Simple Summary
This paper provides a definition of the sella, a description of common pathologies affecting the region, and an overview of the historical development of surgical approaches, as well as the advantages of techniques that are commonly used today.
Abstract
The sellar and parasellar region can be affected by diverse pathologies. The deep-seated location and surrounding critical neurovascular structures make treatment challenging; there is no singular, optimal approach for management. The history and development of transcranial and transsphenoidal approaches by pioneers in skull base surgery were largely aimed at treating pituitary adenomas, which are the most common lesions of the sella. This review explores the history of sellar surgery, the most commonly used approaches today, and future considerations for surgery of the sellar/parasellar region.
1. Introduction
The sellar/parasellar region can be affected by a multitude of neoplastic, vascular, and inflammatory pathologies [1]. Its deep-seated location is in close proximity to vital neurovascular structures, and tumor mass effect results in characteristic symptoms including ophthalmoplegia, visual field deficits, cranial neuropathies, and endocrine dysfunction [1]. The surrounding optic chiasm, pituitary–hypothalamic tract, and carotid artery segments make treatment challenging, and even small lesions can cause significant morbidity [2]. In the modern era, transcranial and transsphenoidal approaches to the sellar and parasellar region, with endoscopic or microscopic techniques, are regularly used to treat a diverse collection of pathologies; both possess advantages and limitations when applied in specific cases [3]. The refinement and development of the operative approaches used today represent the progressive evolution of concepts introduced just a century ago [4,5]. In this review, we provide a historical commentary about the pioneers of the development of transcranial and transsphenoidal surgical approaches to the sella, discuss the commonly used, modified, and nuanced procedures of the present, and consider future directions.
2. Anatomy
The sella turcica is a bony depression situated deeply in the middle fossa between the anterior clinoid and posterior clinoid processes [6]. Because of the surrounding critical structures and the frequency of substantial anatomic variations seen in the sella and the sphenoid sinus, management of pathology in this location is exceedingly difficult [7]. The pituitary gland sits in the sella turcica, with the optic chiasm positioned superiorly, the cavernous sinus and carotid arteries bounded laterally, the basilar artery and brainstem posteriorly, and the clivus inferiorly [3,8]. The space surrounding the sella turcica is termed “parasellar” space. The suprasellar region is above the sellar diaphragm and extends to the floor of the third ventricle [6]. These sellar and sellar-adjacent regions can be affected by diverse pathologies. The most common lesion of the sella is a nonfunctioning pituitary adenoma, followed by meningiomas (Figure 1) [6,9,10,11]. Meningiomas can arise from the diaphragm, tuberculum, anterior clinoid process, as well as from the chiasmatic sulcus dura and limbus and planum sphenoidale [6,12]. Tuberculum sellae meningiomas comprise nearly 5–10% of all intracranial meningiomas and regularly cause visual disturbances because of local mass effect on the optic apparatus [13,14]. Other pathologies of interest include craniopharyngiomas, Rathke cleft cysts, chordomas, metastases, and aneurysms [1,15]. Because pituitary adenomas make up nearly 90% of all sellar lesions [8], surgery to the region was largely developed to manage these tumors.
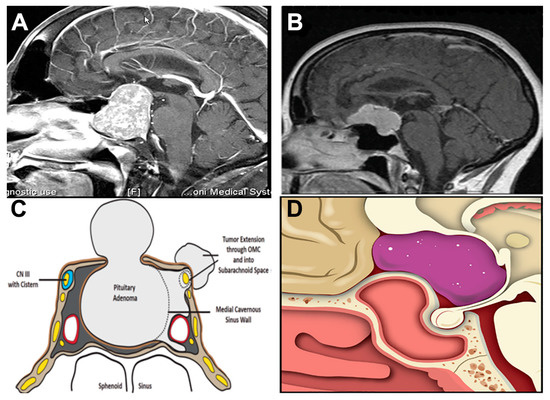
Figure 1.
Neuroanatomy of the most common sellar lesions. (A,C) Pituitary adenomas originate from the gland as it sits in the sella turcica. Macroadenomas can extend to the parasellar, retrosellar, suprasellar, and diaphragma sellar space, which results in compression of neurological structures. Panel C reprinted from: Hoang, N., Tran, D. K., Herde, R., Couldwell, G. C., Osborn, A. G., and Couldwell, W. T. (2016). Pituitary macroadenomas with oculomotor cistern extension and tracking: implications for surgical management, J. Neurosurg. 125(2), 315–322. (B,D) Tuberculum sellae meningiomas may extend to the planum sphenoidale, clivus, and sinus wall. Panels B and D reprinted from Raheja, A., Karsy, M., Eli, I., Guan, J., and Couldwell, W.T. (2017). Endonasal operative corridor expansion by sphenoidal pneumosinus dilatans in tuberculum sellae meningiomas, World Neurosurg. 106, 686–692, with permission from Elsevier.
3. History
The earliest accounts of a transsphenoidal approach can be credited to the ancient Egyptians [16] (Figure 2). During the mummification process, they used transnasal routes to remove the brain with long, customized instruments [17]. Their ancient practices provide insight into an advanced knowledge of anatomy and recognition of transnasal routes to the cerebrum. The origin of neurosurgical approaches to the sella dates to the late 19th century, when Richard Caton and F.T. Paul unsuccessfully attempted a pituitary tumor resection using a temporal approach [18]. Subsequently, transcranial and transsphenoidal approaches were developed to reach the pituitary. From the early days of extensive, disfiguring pituitary surgery with illumination by candlelight in the pre-antibiotic era to the introduction of the operative microscope and then endoscope to facilitate minimally invasive approaches [15,19], the evolution of surgical approaches to the sella was achieved through mentorship, trial and error, collaboration, and innovation.
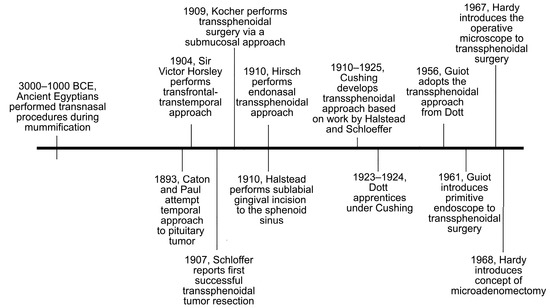
Figure 2.
Timeline of events leading to development of transsphenoidal approaches to the sella.
Caton and Paul attempted their temporal approach to the pituitary at the suggestion of Sir Victor Horsley, who himself was studying the ability to reach the sella turcica via a transcranial–transfacial route [15]. Between 1904 and 1906, Horsley attempted a transfrontal–transtemporal approach to treat pituitary tumors in a case series of 10 patients; he reported a mortality rate of 20% [1,15,18,19]. Around the same time in Austria, Hermann Schloffer was studying the work of Davide Giordano, who proposed the removal a pituitary tumor transfacially using a transglabellar nasal approach [18]. In 1907, Schloffer reported the first successful tumor resection via a superior transsphenoidal approach [15,20,21,22]. Although the success of these early approaches was limited by infection, meningitis, extensive operating time, and cosmetic defects, the interest in transsphenoidal pituitary surgery continued to grow. In 1909, Emil Theodor Kocher implemented the transsphenoidal approach using a submucosal dissection of the nasal septum, which expanded visualization of the sella, reduced risk of infection, and improved cosmetic outcomes [15,18,21]. The principle of submucosal dissection of the septum was a milestone for inferior extracranial approaches [19]. Two Viennese rhinologists, Oskar Hirsch and Markus Hajek, continued to develop transsphenoidal surgery and implemented the lateral endonasal approach through a direct transethmoidal route without reflection of the nose [1,15,18,19,23]. Throughout his career, Hirsch performed the endonasal transeptal transsphenoidal approach on 413 patients, and between 1919 and 1937, reported a mortality rate of only 5.4% [3]. His contributions to transsphenoidal surgery were great, and he continued to develop his practice, with improved outcomes at a time when transsphenoidal surgery was largely left to the wayside.
In 1910, Albert E. Halstead introduced a modified sublabial gingival incision to expose the sphenoid sinus [15]. This approach, as well as previous work by Schloffer, influenced Harvey Cushing and became the impetus for his own contribution to transsphenoidal surgery. Cushing attempted transsphenoidal resection to the pituitary using the approach from Halstead that he modified and refined, and from 1910 to 1925, Cushing treated patients while achieving a 5.6% mortality rate in this pre-antibiotic era [15,19]. Despite the acceptable results of his series, early transsphenoidal surgery was limited by poor visualization and limited resection capability, and Cushing was partial to mastering transcranial techniques. Specifically, he used a transfrontal craniotomy with a direct subfrontal midline approach to treat sellar lesions (Figure 3) [1,18,24]. Nearing the twilight of his career, from 1929 to 1931, Cushing virtually abandoned the transsphenoidal approach in favor of transcranial approaches [15,18,21]. His influence over the neurosurgical community at the time led to an overall decline in transsphenoidal surgery in the 1930s and onwards [15,19,21].
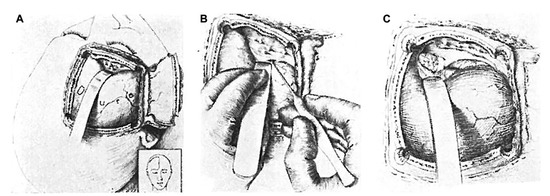
Figure 3.
The transfrontal approach to the sella was favored by Cushing. His preference for transcranial surgery had great influence over the neurosurgical community in North America. Illustration of the (A) craniotomy, (B) retraction of the frontal dura, and (C) exposure of the tumor. Reprinted from Cushing H, Eisenhardt L. Meningiomas arising from the tuberculum sellae. With the syndrome of primary optic atrophy and bitemporal field defects combined with a normal sella turcica in a middle-aged person. Arch. Ophthal. 1929;1(2):168–206.
The survival, and eventual revival, of transsphenoidal surgery is largely credited to the work of Norman Dott, Gerard Guiot, and Jules Hardy. Dott, as a fellow from Edinburgh, observed the transsphenoidal approach to the pituitary from Cushing and adopted it into his own practice [18]. In a series of 120 patients, using the transsphenoidal approach, Dott recorded great success and eventually achieved a mortality rate of 0% in his final 80 patients [21]. His abundant experience in pediatric surgery may have contributed to his comfort operating in the dark, narrow corridors inherent in the transsphenoidal approaches of the time [4]. His interest in engineering led to his designing of a speculum with a light attachment to improve illumination and visualization [4,18,19,21]. Guiot, a French neurosurgeon, learned the transsphenoidal technique from Dott, and in the 1950s, he introduced intraoperative radiofluoroscopy to transsphenoidal surgery to achieve visual confirmation of the depth and position of his instruments [4,15,18,19]. In his own series of 1000 patients, Guiot demonstrated superiority of the transsphenoidal approach to the transcranial approach through reduction in morbidity and better visual outcomes for patients with suprasellar tumors [21]. He went on to report the first primitive endoscopic endonasal transsphenoidal approach in 1963, although the quality of endoscopes was poor at the time [15,17]. Finally, Hardy was a mentee of Guiot who revolutionized the transsphenoidal approach. Hardy introduced the binocular microscope to transsphenoidal pituitary surgery in 1967 to overcome many of the disadvantages of the approach at the time [15,19,21]. With the operative microscope, Hardy introduced the concept of selective microadenomectomy to remove the tumor, spare the normal pituitary gland, and preserve endocrine function, and this obviated the need for regular hormonal replacement therapy [18,19,20,21]. The collaboration and mentorship among early innovators led to the development, and survival, of transcranial and transsphenoidal approaches to the sella that became the foundation for techniques used in the present. Today, transsphenoidal surgery is the gold standard for lesions of the pituitary gland and parasellar lesions [7]. Further advancements in intraoperative imaging with endoscope and microscope technology continually expand the opportunities and possibilities in skull base surgery.
4. Current Treatment Paradigm
The two main approaches to the sella are transcranial and transsphenoidal [25] (Figure 4). Transcranial surgery can be bi- or unilateral; commonly, a pterional, frontolateral, or orbitozygomatic approach is used. Within the last decade, keyhole approaches have risen in popularity [26]. Bilateral approaches include bifrontal and subfrontal craniotomies [13,14]. Transcranial approaches are typically performed in anterior or anterolateral corridors and are preferred for large tumors, those with extrasellar extension, and fibrous or indurated tumors [1]. They offer a wide exposure, but this comes at the cost of increased brain retraction and/or bone removal for a craniotomy [27,28]. The decision to approach a tumor via open approach versus endoscopically is based on numerous factors including surgeon preference; often, both methods can be viable options for the same skull base lesion [29].
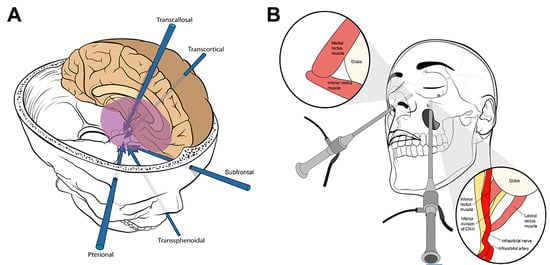
Figure 4.
(A) Surgical approaches and trajectories to the sellar/parasellar region. Reproduced with permission of the Department of Neurosurgery, University of Utah. (B) Endoscopic endonasal approach and transantral approach with endoscopic assistance. © 2020 Abou-Al-Shaar, Krisht, Cohen, Abunimer, Neil, Karsy, Alzhrani, and Couldwell. Reproduced under the terms of the Creative Commons Attribution License (CC BY).
Common approaches include pterional, orbitozygomatic, frontolateral, and more recently supraorbital keyhole approaches (Figure 5; Table 1) [13]. More minimally invasive approaches, including microscopic and endoscopic transsphenoidal surgery, exist to establish direct routes to the sella without the intrinsic morbidity associated with a transfacial or transcranial craniotomy [30,31]. There are advantages and disadvantages to both, and there is extensive overlap between the applicability of each approach. Operative decision-making is contingent on a range of factors including lesion type, growth trajectory and anatomical location, the symptoms at presentation, and the need for vascular control, among others [1]. A proposed grading system by McDermott and colleagues incorporates three key characteristics into determination of the optimal approach: tumor size, optic canal invasion, and arterial encasement [2,32]. Tumors with lower scores, i.e., those with smaller size and no arterial encasement or optic canal invasion were amenable to transsphenoidal surgery, whereas larger tumors with arterial and surrounding structure extension may be better managed with an open approach [2]. Another important tumor characteristic to consider when planning the ideal approach is consistency. Fibrous tumors are less amenable to suction and dissection and can present with adhesions; these tumors are better managed with an open approach [33].
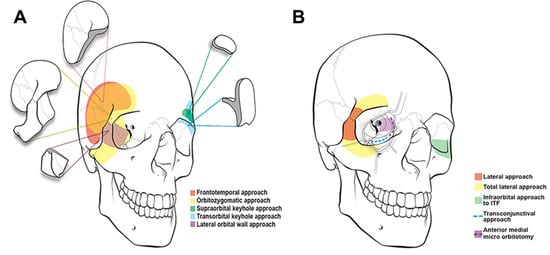
Figure 5.
(A) Cranio-orbital and (B) orbito-cranial approaches to lesions in the anterior and middle cranial fossa. There is no one-size-fits-all approach. Selection of traditional open approaches versus minimally invasive and keyhole surgery is case-dependent. © 2020 Abou-Al-Shaar, Krisht, Cohen, Abunimer, Neil, Karsy, Alzhrani and Couldwell. Reproduced under the terms of the Creative Commons Attribution License (CC BY).

Table 1.
Common surgical approaches to the sella/parasella.
Generally, the open craniotomy is the gold standard for meningiomas, such as tuberculum sellae meningiomas, because of the access to and ability to visualize the optic chiasm and nerves [33]. In contrast, in the case of pituitary adenomas, neurosurgeons are moving toward regular use of an endoscopic approach [34]. The endoscopic endonasal approach for tuberculum sellae meningiomas is most appropriate when the tumors are small and reside at the midline [35]. Some studies have reported that open transcranial approaches for lesions such as tuberculum sellae meningiomas result in higher rates of total resection and fewer complications such as cerebrospinal fluid (CSF) leak, while others suggest endonasal approaches may yield superior outcomes with respect to vision [27,36].
Ultimately, sellar lesions can be managed with different approaches [28,37]. Decision-making is nuanced and must be patient-specific; the optimal approach comes down to surgeon preference and experience. Familiarity with both transsphenoidal and transcranial techniques should be achieved so that both can be at the surgeon’s disposal.
4.1. Transsphenoidal Endoscopic Endonasal Approach
Transnasal transsphenoidal surgery is the most common approach to pituitary tumors that are confined to the sella and parasella [38]. Transsphenoidal surgery was performed and perfected under the microscope in the 20th century, but the use of the endoscope led to a boom in popularity while greatly enhancing the experience. Michael Apuzzo at the University of Southern California began to use the endoscope as an adjunct to conventional transsphenoidal surgery in 1977 [15,39], but it was not until the 1990s that purely endoscopic endonasal transsphenoidal surgery to the pituitary gained a true foothold, and Ricardo Carrau and Hae-Dong Jho published the first large case series of their experience with the endoscope, operating on 50 patients [17,40]. Today, endoscopic transsphenoidal surgery is a preferred route for pituitary adenomas and many sellar tumors because of the higher likelihood of preserving pituitary and visual function [31,41].
The endoscopic endonasal procedure can be performed independently or by two surgeons. A multidisciplinary effort may include an otolaryngologist driving the endoscope and establishing the access corridor to the sphenoid sinus, followed by a neurosurgeon dissecting the sinus and the tumor. The decision to collaborate with otolaryngology or operate as a single surgeon varies based on institution and surgeon preference. During the approach, key landmarks including the vomer, sellar floor, sphenoid rostrum, and opticocarotid recesses should be identified [7]. The procedure has been well described in the literature [42]. In brief, the endoscope is introduced to the nasal cavity and navigated to the sphenoid ostium. A bilateral sphenoidotomy and posterior nasal septectomy expose the keel of the sphenoid rostrum; this facilitates opening of the sellar floor and observation of the dura [1]. During pituitary tumor resection, the lateral boundaries are the cavernous sinuses bilaterally. Extension of the approach to access parasellar and clival tumors can be achieved by repositioning self-retaining retractors and resecting additional bone in the superior, inferior, and lateral directions [18,43]. The main advantages of the endoscopic endonasal approach are minimized brain retraction and superior visualization and illumination of the sellar anatomy [19,41]. The additional use of intraoperative navigation with stereotactic CT imaging can further reduce operative morbidity without an increase in operative time [44].
The approach is versatile, but it is mainly used for midline tumors. Access to compartments laterally beyond the optic nerves, cranial nerves, and surrounding vasculature can be limited [14,31]. There is a risk of cerebrospinal fluid leak—reports state it is as high as 30%, and a cerebrospinal fluid fistula can occur [13,28]. The two-dimensional field of view that is offered by endoscopic navigation can be a limitation, as can the restricted surgical instrument maneuverability compared with open surgery and a possibly significant learning curve required to master the endoscope [41]. Neurosurgeons reach proficiency operating under the binocular microscope during training and throughout their careers, but endoscopic surgery introduces a new set of instruments that require familiarization and skills that must be sharpened to achieve satisfactory results [45]. When resecting tumors near the midline, inadvertent injury to the internal carotid arteries, cavernous sinus, or optic nerves is possible, so spatial awareness and careful dissection technique is essential [7]. Transcranial approaches offer surgical maneuverability and can effectively remove tumors of the sella/parasella, but increasing application of minimally invasive endoscopic approaches has been shown to speed recovery, reduce perioperative risks, and lead to comparable or, in some cases, improved outcomes [46].
4.2. Pterional Approach
The pterional approach is the anterolateral workhorse in the skull base neurosurgeon’s armamentarium (Figure 6). It was described by Walter Dandy in 1938 and popularized by Gazi Yaşargil [32]. It is centered on the sylvian fissure over the sphenoid ridge and provides an operative window to the suprasellar, paraclinoid, and parachiasmal spaces [1,47]. The main advantage to the pterional approach is its wide access and ability to gain early vascular control, but the procedure is maximally invasive, can lead to postoperative cosmetic defects from the craniotomy, and frequently results in atrophy of the facial nerve and temporalis muscle [32]. Modifications to the pterional craniotomy include minimally invasive options such as the lateral supraorbital and mini-pterional approaches.
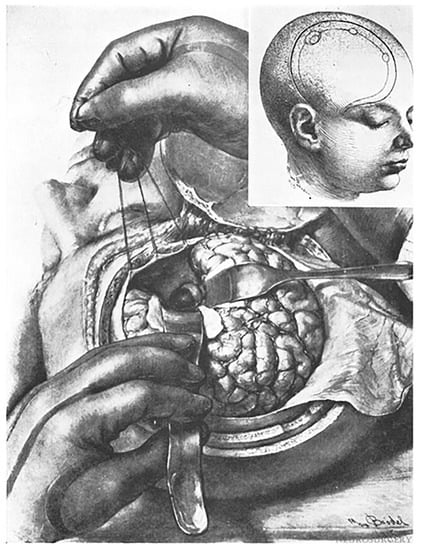
Figure 6.
Illustration of an early rendition of a frontotemporal approach favored by Heuer. Reprinted from Heuer GJ. Surgical experiences with an intracranial approach to chiasmal lesions. Arch. Surg. 1920;1(1):368–381.
4.3. Orbitozygomatic Approach
The orbitozygomatic approach is as maximally invasive as the pterional approach. It is essentially a modified pterional craniotomy with additional removal of the superior and lateral orbital rim plus a zygomatic osteotomy [1]. It can be advantageous when treating challenging lesions in the parasellar region, interpeduncular fossa, and tumors with significant superior and lateral extension from the sella turcica such as tuberculum sellae meningiomas [48]. The additional removal of the zygoma, superolateral orbital rim, and orbital wall facilitates improved multidirectional operative corridor access, surgical maneuverability, and reduced brain retraction at the expense of greater bone removal [47]. The disadvantages and risk profile are similar to those of the pterional approach.
4.4. Mini-Pterional Approach
The mini-pterional approach uses a smaller craniotomy than a pterional approach, with a transsylvian dissection that yields an exposure comparable with that of the standard procedure [47,49]. Centered on the sphenoid ridge, an incision is made approximately 1 cm above the zygomatic arch at the anterior border of the hairline and extended to the ipsilateral midpupillary line. A burr hole is made superior to the frontozygomatic suture, beneath the line temporalis, and an osteotomy is made elevating a bone flap that includes part of the frontal bone inferior to the superior temporal line, a minimal portion of the temporal bone, and the lateral aspect of the sphenoid bone [49]. The reduced size of the craniotomy lessens temporalis muscle dissection and tissue trauma, minimizes lobar retraction, and improves cosmetic outcomes without sacrificing the working angles of the approach [49]. The operative corridor is inherently more limited than the pterional approach, thus the mini-pterional is a suitable alternative in properly selected patients [47].
4.5. Lateral Supraorbital Approach
An additional minimally invasive modification of the pterional approach is the lateral supraorbital craniotomy (Figure 7) [32,50]. Using an incision behind the hairline, above the pinna, and extending medially towards the midpoint between the superior temporal line and the midline, the lateral supraorbital approach dissects a small portion of the superior and anterior temporalis muscles and requires a single, small burr hole at the MacCarty keyhole.
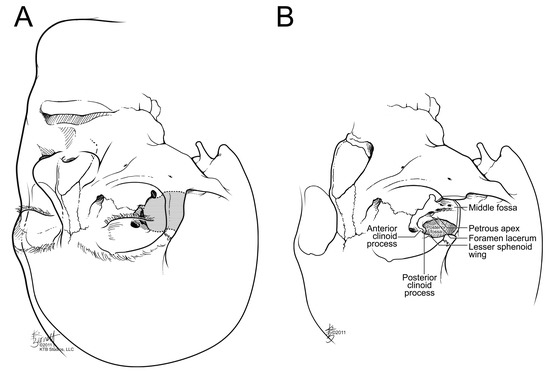
Figure 7.
(A) Sellar/parasellar region accessible from a lateral orbital approach. (B) Illustration showing the parasellar area and middle fossa structures after removal of the lateral orbital rim and wall in the translateral orbital approach. (Reprinted with permission from KTB Studios, LLC.).
A small bone flap is elevated with the keyhole at the center of the inferior margin [32]. The minimally invasive exposure is comparable with that of the pterional approach to reach parachiasmal lesions with a direct route [32,51]. In properly selected patients, the lateral supraorbital approach can be used as an alternative to the pterional approach for tuberculum sellae and planum sphenoidale meningiomas [32].
4.6. Supraorbital Approach
A supraorbital craniotomy can access deep-seated sellar/parasellar lesions of the tuberculum sellae, planum sphenoidale, and anterior clinoid process with minimal brain retraction [1,45,52]. It was first described by John Jane, Sr. in 1982 [47]; it is a suitable keyhole approach to the anterolateral skull base [53]. A short skin incision within the eyebrow is made along the superior orbital rim, avoiding the supraorbital nerve medially and the frontal branch of the facial nerve superiorly, and a superior orbital rim osteotomy is performed [1,28,47,52]. The limited skin incision yields a good cosmetic outcome, and attention is paid to preserve the frontal branch of the facial nerve and superficial temporal artery [52]. Like other keyhole approaches, limitations to the supraorbital craniotomy include narrow viewing angles, smaller working corridor, and decreased exposure width [45].
4.7. Interhemispheric and Combined Endoscopic Approaches
There are a multitude of other approaches to reach the sellar/parasellar region. Preclinical studies in cadaveric models have given rise to attempts at developing more direct, minimally invasive routes that retain the benefits of standard approaches. An anterior interhemispheric route favored by Bruneau and colleagues uses neuronavigation and a limited bicoronal incision behind the hairline with a midline anterior burr hole above the superior longitudinal sinus to reach tuberculum sellae meningiomas [12]. They describe their experience of achieving a symmetrical superior view of bilateral optic canals, optic nerves, and the optic chiasm with a unilateral incision while maintaining full proximal and distal control over vessels and visualizing posteroinferior tumor extension. An endoscopic intradural subtemporal keyhole approach as described by Ding et al. [54] uses frameless navigation and endoscope to reach the suprasellar, paraclival, and ventrolateral brainstem regions with minimal invasiveness. Additionally, a microscopic endoscope-assisted transmaxillosphenoidal approach evaluated by Gagliardi et al. [30] capably accessed the sellar, suprasellar, and parasellar region with minimal invasiveness, wide exposure, and avoidance of critical neurovascular structures encountered transsphenoidally by obtaining access through the maxillary sinus. The combined transmaxillary–transsphenoidal approach avoids violating the nasal cavity and obviates the need for a craniotomy [55]. Proper selection of patients is imperative during preoperative planning so that a surgical approach can be tailored on an individual basis.
5. Future Directions
Although the mainstays of treatment are microscopic, endoscopic, and keyhole transcranial and transsphenoidal approaches, innovations to enhance skull base surgery of the sellar/parasellar region are taking place. The evolution of three-dimensional technology to improve upon the two-dimensional visualization provided by endoscopes has occurred in the past decade [15]. The newly introduced exoscope, a high-definition telescopic device, has yet to be studied extensively in skull base surgery to understand its range of functionality [17]. Intraoperative use of agents such as indocyanine green, fluorescein, and 5-aminolevulinic acid are being implemented in endoscopic skull base surgery to improve safety and visualization. Fluorescein has been studied in pituitary adenomas and can differentiate tumor from healthy tissue, while indocyanine green and 5-aminolevulinic acid can enhance tumor dissection by highlighting nearby vessels and delineating the tumor as it is being dissected in difficult-to-visualize locations such as in proximity to the optic canals and cranial nerves [5,17]. Finally, there have been great strides in robotics in surgery. Although these applications are more often seen in other disciplines such as general surgery and orthopedics, robotics continues to be incorporated at a greater rate in neurosurgery. In skull base surgery, the use of robotic endoscope holders has been implemented with considerable success. Transoral robotic surgery has also been attempted to access the sella [41,56,57]. However, the large start-up costs to the hospital and the patient currently make robotic skull base surgery unfavorable [41]. In addition, with the current generation of robotics that were not specifically engineered for neurosurgical procedures, there are inherent limitations in maneuverability that do not permit access to the small, deep, working corridors of the skull base. Nor do the robots possess the fine, slight, dexterous movements necessary for the region [41,58]. Additional limitations that have been described include the lack of haptic feedback [17,57]. Nevertheless, as robotics continue to improve, their use in skull base neurosurgery is expected to expand. Their greatest utility will not come from replacing the surgeon’s skills but rather by improving intraoperative comfort and enhancing safety.
6. Conclusions
Surgery of the sellar and parasellar region is richly steeped in neurosurgical history. Through collaborative efforts among many of the greats and pioneers of the field, stepwise innovations and modifications have led to the development of the techniques that are regularly used today. A transsphenoidal approach to the sella, nearly abandoned at the midpoint of the 20th century, is the mainstay approach used in modern practice. Introduction of the operative microscope and then the endoscope brought forth a trove of new possibilities and expanded operative versatility for treating sellar/parasellar lesions. Future directions will be similarly established by boundary-pushing surgeons working towards a goal of improving and providing optimal treatment to patients.
Author Contributions
Conceptualization: W.T.C.; methodology: C.A.R.; writing—original draft preparation: C.A.R.; writing—review and editing: W.T.C.; visualization: C.A.R.; supervision: W.T.C. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Acknowledgments
We thank Vance Mortimer for assistance in preparing the operative images and Kristin Kraus for editorial assistance.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Lubomirsky, B.; Jenner, Z.B.; Jude, M.B.; Shahlaie, K.; Assadsangabi, R.; Ivanovic, V. Sellar, suprasellar, and parasellar masses: Imaging features and neurosurgical approaches. Neuroradiol. J. 2022, 35, 269–283. [Google Scholar] [CrossRef] [PubMed]
- Magill, S.T.; Morshed, R.A.; Lucas, C.G.; Aghi, M.K.; Theodosopoulos, P.V.; Berger, M.S.; de Divitiis, O.; Solari, D.; Cappabianca, P.; Cavallo, L.M.; et al. Tuberculum sellae meningiomas: Grading scale to assess surgical outcomes using the transcranial versus transsphenoidal approach. Neurosurg. Focus 2018, 44, E9. [Google Scholar] [CrossRef]
- Ben-Shlomo, N.; Mudry, A.; Naples, J.; Walsh, J.; Smith, T.R.; Laws, E.R.; Corrales, C.E. Hajek and Hirsch: Otolaryngology pioneers of endonasal transsphenoidal pituitary surgery. Laryngoscope 2022, 133, 807–813. [Google Scholar] [CrossRef] [PubMed]
- Lanzino, G.; Laws, E.R., Jr. Pioneers in the development of transsphenoidal surgery: Theodor Kocher, Oskar Hirsch, and Norman Dott. J. Neurosurg. 2001, 95, 1097–1103. [Google Scholar] [CrossRef]
- Riley, C.A.; Soneru, C.P.; Tabaee, A.; Kacker, A.; Anand, V.K.; Schwartz, T.H. Technological and ideological innovations in endoscopic skull base surgery. World Neurosurg. 2019, 124, 513–521. [Google Scholar] [CrossRef] [PubMed]
- Emanuelli, E.; Zanotti, C.; Munari, S.; Baldovin, M.; Schiavo, G.; Denaro, L. Sellar and parasellar lesions: Multidisciplinary management. Acta Otorhinolaryngol. Italy 2021, 41, S30–S41. [Google Scholar] [CrossRef] [PubMed]
- Zada, G.; Agarwalla, P.K.; Mukundan, S., Jr.; Dunn, I.; Golby, A.J.; Laws, E.R., Jr. The neurosurgical anatomy of the sphenoid sinus and sellar floor in endoscopic transsphenoidal surgery. J. Neurosurg. 2011, 114, 1319–1330. [Google Scholar] [CrossRef]
- Petrakakis, I.; Pirayesh, A.; Krauss, J.K.; Raab, P.; Hartmann, C.; Nakamura, M. The sellar and suprasellar region: A “hideaway” of rare lesions. Clinical aspects, imaging findings, surgical outcome and comparative analysis. Clin. Neurol. Neurosurg. 2016, 149, 154–165. [Google Scholar] [CrossRef]
- Al-Dahmani, K.; Mohammad, S.; Imran, F.; Theriault, C.; Doucette, S.; Zwicker, D.; Yip, C.E.; Clarke, D.B.; Imran, S.A. Sellar masses: An epidemiological study. Can. J. Neurol. Sci. 2016, 43, 291–297. [Google Scholar] [CrossRef]
- Raheja, A.; Abou Al-Shaar, H.; Patel, B.C.; Couldwell, W.T. Surgical implications of frontoethmoidal pneumosinus dilatans-associated proptosis caused by meningioma. Acta Neurochir. 2016, 158, 1597–1600. [Google Scholar] [CrossRef]
- Hoang, N.; Tran, D.K.; Herde, R.; Couldwell, G.C.; Osborn, A.G.; Couldwell, W.T. Pituitary macroadenomas with oculomotor cistern extension and tracking: Implications for surgical management. J. Neurosurg. 2016, 125, 315–322. [Google Scholar] [CrossRef] [PubMed]
- Bruneau, M.; Grenier-Chantrand, F.; Riva, M. How I do it: Anterior interhemispheric approach to tuberculum sellae meningiomas. Acta Neurochir. 2021, 163, 643–648. [Google Scholar] [CrossRef] [PubMed]
- Giammattei, L.; Starnoni, D.; Cossu, G.; Bruneau, M.; Cavallo, L.M.; Cappabianca, P.; Meling, T.R.; Jouanneau, E.; Schaller, K.; Benes, V.; et al. Surgical management of tuberculum sellae meningiomas: Myths, facts, and controversies. Acta Neurochir. 2020, 162, 631–640. [Google Scholar] [CrossRef] [PubMed]
- Wong, A.K.; Kramer, D.E.; Wong, R.H. Keyhole superior interhemispheric transfalcine approach for tuberculum sellae meningioma: Technical nuances and visual outcomes. World Neurosurg. 2021, 145, 5–12. [Google Scholar] [CrossRef] [PubMed]
- Cavallo, L.M.; Somma, T.; Solari, D.; Iannuzzo, G.; Frio, F.; Baiano, C.; Cappabianca, P. Endoscopic endonasal transsphenoidal surgery: History and evolution. World Neurosurg. 2019, 127, 686–694. [Google Scholar] [CrossRef] [PubMed]
- Fanous, A.A.; Couldwell, W.T. Transnasal excerebration surgery in ancient Egypt. J. Neurosurg. 2012, 116, 743–748. [Google Scholar] [CrossRef] [PubMed]
- Jarmula, J.; de Andrade, E.J.; Kshettry, V.R.; Recinos, P.F. The current state of visualization techniques in endoscopic skull base surgery. Brain Sci. 2022, 12, 1337. [Google Scholar] [CrossRef] [PubMed]
- Liu, J.K.; Das, K.; Weiss, M.H.; Laws, E.R., Jr.; Couldwell, W.T. The history and evolution of transsphenoidal surgery. J. Neurosurg. 2001, 95, 1083–1096. [Google Scholar] [CrossRef]
- Kanter, A.S.; Dumont, A.S.; Asthagiri, A.R.; Oskouian, R.J.; Jane, J.A., Jr.; Laws, E.R., Jr. The transsphenoidal approach. A historical perspective. Neurosurg. Focus 2005, 18, e6. [Google Scholar] [CrossRef]
- Mehta, G.U.; Lonser, R.R.; Oldfield, E.H. The history of pituitary surgery for Cushing disease. J. Neurosurg. 2012, 116, 261–268. [Google Scholar] [CrossRef]
- Patel, S.K.; Husain, Q.; Eloy, J.A.; Couldwell, W.T.; Liu, J.K. Norman Dott, Gerard Guiot, and Jules Hardy: Key players in the resurrection and preservation of transsphenoidal surgery. Neurosurg. Focus 2012, 33, E6. [Google Scholar] [CrossRef] [PubMed]
- Couldwell, W.T. Transsphenoidal and transcranial surgery for pituitary adenomas. J. Neurooncol. 2004, 69, 237–256. [Google Scholar] [CrossRef] [PubMed]
- Liu, J.K.; Cohen-Gadol, A.A.; Laws, E.R., Jr.; Cole, C.D.; Kan, P.; Couldwell, W.T. Harvey Cushing and Oskar Hirsch: Early forefathers of modern transsphenoidal surgery. J. Neurosurg. 2005, 103, 1096–1104. [Google Scholar] [CrossRef] [PubMed]
- Altay, T.; Couldwell, W.T. The frontotemporal (pterional) approach: An historical perspective. Neurosurgery 2012, 71, 481–491, discussion 491–492. [Google Scholar] [CrossRef]
- Makarenko, S.; Alzahrani, I.; Karsy, M.; Deopujari, C.; Couldwell, W.T. Outcomes and surgical nuances in management of giant pituitary adenomas: A review of 108 cases in the endoscopic era. J. Neurosurg. 2022, 137, 635–646. [Google Scholar] [CrossRef]
- Kachhara, R.; Nigam, P.; Nair, S. Tuberculum sella meningioma: Surgical management and results with emphasis on visual outcome. J. Neurosci. Rural Pract. 2022, 13, 431–440. [Google Scholar] [CrossRef] [PubMed]
- Marx, S.; Clemens, S.; Schroeder, H.W.S. The value of endoscope assistance during transcranial surgery for tuberculum sellae meningiomas. J. Neurosurg. 2018, 128, 32–39. [Google Scholar] [CrossRef]
- Linsler, S.; Fischer, G.; Skliarenko, V.; Stadie, A.; Oertel, J. Endoscopic assisted supraorbital keyhole approach or endoscopic endonasal approach in cases of tuberculum sellae meningioma: Which surgical route should be favored? World Neurosurg. 2017, 104, 601–611. [Google Scholar] [CrossRef] [PubMed]
- Sekhar, L.; Mantovani, A.; Mortazavi, M.; Schwartz, T.H.; Couldwell, W.T. Open vs endoscopic: When to use which. Neurosurgery 2014, 61 (Suppl. S1), 84–92. [Google Scholar] [CrossRef]
- Gagliardi, F.; Donofrio, C.A.; Spina, A.; Bailo, M.; Gragnaniello, C.; Gallotti, A.L.; Elbabaa, S.K.; Caputy, A.J.; Mortini, P. Endoscope-assisted transmaxillosphenoidal approach to the sellar and parasellar regions: An anatomic study. World Neurosurg. 2016, 95, 246–252. [Google Scholar] [CrossRef]
- Baker, C.; Karsy, M.; Couldwell, W.T. Resection of pituitary tumor with lateral extension to the temporal fossa: The toothpaste extrusion technique. Cureus 2019, 11, e5953. [Google Scholar] [CrossRef] [PubMed]
- Park, H.H.; Sung, K.S.; Moon, J.H.; Kim, E.H.; Kim, S.H.; Lee, K.S.; Hong, C.K.; Chang, J.H. Lateral supraorbital versus pterional approach for parachiasmal meningiomas: Surgical indications and esthetic benefits. Neurosurg. Rev. 2020, 43, 313–322. [Google Scholar] [CrossRef] [PubMed]
- Zada, G.; Du, R.; Laws, E.R., Jr. Defining the “edge of the envelope”: Patient selection in treating complex sellar-based neoplasms via transsphenoidal versus open craniotomy. J. Neurosurg. 2011, 114, 286–300. [Google Scholar] [CrossRef] [PubMed]
- Goshtasbi, K.; Lehrich, B.M.; Abouzari, M.; Abiri, A.; Birkenbeuel, J.; Lan, M.Y.; Wang, W.H.; Cadena, G.; Hsu, F.P.K.; Kuan, E.C. Endoscopic versus nonendoscopic surgery for resection of pituitary adenomas: A national database study. J. Neurosurg. 2020, 134, 816–824. [Google Scholar] [CrossRef]
- Alam, S.; Ferini, G.; Muhammad, N.; Ahmed, N.; Wakil, A.N.M.; Islam, K.M.A.; Arifin, M.S.; Al Mahbub, A.; Habib, R.; Mojumder, M.R.; et al. Skull base approaches for tuberculum sellae meningiomas: Institutional experience in a series of 34 patients. Life 2022, 12, 492. [Google Scholar] [CrossRef]
- Komotar, R.J.; Starke, R.M.; Raper, D.M.; Anand, V.K.; Schwartz, T.H. Endoscopic endonasal versus open transcranial resection of anterior midline skull base meningiomas. World Neurosurg. 2012, 77, 713–724. [Google Scholar] [CrossRef]
- Kong, D.S.; Hong, C.K.; Hong, S.D.; Nam, D.H.; Lee, J.I.; Seol, H.J.; Oh, J.; Kim, D.G.; Kim, Y.H. Selection of endoscopic or transcranial surgery for tuberculum sellae meningiomas according to specific anatomical features: A retrospective multicenter analysis (KOSEN-002). J. Neurosurg. 2018, 130, 838–847. [Google Scholar] [CrossRef]
- Liu, J.K.; Weiss, M.H.; Couldwell, W.T. Surgical approaches to pituitary tumors. Neurosurg. Clin. N. Am. 2003, 14, 93–107. [Google Scholar] [CrossRef]
- Apuzzo, M.L.; Heifetz, M.D.; Weiss, M.H.; Kurze, T. Neurosurgical endoscopy using the side-viewing telescope. J. Neurosurg. 1977, 46, 398–400. [Google Scholar] [CrossRef]
- Jho, H.D.; Carrau, R.L. Endoscopic endonasal transsphenoidal surgery: Experience with 50 patients. J. Neurosurg. 1997, 87, 44–51. [Google Scholar] [CrossRef]
- Pangal, D.J.; Cote, D.J.; Ruzevick, J.; Yarovinsky, B.; Kugener, G.; Wrobel, B.; Ference, E.H.; Swanson, M.; Hung, A.J.; Donoho, D.A.; et al. Robotic and robot-assisted skull base neurosurgery: Systematic review of current applications and future directions. Neurosurg. Focus 2022, 52, E15. [Google Scholar] [CrossRef] [PubMed]
- Kasemsiri, P.; Prevedello, D.M.; Otto, B.A.; Old, M.; Ditzel Filho, L.; Kassam, A.B.; Carrau, R.L. Endoscopic endonasal technique: Treatment of paranasal and anterior skull base malignancies. Braz. J. Otorhinolaryngol. 2013, 79, 760–779. [Google Scholar] [CrossRef] [PubMed]
- Couldwell, W.T.; Weiss, M.H.; Rabb, C.; Liu, J.K.; Apfelbaum, R.I.; Fukushima, T. Variations on the standard transsphenoidal approach to the sellar region, with emphasis on the extended approaches and parasellar approaches: Surgical experience in 105 cases. Neurosurgery 2004, 55, 539–547, discussion 547–550. [Google Scholar] [CrossRef]
- Achey, R.L.; Karsy, M.; Azab, M.A.; Scoville, J.; Kundu, B.; Bowers, C.A.; Couldwell, W.T. Improved surgical safety via intraoperative navigation for transnasal transsphenoidal resection of pituitary adenomas. J. Neurol. Surg. B Skull Base 2019, 80, 626–631. [Google Scholar] [CrossRef] [PubMed]
- Louis, R.G.; Eisenberg, A.; Barkhoudarian, G.; Griffiths, C.; Kelly, D.F. Evolution of minimally invasive approaches to the sella and parasellar region. Int. Arch. Otorhinolaryngol. 2014, 18, S136–S148. [Google Scholar] [CrossRef] [PubMed]
- Ottenhausen, M.; Rumalla, K.; Alalade, A.F.; Nair, P.; La Corte, E.; Younus, I.; Forbes, J.A.; Ben Nsir, A.; Banu, M.A.; Tsiouris, A.J.; et al. Decision-making algorithm for minimally invasive approaches to anterior skull base meningiomas. Neurosurg. Focus 2018, 44, E7. [Google Scholar] [CrossRef]
- Abou-Al-Shaar, H.; Krisht, K.M.; Cohen, M.A.; Abunimer, A.M.; Neil, J.A.; Karsy, M.; Alzhrani, G.; Couldwell, W.T. Cranio-orbital and orbitocranial approaches to orbital and intracranial disease: Eye-opening approaches for neurosurgeons. Front. Surg. 2020, 7, 1. [Google Scholar] [CrossRef]
- Klironomos, G.; Dehdashti, A.R. Orbitozygomatic craniotomy and trans-sylvian approach for resection of a tuberculum sella meningioma with extension to the posterior fossa. Neurosurg. Focus 2017, 43 (video suppl. 2), V13. [Google Scholar] [CrossRef]
- Figueiredo, E.G.; Deshmukh, P.; Nakaji, P.; Crusius, M.U.; Crawford, N.; Spetzler, R.F.; Preul, M.C. The minipterional craniotomy: Technical description and anatomic assessment. Neurosurgery 2007, 61, 256–264, discussion 264–265. [Google Scholar] [CrossRef]
- Altay, T.; Patel, B.C.; Couldwell, W.T. Lateral orbital wall approach to the cavernous sinus. J. Neurosurg. 2012, 116, 755–763. [Google Scholar] [CrossRef]
- Klironomos, G.; Mehan, N.; Dehdashti, A.R. Lateral supraorbital craniotomy for tuberculum sella meningioma resection. J. Neurol. Surg. B Skull Base 2018, 79, S263–S264. [Google Scholar] [CrossRef] [PubMed]
- Reisch, R.; Perneczky, A.; Filippi, R. Surgical technique of the supraorbital key-hole craniotomy. Surg. Neurol. 2003, 59, 223–227. [Google Scholar] [CrossRef] [PubMed]
- Tai, A.X.; Sack, K.D.; Herur-Raman, A.; Jean, W.C. The benefits of limited orbitotomy on the supraorbital approach: An anatomic and morphometric study in virtual reality. Oper. Neurosurg. 2020, 18, 542–550. [Google Scholar] [CrossRef]
- Ding, Z.; Wang, Q.; Lu, X.; Qian, X. Endoscopic intradural subtemporal keyhole approach with neuronavigational assistance to the suprasellar, petroclival, and ventrolateral brainstem regions: An anatomic study. World Neurosurg. 2017, 101, 606–614. [Google Scholar] [CrossRef] [PubMed]
- Sabit, I.; Schaefer, S.D.; Couldwell, W.T. Extradural extranasal combined transmaxillary transsphenoidal approach to the cavernous sinus: A minimally invasive microsurgical model. Laryngoscope 2000, 110, 286–291. [Google Scholar] [CrossRef] [PubMed]
- Chauvet, D.; Missistrano, A.; Hivelin, M.; Carpentier, A.; Cornu, P.; Hans, S. Transoral robotic-assisted skull base surgery to approach the sella turcica: Cadaveric study. Neurosurg. Rev. 2014, 37, 609–617. [Google Scholar] [CrossRef] [PubMed]
- Soldozy, S.; Young, S.; Yagmurlu, K.; Norat, P.; Sokolowski, J.; Park, M.S.; Jane, J.A., Jr.; Syed, H.R. Transsphenoidal surgery using robotics to approach the sella turcica: Integrative use of artificial intelligence, realistic motion tracking and telesurgery. Clin. Neurol. Neurosurg. 2020, 197, 106152. [Google Scholar] [CrossRef]
- Zappa, F.; Madoglio, A.; Ferrari, M.; Mattavelli, D.; Schreiber, A.; Taboni, S.; Ferrari, E.; Rampinelli, V.; Belotti, F.; Piazza, C.; et al. Hybrid robotics for endoscopic transnasal skull base surgery: Single-centre case series. Oper. Neurosurg. 2021, 21, 426–435. [Google Scholar] [CrossRef]







Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).