–3.41) | 1.07(0.76–1.52) | 1.42(0.68–2.97) | |||||||||
| +Elixhauser | 1.90(1.10–3.27) | 1.35(0.97–1.88) | 1.48(0.83–2.64) | |||||||||
| +Gagne | 1.90(1.06–3.41) | 1.52(1.07–2.16) | 1.92(1.07–3.45) | |||||||||
| +CIRS-G | 1.90(1.17–3.11) | 1.45(1.12–1.87) | 2.56(1.31–4.98) | |||||||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Canoui-Poitrine, F.; Segaux, L.; Benderra, M.-A.; About, F.; Tournigand, C.; Laurent, M.; Caillet, P.; Audureau, E.; Ferrat, E.; Lagrange, J.-L.; et al. The Prognostic Value of Eight Comorbidity Indices in Older Patients with Cancer: The ELCAPA Cohort Study. Cancers 2022, 14, 2236. https://doi.org/10.3390/cancers14092236
Canoui-Poitrine F, Segaux L, Benderra M-A, About F, Tournigand C, Laurent M, Caillet P, Audureau E, Ferrat E, Lagrange J-L, et al. The Prognostic Value of Eight Comorbidity Indices in Older Patients with Cancer: The ELCAPA Cohort Study. Cancers. 2022; 14(9):2236. https://doi.org/10.3390/cancers14092236
Chicago/Turabian StyleCanoui-Poitrine, Florence, Lauriane Segaux, Marc-Antoine Benderra, Frédégonde About, Christophe Tournigand, Marie Laurent, Philippe Caillet, Etienne Audureau, Emilie Ferrat, Jean-Leon Lagrange, and et al. 2022. "The Prognostic Value of Eight Comorbidity Indices in Older Patients with Cancer: The ELCAPA Cohort Study" Cancers 14, no. 9: 2236. https://doi.org/10.3390/cancers14092236