

Cryopreserved Thyroid Tissue Autotransplant in Pediatric Age Patients: A Feasibility Study and Literature Review


 , , ,
, , , 
Abstract
Simple Summary
Abstract
1. Introduction
2. Materials and Methods
3. Results
Literature Review
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Sakr, M.; Mahmoud, A. Review of Heterotopic Thyroid Autotransplantation. Clin. Exp. Otorhinolaryngol. 2017, 10, 289–295. [Google Scholar] [CrossRef] [PubMed]
- Ray, B.S. Lingual Thyroid. Arch. Surg. 1938, 37, 316. [Google Scholar] [CrossRef]
- Minuto, F.M.; Fazzuoli, L.; Rollandi, G.; Derchi, L.E.; Biassoni, P. Successful autotransplantation of lingual thyroid: 37-year follow-up. Lancet 1995, 346, 910. [Google Scholar] [CrossRef] [PubMed]
- Krátký, J. Levotyroxyn. Vnitr. Lek. 2022, 68, 68–72. [Google Scholar] [CrossRef] [PubMed]
- Perez, C.L.; Araki, F.S.; Graf, H.; de Carvalho, G.A. Serum Thyrotropin Levels Following Levothyroxine Administration at Breakfast. Thyroid 2013, 23, 779–784. [Google Scholar] [CrossRef] [PubMed]
- Wiesner, A.; Gajewska, D.; Paśko, P. Levothyroxine Interactions with Food and Dietary Supplements—A Systematic Review. Pharmaceuticals 2021, 14, 206. [Google Scholar] [CrossRef] [PubMed]
- Chaker, L.; Bianco, A.C.; Jonklaas, J.; Peeters, R.P. Hypothyroidism. Lancet 2017, 390, 1550–1562. [Google Scholar] [CrossRef]
- McHenry, C.R.; Slusarczyk, S.J. Hypothyroidism following hemithyroidectomy: Incidence, risk factors, and management. Surgery 2000, 128, 994–998. [Google Scholar] [CrossRef]
- Hanley, P.; Lord, K.; Bauer, A.J. Thyroid Disorders in Children and Adolescents. JAMA Pediatr. 2016, 170, 1008. [Google Scholar] [CrossRef]
- Duntas, L.H.; Jonklaas, J. Levothyroxine Dose Adjustement to Optimise Therapy Throughout a Patient’s Lifetime. Adv. Ther. 2019, 36, 30–46. [Google Scholar] [CrossRef]
- Jonklaas, J. Optimal Thyroid Hormone Replacement. Endocr. Rev. 2022, 43, 366–404. [Google Scholar] [CrossRef] [PubMed]
- Jang, T.H.; Park, S.C.; Yang, J.H.; Kim, J.Y.; Seok, J.H.; Park, U.S.; Choi, C.W.; Lee, S.R.; Han, J. Cryopreservation and its clinical applications. Integr. Med. Res. 2017, 6, 12–18. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Morris, G.J.; Acton, E. Controlled ice nucleation in cryopreservation—A review. Cryobiology 2013, 66, 85–92. [Google Scholar] [CrossRef] [PubMed]
- Whaley, D.; Damyar, K.; Witek, R.P.; Mendoza, A.; Alexander, M.; Lakey, J.R. Cryopreservation: An Overview of Principles and Cell-Specific Consideration. Cell Transpl. 2021, 30, 0963689721999617. [Google Scholar] [CrossRef] [PubMed]
- Pushkar’, N.S.; Makedonskaia, V.A.; Utevskiĭ, A.M.; Chuĭko, V.A.; Karpenko, L.G. Autoimplantation of cryopreserved (-196 degrees C) thyroid gland parenchyma as a treatment method in postoperative hypothyroidism. Probl. Endokrinol. 1984, 30, 42–46. [Google Scholar]
- Shimizu, K.; Kumita, S.; Kitamura, Y.; Nagahama, M.; Kitagawa, W.; Akasu, H.; Oshina, T.; Kumasaki, T.; Tanaka, S. Trial of autotransplantation of cryopreserved thyroid tissue for postoperative hypothyroidism in patients with Graves’ disease. J. Am. Coll. Surg. 2002, 194, 14–22. [Google Scholar] [CrossRef] [PubMed]
- Shimizu, K.; Kitamura, Y.; Nagahama, M.; Shoji, T. A fundamental study of the thyroid transplantation for the patient with irreversible hypothyroidism (the first report: An autotransplantation of cryopreserved thyroid): Preliminary report. Nihon Geka Gakkai Zasshi 1991, 92, 1728. [Google Scholar] [PubMed]
- Papaziogas, B.; Antoniadis, A.; Lazaridis Ch Makris, J.; Kotakidou, R.; Paraskevas, G.; Papaziogas, T. Functional capacity of the thyroid autograft: An experimental study. J. Surg. Res. 2002, 103, 223–227. [Google Scholar] [CrossRef] [PubMed]
- Kitamura, Y.; Shimizu, K.; Nagahama, M.; Shoji, T. Cryioreservation of thyroid pieces—Optimal freezing condition and recovery. Nihon Geka Gakkai Zasshi 1994, 95, 14–20. [Google Scholar]
- Chen, Z.; Ding, Y.; Zhang, H. Cryopreservation of suckling pig hepatocytes. Ann. Clin. Lab. Sci. 2001, 31, 391–398. [Google Scholar]
- Horváthy, D.B.; Simon, M.; Schwarz, C.M.; Masteling, M.; Vácz, G.; Hornyák, I.; Lacza, Z. Serum albumin as a local therapeutic agent in cell therapy and tissue engineering. Biofactors 2017, 43, 315–330. [Google Scholar] [CrossRef] [PubMed]
- Klbik, I.; Čechová, K.; Maťko, I.; Lakota, J.; Šauša, O. On crystallization of water confined in liposomes and cryoprotective action of DMSO. RSC Adv. 2022, 12, 2300–2309. [Google Scholar] [CrossRef] [PubMed]
- Mandumpal, J.B.; Kreck, C.A.; Mancera, R.L. A molecular mechanism of solvent cryoprotection in aqueous DMSO solutions. Phys. Chem. Chem. Phys. 2011, 13, 3839. [Google Scholar] [CrossRef] [PubMed]
- Spinelli, C.; Strambi, S.; Rossi, L.; Bakkar, S.; Massimino, M.; Ferrari, A.; Collini, P.; Cecchetto, G.; Bisogno, G.; Inserra, A.; et al. Surgical management of papillary thyroid carcinoma in childhood and adolescence: An Italian multicenter study on 250 patients. J. Endocrinol. Investig. 2016, 39, 1055–1059. [Google Scholar] [CrossRef] [PubMed]
- Horch, D.F.; Mehlitz, T.; Laurich, O.; Abel, A.; Reuter, S.; Pratschke, H.; Neuhaus, P.; Wesslau, C. Organ transport temperature box: Multicenter study on transport temperature of organs. Transplant. Proc. 2002, 34, 2320. [Google Scholar] [CrossRef] [PubMed]
- Antonelli, A.; Ferrari, S.M.; Fallahi, P.; Frascerra, S.; Piaggi, S.; Gelmini, S.; Lupi, C.; Minuto, M.; Berti, P.; Benvenga, S.; et al. Dysregulation of secretion of CXC alpha-chemokine CXCL10 in papillary thyroid cancer: Modulation by peroxisome proliferator-activated receptor-gamma agonists. Endocr.-Relat. Cancer 2009, 16, 1299–1311. [Google Scholar] [CrossRef] [PubMed]
- Blumenthal, H.T.; Walsh, L.B. Survival of Guinea Pig Thyroid and Parathyroid Autotransplants Previously Subjected to Extremely Low Temperatures. Exp. Biol. Med. 1950, 73, 62–67. [Google Scholar] [CrossRef] [PubMed]
- Liddle, E.B.; Wittenstein, G.J.; Swan, H. Studies on autotransplantation of thyroid and adrenal gland in dogs. Surg. Forum 1953, 4, 701–705. [Google Scholar] [PubMed]
- Hamolski, M.W.; Gierlach, Z.S. Hepatic Catabolism of Thyroid Hormone Studied by Radioactive Iodine in Splenic Autotransplants. Exp. Biol. Med. 1952, 80, 288–291. [Google Scholar] [CrossRef]
- Kawamura, K. Studies on organ transplantation. J. Exp. Med. 1919, 30, 45–63. [Google Scholar] [CrossRef]
- Goodman, C. The transplantation of the thyroid gland in dogs. Am. J. Med. Sci. 1916, 152, 348–354. [Google Scholar] [CrossRef]
- Hesselberg, C. A comparison of autoplastic and homeoplastic transplantation of thyroid tissue in the guinea pig. J. Exp. Med. 1915, 21, 164–178. [Google Scholar] [CrossRef] [PubMed]
- O’Malley, B.W.; Finegold, M.J.; Ledley, F.D. Autologous, Orthotopic Thyroid Follicular Cell Transplantation: A Surgical Component of Ex Vivo Somatic Gene Therapy. Otolaryngol.-Head Neck Surg. 1993, 108, 51–62. [Google Scholar] [CrossRef]
- Chernozemsky, I.; Christov, K. Autotransplantation and Homotransplantation of Thyroid Gland in the Hamster Cheek Pouch. Nature 1967, 215, 70. [Google Scholar] [CrossRef] [PubMed]
- Pasteur, I.P.; Tronko, N.D.; Drozdovich, I.I.; Turchin, I.S.; Balla, I.A. Thyroid Transplantation: Possibility of Application for the Treatment of Persistent Hypothyroidism and Study of Mechanisms of Interaction between Graft and Hypothalamic-Pituitary Axis of Recipient. In Animal Cell Technology: Basic & Applied Aspects; Kitagawa, Y., Matsuda, T., Iijima, S., Eds.; Springer: Dordrecht, The Netherlands, 1999; pp. 289–293. [Google Scholar] [CrossRef]
- Gál, I.; Mikó, I.; Furka, I.; Nagy, D. Autotransplantation of cryopreserved thyroid tissue in dogs. Magy. Sebészet 2005, 58, 93–99. [Google Scholar] [PubMed]
- Dobrinja, C.; Trevisan, R.; Trevisan, G.; Liguori, G. Autotransplantation of thyroid tissue in rats. An experimental study. Ann. Ital. Chir. 2008, 79, 389–395. [Google Scholar]
- Shimizu, K.; Nagahama, M.; Kitamura, Y.; Igarashi, T.; Aida, N.; Tanaka, S. Improvement of thyroid function after autotransplantation of cryopreserved thyroid tissues in rats: Clinical application of the procedure to patients with persistent hypothyroid Graves’ disease after thyroidectomy. Thyroidol. Clin. Exp. 1996, 8, 55–62. [Google Scholar]
- Iwai, H.; Yamashita, T.; Kubo, N.; Tomoda, K.; Tsujikawa, S.; Inaba, M.; Ikehara, S.; Kumazawa, T. Thyroid follicle transplantation by percutaneous injection. Acta Otolaryngol. Suppl. 1993, 500, 135–137. [Google Scholar] [CrossRef] [PubMed]
- Brachetto-Brian, D.; Grinberg, R. The histological process of thyroid intrasplenic autografts in thyroidectomized rats. C R Seances Soc. Biol. Fil. 1952, 146, 136–137. [Google Scholar]
- Vasconcellos, M.; Carra, A.M.; Franco, O.B.; Baetas-da-Cruz, W.; Ferreira, M.L.; Silva, P.C.; Lopes de Souza, S.A.; Miranda-Alves, L.; de Carvalho, D.P.; Schanaider, A. Cryopreserved Rat Thyroid Autotransplantation in the Treatment of Postoperative Hypothyroidism. Front. Endocrinol. 2021, 12, 625173. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Nagamine, S. Experimental studies on the autotransplantation of thyroid gland using micro-vascular anastomoses. Nippon. Geka Hokan 1968, 37, 32–57. [Google Scholar] [PubMed]
- Karaman, M.; Tuncel, A.; Sheidaei, S.; Karabulut, M.H.; Tatlıpınar, A. Functional capacity of the thyroid autograft and heterograft: An experimental study. Head Neck 2012, 34, 702–708. [Google Scholar] [CrossRef] [PubMed]
- Yüce, İ.; Okuducu, H.; Çağlı, S.; Vural, A.; Gündoğdu, R.; Abdülrezzak, Ü.; Arlı, T.; Aydın, M.; Güney, E. Experimental autotransplantation and cryopreservation of the thyroid gland. Head Neck 2015, 37, 940–945. [Google Scholar] [CrossRef] [PubMed]
- Narayan, K.; Cliff, W.J. In vivo morphology and ultrastructure of thyroid autografts in rabbit ear chambers. Q. J. Exp. Physiol. 1981, 66, 237–252. [Google Scholar] [CrossRef] [PubMed]
- Swan, H.; Jenkins, D.; Schemmel, J. Thyroid Autograft. A 12-year follow-up. Arch. Surg. 1967, 94, 817–820. [Google Scholar] [CrossRef] [PubMed]
- Swan, H.; Jenkins, D.; MacGregor, C. Autotransplantation of the Lingual Thyroid. Arch. Surg. 1958, 76, 458. [Google Scholar] [CrossRef] [PubMed]
- Low, H.B. Thyroid Grafts. Arch. Surg. 1961, 83, 767. [Google Scholar] [CrossRef]
- Steinwald, O.P.; Muehrcke, R.C.; Economou, S.G. Surgical Correction of Complete Lingual Ectopia of the Thyroid Gland. Surg. Clin. N. Am. 1970, 50, 1177–1186. [Google Scholar] [CrossRef] [PubMed]
- Neinas, F.W.; Gorman, C.A.; Devine, K.D.; Woolner, L.B. Lingual thyroid. Clinical characteristics of 15 cases. Ann. Intern. Med. 1973, 79, 205. [Google Scholar] [CrossRef]
- Lawson, R.S. Case of lingual thyroid with successful grafting after operative removal. ANZ J. Surg. 1957, 26, 241–243. [Google Scholar] [CrossRef]
- Monib, S.; Habashy, H.; Ibrahim, M. Thyroid autotransplantation after total thyroidectomy in multi-nodular goiter—A case series analysis. Indian J. Surg. 2021, 83, 1451–1456. [Google Scholar] [CrossRef]
- El Hadad, L.H.; Mohsen, A.A.; El Sanadeki, M.N.; Mahran, K. Assessment of Survival and Function of Heterotopic Auto-transplanted Thyroid Tissue after Total Thyroidectomy for Non-toxic Multinodular Goiters. Indian J. Public Health Res. Dev. 2020, 11, 1647. [Google Scholar] [CrossRef]
- Gamal, A.M.; Elnaga, N.E.; Ayoub, M.T.; Farghally, A.R. Thyroid autotransplantation following total thyroidectomy in benign thyroid disorders: A new technique to avoid postoperative hypothyroidism. Int. Surg. J. 2019, 6, 2267. [Google Scholar] [CrossRef]
- Mohsen, A.A.; Nada, A.A.; Ibrahim, M.Y.; Ghaleb, A.H.; Abou-Gabal, M.A.; Mohsen, A.A.; Wassef, A.T. Technique and outcome of autotransplanting thyroid tissue after total thyroidectomy for simple multinodular goiters. Asian J. Surg. 2017, 40, 17–22. [Google Scholar] [CrossRef] [PubMed]
- Sakr, M.; El-kherm, Y.; Abo-Elwafa, W.; Mahmoud, A.; Fathi, I. Heterotopic thyroid autotransplantation: A preliminary clinical study. Head Neck 2018, 40, 34–45. [Google Scholar] [CrossRef] [PubMed]
- Dayal, D.; Gupta, K.R.; Singh, M. Ectopic lingual thyroid autotransplantation. Indian J. Otolaryngol. 1968, 20, 124–127. [Google Scholar] [CrossRef]
- Jones, P. Autotransplantation in Lingual Ectopia of the Thyroid Gland: Review of the Literature and Report of a Successful Case. Arch. Dis. Child. 1961, 36, 164–170. [Google Scholar] [CrossRef] [PubMed]
- Turcot, J. Lingual and hyoid thyroid. Am. J. Surg. 1962, 104, 677–681. [Google Scholar] [CrossRef] [PubMed]
- Al-Samarrai, A.Y.; Crankson, S.J.; Al-Jobori, A. Autotransplantation of lingual thyroid into the neck. Br. J. Surg. 2005, 75, 287. [Google Scholar] [CrossRef]
- Wapshaw, H. Lingual thyroid a report of a case with unusual histology. Br. J. Surg. 2005, 30, 160–165. [Google Scholar] [CrossRef]
- Hilless, A.D.; Black, J.E. Lingual ectopia of the thyroid gland and autotransplantation. Br. J. Surg. 2005, 63, 924–926. [Google Scholar] [CrossRef] [PubMed]
- Sankar, R.; Roy, P.G.; Saund, M.S.; Thusoo, T.K.; Roy, D. Fate of Human Thyroid Tissue Autotransplants. Surg. Today 2003, 33, 571–576. [Google Scholar] [CrossRef] [PubMed]
- Okamoto, T.; Fujimoto, Y.; Obara, T.; Ito, J.; Kodama, T.; Kusakabe, K. Trial of Thyroid Autotransplantation in Patients with Graves’ Disease Whose Remnant Thyroid has Unintentionally been Made too Small at Subtotal Thyroidectomy. Endocrinol. Jpn. 1990, 37, 95–101. [Google Scholar] [CrossRef] [PubMed]
- Sheverdin, I.P. The results of a 15-year observation of patients with an autotransplant of thyroid gland fragments performed to prevent postoperative hypothyroidism. Vestn. Khirurgii Im. II Grek. 1992, 148, 152–156. [Google Scholar]
- Danis, R.K. An alternative in management of lingual thyroid: Excision with implantation. J. Pediatr. Surg. 1973, 8, 869–870. [Google Scholar] [CrossRef] [PubMed]
- Ingle, D.J.; Cragg, R.W. The regeneration of autografts of thyroid tissue in partially and completely thyroidectomized rats. Endocrinology 1939, 24, 550–552. [Google Scholar] [CrossRef]
- Schanaider, A.; Barboza, T.; Vasconcellos, M.; Gutfilen-Schlesinger, G.; Augusto, S. Rat thyroid graft transplantation after cryopreservation with scintigraphic standardization for an experimental study. Clinics 2022, 77, 100065. [Google Scholar] [CrossRef] [PubMed]
- Mohamed Kotb, M.B.; Hemdan, A.M.; Ayoub, M.T. Thyroid Autotransplantation after Total Thyroidectomy in Benign Thyroid Diseases. Egypt. J. Hosp. Med. 2022, 89, 5544–5549. [Google Scholar] [CrossRef]
- Weider, D.J.; Parker, W. Lingual Thyroid. Ann. Otol. Rhinol. Laryngol. 1977, 86, 841–848. [Google Scholar] [CrossRef]
- Spinelli, C.; Ghionzoli, M.; Oreglio, C.; Sanna, B.; De Napoli, L.; Morganti, R.; Antonelli, A.; Morabito, A.; Miccoli, P. Increased trend of thyroid cancer in childhood over the last 30 years in EU countries: A call for the pediatric surgeon. Eur. J. Pediatr. 2022, 181, 3907–3913. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Moleti, M.; Aversa, T.; Crisafulli, S.; Trifirò, G.; Corica, D.; Pepe, G.; Cannavò, L.; Di Mauro, M.; Paola, G.; Fontana, A.; et al. Global incidence and prevalence of differentiated thyroid cancer in childhood: Systematic review and meta-analysis. Front. Endocrinol. 2023, 14, 1270518. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Spinelli, C.; Ghionzoli, M.; Zinaida, S. IL Carcinoma Della Tiroide Nei Giovani Adulti Dopo Chernobyl E Fukushima; Pisa University Press: Pisa, Italy, 2023. [Google Scholar]
- Bojic, S.; Murray, A.; Bentley, B.L.; Spindler, R.; Magalhes, J. Winter is coming: The future of cryopreservation. BMC Biol. 2021, 19, 56. [Google Scholar] [CrossRef] [PubMed]
- Mazur, P.; Leibo, S.P.; Chu, E.Y. A two-factor hypothesis of freezing injury. Exp. Cell Res. 1972, 71, 345–355. [Google Scholar] [CrossRef] [PubMed]
- Pegg, D.E. Mechanisms of freezing damage. Symp. Soc. Exp. Biol. 1987, 41, 363–378. [Google Scholar]
- Han, B.; Bischof, J.C. Direct cell injury associated with eutectic crystallization during freezing. Cryobiology 2004, 48, 8–21. [Google Scholar] [CrossRef] [PubMed]
- Akhoondi, M.; Oldenhof, M.H.; Sieme, H.; Wolkers, W.F. Freezing-induced cellular and membrane dehydration in the presence of cryoprotective agents. Mol. Membr. Biol. 2012, 29, 197–206. [Google Scholar] [CrossRef]
- Pegg, D.E. Principles of Cryopreservation. Methods Mol. Biol. 2007, 368, 39–57. [Google Scholar] [CrossRef] [PubMed]
- Lee, E.; Baiz, C.R. How cryoprotectants work: Hydrogen-bonding in low-temperature vitrified solutions. Chem. Sci. 2022, 13, 9980–9984. [Google Scholar] [CrossRef] [PubMed]
- Karlsson, J.O.; Toner, M. Long-term storage of tissues by cryopreservation: Critical issues. Biomaterials 1996, 17, 243–256. [Google Scholar] [CrossRef]
- The Practice Committees of the American Society for Reproductive Medicine and the Society for Assisted Reproductive Technology. Mature oocyte cryopreservation: A guideline. Fertil. Steril. 2013, 99, 37–43. [Google Scholar] [CrossRef]
- Poisson, J.S.; Acker, J.P.; Briard, J.G.; Meyer, J.E.; Ben, R.N. Modulating Intracellular Ice Growth with Cell-Permeating Small-Molecule Ice Recrystallization Inhibitors. Langmuir 2019, 35, 7452–7458. [Google Scholar] [CrossRef]
- Berridge, M.V.; Herst, P.M.; Tan, A.S. Tetrazolium dyes as tools in cell biology: New insights into their cellular reduction. Biotechnol. Annu. Rev. 2005, 11, 127–152. [Google Scholar] [CrossRef]
- Spinelli, C.; Ghionzoli, M.; Sahli, L.I.; Guglielmo, C.; Frascella, S.; Romano, S.; Ferrari, C.; Gennari, F.; Conzo, G.; Morganti, R.; et al. DICER1 Syndrome: A Multicenter Surgical Experience and Systematic Review. Cancers 2023, 15, 3681. [Google Scholar] [CrossRef] [PubMed]
- Viduetsky, A.; Herrejon, C.L. Sonographic Evaluation of Thyroid Size: A Review of Important Measurement Parameters. J. Diagn. Med. Sonogr. 2019, 35, 206–210. [Google Scholar] [CrossRef]
- Pankow, B.G.; Michalak, J.; McGee, M.K. Adult Human Thyroid Weight. Health Phys. 1985, 49, 1097–1104. [Google Scholar] [CrossRef] [PubMed]
- Nardi, F.; Basolo, F.; Crescenzi, A.; Fadda, G.; Frasoldati, A.; Orlandi, F.; Palombini, L.; Papini, E.; Zini, M.; Pontecorvi, A.; et al. Italian consensus for the classification and reporting of thyroid cytology. J. Endocrinol. Investig. 2014, 37, 593–599. [Google Scholar] [CrossRef] [PubMed]
- Koh, Y.W.; Lee, S.W.; Choi, E.C.; Lee, J.D.; Mok, J.O.; Kim, H.K.; Koh, E.S.; Lee, J.Y.; Kim, S.C. Prediction of hypothyroidism after hemithyroidectomy: A biochemical and pathological analysis. Eur. Arch. Otorhinolaryngol. 2008, 265, 453–457. [Google Scholar] [CrossRef] [PubMed]
- Wormald, R.; Sheahan, P.; Rowley, S.; Rizkalla, H.; Toner, M.; Timon, C. Hemithyroidectomy for benign thyroid disease: Who needs follow-up for hypothyroidism? Clin. Otolaryngol. 2008, 33, 587–591. [Google Scholar] [CrossRef] [PubMed]
- Su, S.Y.; Grodski, S.; Serpell, J.W. Hypothyroidism Following Hemithyroidectomy. Ann. Surg. 2009, 250, 991–994. [Google Scholar] [CrossRef]
- Sala, A.; Labrador-Horrillo, M.; Guilarte, M.; Luengo, O.; Rueda, M.; Cardona, V. Immediate-type hypersensitivity reaction to levothyroxine and desensitization. Ann. Allergy Asthma Immunol. 2008, 100, 513–514. [Google Scholar] [CrossRef]
- Bahloul, N.; Ben Mahmoud, L.; Ghozzi, H.; Hadjkacem, F.; Zeghal, K.; Abid, M.; Kammoun, S. Hypersensitivity to levothyroxine: A case report of a successful oral desensitization. Therapie 2018, 73, 349–350. [Google Scholar] [CrossRef] [PubMed]
- Shibata, H.; Hayakawa, H.; Hirukawa, M.; Tadokoro, K.; Ogata, E. Hypersensitivity caused by synthetic thyroid hormones in a hypothyroid patient with Hashimoto’s thyroiditis. Arch. Intern. Med. 1986, 146, 1624–1625. [Google Scholar] [CrossRef] [PubMed]
- Gansert, E.; Garzon-Siatoya, W.; Morgenstern-Kaplan, D.; Gonzalez-Estrada, A. A tale of two patients with hypersensitivity reactions to levothyroxine. QJM Int. J. Med. 2022, 115, 327–328. [Google Scholar] [CrossRef] [PubMed]
- Saleh, A. Survival and Functional Capacity of Heterotopic Thyroid Autograft after Total Thyroidectomy for Benign Goiters. Master’s Thesis, Faculty of Medicine, Alexandria University, Alexandria, Egypt, 2016. [Google Scholar]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
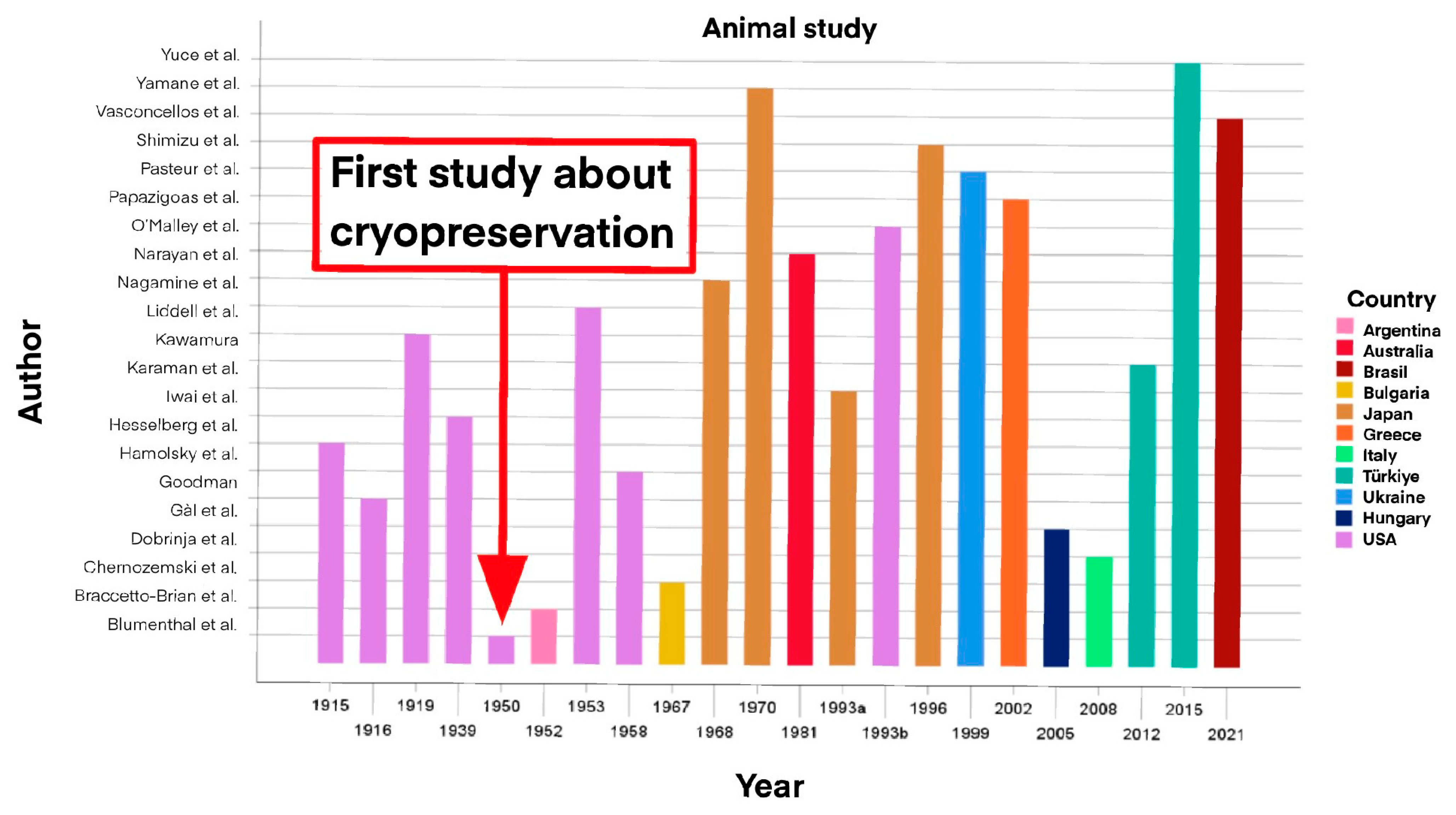
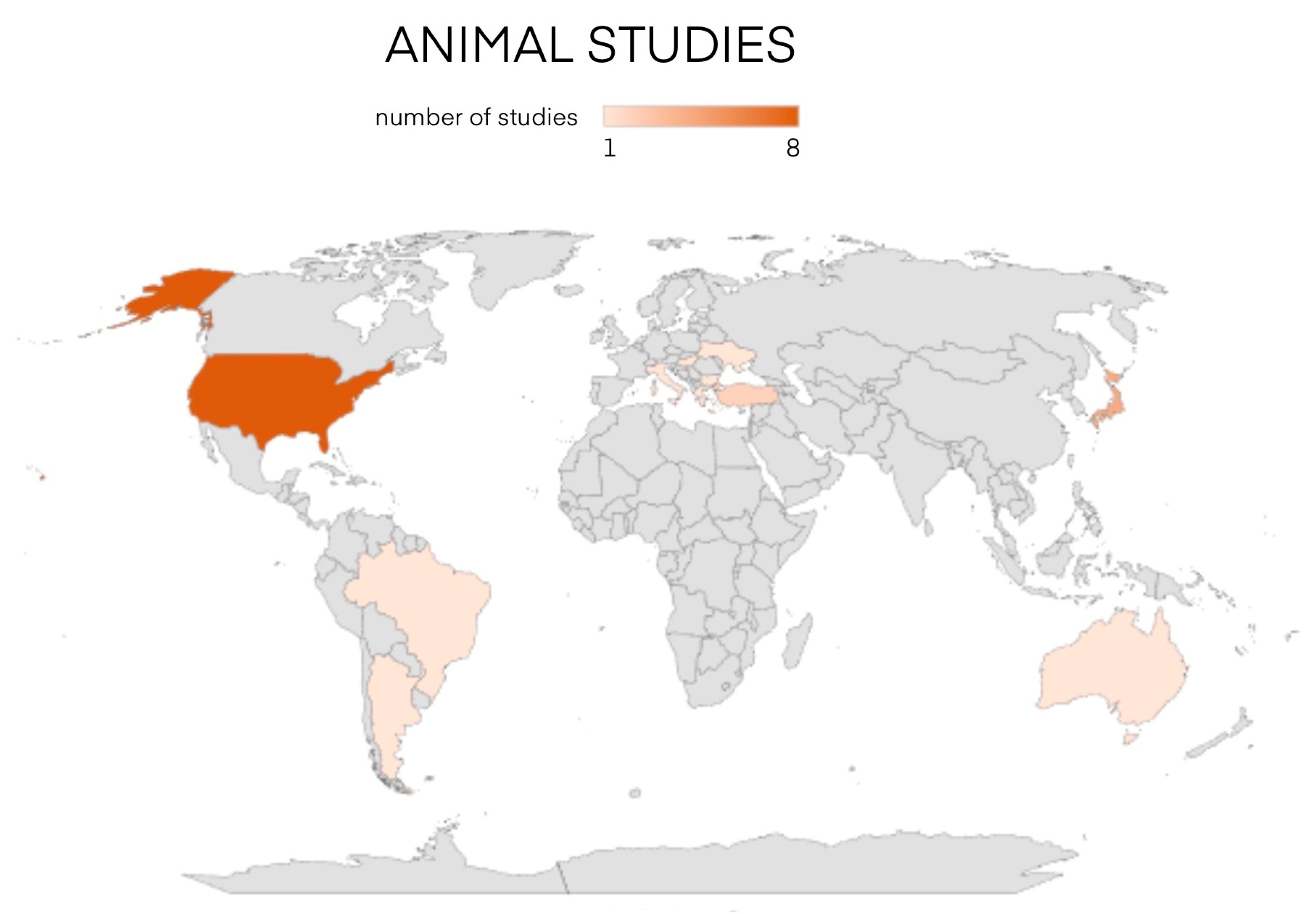
| Authors | Year | Country | Animal | No. of Animals | Site of Transplant | Surgery | Follow-Up (Months) | Success |
|---|---|---|---|---|---|---|---|---|
| Hesselberg et al. [32] | 1915 | USA | Guinea pigs | 75 | Abdomen | Immediate autotransplant Immediate allotransplant | 0–2 | Good |
| Goodman [31] | 1916 | USA | Dogs | 3 | Vessels | Immediate autotransplant | 1< | Dead |
| Kawamura [30] | 1919 | USA | Dogs | 8 7 | Vessels | Immediate autotransplant Immediate allotransplant | 2 | Dead |
| Ingle et al. [67] | 1939 | USA | Rats | 22 | Ovary | Immediate autotransplant | 0–3 | Good |
| Blumenthal et al. [27] | 1950 | USA | Guinea pigs | 12 12 | Subcutis | Post-cryopreservation Autotransplant at −70 °C Post-cryopreservation Autotransplant at −190 °C Immediate autotransplant | 0.5 | 1 8 <1 |
| Brachetto-Brian et al. [40] | 1952 | Argentina | Rats | - | Spleen | Non-specified autotransplant | - | - |
| Liddle et al. [28] | 1953 | USA | Dogs | - | - | Non-specified autotransplant | - | - |
| Hamolsky et al. [29] | 1958 | USA | Rats | - | Armpit Spleen | Only thyroidectomy Immediate autotransplant Sham surgery | Up to 12 | Good |
| Chernozemski et al. [34] | 1967 | Bulgaria | Syrian hamsters | 13 16 19 | Cheek | Immediate autotransplant Allotransplant Allotransplant (without thyroidectomy) | 1.5–3 | 12 13 4 |
| Nagamine et al. [42] | 1968 | Japan | Dogs | 100 | Bikini lineNeck | Immediate autotransplantSham surgeryThyroid denervationLymphatics binding | >2 | Yes |
| Narayan et al. [45] | 1981 | Australia | Rabbits | 17 | Ear | Immediate autotransplant | 11 | Good |
| Iwai et al. [39] | 1993 | Japan | Rats | 8 | Spleen and retroperitoneal fat | Immediate autotransplant | 0.7 | Positive |
| O’Malley et al. [33] | 1993 | USA | Dogs | - | Thyroid | Immediate orthotopic autotransplant | 0.5 | Positive |
| Shimizu et al. [38] | 1996 | Japan | Rats | - | Renal capsule or muscles | Immediate autotransplant Cryopreserved autotransplant | 1.5–2 | Both |
| Pasteur et al. [35] | 1999 | Ukraine | Pig | - | In vitro | - | 1 | Yes |
| Papaziogas et al. [18] | 2002 | Greece | Rabbits | 10 10 10 8 | Quadriceps Rectus abdominis Back muscle | Immediate autotransplant Control | 2 | Very good |
| Gál et al. [36] | 2005 | Hungary | Dogs | 12 | Sternocleidomastoid and greater omentum | Cryopreserved autotransplant | 1 | Yes |
| Dobrinja et al. [37] | 2008 | Italy | Rats | 60 | Rectus abdominis | Immediate autotransplant Non-specified autotransplant | 1 | 70% |
| Karaman et al. [43] | 2012 | Turkey | Guinea pigs | 6 6 6 6 | Back muscle | Incision only Thyroidectomy Immediate autotransplant Heterotransplant | 2 | Yes |
| Yüce et al. [44] | 2015 | Turkey | Rabbits | 16 | Quadriceps | Immediate autotransplant Cryopreserved autotransplant | 2 | Euthyroid AI (autotrap) Increasing AC (cryopreserved autotransplant) |
| Vasconcellos et al. [41] | 2021 | Brazil | Male albino rats | 8 8 8 8 | Biceps femoris muscle | Control Sham surgery Thyroidectomy Cryopreserved autotransplant | 3.3 | 8 |
| Schanaider et al. [68] | 2022 | Brazil | Rats | 8 8 8 | Biceps femoris muscle | Control Thyroidectomy Cryopreserved autotransplant | 3.5 | Yes |
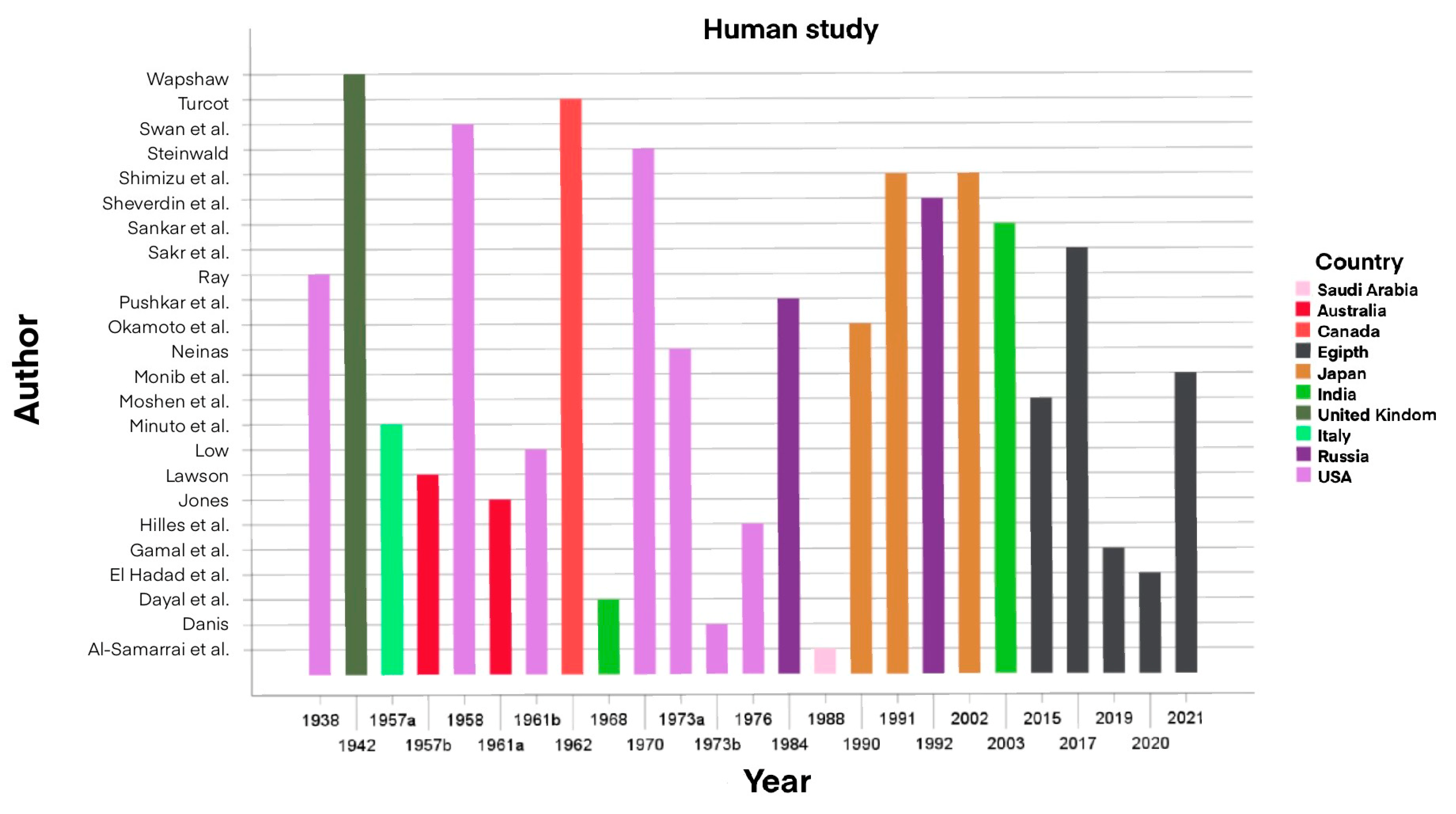
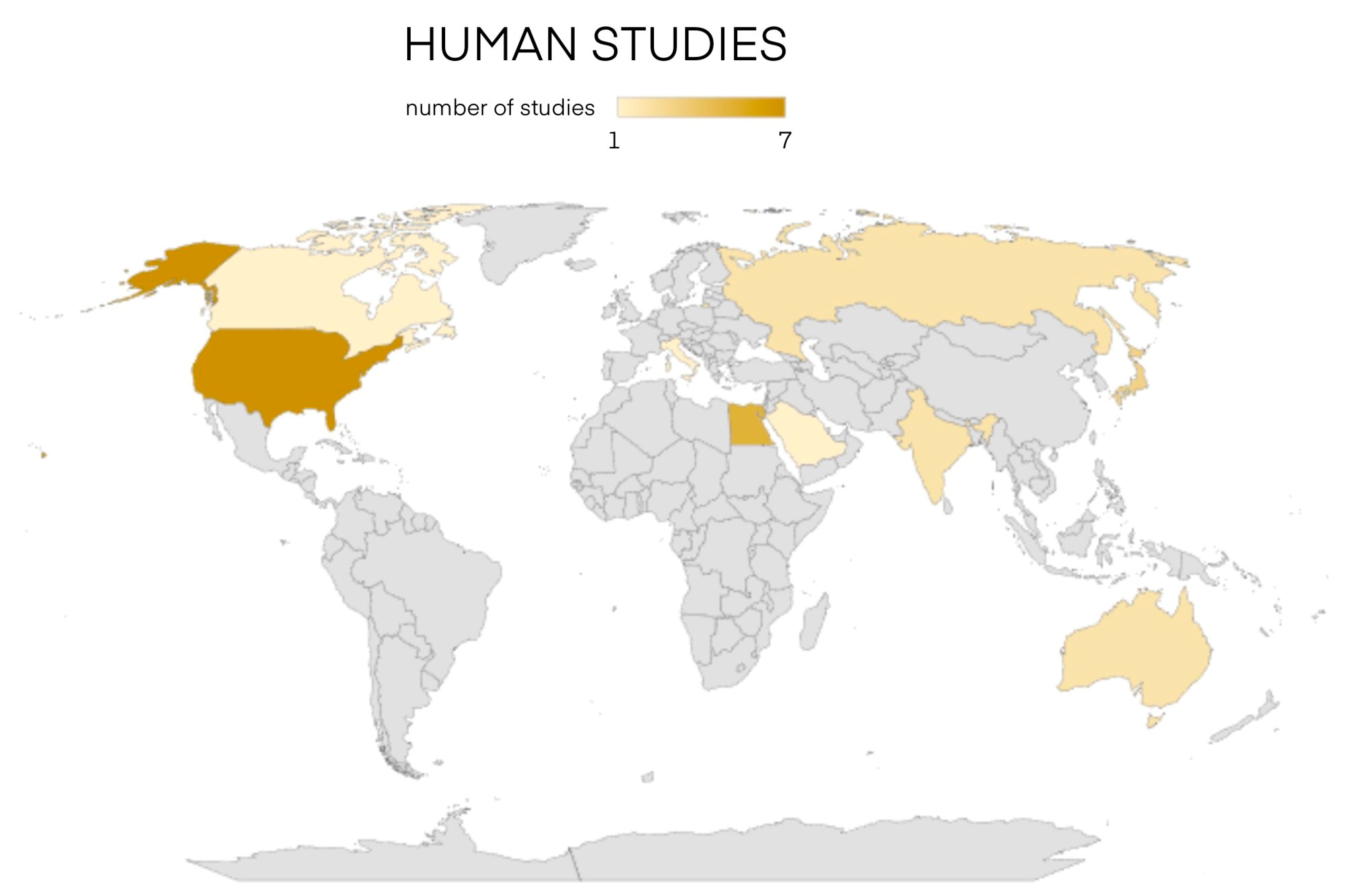
| Author | Year | Country | No. of Patients | Patient’s Age (Years) | Sex | Pathology | Transplant Site | Surgery | Weight (g) | Months to Return to Euthyroid | Follow-Up Length (Months) |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Ray [2] | 1938 | USA | 1 | 39 | M | Lingual thyroid ectopia | Rectus abdominis | Immediate autotransplant | - | Failure | - |
| Wapshaw [61] | 1942 | England | 1 | 20 | F | Lingual thyroid ectopia | Neck | Immediate autotransplant | - | Failure | >12 |
| Minuto et al. [3] | 1995 | Italy | 1 | 18 | F | Lingual thyroid ectopia | Rectus abdominis | Immediate autotransplant | - | 5 months | 444 |
| Lawson [51] | 1957 | Australia | 2 | 11 | F | Lingual thyroid ectopia | Rectus abdominis | Immediate autotransplant | - | - | 9 |
| Swan et al. [46,47] | 1958 | USA | 1 | 7 | F | Lingual thyroid ectopia | Rectus abdominis | Immediate autotransplant | 2 | 6 months | 96 |
| Jones [58] | 1961 | Australia | 1 | 9 | F | Lingual thyroid ectopia | Rectus abdominis | Immediate autotransplant | - | 1 | 24 |
| Low [48] | 1961 | USA | 1 | 2 | F | Lingual thyroid ectopia | Sternocleidomastoid | Immediate autotransplant | - | 6 | 6 |
| Turcot [59] | 1962 | Canada | 2 | 514 | F | Lingual thyroid ectopia | Rectus abdominis | Immediate autotransplant | - | Transplant failure | 2 |
| Dayal et al. [57] | 1968 | India | 1 | 20 | F | Lingual thyroid ectopia | Submandibular glands neck | Immediate autotransplant | - | - | 12 |
| Steinwald [49] | 1970 | USA | 1 | 9 | F | Lingual thyroid ectopia | Pectoralis major and rectus abdominis | Immediate autotransplant | - | - | 7 |
| Neinas [50] | 1973 | USA | 2 | - | F | Lingual thyroid ectopia | Neck and abdomen | Immediate autotransplant | - | 1 failure - | 1 |
| Danis [66] | 1973 | USA | 1 | 8 | M | Lingual thyroid ectopia | Thigh | Immediate autotransplant | - | - | 72 |
| Hilles et al. [62] | 1976 | USA | 1 | 39 | F | Lingual thyroid ectopia with nodular goiter | Rectus abdominis | Immediate autotransplant | 20 | - | 8 |
| Pushkar’ et al. [15] | 1984 | Russia | - | - | - | Post-surgical hypothyroidism | - | Post-cryopreservation (4–12 months) autotransplant | - | - | 18 |
| Al-Samarrai et al. [60] | 1988 | Saudi Arabia | 1 | 9 | F | Lingual thyroid ectopia | Neck | Immediate autotransplant | - | 4 | 5,5 |
| Okamoto et al. [64] | 1990 | Japan | 5 | 39 34 28 26 26 | 2M 3F | Graves’ disease | Sternocleidomastoid or neck muscles | Immediate autotransplant (with STT) | 0.5–2 | - | 26.4–84 |
| Shimizu et al. [17] | 1991 | Japan | 1 | - | - | Graves’ disease | - | Post-cryopreservation autotransplant post-STT | - | - | - |
| Sheverdin et al. [65] | 1992 | Russia | 246 | Children and adults | - | Thyrotoxicosis | - | Immediate autotransplant vs. Thyroidectomy | - | 3,2% of patients, 6 months in transplants vs. 6,6% non-treated patients | 2–180 |
| Shimizu et al. [16] | 2002 | Japan | 4 | 58 45 21 34 | 3F 1M | Graves’ disease | Forearm | Post-cryopreservation autotransplant post-STT | 2.5–3.5 | 6 (3 out of 4 patients) | - |
| Sankar et al. [63] | 2003 | India | 15 | - | - | 7 Graves’ disease 8 Multinodular goiter | Sternocleidomastoid | Immediate autotransplant with STT | 3–5 | 6 months in functioning transplanted patients (9 out of 15) | 6 |
| Mohsen et al. [55] | 2017 | Egypt | 40 | - | - | Multinodular goiter | Thigh | Immediate autotransplant | 5–10 | Some months | 12 |
| Sakr et al. [1,56] | 2017 | Egypt | 20 | 24–49 | 15 F 5 M | 13 Multinodular goiter 4 Graves’ disease 3 Nodular goiter | Thigh | Immediate autotransplant | 10–15 | 2–12 (2 papillary carcinomas with transplant removal) | 12 |
| Gamal et al. [54] Mohamed Kotb et al. [69] | 2019 2022 | Egypt | 30 | 20–55 | 7 M 23 F | 4 Graves’ disease 2 Hashimoto 24 Nodular goiter | Sternocleidomastoid | Immediate autotransplant | 2–5 | 6 | 12 |
| El Hadad et al. [53] | 2020 | Egypt | 40 | - | - | Multinodular goiter | Thigh | Immediate autotransplant | 5–10 | 2–12 | 12 |
| Monib et al. [52] | 2021 | Egypt | 40 | 24–53 | F | Multinodular goiter | Thigh | Immediate autotransplant | 10–15 | 2–12 | 12 |
| CASES | Gender | Age (Years) | Thyroid Pathology | Cytological Examination | Surgery | Histological Examination |
|---|---|---|---|---|---|---|
| CASE1 | F | 13 | Multinodular goiter of the left lobe | TIR2A nodule | Left hemithyroidectomy | Micro-macrofollicular nodule with hyperplastic aspects and collateral multinodular thyroid parenchyma |
| CASE2 | F | 16 | Nodular goiter of the left lobe | TIR2 oxyphilic cell nodule | Left lobe-isthmectomy | Papillary carcinoma (3 cm) follicular variant with solid aspects (30%), capsulated, multifocal |
| CASE3 | F | 17 | Nodular goiter of the right lobe | TIR3B oxyphilic cell microfollicular nodule | Right lobectomy | Micro-macrofollicular thyroid parenchyma |
| CASE4 | F | 13 | Isthmic nodular goiter of the right lobe | TIR3A isthmic thyroid nodule with microfollicular cytology | Right lobe-isthmectomy | Micro-macrofollicular isthmic nodule with marked hyperplastic aspects and regressive phenomena |
| CASE5 | F | 9 | Nodular goiter of the right lobe | Nodule in the right lobe of the thyroid TIR2 | Right lobectomy | Micro-macrofollicular nodule with widespread and marked hyperplastic aspects and focal regressive phenomena |
| CASE6 | F | 10 | Nodular goiter of the left lobe | Papillary thyroid carcinoma TIR5 | Left lobe-isthmectomy | Classic variant papillary carcinoma focally infiltrating the loose perithyroid tissues and, microscopically, the muscular tissues; multifocal; presence of widespread lymphatic and vascular embolization (No. emboli < 4) and multiple lymph node metastases |
| CASE7 | M | 15 | Bilateral multinodular goiter | TIR3A thyroid nodule | Near total thyroidectomy | Bilateral micro-macrofollicular nodules with marked hyperplastic aspects; collateral multinodular thyroid parenchyma |
| CASE8 | M | 8 | MEN2A | - | Total thyroidectomy | Focal C cell hyperplasia |
| CASE9 | F | 10 | Multinodular goiter of the right lobe | TIR3B microfollicular architecture nodule | Total thyroidectomy | Classic variant papillary carcinoma (1.5 cm), capsulated, bilateral in multinodular goiter |
| CASE10 | F | 18 | Nodular goiter of the right lobe | TIR3B cytology nodule | Right lobectomy | Microfollicular adenoma |
| CASE 11 | F | 12 | Nodular goiter of the right lobe | TIR3 cytology nodule | Thyroidectomy | Microfollicular adenoma with hyperplastic aspects |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Spinelli, C.; Ghionzoli, M.; Sahli, L.I.; Visintainer, S.; Guglielmo, C.; Cordola, C.; Lapi, S.; Biagi, E.; Pucci, A.; Morganti, R.; et al. Cryopreserved Thyroid Tissue Autotransplant in Pediatric Age Patients: A Feasibility Study and Literature Review. Cancers 2024, 16, 2112. https://doi.org/10.3390/cancers16112112
Spinelli C, Ghionzoli M, Sahli LI, Visintainer S, Guglielmo C, Cordola C, Lapi S, Biagi E, Pucci A, Morganti R, et al. Cryopreserved Thyroid Tissue Autotransplant in Pediatric Age Patients: A Feasibility Study and Literature Review. Cancers. 2024; 16(11):2112. https://doi.org/10.3390/cancers16112112
Chicago/Turabian StyleSpinelli, Claudio, Marco Ghionzoli, Linda Idrissi Sahli, Silvia Visintainer, Carla Guglielmo, Chiara Cordola, Simone Lapi, Elisa Biagi, Angela Pucci, Riccardo Morganti, and et al. 2024. "Cryopreserved Thyroid Tissue Autotransplant in Pediatric Age Patients: A Feasibility Study and Literature Review" Cancers 16, no. 11: 2112. https://doi.org/10.3390/cancers16112112
APA StyleSpinelli, C., Ghionzoli, M., Sahli, L. I., Visintainer, S., Guglielmo, C., Cordola, C., Lapi, S., Biagi, E., Pucci, A., Morganti, R., Ferrari, S. M., & Antonelli, A. (2024). Cryopreserved Thyroid Tissue Autotransplant in Pediatric Age Patients: A Feasibility Study and Literature Review. Cancers, 16(11), 2112. https://doi.org/10.3390/cancers16112112