1. Introduction
The incidence of cancer during childbearing is rising due to the increasing age of first pregnancy [
1]. Ovarian cancer represents 7% of all cancers in pregnant women [
2]. The frequency of adnexal masses in pregnancy differs between different studies—approximately between 0.05% and 2.4% of all pregnancies [
3,
4,
5,
6]. Most of the masses are benign [
3,
4,
5,
6], and malignant ones are reported between 1 and 8% [
3,
4,
5,
6]. Therefore, characterising an ovarian mass during pregnancy is essential to avoid unnecessary treatment and, if treatment is required, to plan it accordingly.
Ultrasound (US) is the first-line modality to characterise adnexal masses, and various diagnostic scores have been proposed and evaluated for sensitivity and specificity to diagnose malignant lesions; the IOTA’s (International Ovarian Tumour Analysis) simple rules provide a sensitivity of 92% and a specificity of 69% [
6,
7]. MRI is indicated when adnexal masses are indeterminate at the US examination [
8,
9,
10]. The success of the use of MRI was due to its better detection of fat and blood content in lesions.
High rates of MRI were reported in young women (pregnant and non-pregnant) for diagnoses in many body organs. Regarding MRI in pregnancy, the prevalence of 1 gadolinium exposure every 860 pregnancies was detected in a large American study [
11]. This prevalence was 4.3-fold greater during the first trimester than during the second trimester and 5.1-fold greater than during the third trimester. In non-pregnant women, the Ovarian–Adnexal Imaging–Reporting–Data System (O-RADS) MRI risk stratification system has been proposed to assign a malignancy probability based on the adnexal lesion’s MRI features [
12,
13]. The score yielded high sensitivity (93%) and specificity (91%) for stratifying the risk of malignancy in adnexal masses [
13]. Moreover, Thomassin-Naggara et al. showed that MRI has a high accuracy (>80%) in the characterisation of adnexal masses in pregnancy, especially when evaluating images using the AdnexMR score, in a cohort study of 1340 women [
12]. Both these scoring systems require the administration of intravenous gadolinium-based contrast agents (GBCAs) [
12,
13]. Some clinical studies have shown that, despite gadolinium-based contrast media during pregnancy being relatively safe, with a low incidence of adverse effects, its use should be limited in clinical practice when strictly necessary [
14,
15,
16,
17]. Recently, the non-Contrast MRI score (NCMS) was proposed [
18]. The score includes five categories—from 1 to 5—and does not require the administration of GBCAs (
Table 1).
The use of the NCMS, which has already shown promising results in non-pregnant patients, may have an added value in the clinical scenario of pregnancy when the use GBCAs is discouraged.
This study aims to investigate the accuracy of non-contrast MRI in the prediction of the risk of malignancy of indeterminate adnexal masses at ultrasonography in pregnancy, comparing subjective assessments (SAs) and NCMSs between radiologists with “different expertise”.
Considering the wide range of possible diagnoses, an additional task of the radiologist was to provide diagnostic hypotheses regarding the nature of the mass.
3. Results
Twenty pregnant women were included in this study.
Table 2 reports their mean age and range, separated by diagnosis. Information about laterality, dimension and histologic results is included in
Supplementary Table S2.
There was no difference in the diagnostic outcomes performed by the expert radiologist using either a subjective assessment (
Table 3a) or the NCMS (
Table 3b).
The diagnostic accuracy of the expert radiologist, reported in
Table 3c, was the same for the use of SAs and the NCMS, with the following values: sensitivity, 85.7%; specificity, 92.3%; positive predictive value, 85.7%; negative predictive value, 92.3%; false positive rate, 7.7%; false negative rate, 14.3%. The expert radiologist correctly classified 90.0% of cases, using both SA and the NCMS.
Different results are shown for the non-expert radiologist with a low rate of correctly identified patients (12/20; 60%), especially for the SA (
Table 4a,b), where the specificity was very low (46.2%).
Table 5a shows the inter-observer agreement between the non-expert and expert radiologists regarding the diagnostic outcomes with SAs: they agreed in 71.4% of the cases with a K = 0.47 (95% CI: 0.48–0.94).
Table 5b shows the inter-observer agreement between the non-expert and the expert radiologists regarding the diagnostic outcomes with the use of the NMCS: they agreed in 90.5% of cases with a K = 0.8 (95% CI: 0.77–1.00).
The analytical description of the diagnoses performed by the two radiologists using the NCMS, according to each single score, is reported in
Table 6. There were differences for score 3 (6/20 for the non-expert and 3/20 and for the expert) and for the diagnosis of malignant masses (more scores of 4 and 5 by the non-expert). It is interesting to note that the non-expert radiologist tended to overcall on the side of malignancy, with two benign masses classified by the expert radiologist as benign and as malignant by the non-expert one.
4. Discussion
This retrospective study aimed at investigating the accuracy of non-contrast MRI in characterising sonographically indeterminate adnexal masses upon US examination in pregnant women and also in evaluating the diagnostic accuracy of radiologists with different expertise. In our study, the diagnostic accuracy was high using the NCMS (80% of correctly classified diagnoses for the non-expert radiologist and 90% for the expert one). Furthermore, we found that the agreement between the expert and the non-expert radiologists using the SA was low, while it improved with the use of the NCMS, although the non-expert radiologist tended to over-diagnose malignancy.
Sahin et al. used a similar approach to characterise 350 adnexal masses in non-pregnant women, with promising results. An NCMS ≥4 was associated with malignancy with an accuracy of 94.2%, a sensitivity of 84.9%, a specificity of 95.9% and a very good positive likelihood ratio [
18], when compared to histology or imaging follow-up at one year. These findings were comparable to those from contrast-enhanced studies [
11]. The interpretation of images without post-contrast enhancement performed in our study was corroborated by the Sahin study.
Although exposure to MRI in pregnancy is relatively safe for the foetus [
20,
21], we know that GBCAs pass through the placental barrier and enter foetal circulation, increasing the risk of rheumatological diseases, inflammatory skin diseases and stillbirth or neonatal undesired birth outcomes [
14,
15,
20,
21], therefore restricting the use of contrast-enhanced MRIs to very select cases where the benefit outweighs the risk, only if the imaging is essential and cannot be delayed [
20,
22].
In this context, our study becomes more valuable.
In the literature, only one study characterised sonographically indeterminate adnexal masses in pregnant women with contrast-enhanced MRIs [
23]. In this study, 88.9% of cases were correctly classified, and the result was very similar to our expert radiologist’s performance (90%) using the NCMS; this finding suggests that contrast is probably not necessary in this delicate scenario. A few other studies have reported data on the prevalence of malignant adnexal masses in pregnancy but not on the diagnostic accuracy of MRIs. Moreover, they are not comparable since they have been carried out in different settings, observing patients with different characteristics, and are not limited to ovarian masses undetermined at the US examination [
3,
24,
25].
Our results highlighted that the diagnostic accuracy was affected by the fact that, in rare cases, there may be subtle differences between a benign and a malignant lesion, causing misinterpretations, thus leading to an increase in false negatives or false positives for both the expert and the non-expert radiologists. One example in our study population, also reported in the literature, was the correct interpretation of decidualised endometrioma [
26,
27,
28,
29,
30,
31,
32]. During pregnancy, decidual endometrium changes are due to high levels of progesterone, so endometrioma can undergo decidualisation. Even if the decidualisation of ovarian endometrioma is rare, when it occurs, it is difficult to differentiate from ovarian cancer. In fact, the presence of irregular wall thickening in the decidualised endometrioma can mimic the papillary projections of ovarian cancer [
26,
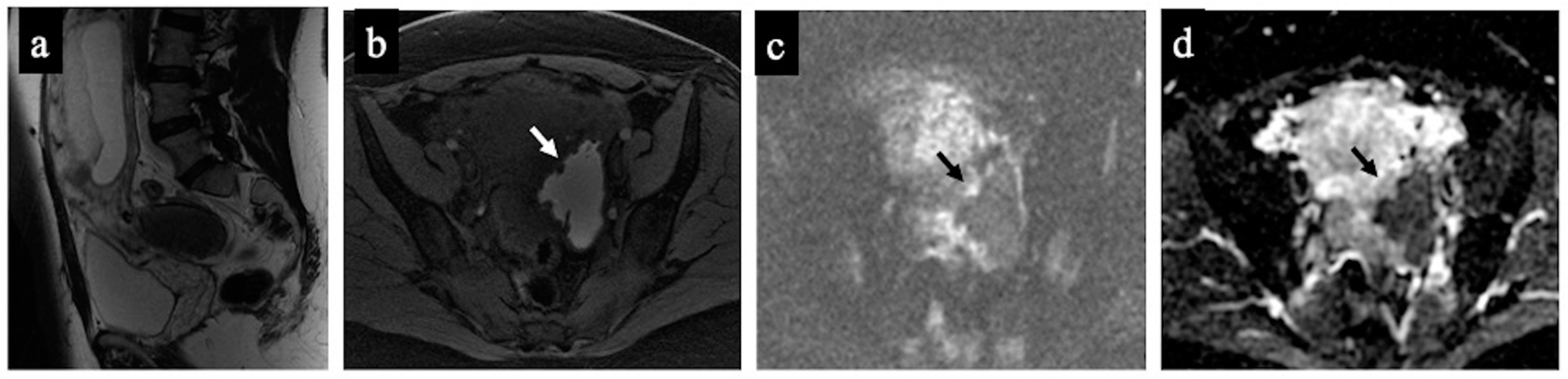
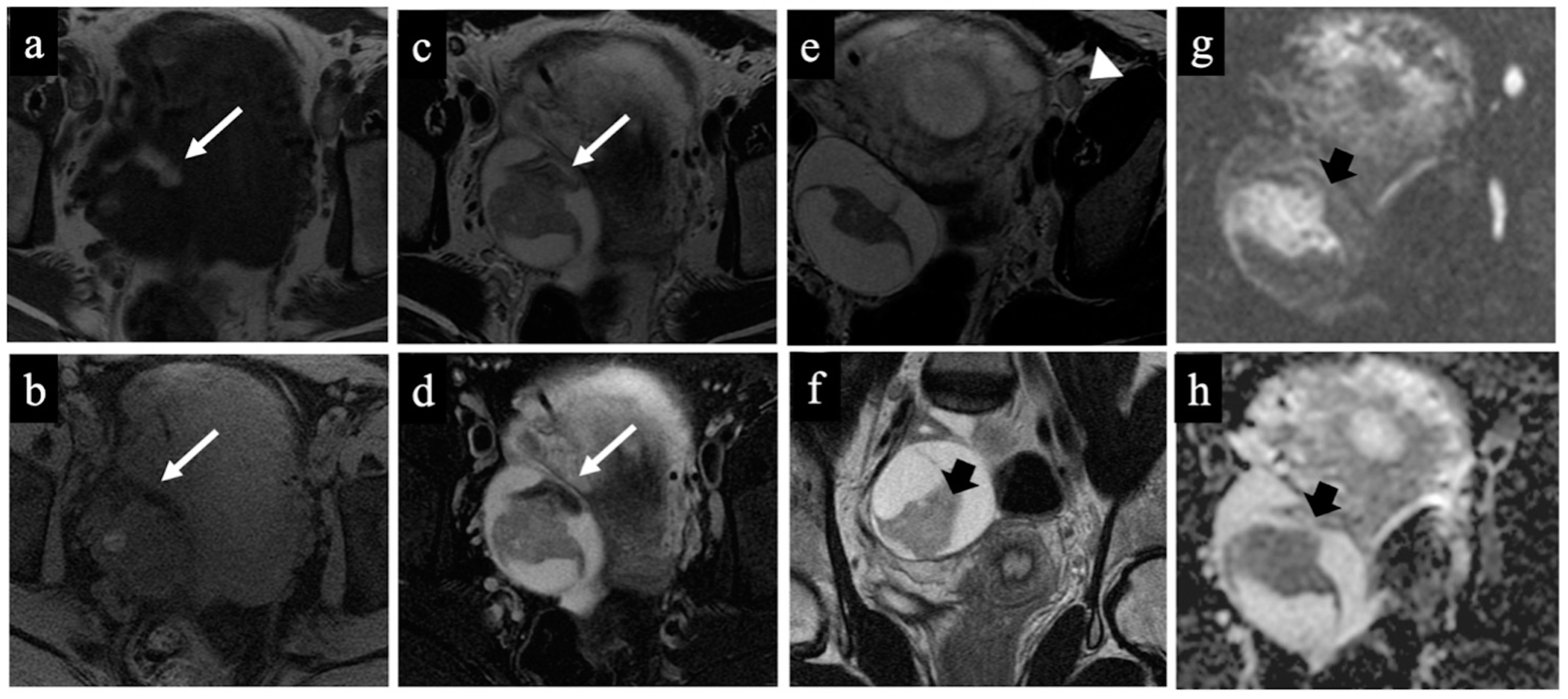
32]. Supported by the existing literature, our results also suggested that the evaluation of the ADC value is key for the correct diagnosis because it is significantly higher in benign disease than in ovarian cancers [
33] (
Figure 1 and
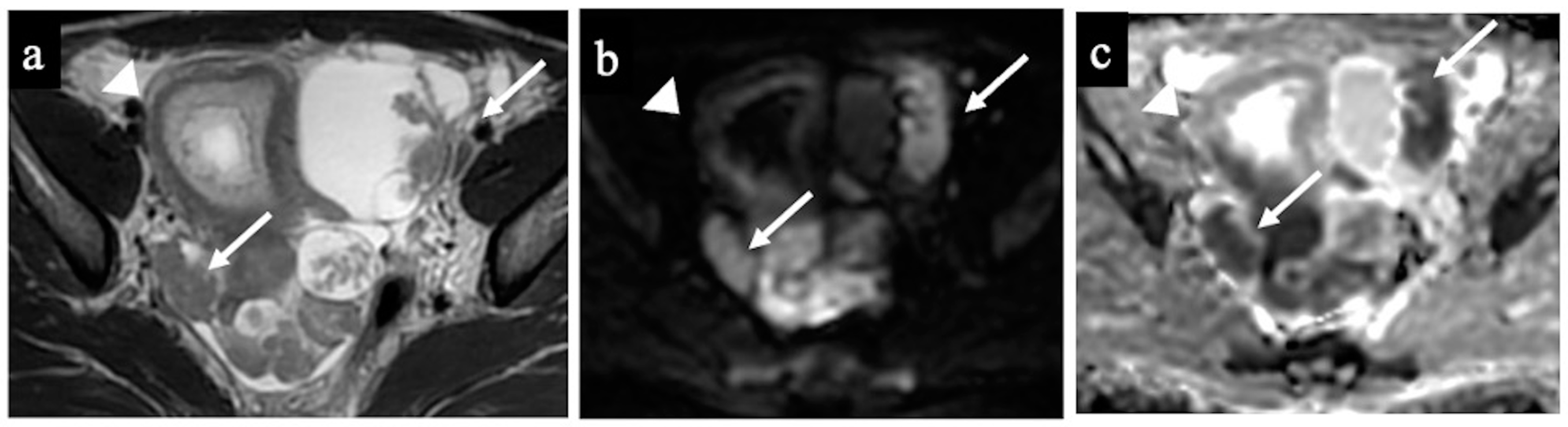
Figure 2). Another difficult case was the interpretation of a borderline cystadenoma, which was classified as benign using the SA, with a score of three in the NCMS by both the expert and non-expert radiologists due to the presence of multiple thin septations without the detection of macroscopic solid tissue. However, at histopathology, it was classified as malignant. No solid tissue was seen on the MRI images, due to the difficulty of detecting micro-invasive components [
34] (
Figure 3). On the other hand, the diagnosis of a benign mature cystic teratoma was correctly made by the expert radiologist, while the lesion was misclassified as malignant by the non-expert radiologist (NCMS 5). In fact, the fat component, which is the main sign of a dermoid cyst, was relatively minimal and was not identified by the non-expert radiologist (
Figure 4).
Figure 5 and
Figure 6 show two cases of correct diagnoses made by the expert and the non-expert radiologists: one case of a struma ovarii, a multilocular cystic mass without solid tissue that was correctly considered benign/NCMS 2 (true negative), and a case of a low-grade ovarian serous cancer with papillary projections and mural nodules (solid tissue) correctly classified as malignant/score 4 (true positive).
The strength of our study was the use of the histopathological results after surgery or the imaging follow-up after one year as the gold standard. Moreover, we evaluated patients with a standard multidisciplinary approach.
Our study has some limitations. First, the retrospective design. Second, the fact that it was performed in a highly specialised institution, and this may provide results that are not easily generalisable to other health institutions. Third, the low number of patients; however, our numbers are not very far from the 31 cases of the only other previous study investigating the diagnostic performance of MRI in pregnant women [
23]. Moreover, adnexal masses in pregnancy are rare, and this is the reason for the low number of cases included; multicentric studies may be considered to improve the sample number.
Although in pregnant women, non-contrast MRI is applied, our results support the use of a quantitative score, i.e., the NCMS, as an accurate tool for the characterisation of adnexal masses. This procedure may help less experienced radiologists to reduce the rate of false negatives or positives, especially in centres not specialised in gynaecological imaging, making MRI interpretation easier and more accurate, also for radiologists who are not experts in the field. Nevertheless, it is crucial to emphasise that the patient’s overall clinical scenario has a pivotal role; clinical reasoning is the key to the diagnostic process and, together with imaging features, is fundamental for the radiologist to reach an accurate diagnosis.


 ,
, 






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}