
Imaging Correlates between Headache and Breast Cancer: An [18F]FDG PET Study

 , ,
, ,  , ,
, , 
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Patient Population
2.2. PET Acquisition and Image Analyses
2.3. Statistical Analysis
2.3.1. Population Comparative Analysis
Metabolic Correlates in Primary Headache Types
Tumor Subtype
2.3.2. Single-Subject Analysis
3. Results
3.1. Population Comparative Analysis
3.1.1. Metabolic Correlates in Primary Headache Types
3.1.2. Tumor Subtype
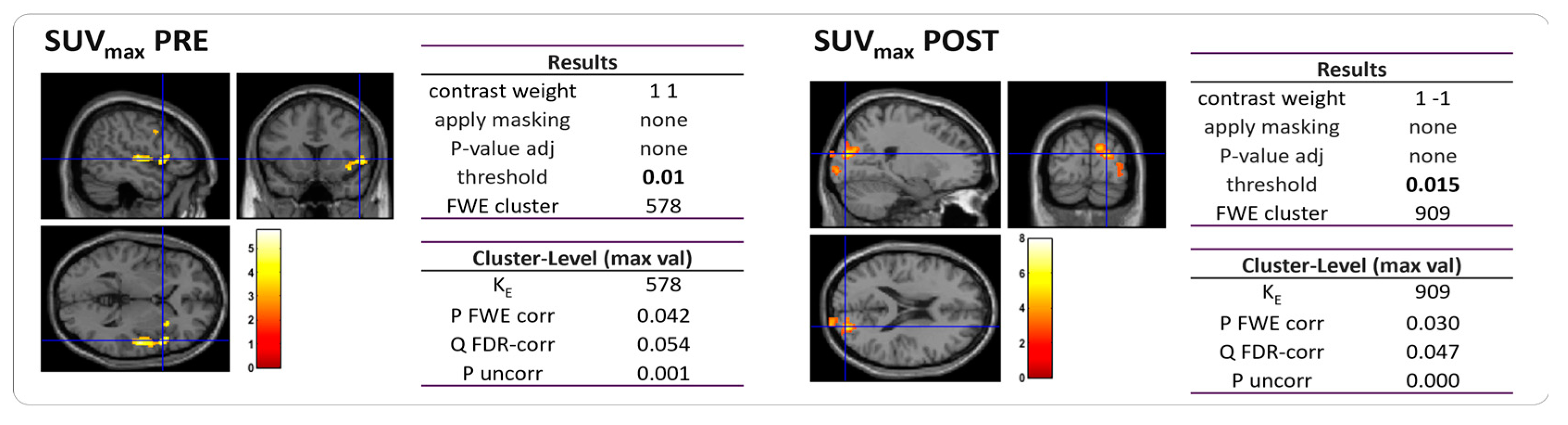
3.2. Single-Subject Analysis
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Vos, T.; Flaxman, A.D.; Naghavi, M.; Lozano, R.; Michaud, C.; Ezzati, M.; Shibuya, K.; Salomon, J.A.; Abdalla, S.; Aboyans, V.; et al. Years lived with disability (YLDs) for 1160 sequelae of 289 diseases and injuries 1990-2010: A systematic analysis for the Global Burden of Disease Study 2010. Lancet 2012, 380, 2163–2196. [Google Scholar] [CrossRef] [PubMed]
- Olesen, J. Headache Classification Committee of the International Headache Society (IHS) The International Classification of Headache Disorders, 3rd edition. Cephalalgia 2018, 38, 1–211. [Google Scholar] [CrossRef]
- Kuruvilla, D.E.; Lipton, R.B. Appropriate Use of Neuroimaging in Headache. Curr. Pain Headache Rep. 2015, 19, 17. [Google Scholar] [CrossRef]
- Hougaard, A.; Amin, F.M.; Larsson, H.B.W.; Rostrup, E.; Ashina, M. Increased intrinsic brain connectivity between pons and somatosensory cortex during attacks of migraine with aura. Hum. Brain Mapp. 2017, 38, 2635–2642. [Google Scholar] [CrossRef] [PubMed]
- Colombo, B.; Rocca, M.A.; Messina, R.; Guerrieri, S.; Filippi, M. Resting-state fMRI functional connectivity: A new perspective to evaluate pain modulation in migraine? Neurol. Sci. 2015, 36, 41–45. [Google Scholar] [CrossRef]
- Cai, M.; Liu, J.; Wang, X.; Ma, J.; Ma, L.; Liu, M.; Zhao, Y.; Wang, H.; Fu, D.; Wang, W.; et al. Spontaneous brain activity abnormalities in migraine: A meta-analysis of functional neuroimaging. Hum. Brain Mapp. 2022, 44, 571–584. [Google Scholar] [CrossRef]
- Zhang, X.; Zhou, J.; Guo, M.; Cheng, S.; Chen, Y.; Jiang, N.; Li, X.; Hu, S.; Tian, Z.; Li, Z.; et al. A systematic review and meta-analysis of voxel-based morphometric studies of migraine. J. Neurol. 2022, 270, 152–170. [Google Scholar] [CrossRef]
- Mahammedi, A.; Wang, L.L.; Vagal, A.S. Imaging Appearance of Migraine and Tension Type Headache. Neurol. Clin. 2022, 40, 491–505. [Google Scholar] [CrossRef]
- Wang, Y.; Wang, Y.; Bu, L.; Wang, S.; Xie, X.; Lin, F.; Xiao, Z. Functional Connectivity Features of Resting-State Functional Magnetic Resonance Imaging May Distinguish Migraine from Tension-Type Headache. Front. Neurosci. 2022, 16, 851111. [Google Scholar] [CrossRef]
- Kim, J.H.; Kim, S.; Suh, S.I.; Koh, S.B.; Park, K.W.; Oh, K. Interictal metabolic changes in episodic migraine: A voxel-based FDG-PET study. Cephalalgia 2010, 30, 53–61. [Google Scholar] [CrossRef]
- Lisicki, M.; D’Ostilio, K.; Coppola, G.; Scholtes, F.; Maertens de Noordhout, A.; Parisi, V.; Schoenen, J.; Magis, D. Evidence of an increased neuronal activation-to-resting glucose uptake ratio in the visual cortex of migraine patients: A study comparing 18FDG-PET and visual evoked potentials. J. Headache Pain 2018, 19, 49. [Google Scholar] [CrossRef] [PubMed]
- Torres-Ferrus, M.; Pareto, D.; Gallardo, V.J.; Cuberas-Borrós, G.; Alpuente, A.; Caronna, E.; Vila-Balló, A.; Lorenzo-Bosquet, C.; Castell-Conesa, J.; Rovira, A.; et al. Cortical metabolic and structural differences in patients with chronic migraine. An exploratory 18FDG-PET and MRI study. J. Headache Pain 2021, 22, 75. [Google Scholar] [CrossRef] [PubMed]
- Gomez-Pilar, J.; Martínez-Cagigal, V.; García-Azorín, D.; Gómez, C.; Guerrero, Á.; Hornero, R. Headache-related circuits and high frequencies evaluated by EEG, MRI, PET as potential biomarkers to differentiate chronic and episodic migraine: Evidence from a systematic review. J. Headache Pain 2022, 23, 95. [Google Scholar] [CrossRef] [PubMed]
- Todd, C.; Lagman-Bartolome, A.M.; Lay, C. Women and Migraine: The Role of Hormones. Curr. Neurol. Neurosci. Reports 2018, 18, 42. [Google Scholar] [CrossRef]
- Ritte, R.; Lukanova, A.; Tjønneland, A.; Olsen, A.; Overvad, K.; Mesrine, S.; Fagherazzi, G.; Dossus, L.; Teucher, B.; Steindorf, K.; et al. Height, age at menarche and risk of hormone receptor-positive and -negative breast cancer: A cohort study. Int. J. Cancer 2013, 132, 2619–2629. [Google Scholar] [CrossRef]
- Britt, K. Menarche, menopause, and breast cancer risk. Lancet Oncol. 2012, 13, 1071–1072. [Google Scholar] [CrossRef] [PubMed]
- Behl, A.; Wani, Z.A.; Das, N.N.; Parmar, V.S.; Len, C.; Malhotra, S.; Chhillar, A.K. Monoclonal antibodies in breast cancer: A critical appraisal. Crit. Rev. Oncol. Hematol. 2023, 183, 103915. [Google Scholar] [CrossRef]
- Bernstein, C.A. Evaluation of headache in patients with cancer. Cancer 2021, 127, 4368–4375. [Google Scholar] [CrossRef]
- De Sanctis, R.; Viganò, A.; Pindilli, S.; Torrisi, R.; Santoro, A. A pilot analysis of headache disorders in breast cancer patients. Neurol. Sci. 2022, 43, 3313–3320. [Google Scholar] [CrossRef]
- Kursun, O.; Yemisci, M.; van den Maagdenberg, A.M.J.M.; Karatas, H. Migraine and neuroinflammation: The inflammasome perspective. J. Headache Pain 2021, 22, 55. [Google Scholar] [CrossRef]
- Yamanaka, G.; Suzuki, S.; Morishita, N.; Takeshita, M.; Kanou, K.; Takamatsu, T.; Suzuki, S.; Morichi, S.; Watanabe, Y.; Ishida, Y.; et al. Role of Neuroinflammation and Blood-Brain Barrier Permutability on Migraine. Int. J. Mol. Sci. 2021, 22, 8929. [Google Scholar] [CrossRef] [PubMed]
- Salahi, M.; Parsa, S.; Nourmohammadi, D.; Razmkhah, Z.; Salimi, O.; Rahmani, M.; Zivary, S.; Askarzadeh, M.; Tapak, M.A.; Vaezi, A.; et al. Immunologic aspects of migraine: A review of literature. Front. Neurol. 2022, 13, 2117. [Google Scholar] [CrossRef] [PubMed]
- Biscetti, L.; De Vanna, G.; Cresta, E.; Bellotti, A.; Corbelli, I.; Cupini, M.L.; Calabresi, P.; Sarchielli, P. Immunological findings in patients with migraine and other primary headaches: A narrative review. Clin. Exp. Immunol. 2022, 207, 11–26. [Google Scholar] [CrossRef] [PubMed]
- Marinovic, D.A.; Hunter, R.L. Examining the interrelationships between mindfulness-based interventions, depression, inflammation, and cancer survival. CA Cancer J. Clin. 2022, 72, 490–502. [Google Scholar] [CrossRef]
- Mathes, R.W.; Malone, K.E.; Daling, J.R.; Davis, S.; Lucas, S.M.; Porter, P.L.; Li, C.I. Migraine in postmenopausal women and the risk of invasive breast cancer. Cancer Epidemiol. Biomark. Prev. 2008, 17, 3116–3122. [Google Scholar] [CrossRef]
- Li, C.I.; Mathes, R.W.; Malone, K.E.; Daling, J.R.; Bernstein, L.; Marchbanks, P.A.; Strom, B.L.; Simon, M.S.; Press, M.F.; Deapen, D.; et al. Relationship between migraine history and breast cancer risk among premenopausal and postmenopausal women. Cancer Epidemiol. Biomark. Prev. 2009, 18, 2030–2034. [Google Scholar] [CrossRef]
- Hesari, E.; Ahmadinezhad, M.; Arshadi, M.; Azizi, H.; Khodamoradi, F. The association between migraine and breast cancer risk: A systematic review and meta-analysis. PLoS ONE 2022, 17, e0263628. [Google Scholar] [CrossRef]
- Ghorbani, A.; Moradi, A.; Gookizadeh, A.; Jokar, S.; Sonbolestan, S. Evaluation of relationship between breast cancer and migraine. Adv. Biomed. Res. 2015, 4, 14. [Google Scholar] [CrossRef]
- Peng, C.; Wu, K.; Chen, X.; Lang, H.; Li, C.; He, L.; Chen, N. Migraine and Risk of Breast Cancer: A Systematic Review and Meta-analysis. Clin. Breast Cancer 2022, 23, e122–e130. [Google Scholar] [CrossRef]
- De Sanctis, R.; Viganò, A.; Torrisi, R.; Santoro, A. Re: Carvedilol blocks neural regulation of breast cancer progression in vivo and is associated with reduced breast cancer mortality in patients: Sympathetic nervous system activity on breast cancer: The story of migraine. Eur. J. Cancer 2021, 152, 250–251. [Google Scholar] [CrossRef]
- Tiberio, P.; Viganò, A.; Ilieva, M.B.; Pindilli, S.; Bianchi, A.; Zambelli, A.; Santoro, A.; De Sanctis, R. The Role of Female Reproductive Hormones in the Association between Migraine and Breast Cancer: An Unanswered Question. Biomedicines 2023, 11, 1613. [Google Scholar] [CrossRef] [PubMed]
- Winter, A.C.; Rice, M.S.; Fortner, R.T.; Eliassen, A.H.; Kurth, T.; Tamimi, R.M. Migraine and breast cancer risk: A prospective cohort study and meta-analysis. J. Natl. Cancer Inst. 2015, 107, 381. [Google Scholar] [CrossRef] [PubMed]
- Ilieva, M.B.; Tiberio, P.; Torrisi, R.; Lanzone, J.; Di Piero, V.; Santoro, A.; Viganò, A.; De Sanctis, R. Profiling the Spectrum of Headache Disorders on 440 Breast Cancer Patients: Highlights on Clinical and Pathological Mechanisms. Biomed 2023, 11, 1059. [Google Scholar] [CrossRef] [PubMed]
- Guedj, E.; Varrone, A.; Boellaard, R.; Albert, N.L.; Barthel, H.; van Berckel, B.; Brendel, M.; Cecchin, D.; Ekmekcioglu, O.; Garibotto, V.; et al. EANM procedure guidelines for brain PET imaging using [18F]FDG, version 3. Eur. J. Nucl. Med. Mol. Imaging 2022, 49, 632–651. [Google Scholar] [CrossRef]
- Boellaard, R.; Delgado-Bolton, R.; Oyen, W.J.G.; Giammarile, F.; Tatsch, K.; Eschner, W.; Verzijlbergen, F.J.; Barrington, S.F.; Pike, L.C.; Weber, W.A.; et al. FDG PET/CT: EANM procedure guidelines for tumour imaging: Version 2.0. Eur. J. Nucl. Med. Mol. Imaging 2014, 42, 328–354. [Google Scholar] [CrossRef] [PubMed]
- Penny, W.; Friston, K.; Ashburner, J.; Kiebel, S.; Nichols, T. Statistical Parametric Mapping: The Analysis of Functional Brain Images; Elsevier: Amsterdam, The Netherlands, 2007; ISBN 9780123725608. [Google Scholar]
- Della Rosa, P.A.; Cerami, C.; Gallivanone, F.; Prestia, A.; Caroli, A.; Castiglioni, I.; Gilardi, M.C.; Frisoni, G.; Friston, K.; Ashburner, J.; et al. A Standardized [18F]-FDG-PET Template for Spatial Normalization in Statistical Parametric Mapping of Dementia. Neuroinformatics 2014, 12, 575–593. [Google Scholar] [CrossRef] [PubMed]
- Caminiti, S.P.; Sala, A.; Presotto, L.; Chincarini, A.; Sestini, S.; Perani, D.; Schillaci, O.; Berti, V.; Calcagni, M.L.; Cistaro, A.; et al. Validation of FDG-PET datasets of normal controls for the extraction of SPM-based brain metabolism maps. Eur. J. Nucl. Med. Mol. Imaging 2021, 48, 2486–2499. [Google Scholar] [CrossRef]
- Wolff, B.J.; Wolff, M.J.; Wolff, J.E. Headache Reporting in Oncology Trials Depends on the Demographics of the Study Population. Vivo 2021, 35, 1939. [Google Scholar] [CrossRef]
- Wu, X.; Wang, M.; Li, S.; Zhang, Y. Migraine and breast cancer risk: A meta-analysis of observational studies based on MOOSE compliant. Medicine 2016, 95, e4031. [Google Scholar] [CrossRef]
- Harder, A.V.E.; Vijfhuizen, L.S.; Henneman, P.; Willems van Dijk, K.; van Duijn, C.M.; Terwindt, G.M.; van den Maagdenberg, A.M.J.M. Metabolic profile changes in serum of migraine patients detected using 1H-NMR spectroscopy. J. Headache Pain 2021, 22, 142. [Google Scholar] [CrossRef]
- Ren, C.; Liu, J.; Zhou, J.; Liang, H.; Wang, Y.; Sun, Y.; Ma, B.; Yin, Y. Low levels of serum serotonin and amino acids identified in migraine patients. Biochem. Biophys. Res. Commun. 2018, 496, 267–273. [Google Scholar] [CrossRef] [PubMed]
- Panconesi, A. Serotonin and migraine: A reconsideration of the central theory. J. Headache Pain 2008, 9, 267–276. [Google Scholar] [CrossRef] [PubMed]
- Viganò, A.; Torrieri, M.C.; Toscano, M.; Puledda, F.; Petolicchio, B.; Sasso D’Elia, T.; Verzina, A.; Ruggiero, S.; Altieri, M.; Vicenzini, E.; et al. Neurophysiological correlates of clinical improvement after greater occipital nerve (GON) block in chronic migraine: Relevance for chronic migraine pathophysiology. J. Headache Pain 2018, 19, 73. [Google Scholar] [CrossRef] [PubMed]
- Matheja, P.; Kuwert, T.; Lüdemann, P.; Weckesser, M.; Kellinghaus, C.; Schuierer, G.; Diehl, B.; Ringelstein, E.B.; Schober, O. Temporal hypometabolism at the onset of cryptogenic temporal lobe epilepsy. Eur. J. Nucl. Med. 2001, 28, 625–632. [Google Scholar] [CrossRef]
- Wen, J.F.; Guo, X.W.; Cao, X.Y.; Liao, J.W.; Ma, P.; Hu, X.S.; Pan, J.Y. A PET imaging study of the brain changes of glucose metabolism in patients with temporal lobe epilepsy and depressive disorder. BMC Med. Imaging 2021, 21, 33. [Google Scholar] [CrossRef]
- Frings, L.; Blazhenets, G.; Binder, R.; Bormann, T.; Hellwig, S.; Meyer, P.T. More extensive hypometabolism and higher mortality risk in patients with right- than left-predominant neurodegeneration of the anterior temporal lobe. Alzheimer’s Res. Ther. 2023, 15, 11. [Google Scholar] [CrossRef]
- Tyrrell, P.J.; Warrington, E.K.; J Frackowiak, R.S.; Rossor, M.N. Progressive degeneration of the right temporal lobe studied with positron emission tomography. J Neurol. Neurosurg. Psychiatry 1990, 53, 1046–1050. [Google Scholar] [CrossRef]
- Groot, C.; Risacher, S.L.; Chen, J.Q.A.; Dicks, E.; Saykin, A.J.; Mac Donald, C.L.; Mez, J.; Trittschuh, E.H.; Mukherjee, S.; Barkhof, F.; et al. Differential trajectories of hypometabolism across cognitively-defined Alzheimer’s disease subgroups. Neuroimage 2021, 31, 102725. [Google Scholar] [CrossRef]
- Zilberter, Y.; Zilberter, M. The vicious circle of hypometabolism in neurodegenerative diseases: Ways and mechanisms of metabolic correction. J. Neurosci. Res. 2017, 95, 2217–2235. [Google Scholar] [CrossRef]
- Mauvais-Jarvis, F.; Clegg, D.J.; Hevener, A.L. The role of estrogens in control of energy balance and glucose homeostasis. Endocr. Rev. 2013, 34, 309–338. [Google Scholar] [CrossRef]
- Tramunt, B.; Smati, S.; Grandgeorge, N.; Lenfant, F.; Arnal, J.F.; Montagner, A.; Gourdy, P. Sex differences in metabolic regulation and diabetes susceptibility. Diabetologia 2020, 63, 453–461. [Google Scholar] [CrossRef]
- Képes, Z.; Aranyi, C.; Forgács, A.; Nagy, F.; Kukuts, K.; Hascsi, Z.; Esze, R.; Somodi, S.; Káplár, M.; Varga, J.; et al. Glucose-level dependent brain hypometabolism in type 2 diabetes mellitus and obesity. Eur. J. Hybrid Imaging 2021, 5, 3. [Google Scholar] [CrossRef] [PubMed]
- Schroyen, G.; Schramm, G.; Van Weehaeghe, D.; Leenaerts, N.; Vande Casteele, T.; Blommaert, J.; Koole, M.; Smeets, A.; Van Laere, K.; Sunaert, S.; et al. Cerebral glucose changes after chemotherapy and their relation to long-term cognitive complaints and fatigue. Front. Oncol. 2022, 12, 5501. [Google Scholar] [CrossRef]
- von Minckwitz, G.; Untch, M.; Blohmer, J.-U.; Costa, S.D.; Eidtmann, H.; Fasching, P.A.; Gerber, B.; Eiermann, W.; Hilfrich, J.; Huober, J.; et al. Definition and impact of pathologic complete response on prognosis after neoadjuvant chemotherapy in various intrinsic breast cancer subtypes. J. Clin. Oncol. 2012, 30, 1796–1804. [Google Scholar] [CrossRef]
- Cortazar, P.; Zhang, L.; Untch, M.; Mehta, K.; Costantino, J.P.; Wolmark, N.; Bonnefoi, H.; Cameron, D.; Gianni, L.; Valagussa, P.; et al. Pathological complete response and long-term clinical benefit in breast cancer: The CTNeoBC pooled analysis. Lancet 2014, 384, 164–172. [Google Scholar] [CrossRef] [PubMed]
- Rasmussen, B.K. Migraine and tension-type headache in a general population: Precipitating factors, female hormones, sleep pattern and relation to lifestyle. Pain 1993, 53, 65–72. [Google Scholar] [CrossRef] [PubMed]
- Krause, D.N.; Warfvinge, K.; Haanes, K.A.; Edvinsson, L. Hormonal influences in migraine—interactions of oestrogen, oxytocin and CGRP. Nat. Rev. Neurol. 2021, 17, 621–633. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Population | TTH | MIG | No Headache | |
|---|---|---|---|---|
| Population (n (%)) | 46 | 18 (39%) | 21 (46%) | 7 (15%) |
| Age (mean) | 50 | 52 | 48 | 53 |
| stdv | 11 | 9 | 12 | 16 |
| median | 52 | 52 | 47 | 55 |
| range | 27–77 | 27–65 | 30–72 | 33–77 |
| Hormone Receptor | ||||
| Estrogen (n and mean ± stdv) | ||||
| ER < 20% | 28 1.4 ± 3.6 | 11 2.1 ± 3.3 | 14 1.1 ± 4.0 | 3 2.5 ± 4.3 |
| ER > 20% | 18 76.4 ± 19.4 | 7 80.0 ± 11.2 | 7 68.6 ± 21.1 | 4 83.8 ± 12.5 |
| Progesteron (n and mean ± stdv) | ||||
| PgR < 20% | 33 0.4 ± 1.1 | 14 0.5 ± 1.5 | 14 0.1 ± 0.3 | 5 0.8 ± 1.8 |
| PgR > 20% | 13 (28%) 61.5 ± 26.3 | 4 46.3 ± 27.2 | 7 65.7 ± 27.5 | 2 77.5 ± 3.5 |
| Ki-67 (n (%) and mean ± stdv) | ||||
| Ki-67 < 20% | 11 16.7 ± 3.1 | 6 15.9 ± 3.5 | 5 17.6 ± 2.5 | 0 - |
| Ki-67 > 20% | 35 49.7 ± 20.2 | 12 47.6 ± 21 | 16 52.2 ± 18.3 | 7 47.5 ± 25.2 |
| Tumor Subtype (n (%)) | ||||
| TNBC | 18 (39%) | 7 (39%) | 8 (44%) | 3 (17%) |
| HER2+ | 8 (17%) | 4 (50%) | 4 (50%) | 0 (0%) |
| LUMHER2 | 20 (43%) | 7 (35%) | 9 (45%) | 4 (20%) |
| Menopause (n (%)) | ||||
| Premenopausal | 21 (43%) | 5 (24%) | 13 (62%) | 3 (14%) |
| Perimenopausal | 4 (11%) | 2 (40%) | 2 (40%) | 0 (0%) |
| Postmenopausal | 21 (46%) | 11 (52%) | 6 (29%) | 4 (19%) |
| BMI (n (%)) | ||||
| <18.5 | 6 (13%) | 2 | 2 | 2 |
| 18.5–23.8 | 20 (44%) | 6 | 11 | 3 |
| 23.9–28.6 | 15 (33%) | 8 | 6 | 1 |
| 28.7–34.9 | 3 (6%) | 1 | 1 | 1 |
| 35–39.9 | 1 (2%) | 0 | 0 | 1 |
| >40 | 1 (2%) | 1 | 0 | 0 |
| Outcome (n (%)) | ||||
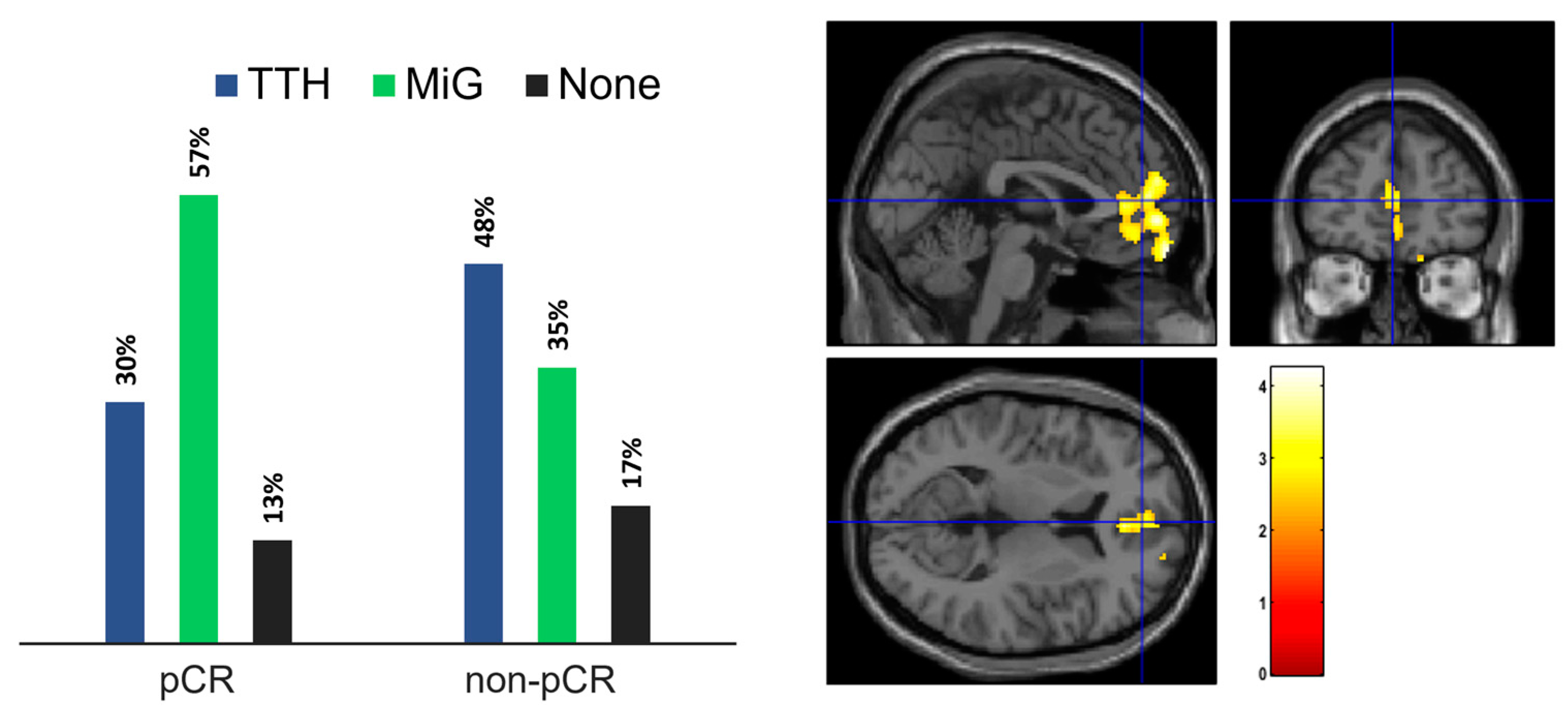
| pCR | 23 (50%) | 7 (30%) | 13 (57%) | 3 (13%) |
| non-pCR | 22 (48%) | 10 (45%) | 8 (36%) | 4 (18%) |
| Not available | 1 (2%) | 1 (100%) | 0 (0%) | 0 (0%) |
| Headache (mean ± std) | ||||
| Frequency * | 1.7 ± 2.1 | 0.8 ± 0.7 | 2.0 ± 2.7 | 0.0 ± 0.4 |
| [18F]FDG PET/CT (n (%)) | ||||
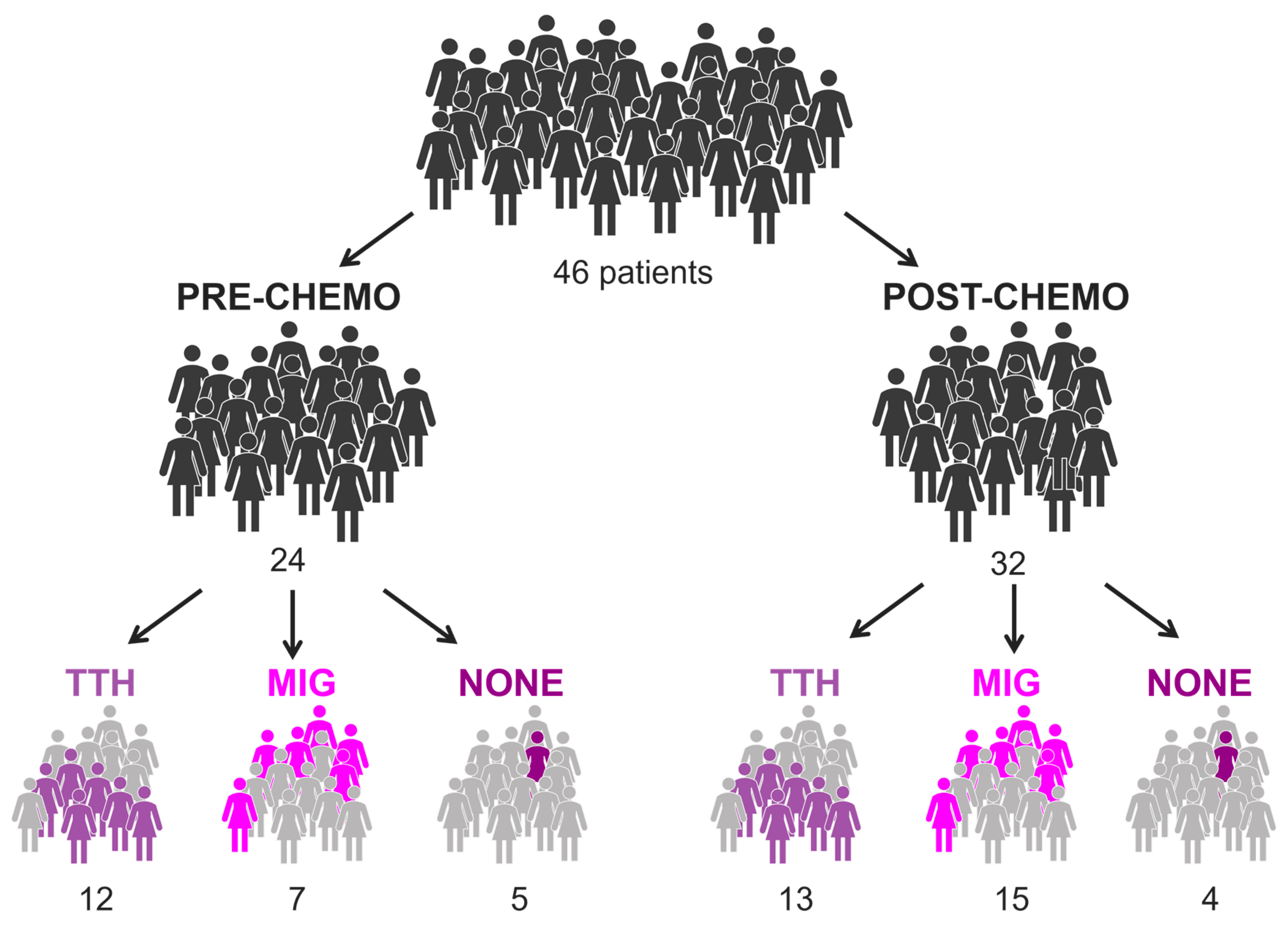
| Pre-chemotherapy | 14 (30%) | 5 | 6 | 3 |
| Post-chemotherapy | 22 (30%) | 6 | 14 | 2 |
| Both | 10 (22%) | 7 | 1 | 2 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Antunovic, L.; Artesani, A.; Viganò, A.; Chiti, A.; Santoro, A.; Sollini, M.; Morbelli, S.D.; De Sanctis, R. Imaging Correlates between Headache and Breast Cancer: An [18F]FDG PET Study. Cancers 2023, 15, 4147. https://doi.org/10.3390/cancers15164147
Antunovic L, Artesani A, Viganò A, Chiti A, Santoro A, Sollini M, Morbelli SD, De Sanctis R. Imaging Correlates between Headache and Breast Cancer: An [18F]FDG PET Study. Cancers. 2023; 15(16):4147. https://doi.org/10.3390/cancers15164147
Chicago/Turabian StyleAntunovic, Lidija, Alessia Artesani, Alessandro Viganò, Arturo Chiti, Armando Santoro, Martina Sollini, Silvia D. Morbelli, and Rita De Sanctis. 2023. "Imaging Correlates between Headache and Breast Cancer: An [18F]FDG PET Study" Cancers 15, no. 16: 4147. https://doi.org/10.3390/cancers15164147
APA StyleAntunovic, L., Artesani, A., Viganò, A., Chiti, A., Santoro, A., Sollini, M., Morbelli, S. D., & De Sanctis, R. (2023). Imaging Correlates between Headache and Breast Cancer: An [18F]FDG PET Study. Cancers, 15(16), 4147. https://doi.org/10.3390/cancers15164147